AIBMS Lab Report: Bromocresol Green vs. Purple Albumin Assays, 2017-8
VerifiedAdded on 2023/06/15
|11
|2799
|162
Report
AI Summary
This AIBMS laboratory report compares the use of Bromocresol Green (BCG) and Bromocresol Purple (BCP) in albumin concentration analysis in human serum. The study involves analyzing patient serum samples using both methods with varying incubation times. The results show a strong correlation between the methods, with BCG tending to yield slightly higher values. The discussion covers the advantages and disadvantages of each method, including specificity, accuracy, and potential interference. The report concludes that while BCP is more specific, BCG with a short reaction time remains a viable option, especially considering the practical implications of switching methodologies in clinical settings. The report also includes standard curves, data analysis, and answers to supplementary questions regarding the quality of standard curves, acceptable CV for albumin assays, and the effects of heparin on albumin levels. This assignment is available on Desklib, a platform that provides AI-based study tools and solved assignments for students.

Running head: REPORT 1
AIBMS Laboratory Report
By (Author’s Name)
(Institutional Affiliation)
(Instructor’s Name)
(Course Tittle/ Code)
(Date of Submission)
AIBMS Laboratory Report
By (Author’s Name)
(Institutional Affiliation)
(Instructor’s Name)
(Course Tittle/ Code)
(Date of Submission)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REPORT 2
Abstract
Patient’s serum with a wide range of albumin was pooled and analyzed for albumin by
Bromocresol purple with both short and long incubation times and also by bromocresol green.
The linear correlations of all the two methods used to measure albumin were almost similar. The
values of albumin measured by bromocresol green with a short period of incubation averaged
higher as compared by those measured by bromocresol purple across all the concentrations.
Closely observed, we found out that there were negligible differences when the different
methods were used. When closely monitored bromocresol purple has no significant difference or
benefits as compared to bromocresol green with a short time of incubation for the medical uses
for which albumin is measured for example in the detection of abnormality, monitoring of
change, approximation of the colloid osmotic pressure and in the adjustment of either
magnesium or calcium for normal concentrations of protein. This experiment is one of the most
risky ones since it involves blood serum and can be very infectious. We therefore took
appropriate measures to ensure our safety when performing the experiment. Preferably we liked
the BCG since it’s consistent and fast.
Introduction
The analysis of serum albumin for many years has been used across the world in the diagnosis of
disease. It is particularly important in the consideration of liver and kidney diseases for example;
nephropathy and cirrhosis. Levels of albumin have also been crucial in monitoring diseases for
example kidney dialysis and transplants, and to contribute to the prognosis of mortality and
morbidity after a stroke or heart surgery.
In addition, serum albumin has been used as an indicator of malnutrition although it is not
considered reliable and history and clinical presentation of the patient is more important in
making a diagnosis. Debate on which dye is the best when analysing the human blood serum and
specifically the albumin component continue to thrive and as much as many clinical medics still
insist on using the BCG, other Biologists have adopted BCP. BCP results though highly specific
may underestimate albumin in patients who are suffering from renal diseases and those with
serum albumin complications. BCG is however consistent and give more accurate results. Apart
from this fact BCG is also easy to learn how to use.
Abstract
Patient’s serum with a wide range of albumin was pooled and analyzed for albumin by
Bromocresol purple with both short and long incubation times and also by bromocresol green.
The linear correlations of all the two methods used to measure albumin were almost similar. The
values of albumin measured by bromocresol green with a short period of incubation averaged
higher as compared by those measured by bromocresol purple across all the concentrations.
Closely observed, we found out that there were negligible differences when the different
methods were used. When closely monitored bromocresol purple has no significant difference or
benefits as compared to bromocresol green with a short time of incubation for the medical uses
for which albumin is measured for example in the detection of abnormality, monitoring of
change, approximation of the colloid osmotic pressure and in the adjustment of either
magnesium or calcium for normal concentrations of protein. This experiment is one of the most
risky ones since it involves blood serum and can be very infectious. We therefore took
appropriate measures to ensure our safety when performing the experiment. Preferably we liked
the BCG since it’s consistent and fast.
Introduction
The analysis of serum albumin for many years has been used across the world in the diagnosis of
disease. It is particularly important in the consideration of liver and kidney diseases for example;
nephropathy and cirrhosis. Levels of albumin have also been crucial in monitoring diseases for
example kidney dialysis and transplants, and to contribute to the prognosis of mortality and
morbidity after a stroke or heart surgery.
In addition, serum albumin has been used as an indicator of malnutrition although it is not
considered reliable and history and clinical presentation of the patient is more important in
making a diagnosis. Debate on which dye is the best when analysing the human blood serum and
specifically the albumin component continue to thrive and as much as many clinical medics still
insist on using the BCG, other Biologists have adopted BCP. BCP results though highly specific
may underestimate albumin in patients who are suffering from renal diseases and those with
serum albumin complications. BCG is however consistent and give more accurate results. Apart
from this fact BCG is also easy to learn how to use.
REPORT 3
Principle of the Experiment
The Bromcresol green (BCG) dye-binding assay for the determination of serum albumin was
developed in 1965 by Rodkey. It was again revised (Bartholomew & Delaney, 1965; Doumas,
Watson & Biggs, 1971) to give out a more reliable, sensitive and inexpensive assay that was
used widely in clinical biochemistry laboratories for many years. Increasing concern that the
technique was limited in its specificity and provided an overestimation of values determined by
immunoassay led to the introduction of an a different dye-binding assay founded on Bromcresol
purple ( abbreviated as BCP) (Louderback, Mealy & Taylor, 1968; Carter, 1970; Pinnell &
Northam, 1978). However, the bromocresol purple assay, though more specific, is widely
variable than analysis by BCG and also gives a lower serum albumin reading in patients
undergoing hemodialysis. Despite the shortcomings of the assays both are still routinely used,
the particular technique adopted depending on the preference of each individual laboratory.
Planning
The task before us was to conduct an investigation to find out and compare the usage of BCG
and BCP in the analysis of albumin concentrations in the serum of human beings. Standard
curves were performed in the first session thereafter the planned experiment took place in the
session that followed.
The major points that were considered during the experiment were: standard curves, incubation
times, patient samples and QC. In our individual log books we designed an experiment
comparing the two methods.
The following materials were provided:
1. Stock standard solution of BCP.
2. Stock standard solution of BCG.
3. Samples from 10 patients.
The experiment was carried out with a lot of precaution because human blood is considered to be
potentially infectious. The samples were handled carefully then disposed off appropriately.
Principle of the Experiment
The Bromcresol green (BCG) dye-binding assay for the determination of serum albumin was
developed in 1965 by Rodkey. It was again revised (Bartholomew & Delaney, 1965; Doumas,
Watson & Biggs, 1971) to give out a more reliable, sensitive and inexpensive assay that was
used widely in clinical biochemistry laboratories for many years. Increasing concern that the
technique was limited in its specificity and provided an overestimation of values determined by
immunoassay led to the introduction of an a different dye-binding assay founded on Bromcresol
purple ( abbreviated as BCP) (Louderback, Mealy & Taylor, 1968; Carter, 1970; Pinnell &
Northam, 1978). However, the bromocresol purple assay, though more specific, is widely
variable than analysis by BCG and also gives a lower serum albumin reading in patients
undergoing hemodialysis. Despite the shortcomings of the assays both are still routinely used,
the particular technique adopted depending on the preference of each individual laboratory.
Planning
The task before us was to conduct an investigation to find out and compare the usage of BCG
and BCP in the analysis of albumin concentrations in the serum of human beings. Standard
curves were performed in the first session thereafter the planned experiment took place in the
session that followed.
The major points that were considered during the experiment were: standard curves, incubation
times, patient samples and QC. In our individual log books we designed an experiment
comparing the two methods.
The following materials were provided:
1. Stock standard solution of BCP.
2. Stock standard solution of BCG.
3. Samples from 10 patients.
The experiment was carried out with a lot of precaution because human blood is considered to be
potentially infectious. The samples were handled carefully then disposed off appropriately.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
REPORT 4
Outline Protocol for Bromocresol Green Assay
• Set the spectrophotometer to 628nm wavelength and zero using BCG reagent.
• In a test tube add 24 μl of standard or 10μl of sample or QC to 2mls of BCG reagent and
mix well.
• Incubate at room temperature.
• Measure the absorbance for each and use the data to determine the concentration of
albumin.
The Procedure for Bromocresol Green Assay Preparation
The spectrophotometer was set to give a reading of 628nm wavelength and then zeroed using a
BCP reagent. 10μl of sample was then added to the test tube containing 2ml of BCG reagent. The
mixture was then slightly shaken to mix it well. It was then incubated at room temperature. The
absorbance was then measured for each sample and resulting data used to calculate the
concentration of albumin.
The Procedure for Bromocresol Purple Assay
The spectrophotometer was set to give a reading of 600nm wavelength and then zeroed using a
BCP reagent. 10μl of sample was then added to the test tube containing 2ml of BCG reagent.
The mixture was then slightly shaken to mix it well. It was then incubated at room temperature.
The absorbance was then measured for each sample and resulting data used to calculate the
concentration of albumin.
Part 2: The information in the table below was used to construct a set of standard curves.
The table below shows the volumes of stock serum and saline needed to make up and appropriate
set of standards.
Tube 0.9% NaCl (μl) Stock Serum (μl) The Final Concentration (grams/L)
Saline Blank 60 0 0.0
S1 35 25 27.0
Outline Protocol for Bromocresol Green Assay
• Set the spectrophotometer to 628nm wavelength and zero using BCG reagent.
• In a test tube add 24 μl of standard or 10μl of sample or QC to 2mls of BCG reagent and
mix well.
• Incubate at room temperature.
• Measure the absorbance for each and use the data to determine the concentration of
albumin.
The Procedure for Bromocresol Green Assay Preparation
The spectrophotometer was set to give a reading of 628nm wavelength and then zeroed using a
BCP reagent. 10μl of sample was then added to the test tube containing 2ml of BCG reagent. The
mixture was then slightly shaken to mix it well. It was then incubated at room temperature. The
absorbance was then measured for each sample and resulting data used to calculate the
concentration of albumin.
The Procedure for Bromocresol Purple Assay
The spectrophotometer was set to give a reading of 600nm wavelength and then zeroed using a
BCP reagent. 10μl of sample was then added to the test tube containing 2ml of BCG reagent.
The mixture was then slightly shaken to mix it well. It was then incubated at room temperature.
The absorbance was then measured for each sample and resulting data used to calculate the
concentration of albumin.
Part 2: The information in the table below was used to construct a set of standard curves.
The table below shows the volumes of stock serum and saline needed to make up and appropriate
set of standards.
Tube 0.9% NaCl (μl) Stock Serum (μl) The Final Concentration (grams/L)
Saline Blank 60 0 0.0
S1 35 25 27.0
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REPORT 5
S2 30 30 32.4
S3 25 35 37.8
S4 20 40 43.2
S5 15 45 48.6
S6 10 50 54.0
S7 5 55 59.4
S8 0 60 64.8
AI-P2b: Evaluation of two albumin assays
This experiments helps to understand the considerations necessary when developing biochemical
assay for clinical use.
Determination of inter-assay variation
The assay was repeated 5 times using every patients sample for each reagent at a chosen
incubation time. The coefficients for each set of assays was then calculated.
S2 30 30 32.4
S3 25 35 37.8
S4 20 40 43.2
S5 15 45 48.6
S6 10 50 54.0
S7 5 55 59.4
S8 0 60 64.8
AI-P2b: Evaluation of two albumin assays
This experiments helps to understand the considerations necessary when developing biochemical
assay for clinical use.
Determination of inter-assay variation
The assay was repeated 5 times using every patients sample for each reagent at a chosen
incubation time. The coefficients for each set of assays was then calculated.
REPORT 6
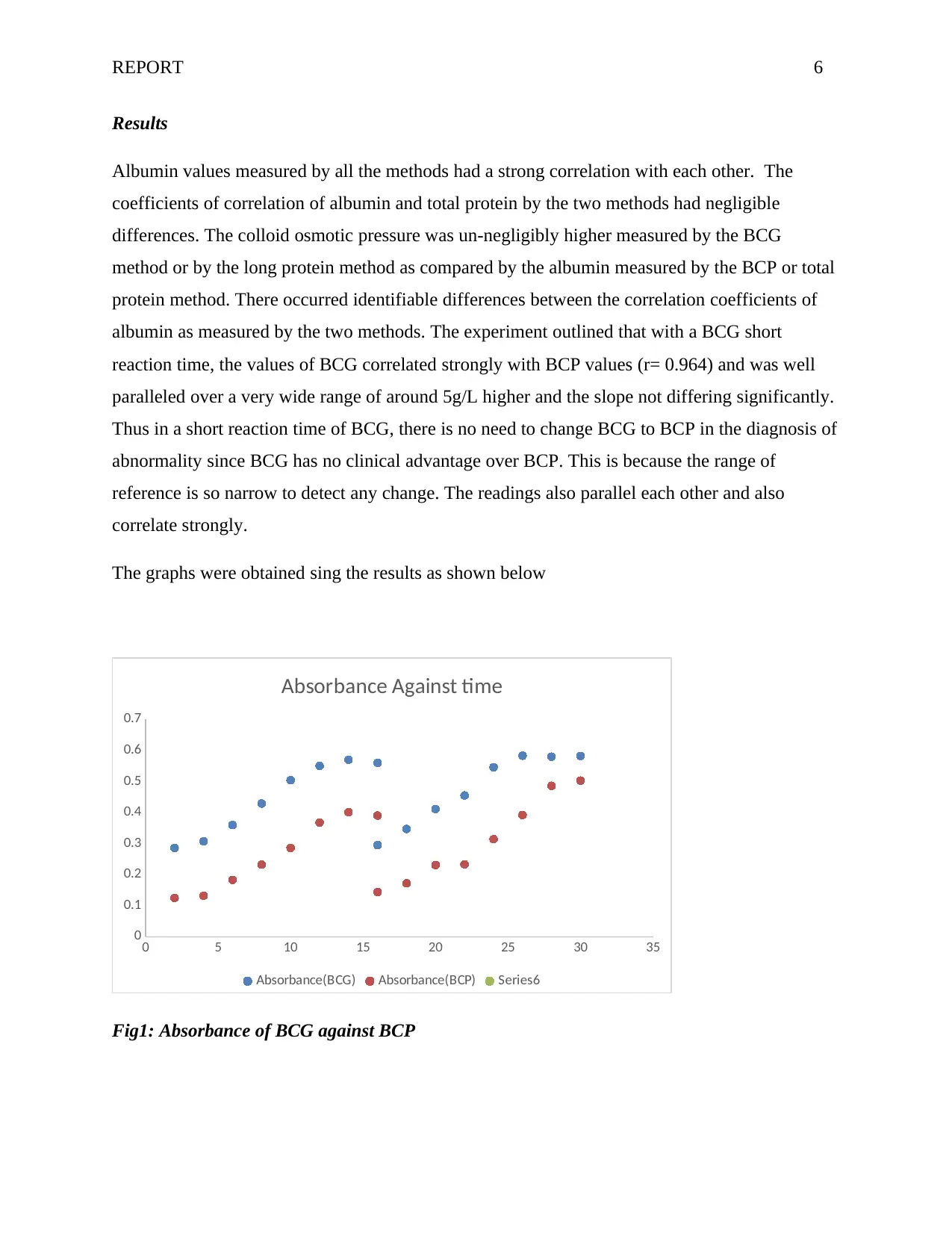
Results
Albumin values measured by all the methods had a strong correlation with each other. The
coefficients of correlation of albumin and total protein by the two methods had negligible
differences. The colloid osmotic pressure was un-negligibly higher measured by the BCG
method or by the long protein method as compared by the albumin measured by the BCP or total
protein method. There occurred identifiable differences between the correlation coefficients of
albumin as measured by the two methods. The experiment outlined that with a BCG short
reaction time, the values of BCG correlated strongly with BCP values (r= 0.964) and was well
paralleled over a very wide range of around 5g/L higher and the slope not differing significantly.
Thus in a short reaction time of BCG, there is no need to change BCG to BCP in the diagnosis of
abnormality since BCG has no clinical advantage over BCP. This is because the range of
reference is so narrow to detect any change. The readings also parallel each other and also
correlate strongly.
The graphs were obtained sing the results as shown below
0 5 10 15 20 25 30 35
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Absorbance Against time
Absorbance(BCG) Absorbance(BCP) Series6
Fig1: Absorbance of BCG against BCP
Results
Albumin values measured by all the methods had a strong correlation with each other. The
coefficients of correlation of albumin and total protein by the two methods had negligible
differences. The colloid osmotic pressure was un-negligibly higher measured by the BCG
method or by the long protein method as compared by the albumin measured by the BCP or total
protein method. There occurred identifiable differences between the correlation coefficients of
albumin as measured by the two methods. The experiment outlined that with a BCG short
reaction time, the values of BCG correlated strongly with BCP values (r= 0.964) and was well
paralleled over a very wide range of around 5g/L higher and the slope not differing significantly.
Thus in a short reaction time of BCG, there is no need to change BCG to BCP in the diagnosis of
abnormality since BCG has no clinical advantage over BCP. This is because the range of
reference is so narrow to detect any change. The readings also parallel each other and also
correlate strongly.
The graphs were obtained sing the results as shown below
0 5 10 15 20 25 30 35
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Absorbance Against time
Absorbance(BCG) Absorbance(BCP) Series6
Fig1: Absorbance of BCG against BCP
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

REPORT 7
Discussion
There was a big difference in the absorbance values of the serum when different dyes were used.
This is caused by the difference in reaction of the dye and the serum. The standard curves of
bromocresol purple depict a more linear standard curve (more so when the albumin
concentration is higher) as compared to the linear standard curves of bromocresol green method.
We found out that bromocresol green method values are more comparable with measurements
obtained from other techniques when compared to the values obtained when bromocresol purple
is used. This gives BCG an advantage over BCP. In other experiments such as those involving
quality control and assurance, calibrations methods, BCP will sharply deviate from the expected
values especially when non-human sera was analyzed. Because of accuracy and consistency,
methods that are more specific should are recommended.
Research has shown that bromocresol green depicts nonspecific binding to non-albumin protein.
However BCP is highly specific as compared to BCG method. The differences between these
methods can be reduced but not completely done away with if the rapid-reaction technique is
employed where absorbance is values are recorded after short incubation times.
The ideology to adopt a new method in the analysis to BCP is not advisable because it will lead
to changed measurements for the similar analysis under investigation. The clinical staff will be
forced to learn a new range of reference in the investigation of the abnormality and also to adjust
the “limits of action” that have taken them a lot of years to acquire. The change will have to be
put into account and BE revised adequately especially when dealing with patients who are under
regular care. However, the new methodology can easily be adopted when it can convince medics
that will improve the medical benefits of the measurements.
The ideology attached to changing automated dye-binding procedure for the albumin serum from
bromocresol green to bromocresol purple is founded wholly on the non-specific reactions of
bromocresol green with serum globulins. In the experiments involving long reaction times the
over approximation of bromocresol green method is particularly marked t very low
concentrations of albumin , these measurements show a higher spread as compared with the
reference methods. Analysis with BCP will underestimate the albumin in the blood serum for
Discussion
There was a big difference in the absorbance values of the serum when different dyes were used.
This is caused by the difference in reaction of the dye and the serum. The standard curves of
bromocresol purple depict a more linear standard curve (more so when the albumin
concentration is higher) as compared to the linear standard curves of bromocresol green method.
We found out that bromocresol green method values are more comparable with measurements
obtained from other techniques when compared to the values obtained when bromocresol purple
is used. This gives BCG an advantage over BCP. In other experiments such as those involving
quality control and assurance, calibrations methods, BCP will sharply deviate from the expected
values especially when non-human sera was analyzed. Because of accuracy and consistency,
methods that are more specific should are recommended.
Research has shown that bromocresol green depicts nonspecific binding to non-albumin protein.
However BCP is highly specific as compared to BCG method. The differences between these
methods can be reduced but not completely done away with if the rapid-reaction technique is
employed where absorbance is values are recorded after short incubation times.
The ideology to adopt a new method in the analysis to BCP is not advisable because it will lead
to changed measurements for the similar analysis under investigation. The clinical staff will be
forced to learn a new range of reference in the investigation of the abnormality and also to adjust
the “limits of action” that have taken them a lot of years to acquire. The change will have to be
put into account and BE revised adequately especially when dealing with patients who are under
regular care. However, the new methodology can easily be adopted when it can convince medics
that will improve the medical benefits of the measurements.
The ideology attached to changing automated dye-binding procedure for the albumin serum from
bromocresol green to bromocresol purple is founded wholly on the non-specific reactions of
bromocresol green with serum globulins. In the experiments involving long reaction times the
over approximation of bromocresol green method is particularly marked t very low
concentrations of albumin , these measurements show a higher spread as compared with the
reference methods. Analysis with BCP will underestimate the albumin in the blood serum for
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REPORT 8
example in patients of pediatric hemodialysis it would give reading of 13g/L, BCG is however
not affected and would give normal readings. Adults suffering from renal insufficiency when
their blood serum is analyzed will also affect the BCP. From the experiment we confirmed that
albumin can be falsely elevated up to 11g/L when plasma is used with BCP. The resemblance of
correlation in turbidity and concentration of albumin in the blood serum is an evidence that the
elevated results of the serum is caused by turbidity that increases the absorbance readings and
hence leading to larger calculated values of concentrations. Our data however did not show that
the higher readings of results we obtained were due to the elevated color of BCP-albumin
complex. It however showed that samples of plasma required blanks that are separate due to
turbidity.
We were unable to single out any benefit of the bromocresol purple-albumin over bromocresol
green that could convince us that patients will find it useful in the event of change. We found out
that laboratories that continue to use BCG in the diagnosis their patients have been criticized for
conservatism however, as long as a method that involves a short reaction time is used, we will
advocate for conservatism.
Questions
a) Comment on the quality of standard curves.
Standard curves allow for comparison of known properties of samples which are then used to
determine the qualities of unknown samples at interpolation. Comparing the slopes and the
coefficients we find that the coefficients are sufficient and therefore we can say that the curves
are of good quality.
b) What is the usual acceptable CV for an albumin assay to enable its use in clinical diagnosis?
2.9% at mean values of 30.6 and 38.3g/L
c) Under which circumstances can the BCG assay give elevated readings for serum albumin?
Assay of BCG can give slightly higher values in patients who are suffering from hypo-albumin
emic and are undergoing hemodialysis.
Or when fibrinogen is involved in the serum, e.g. in heparinized canine plasma due to specific
binding to globulins.
example in patients of pediatric hemodialysis it would give reading of 13g/L, BCG is however
not affected and would give normal readings. Adults suffering from renal insufficiency when
their blood serum is analyzed will also affect the BCP. From the experiment we confirmed that
albumin can be falsely elevated up to 11g/L when plasma is used with BCP. The resemblance of
correlation in turbidity and concentration of albumin in the blood serum is an evidence that the
elevated results of the serum is caused by turbidity that increases the absorbance readings and
hence leading to larger calculated values of concentrations. Our data however did not show that
the higher readings of results we obtained were due to the elevated color of BCP-albumin
complex. It however showed that samples of plasma required blanks that are separate due to
turbidity.
We were unable to single out any benefit of the bromocresol purple-albumin over bromocresol
green that could convince us that patients will find it useful in the event of change. We found out
that laboratories that continue to use BCG in the diagnosis their patients have been criticized for
conservatism however, as long as a method that involves a short reaction time is used, we will
advocate for conservatism.
Questions
a) Comment on the quality of standard curves.
Standard curves allow for comparison of known properties of samples which are then used to
determine the qualities of unknown samples at interpolation. Comparing the slopes and the
coefficients we find that the coefficients are sufficient and therefore we can say that the curves
are of good quality.
b) What is the usual acceptable CV for an albumin assay to enable its use in clinical diagnosis?
2.9% at mean values of 30.6 and 38.3g/L
c) Under which circumstances can the BCG assay give elevated readings for serum albumin?
Assay of BCG can give slightly higher values in patients who are suffering from hypo-albumin
emic and are undergoing hemodialysis.
Or when fibrinogen is involved in the serum, e.g. in heparinized canine plasma due to specific
binding to globulins.
REPORT 9
d) What is the effect of heparin on albumin levels measured by both methods?
Heparin boosts the level of albumin in the samples. Since BCP is more specific it’s readings
would not be much affected but BCG readings would be elevated since the concentration of the
albumin is increased.
Heparin would only BCG readings since and not BCP because BCP is more specific to globulin
e) Which method can be adapted to account for the potential interference by heparin?
Bromocresol purple method.
f) Which pathophysiological circumstances lead to albumin being underestimated by the BCP
assay?
Renal failure in patients who are undergoing hemodialysis care in hospitals. This because of a
uremic toxin that binds to albumin and compete with BCP thus causing temporarily low results.
Reflection
Ligand macromolecule binding is a ubiquitous occurrence of medical importance to numerous
disciplines of Science for example; pharmacology, endocrinology, enzymology, clinical
chemistry and protein chemistry. Albumin can be investigated in biological fluids using methods
such as radioimmunoassay, electro immunoassay, immune cephalometric and radial
immunoassay.
These methods when used are very specific and highly sensitive. However, these methods are not
recommended for routine use because they are very slow, expensive and very difficult to
automate. In clinical chemistry labs, albumin is mostly measured using dye-binding techniques
such as BCP and BCG. However, BCG is mostly used because of its strong binding to other
serum proteins other than albumin. BCP only binds with albumin ligand and is highly specific.
These experiments acted as an eye opener to us as far as BCG and BCP debate is concerned.
BCP results with albumin gives moderately lower values when compared with BCG. The results
however correlate well with specific immunological assays.
d) What is the effect of heparin on albumin levels measured by both methods?
Heparin boosts the level of albumin in the samples. Since BCP is more specific it’s readings
would not be much affected but BCG readings would be elevated since the concentration of the
albumin is increased.
Heparin would only BCG readings since and not BCP because BCP is more specific to globulin
e) Which method can be adapted to account for the potential interference by heparin?
Bromocresol purple method.
f) Which pathophysiological circumstances lead to albumin being underestimated by the BCP
assay?
Renal failure in patients who are undergoing hemodialysis care in hospitals. This because of a
uremic toxin that binds to albumin and compete with BCP thus causing temporarily low results.
Reflection
Ligand macromolecule binding is a ubiquitous occurrence of medical importance to numerous
disciplines of Science for example; pharmacology, endocrinology, enzymology, clinical
chemistry and protein chemistry. Albumin can be investigated in biological fluids using methods
such as radioimmunoassay, electro immunoassay, immune cephalometric and radial
immunoassay.
These methods when used are very specific and highly sensitive. However, these methods are not
recommended for routine use because they are very slow, expensive and very difficult to
automate. In clinical chemistry labs, albumin is mostly measured using dye-binding techniques
such as BCP and BCG. However, BCG is mostly used because of its strong binding to other
serum proteins other than albumin. BCP only binds with albumin ligand and is highly specific.
These experiments acted as an eye opener to us as far as BCG and BCP debate is concerned.
BCP results with albumin gives moderately lower values when compared with BCG. The results
however correlate well with specific immunological assays.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

REPORT 10
When heparin concentration is increased, the concentration of albumin is apparently increased.
Consequently, precipitate is formed that may remain in the solution as a suspension if heparin is
continuously added. Addition of heparin increases the concentration of albumin in the serum
samples. When concentration of serum is increased BCG readings are affected but not BCP
readings. This is because BCP readings are more specific to binding with the albumin. This
experiment had to be carried out with a lot of care because human blood is deemed to be very
infectious.
When heparin concentration is increased, the concentration of albumin is apparently increased.
Consequently, precipitate is formed that may remain in the solution as a suspension if heparin is
continuously added. Addition of heparin increases the concentration of albumin in the serum
samples. When concentration of serum is increased BCG readings are affected but not BCP
readings. This is because BCP readings are more specific to binding with the albumin. This
experiment had to be carried out with a lot of care because human blood is deemed to be very
infectious.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REPORT 11
References
Bartholomew R.J. & Delaney A., (1964). Spectrophotometric studies and analytical application
of the protein error of some pH indicators. Proc Aust Assoc Clin Biochem, 1, 64- 67.
Carter P. (1970). Ultramicroestimation of human serum albumin: binding of the cationic dye 5,
5’dibromo-o-cresolsulfonphthalein. Microchem J, 15, 4, 531-539.
Doumas B.T & Peters T. (1997). Serum and urine albumin: a progress report on their
measurement and clinical significance. Clinica Chimica Acta, 258, 3-20
Doumas B.T., Watson W.A. & Biggs H.G. (1971). Albumin standards and the measurement of
serum albumin with bromcresol green. Clinica Chimica Acta, 31, 87-96.
Louderback A., & Mealy E.H. & Tayor N.A. (1968). A new dye-binding technique using
bromcresol purple for determination of albumin in serum. Clin Chem, 14, 793-794.
Pinnell A.E. & Northam B.E. (1978). New automated dye-binding method for serum albumin
determination with bromcresol purple. Clin Chem, 24, 80-86.
Rodkey F.L. (1965). Direct spectrophotometric determination of albumin in human serum. Clin
Chem, 11, 478-487
References
Bartholomew R.J. & Delaney A., (1964). Spectrophotometric studies and analytical application
of the protein error of some pH indicators. Proc Aust Assoc Clin Biochem, 1, 64- 67.
Carter P. (1970). Ultramicroestimation of human serum albumin: binding of the cationic dye 5,
5’dibromo-o-cresolsulfonphthalein. Microchem J, 15, 4, 531-539.
Doumas B.T & Peters T. (1997). Serum and urine albumin: a progress report on their
measurement and clinical significance. Clinica Chimica Acta, 258, 3-20
Doumas B.T., Watson W.A. & Biggs H.G. (1971). Albumin standards and the measurement of
serum albumin with bromcresol green. Clinica Chimica Acta, 31, 87-96.
Louderback A., & Mealy E.H. & Tayor N.A. (1968). A new dye-binding technique using
bromcresol purple for determination of albumin in serum. Clin Chem, 14, 793-794.
Pinnell A.E. & Northam B.E. (1978). New automated dye-binding method for serum albumin
determination with bromcresol purple. Clin Chem, 24, 80-86.
Rodkey F.L. (1965). Direct spectrophotometric determination of albumin in human serum. Clin
Chem, 11, 478-487
1 out of 11
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.