Burnout Prevalence and Determinants in Emergency Nurses: Review
VerifiedAdded on 2023/04/17
|13
|11465
|250
Literature Review
AI Summary
This literature review, published in the International Journal of Nursing Studies, systematically examines the prevalence and determinants of burnout in emergency nurses. The review analyzed seventeen studies published between 1989 and 2014, revealing that an average of 26% of emergency nurses experience burnout. The study identifies both individual factors, such as demographic variables, personality characteristics, and coping strategies, and work-related factors, including exposure to traumatic events, job characteristics, and organizational variables, as significant predictors of burnout. Key determinants include job demands, job control, social support, and exposure to traumatic events. The review highlights the high burnout rates in this population and formulates specific action targets for hospital management to prevent turnover and burnout, emphasizing the need for interventions addressing these identified factors. The review underscores the importance of understanding and mitigating burnout within this high-stress healthcare environment, offering insights into potential interventions and management strategies.
Review
Determinantsand prevalenceof burnout in emergency
nurses: A systematicreview of 25 years of research
Jef Adriaenssensa,
*, Ve´ronique De Guchtb
, Stan Maesc
a LeidenUniversity,Instituteof PsychologyHealthPsychology,PO Box 9555,2300 RB Leiden,The Netherlands
b LeidenUniversity,Instituteof PsychologyHealthPsychology,2300 RB Leiden,The Netherlands
c LeidenUniversity,Instituteof Psychologyand LeidenUniversityMedicalCenterHealthPsychology,2300RB Leiden,The Netherlands
Contributions of the paper Burnout has important consequencesfor the health care
InternationalJournal of Nursing Studiesxxx (2014) xxx–xxx
A R T I C L E I N F O
Articlehistory:
Received12 April 2014
Receivedin revisedform 24 October2014
Accepted4 November2014
Keywords:
Burnout
Emergencynursing
Literaturereview
Occupationalstress
Work characteristics
A B S T R A C T
Background:Burnoutis an importantproblemin healthcareprofessionalsand is associated
with a decreasein occupationalwell-being and an increasein absenteeism,turnover and
illness.Nursesarefoundto be vulnerableto burnout,but emergencynursesareevenmoreso,
sinceemergencynursingis characterizedby unpredictability,overcrowdingand continuous
confrontationwith a broad rangeof diseases,injuries and traumaticevents.
Objectives:This systematic review aims (1) to explore the prevalence of burnout in
emergencynurses and (2) to identify specific(individual and work related)determinants
of burnout in this population.
Method: A systematicreview of empirical quantitativestudies on burnout in emergency
nurses, published in English between 1989 and 2014.
Data sources:The databasesNCBI PubMed, Embase, ISI Web of Knowledge, Informa
HealthCare,Picarta, Cinahl and Scielo were searched.
Results:Seventeenstudieswere included in this review.On average26%of the emergency
nurses suffered from burnout. Individual factors such as demographic variables,
personality characteristics and coping strategies were predictive of burnout. Work
relatedfactorssuch as exposureto traumaticevents,job characteristicsand organizational
variableswere also found to be determinantsof burnout in this population.
Conclusions:Burnout ratesin emergencynursesare high. Job demands,job control, social
support and exposureto traumaticeventsare determinantsof burnout, as well as several
organizationalvariables.As a consequencespecific action targets for hospital manage-
ment are formulated to prevent turnover and burnout in emergencynurses.
ß 2014 Elsevier Ltd. All rights reserved.
G Model
NS-2472;No. of Pages13
Contents lists available at ScienceDirect
InternationalJournal of Nursing Studies
journal homepage: www.elsevier.com/ijns
Determinantsand prevalenceof burnout in emergency
nurses: A systematicreview of 25 years of research
Jef Adriaenssensa,
*, Ve´ronique De Guchtb
, Stan Maesc
a LeidenUniversity,Instituteof PsychologyHealthPsychology,PO Box 9555,2300 RB Leiden,The Netherlands
b LeidenUniversity,Instituteof PsychologyHealthPsychology,2300 RB Leiden,The Netherlands
c LeidenUniversity,Instituteof Psychologyand LeidenUniversityMedicalCenterHealthPsychology,2300RB Leiden,The Netherlands
Contributions of the paper Burnout has important consequencesfor the health care
InternationalJournal of Nursing Studiesxxx (2014) xxx–xxx
A R T I C L E I N F O
Articlehistory:
Received12 April 2014
Receivedin revisedform 24 October2014
Accepted4 November2014
Keywords:
Burnout
Emergencynursing
Literaturereview
Occupationalstress
Work characteristics
A B S T R A C T
Background:Burnoutis an importantproblemin healthcareprofessionalsand is associated
with a decreasein occupationalwell-being and an increasein absenteeism,turnover and
illness.Nursesarefoundto be vulnerableto burnout,but emergencynursesareevenmoreso,
sinceemergencynursingis characterizedby unpredictability,overcrowdingand continuous
confrontationwith a broad rangeof diseases,injuries and traumaticevents.
Objectives:This systematic review aims (1) to explore the prevalence of burnout in
emergencynurses and (2) to identify specific(individual and work related)determinants
of burnout in this population.
Method: A systematicreview of empirical quantitativestudies on burnout in emergency
nurses, published in English between 1989 and 2014.
Data sources:The databasesNCBI PubMed, Embase, ISI Web of Knowledge, Informa
HealthCare,Picarta, Cinahl and Scielo were searched.
Results:Seventeenstudieswere included in this review.On average26%of the emergency
nurses suffered from burnout. Individual factors such as demographic variables,
personality characteristics and coping strategies were predictive of burnout. Work
relatedfactorssuch as exposureto traumaticevents,job characteristicsand organizational
variableswere also found to be determinantsof burnout in this population.
Conclusions:Burnout ratesin emergencynursesare high. Job demands,job control, social
support and exposureto traumaticeventsare determinantsof burnout, as well as several
organizationalvariables.As a consequencespecific action targets for hospital manage-
ment are formulated to prevent turnover and burnout in emergencynurses.
ß 2014 Elsevier Ltd. All rights reserved.
G Model
NS-2472;No. of Pages13
Contents lists available at ScienceDirect
InternationalJournal of Nursing Studies
journal homepage: www.elsevier.com/ijns
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
A broad set of predictors for burnout in emergency
nurses was described: demographic and personality
characteristics,coping strategies,exposureto traumatic
events,job characteristicsand organizationalfactors.
Level of professionalautonomy,team spirit and social
support,quality of leadership,and frequencyof exposure
to traumaticeventswere found to be strongpredictorsof
burnout in emergencynurses.
1. Introduction
Severalstudies show that a positive experienceof the
work environment(low strain) is relatedto work engage-
ment and professional commitment, while a negative
perception(high strain) is relatedto a stateof depletionof
resources,called ‘burnout’(Ahola et al., 2009).In the early
’70sof the last century,Freudenbergerdefinedburnout as
‘the extinctionof motivationor incentive,especiallywhere
one’sdevotionto a causeor relationshipfails to producethe
desired results’ (Freudenberger, 1974). Shortly after,
Christina Maslach defined burnout as a psychological
stateresultingfrom prolongedemotionalor psychological
stresson the job (Maslach and Jackson,1981a,b;Maslach
et al.,2001).Maslachseesburnoutas an internalemotional
reaction (illness) caused by external factors, resulting in
loss of personal and/or social resources: ‘Burnoutis the
indexof the dislocationbetweenwhat peopleare and what
theyhaveto do.It representserosionin values,dignity,spirit,
and will—an erosionof the human soul. It’s a maladythat
spreadsgraduallyand continuouslyovertime,puttingpeople
into a downward spiral from which it’s hard to recover’
(Maslach and Leiter, 1997).
Burnout,as defined by Maslach,has three dimensions.
The first dimensionof the burnoutsyndromeis ‘‘emotional
exhaustion’’.When the emotional reservesare depleted,
employeesfeel that they are no longerableto providework
of good quality. They have feelingsof extremeenergyloss
and a senseof being completelydrained out of emotional
and physicalstrength(Maslachand Jackson,1981a,b).The
second dimension ‘‘depersonalization’’is defined as the
developmentof negativeattitudes,such as cynicism and
negativism,both in thinking as well as in behavior, in
which coworkers and service recipients are approached
with derogatory prejudices and treated accordingly
(Maslach and Jackson,1981a,b).The third aspectis ‘‘lack
of personal accomplishment’’.This is defined as lack of
feelingsregardingboth job and personalcompetenceand
2011). Finally, burnout can also lead to a significant
economic loss through increased absenteeism,higher
turnover rates and a rise in health care costs (Borritz
et al., 2006).
The prevalenceof burnout, assessedby use of a self-
report instrument in a general working population in
Western countries, ranges from 13% to 27% (Norlund
et al., 2010; Lindblom et al., 2006; Kant et al., 2004;
Houtmanet al., 2000;Aromaaand Koskinen,2004).Nurses
are known to be at higher risk for the developmentof
burnout then other occupations(Maslach,2003; Gelsema
et al., 2006). Researchshowed that nurses indeed report
high levels of work relatedstress(Hasselhornet al., 2003;
Smith et al., 2000; Clegg,2001; McVicar, 2003) and that
30%to 50%reach clinical levels of burnout (Aiken et al.,
2002; Poncetet al., 2007; Gelsemaet al., 2006).According
to severalauthors,the demandsthat burdenthe nurses(in
terms of work setting, task description, responsibility,
unpredictabilityand the exposureto potentiallytraumatic
situations)and the resourcesthey can rely on, are strongly
related to the content of their job and their nursing
specialty(Browninget al.,2007;Ergunet al.,2005;Eriksen,
2006; Kipping, 2000; Mealer et al., 2007).Emergency(ER)
nursing is a specialty that differs from other nursing
specialties: work in emergency departments is hectic,
unpredictable and constantly changing. ER-nurses are
confrontedwith a very broad range of diseases,injuries
and problems.Moreover,due to the hecticwork conditions
and overcrowding,emergencynurses often have to move
from one urgencyto another,with oftenlittle recoverytime
(Alexander and Klein, 2001; Gates et al., 2011). As a
consequence,rates of burnout are found to be very high in
emergencynursing settings (Hooper et al., 2010; Potter,
2006).
2. The review
2.1. Aim
The aim of the presentreview is (1) to examinethe level
of burnout in ER-nurses and (2) to identify specific
determinantsof burnout in thesenurses,includingvarious
individual and work-related factors.
2.2. Searchmethods
The databases NCBI PubMed, Embase, ISI Web of
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx2
nurses was described: demographic and personality
characteristics,coping strategies,exposureto traumatic
events,job characteristicsand organizationalfactors.
Level of professionalautonomy,team spirit and social
support,quality of leadership,and frequencyof exposure
to traumaticeventswere found to be strongpredictorsof
burnout in emergencynurses.
1. Introduction
Severalstudies show that a positive experienceof the
work environment(low strain) is relatedto work engage-
ment and professional commitment, while a negative
perception(high strain) is relatedto a stateof depletionof
resources,called ‘burnout’(Ahola et al., 2009).In the early
’70sof the last century,Freudenbergerdefinedburnout as
‘the extinctionof motivationor incentive,especiallywhere
one’sdevotionto a causeor relationshipfails to producethe
desired results’ (Freudenberger, 1974). Shortly after,
Christina Maslach defined burnout as a psychological
stateresultingfrom prolongedemotionalor psychological
stresson the job (Maslach and Jackson,1981a,b;Maslach
et al.,2001).Maslachseesburnoutas an internalemotional
reaction (illness) caused by external factors, resulting in
loss of personal and/or social resources: ‘Burnoutis the
indexof the dislocationbetweenwhat peopleare and what
theyhaveto do.It representserosionin values,dignity,spirit,
and will—an erosionof the human soul. It’s a maladythat
spreadsgraduallyand continuouslyovertime,puttingpeople
into a downward spiral from which it’s hard to recover’
(Maslach and Leiter, 1997).
Burnout,as defined by Maslach,has three dimensions.
The first dimensionof the burnoutsyndromeis ‘‘emotional
exhaustion’’.When the emotional reservesare depleted,
employeesfeel that they are no longerableto providework
of good quality. They have feelingsof extremeenergyloss
and a senseof being completelydrained out of emotional
and physicalstrength(Maslachand Jackson,1981a,b).The
second dimension ‘‘depersonalization’’is defined as the
developmentof negativeattitudes,such as cynicism and
negativism,both in thinking as well as in behavior, in
which coworkers and service recipients are approached
with derogatory prejudices and treated accordingly
(Maslach and Jackson,1981a,b).The third aspectis ‘‘lack
of personal accomplishment’’.This is defined as lack of
feelingsregardingboth job and personalcompetenceand
2011). Finally, burnout can also lead to a significant
economic loss through increased absenteeism,higher
turnover rates and a rise in health care costs (Borritz
et al., 2006).
The prevalenceof burnout, assessedby use of a self-
report instrument in a general working population in
Western countries, ranges from 13% to 27% (Norlund
et al., 2010; Lindblom et al., 2006; Kant et al., 2004;
Houtmanet al., 2000;Aromaaand Koskinen,2004).Nurses
are known to be at higher risk for the developmentof
burnout then other occupations(Maslach,2003; Gelsema
et al., 2006). Researchshowed that nurses indeed report
high levels of work relatedstress(Hasselhornet al., 2003;
Smith et al., 2000; Clegg,2001; McVicar, 2003) and that
30%to 50%reach clinical levels of burnout (Aiken et al.,
2002; Poncetet al., 2007; Gelsemaet al., 2006).According
to severalauthors,the demandsthat burdenthe nurses(in
terms of work setting, task description, responsibility,
unpredictabilityand the exposureto potentiallytraumatic
situations)and the resourcesthey can rely on, are strongly
related to the content of their job and their nursing
specialty(Browninget al.,2007;Ergunet al.,2005;Eriksen,
2006; Kipping, 2000; Mealer et al., 2007).Emergency(ER)
nursing is a specialty that differs from other nursing
specialties: work in emergency departments is hectic,
unpredictable and constantly changing. ER-nurses are
confrontedwith a very broad range of diseases,injuries
and problems.Moreover,due to the hecticwork conditions
and overcrowding,emergencynurses often have to move
from one urgencyto another,with oftenlittle recoverytime
(Alexander and Klein, 2001; Gates et al., 2011). As a
consequence,rates of burnout are found to be very high in
emergencynursing settings (Hooper et al., 2010; Potter,
2006).
2. The review
2.1. Aim
The aim of the presentreview is (1) to examinethe level
of burnout in ER-nurses and (2) to identify specific
determinantsof burnout in thesenurses,includingvarious
individual and work-related factors.
2.2. Searchmethods
The databases NCBI PubMed, Embase, ISI Web of
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx2
‘‘Nurses’’[Mesh],nursing staff, health professional,para-
medic, medical staff, critical incident, critical event,
traumatic event, predictor, determinant. The primary
outcome key words were burnout, exhaustion, fatigue,
‘‘Burnout, Professional’’[Mesh] and M.B.I. but also the
secondary outcomes job satisfaction, turnover, mental
health, occupationalhealth, anxiety,depression,somatic,
post-traumaticstress,secondarytraumatic stress,‘‘Stress
Disorders,Post-Traumatic’’[Mesh], PTSD and P.T.S.Dwere
taken into account.
Studieswere includedonly if the following criteriawere
met: the respondentsunder study (N 40) were nurses,
and a well-defined part of the respondentsworked in an
emergencyunit or in ambulancecare,(2) the focus of the
study had to be on determinants/predictorsof burnout,
(3) the study had to be empirical and quantitative and
(4) the responserate was higher than 25%.
2.3. Searchoutcome
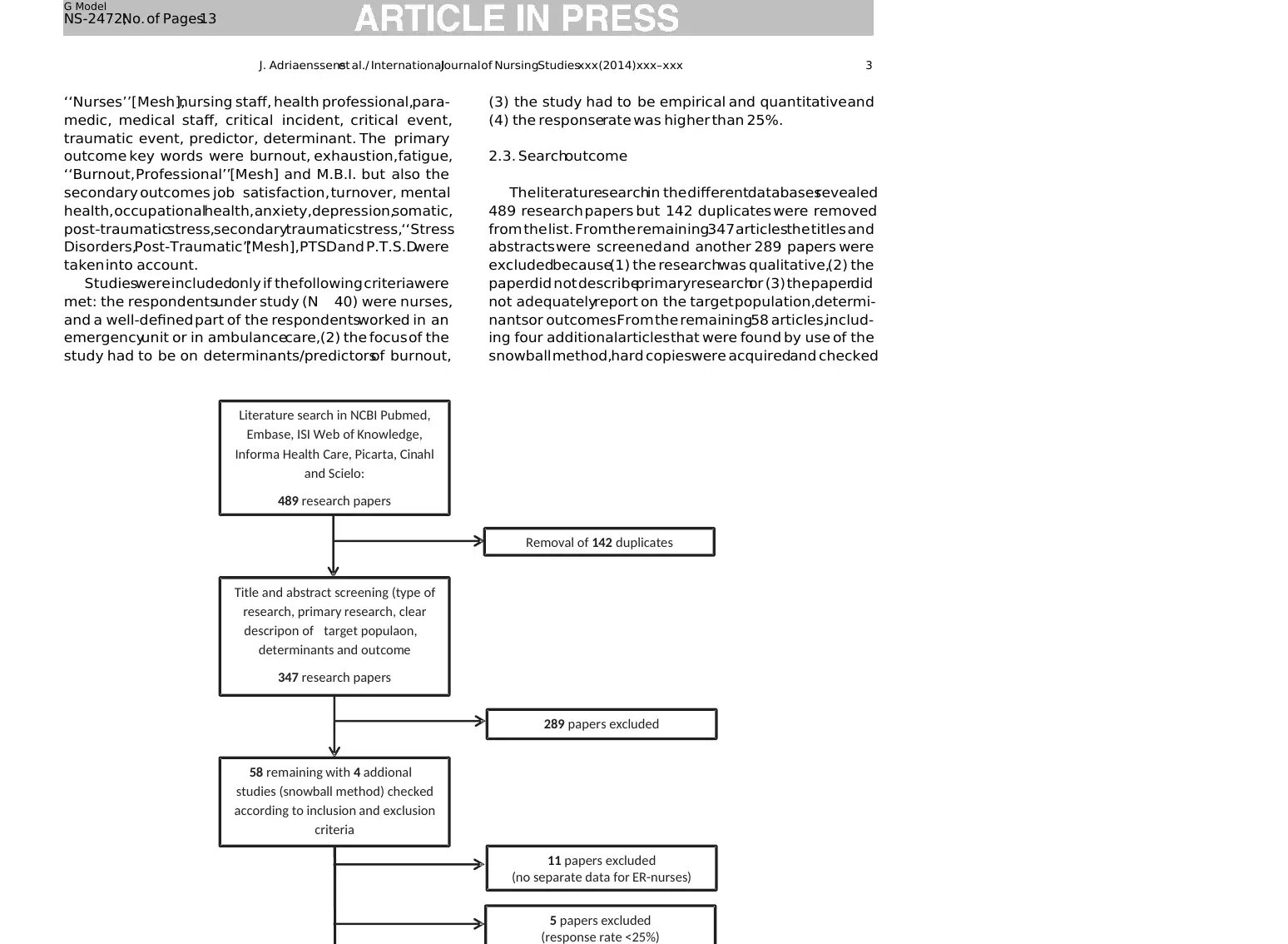
The literaturesearchin the differentdatabasesrevealed
489 research papers but 142 duplicates were removed
from the list. From the remaining347 articlesthe titles and
abstracts were screened and another 289 papers were
excludedbecause(1) the researchwas qualitative,(2) the
paperdid not describeprimaryresearchor (3) the paperdid
not adequatelyreport on the target population,determi-
nantsor outcomes.From the remaining58 articles,includ-
ing four additional articles that were found by use of the
snowball method,hard copieswere acquiredand checked
Literature search in NCBI Pubmed,
Embase, ISI Web of Knowledge,
Informa Health Care, Picarta, Cinahl
and Scielo:
489 research papers
Title and abstract screening (type of
research, primary research, clear
descripon of target populaon,
determinants and outcome
347 research papers
Removal of 142 duplicates
289 papers excluded
58 remaining with 4 addional
studies (snowball method) checked
according to inclusion and exclusion
criteria
11 papers excluded
(no separate data for ER-nurses)
5 papers excluded
(response rate <25%)
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 3
medic, medical staff, critical incident, critical event,
traumatic event, predictor, determinant. The primary
outcome key words were burnout, exhaustion, fatigue,
‘‘Burnout, Professional’’[Mesh] and M.B.I. but also the
secondary outcomes job satisfaction, turnover, mental
health, occupationalhealth, anxiety,depression,somatic,
post-traumaticstress,secondarytraumatic stress,‘‘Stress
Disorders,Post-Traumatic’’[Mesh], PTSD and P.T.S.Dwere
taken into account.
Studieswere includedonly if the following criteriawere
met: the respondentsunder study (N 40) were nurses,
and a well-defined part of the respondentsworked in an
emergencyunit or in ambulancecare,(2) the focus of the
study had to be on determinants/predictorsof burnout,
(3) the study had to be empirical and quantitative and
(4) the responserate was higher than 25%.
2.3. Searchoutcome
The literaturesearchin the differentdatabasesrevealed
489 research papers but 142 duplicates were removed
from the list. From the remaining347 articlesthe titles and
abstracts were screened and another 289 papers were
excludedbecause(1) the researchwas qualitative,(2) the
paperdid not describeprimaryresearchor (3) the paperdid
not adequatelyreport on the target population,determi-
nantsor outcomes.From the remaining58 articles,includ-
ing four additional articles that were found by use of the
snowball method,hard copieswere acquiredand checked
Literature search in NCBI Pubmed,
Embase, ISI Web of Knowledge,
Informa Health Care, Picarta, Cinahl
and Scielo:
489 research papers
Title and abstract screening (type of
research, primary research, clear
descripon of target populaon,
determinants and outcome
347 research papers
Removal of 142 duplicates
289 papers excluded
58 remaining with 4 addional
studies (snowball method) checked
according to inclusion and exclusion
criteria
11 papers excluded
(no separate data for ER-nurses)
5 papers excluded
(response rate <25%)
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
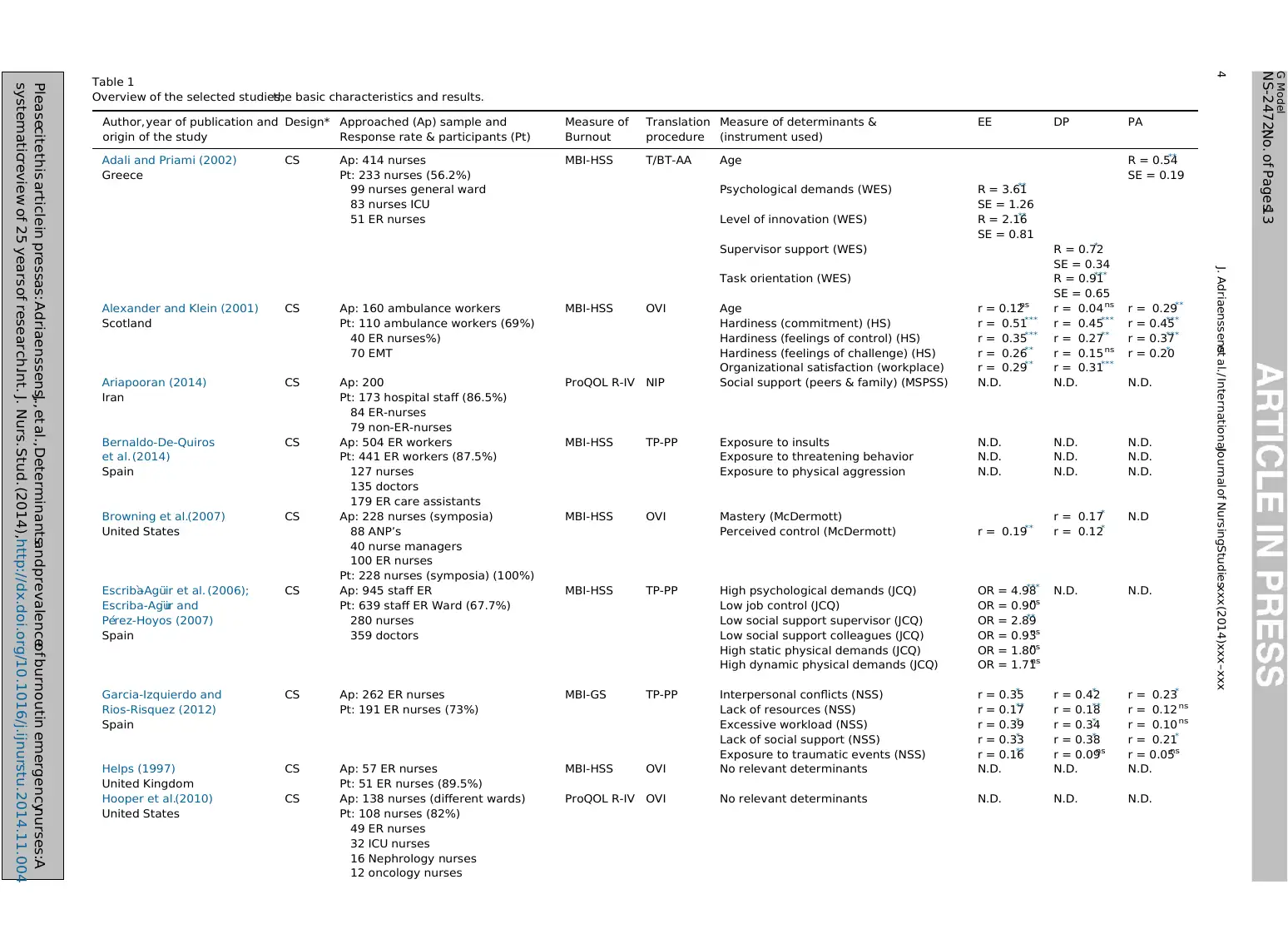
Table 1
Overview of the selected studies,the basic characteristics and results.
Author,year of publication and
origin of the study
Design* Approached (Ap) sample and
Response rate & participants (Pt)
Measure of
Burnout
Translation
procedure
Measure of determinants &
(instrument used)
EE DP PA
Adali and Priami (2002)
Greece
CS Ap: 414 nurses
Pt: 233 nurses (56.2%)
99 nurses general ward
83 nurses ICU
51 ER nurses
MBI-HSS T/BT-AA Age R = 0.54**
SE = 0.19
Psychological demands (WES) R = 3.61**
SE = 1.26
Level of innovation (WES) R = 2.16**
SE = 0.81
Supervisor support (WES) R = 0.72*
SE = 0.34
Task orientation (WES) R = 0.91***
SE = 0.65
Alexander and Klein (2001)
Scotland
CS Ap: 160 ambulance workers
Pt: 110 ambulance workers (69%)
40 ER nurses%)
70 EMT
MBI-HSS OVI Age
Hardiness (commitment) (HS)
Hardiness (feelings of control) (HS)
Hardiness (feelings of challenge) (HS)
Organizational satisfaction (workplace)
r = 0.12ns
r = 0.51***
r = 0.35***
r = 0.26**
r = 0.29**
r = 0.04 ns
r = 0.45***
r = 0.27**
r = 0.15 ns
r = 0.31***
r = 0.29**
r = 0.45***
r = 0.37***
r = 0.20*
Ariapooran (2014)
Iran
CS Ap: 200
Pt: 173 hospital staff (86.5%)
84 ER-nurses
79 non-ER-nurses
ProQOL R-IV NIP Social support (peers & family) (MSPSS) N.D. N.D. N.D.
Bernaldo-De-Quiros
et al. (2014)
Spain
CS Ap: 504 ER workers
Pt: 441 ER workers (87.5%)
127 nurses
135 doctors
179 ER care assistants
MBI-HSS TP-PP Exposure to insults
Exposure to threatening behavior
Exposure to physical aggression
N.D.
N.D.
N.D.
N.D.
N.D.
N.D.
N.D.
N.D.
N.D.
Browning et al.(2007)
United States
CS Ap: 228 nurses (symposia)
88 ANP’s
40 nurse managers
100 ER nurses
Pt: 228 nurses (symposia) (100%)
MBI-HSS OVI Mastery (McDermott) r = 0.17*
r = 0.12*
N.D
Perceived control (McDermott) r = 0.19**
Escriba`-Agu¨ir et al. (2006);
Escriba-Agu¨ir and
Pe´rez-Hoyos (2007)
Spain
CS Ap: 945 staff ER
Pt: 639 staff ER Ward (67.7%)
280 nurses
359 doctors
MBI-HSS TP-PP High psychological demands (JCQ)
Low job control (JCQ)
Low social support supervisor (JCQ)
Low social support colleagues (JCQ)
High static physical demands (JCQ)
High dynamic physical demands (JCQ)
OR = 4.98***
OR = 0.90ns
OR = 2.89**
OR = 0.93ns
OR = 1.80ns
OR = 1.71ns
N.D. N.D.
Garcia-Izquierdo and
Rios-Risquez (2012)
Spain
CS Ap: 262 ER nurses
Pt: 191 ER nurses (73%)
MBI-GS TP-PP Interpersonal conflicts (NSS)
Lack of resources (NSS)
Excessive workload (NSS)
Lack of social support (NSS)
Exposure to traumatic events (NSS)
r = 0.35*
r = 0.17**
r = 0.39*
r = 0.33*
r = 0.16**
r = 0.42*
r = 0.18**
r = 0.34*
r = 0.38*
r = 0.09ns
r = 0.23*
r = 0.12 ns
r = 0.10 ns
r = 0.21*
r = 0.05ns
Helps (1997)
United Kingdom
CS Ap: 57 ER nurses
Pt: 51 ER nurses (89.5%)
MBI-HSS OVI No relevant determinants N.D. N.D. N.D.
Hooper et al.(2010)
United States
CS Ap: 138 nurses (different wards)
Pt: 108 nurses (82%)
49 ER nurses
32 ICU nurses
16 Nephrology nurses
12 oncology nurses
ProQOL R-IV OVI No relevant determinants N.D. N.D. N.D.
G Model
NS-2472;No. of Pages13
Pleasecite this article in pressas: Adriaenssens,J., et al.,Determinantsand prevalenceof burnoutin emergencynurses:A
systematicreview of 25 years of research.Int. J. Nurs. Stud. (2014),http://dx.doi.org/10.1016/j.ijnurstu.2014.11.004
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx4
Overview of the selected studies,the basic characteristics and results.
Author,year of publication and
origin of the study
Design* Approached (Ap) sample and
Response rate & participants (Pt)
Measure of
Burnout
Translation
procedure
Measure of determinants &
(instrument used)
EE DP PA
Adali and Priami (2002)
Greece
CS Ap: 414 nurses
Pt: 233 nurses (56.2%)
99 nurses general ward
83 nurses ICU
51 ER nurses
MBI-HSS T/BT-AA Age R = 0.54**
SE = 0.19
Psychological demands (WES) R = 3.61**
SE = 1.26
Level of innovation (WES) R = 2.16**
SE = 0.81
Supervisor support (WES) R = 0.72*
SE = 0.34
Task orientation (WES) R = 0.91***
SE = 0.65
Alexander and Klein (2001)
Scotland
CS Ap: 160 ambulance workers
Pt: 110 ambulance workers (69%)
40 ER nurses%)
70 EMT
MBI-HSS OVI Age
Hardiness (commitment) (HS)
Hardiness (feelings of control) (HS)
Hardiness (feelings of challenge) (HS)
Organizational satisfaction (workplace)
r = 0.12ns
r = 0.51***
r = 0.35***
r = 0.26**
r = 0.29**
r = 0.04 ns
r = 0.45***
r = 0.27**
r = 0.15 ns
r = 0.31***
r = 0.29**
r = 0.45***
r = 0.37***
r = 0.20*
Ariapooran (2014)
Iran
CS Ap: 200
Pt: 173 hospital staff (86.5%)
84 ER-nurses
79 non-ER-nurses
ProQOL R-IV NIP Social support (peers & family) (MSPSS) N.D. N.D. N.D.
Bernaldo-De-Quiros
et al. (2014)
Spain
CS Ap: 504 ER workers
Pt: 441 ER workers (87.5%)
127 nurses
135 doctors
179 ER care assistants
MBI-HSS TP-PP Exposure to insults
Exposure to threatening behavior
Exposure to physical aggression
N.D.
N.D.
N.D.
N.D.
N.D.
N.D.
N.D.
N.D.
N.D.
Browning et al.(2007)
United States
CS Ap: 228 nurses (symposia)
88 ANP’s
40 nurse managers
100 ER nurses
Pt: 228 nurses (symposia) (100%)
MBI-HSS OVI Mastery (McDermott) r = 0.17*
r = 0.12*
N.D
Perceived control (McDermott) r = 0.19**
Escriba`-Agu¨ir et al. (2006);
Escriba-Agu¨ir and
Pe´rez-Hoyos (2007)
Spain
CS Ap: 945 staff ER
Pt: 639 staff ER Ward (67.7%)
280 nurses
359 doctors
MBI-HSS TP-PP High psychological demands (JCQ)
Low job control (JCQ)
Low social support supervisor (JCQ)
Low social support colleagues (JCQ)
High static physical demands (JCQ)
High dynamic physical demands (JCQ)
OR = 4.98***
OR = 0.90ns
OR = 2.89**
OR = 0.93ns
OR = 1.80ns
OR = 1.71ns
N.D. N.D.
Garcia-Izquierdo and
Rios-Risquez (2012)
Spain
CS Ap: 262 ER nurses
Pt: 191 ER nurses (73%)
MBI-GS TP-PP Interpersonal conflicts (NSS)
Lack of resources (NSS)
Excessive workload (NSS)
Lack of social support (NSS)
Exposure to traumatic events (NSS)
r = 0.35*
r = 0.17**
r = 0.39*
r = 0.33*
r = 0.16**
r = 0.42*
r = 0.18**
r = 0.34*
r = 0.38*
r = 0.09ns
r = 0.23*
r = 0.12 ns
r = 0.10 ns
r = 0.21*
r = 0.05ns
Helps (1997)
United Kingdom
CS Ap: 57 ER nurses
Pt: 51 ER nurses (89.5%)
MBI-HSS OVI No relevant determinants N.D. N.D. N.D.
Hooper et al.(2010)
United States
CS Ap: 138 nurses (different wards)
Pt: 108 nurses (82%)
49 ER nurses
32 ICU nurses
16 Nephrology nurses
12 oncology nurses
ProQOL R-IV OVI No relevant determinants N.D. N.D. N.D.
G Model
NS-2472;No. of Pages13
Pleasecite this article in pressas: Adriaenssens,J., et al.,Determinantsand prevalenceof burnoutin emergencynurses:A
systematicreview of 25 years of research.Int. J. Nurs. Stud. (2014),http://dx.doi.org/10.1016/j.ijnurstu.2014.11.004
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
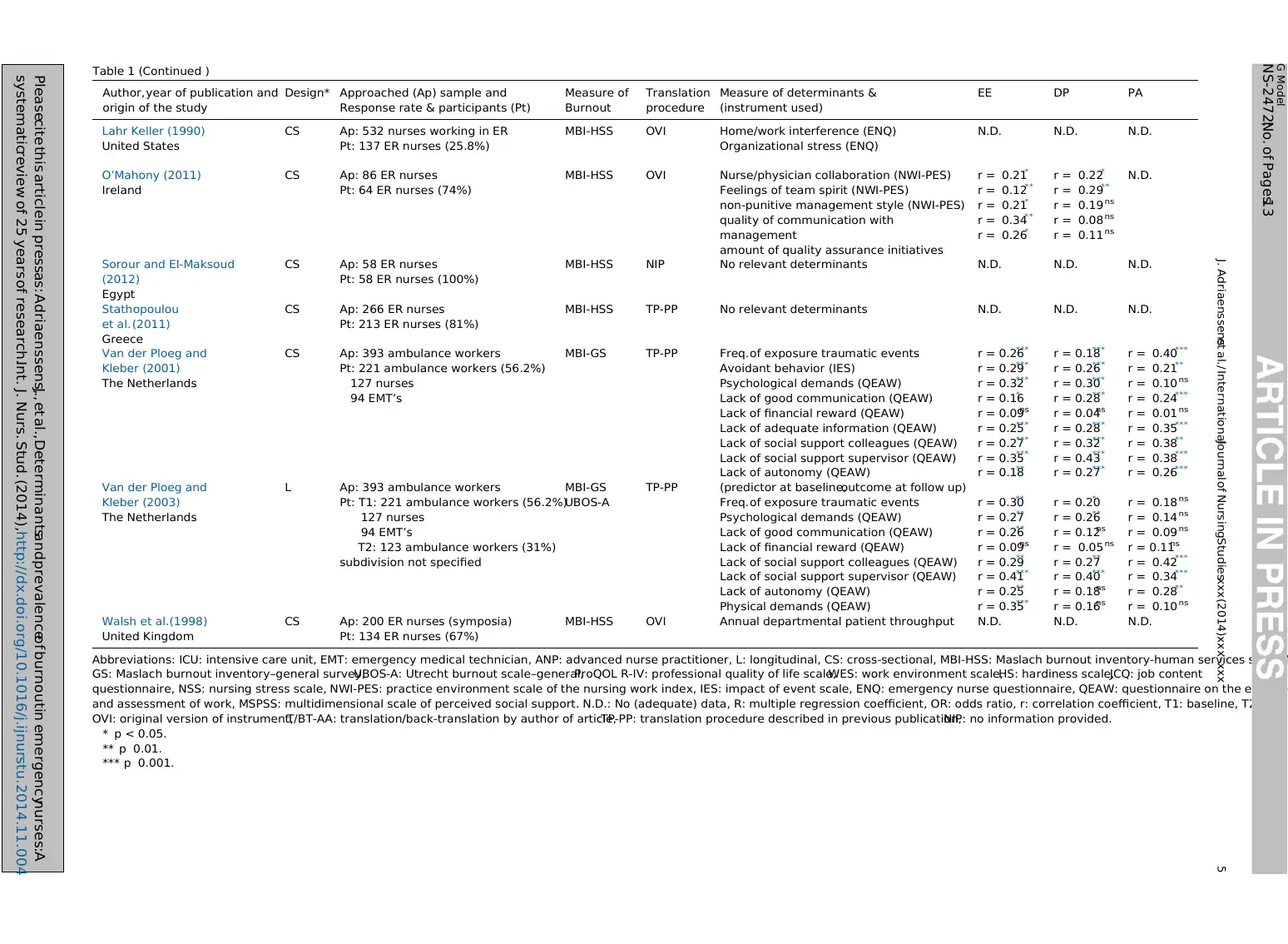
Table 1 (Continued )
Author,year of publication and
origin of the study
Design* Approached (Ap) sample and
Response rate & participants (Pt)
Measure of
Burnout
Translation
procedure
Measure of determinants &
(instrument used)
EE DP PA
Lahr Keller (1990)
United States
CS Ap: 532 nurses working in ER
Pt: 137 ER nurses (25.8%)
MBI-HSS OVI Home/work interference (ENQ)
Organizational stress (ENQ)
N.D. N.D. N.D.
O’Mahony (2011)
Ireland
CS Ap: 86 ER nurses
Pt: 64 ER nurses (74%)
MBI-HSS OVI Nurse/physician collaboration (NWI-PES)
Feelings of team spirit (NWI-PES)
non-punitive management style (NWI-PES)
quality of communication with
management
amount of quality assurance initiatives
r = 0.21*
r = 0.12**
r = 0.21*
r = 0.34**
r = 0.26*
r = 0.22*
r = 0.29**
r = 0.19 ns
r = 0.08 ns
r = 0.11 ns
N.D.
Sorour and El-Maksoud
(2012)
Egypt
CS Ap: 58 ER nurses
Pt: 58 ER nurses (100%)
MBI-HSS NIP No relevant determinants N.D. N.D. N.D.
Stathopoulou
et al. (2011)
Greece
CS Ap: 266 ER nurses
Pt: 213 ER nurses (81%)
MBI-HSS TP-PP No relevant determinants N.D. N.D. N.D.
Van der Ploeg and
Kleber (2001)
The Netherlands
CS Ap: 393 ambulance workers
Pt: 221 ambulance workers (56.2%)
127 nurses
94 EMT’s
MBI-GS TP-PP Freq.of exposure traumatic events
Avoidant behavior (IES)
Psychological demands (QEAW)
Lack of good communication (QEAW)
Lack of financial reward (QEAW)
Lack of adequate information (QEAW)
Lack of social support colleagues (QEAW)
Lack of social support supervisor (QEAW)
Lack of autonomy (QEAW)
r = 0.26***
r = 0.29***
r = 0.32***
r = 0.16*
r = 0.09ns
r = 0.25***
r = 0.27***
r = 0.35***
r = 0.18**
r = 0.18***
r = 0.26***
r = 0.30***
r = 0.28***
r = 0.04ns
r = 0.28***
r = 0.32***
r = 0.43***
r = 0.27***
r = 0.40***
r = 0.21**
r = 0.10 ns
r = 0.24***
r = 0.01 ns
r = 0.35***
r = 0.38**
r = 0.38***
r = 0.26***
Van der Ploeg and
Kleber (2003)
The Netherlands
L Ap: 393 ambulance workers
Pt: T1: 221 ambulance workers (56.2%)
127 nurses
94 EMT’s
T2: 123 ambulance workers (31%)
subdivision not specified
MBI-GS
UBOS-A
TP-PP (predictor at baseline,outcome at follow up)
Freq.of exposure traumatic events
Psychological demands (QEAW)
Lack of good communication (QEAW)
Lack of financial reward (QEAW)
Lack of social support colleagues (QEAW)
Lack of social support supervisor (QEAW)
Lack of autonomy (QEAW)
Physical demands (QEAW)
r = 0.30**
r = 0.27**
r = 0.26**
r = 0.09ns
r = 0.29**
r = 0.41***
r = 0.25**
r = 0.35***
r = 0.20*
r = 0.26**
r = 0.12ns
r = 0.05 ns
r = 0.27**
r = 0.40***
r = 0.18ns
r = 0.16ns
r = 0.18 ns
r = 0.14 ns
r = 0.09 ns
r = 0.11ns
r = 0.42***
r = 0.34***
r = 0.28**
r = 0.10 ns
Walsh et al.(1998)
United Kingdom
CS Ap: 200 ER nurses (symposia)
Pt: 134 ER nurses (67%)
MBI-HSS OVI Annual departmental patient throughput N.D. N.D. N.D.
Abbreviations: ICU: intensive care unit, EMT: emergency medical technician, ANP: advanced nurse practitioner, L: longitudinal, CS: cross-sectional, MBI-HSS: Maslach burnout inventory-human services scale, M
GS: Maslach burnout inventory–general survey,UBOS-A: Utrecht burnout scale–general,ProQOL R-IV: professional quality of life scale,WES: work environment scale,HS: hardiness scale,JCQ: job content
questionnaire, NSS: nursing stress scale, NWI-PES: practice environment scale of the nursing work index, IES: impact of event scale, ENQ: emergency nurse questionnaire, QEAW: questionnaire on the experie
and assessment of work, MSPSS: multidimensional scale of perceived social support. N.D.: No (adequate) data, R: multiple regression coefficient, OR: odds ratio, r: correlation coefficient, T1: baseline, T2: follo
OVI: original version of instrument,T/BT-AA: translation/back-translation by author of article,TP-PP: translation procedure described in previous publication,NIP: no information provided.
* p < 0.05.
** p 0.01.
*** p 0.001.
G Model
NS-2472;No. of Pages13
Pleasecite this article in pressas: Adriaenssens,J., et al.,Determinantsand prevalenceof burnoutin emergencynurses:A
systematicreview of 25 years of research.Int. J. Nurs. Stud. (2014),http://dx.doi.org/10.1016/j.ijnurstu.2014.11.004
J. Adriaenssenset al. / InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 5
Author,year of publication and
origin of the study
Design* Approached (Ap) sample and
Response rate & participants (Pt)
Measure of
Burnout
Translation
procedure
Measure of determinants &
(instrument used)
EE DP PA
Lahr Keller (1990)
United States
CS Ap: 532 nurses working in ER
Pt: 137 ER nurses (25.8%)
MBI-HSS OVI Home/work interference (ENQ)
Organizational stress (ENQ)
N.D. N.D. N.D.
O’Mahony (2011)
Ireland
CS Ap: 86 ER nurses
Pt: 64 ER nurses (74%)
MBI-HSS OVI Nurse/physician collaboration (NWI-PES)
Feelings of team spirit (NWI-PES)
non-punitive management style (NWI-PES)
quality of communication with
management
amount of quality assurance initiatives
r = 0.21*
r = 0.12**
r = 0.21*
r = 0.34**
r = 0.26*
r = 0.22*
r = 0.29**
r = 0.19 ns
r = 0.08 ns
r = 0.11 ns
N.D.
Sorour and El-Maksoud
(2012)
Egypt
CS Ap: 58 ER nurses
Pt: 58 ER nurses (100%)
MBI-HSS NIP No relevant determinants N.D. N.D. N.D.
Stathopoulou
et al. (2011)
Greece
CS Ap: 266 ER nurses
Pt: 213 ER nurses (81%)
MBI-HSS TP-PP No relevant determinants N.D. N.D. N.D.
Van der Ploeg and
Kleber (2001)
The Netherlands
CS Ap: 393 ambulance workers
Pt: 221 ambulance workers (56.2%)
127 nurses
94 EMT’s
MBI-GS TP-PP Freq.of exposure traumatic events
Avoidant behavior (IES)
Psychological demands (QEAW)
Lack of good communication (QEAW)
Lack of financial reward (QEAW)
Lack of adequate information (QEAW)
Lack of social support colleagues (QEAW)
Lack of social support supervisor (QEAW)
Lack of autonomy (QEAW)
r = 0.26***
r = 0.29***
r = 0.32***
r = 0.16*
r = 0.09ns
r = 0.25***
r = 0.27***
r = 0.35***
r = 0.18**
r = 0.18***
r = 0.26***
r = 0.30***
r = 0.28***
r = 0.04ns
r = 0.28***
r = 0.32***
r = 0.43***
r = 0.27***
r = 0.40***
r = 0.21**
r = 0.10 ns
r = 0.24***
r = 0.01 ns
r = 0.35***
r = 0.38**
r = 0.38***
r = 0.26***
Van der Ploeg and
Kleber (2003)
The Netherlands
L Ap: 393 ambulance workers
Pt: T1: 221 ambulance workers (56.2%)
127 nurses
94 EMT’s
T2: 123 ambulance workers (31%)
subdivision not specified
MBI-GS
UBOS-A
TP-PP (predictor at baseline,outcome at follow up)
Freq.of exposure traumatic events
Psychological demands (QEAW)
Lack of good communication (QEAW)
Lack of financial reward (QEAW)
Lack of social support colleagues (QEAW)
Lack of social support supervisor (QEAW)
Lack of autonomy (QEAW)
Physical demands (QEAW)
r = 0.30**
r = 0.27**
r = 0.26**
r = 0.09ns
r = 0.29**
r = 0.41***
r = 0.25**
r = 0.35***
r = 0.20*
r = 0.26**
r = 0.12ns
r = 0.05 ns
r = 0.27**
r = 0.40***
r = 0.18ns
r = 0.16ns
r = 0.18 ns
r = 0.14 ns
r = 0.09 ns
r = 0.11ns
r = 0.42***
r = 0.34***
r = 0.28**
r = 0.10 ns
Walsh et al.(1998)
United Kingdom
CS Ap: 200 ER nurses (symposia)
Pt: 134 ER nurses (67%)
MBI-HSS OVI Annual departmental patient throughput N.D. N.D. N.D.
Abbreviations: ICU: intensive care unit, EMT: emergency medical technician, ANP: advanced nurse practitioner, L: longitudinal, CS: cross-sectional, MBI-HSS: Maslach burnout inventory-human services scale, M
GS: Maslach burnout inventory–general survey,UBOS-A: Utrecht burnout scale–general,ProQOL R-IV: professional quality of life scale,WES: work environment scale,HS: hardiness scale,JCQ: job content
questionnaire, NSS: nursing stress scale, NWI-PES: practice environment scale of the nursing work index, IES: impact of event scale, ENQ: emergency nurse questionnaire, QEAW: questionnaire on the experie
and assessment of work, MSPSS: multidimensional scale of perceived social support. N.D.: No (adequate) data, R: multiple regression coefficient, OR: odds ratio, r: correlation coefficient, T1: baseline, T2: follo
OVI: original version of instrument,T/BT-AA: translation/back-translation by author of article,TP-PP: translation procedure described in previous publication,NIP: no information provided.
* p < 0.05.
** p 0.01.
*** p 0.001.
G Model
NS-2472;No. of Pages13
Pleasecite this article in pressas: Adriaenssens,J., et al.,Determinantsand prevalenceof burnoutin emergencynurses:A
systematicreview of 25 years of research.Int. J. Nurs. Stud. (2014),http://dx.doi.org/10.1016/j.ijnurstu.2014.11.004
J. Adriaenssenset al. / InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 5
accordingto the inclusion and exclusion criteria. Eleven
paperswere excludedbecausetherewere no separatedata
for a subgroupof ER-nursesand five were excludedbecause
the response rates were lower than 25%. One study
(Gillespie and Melby, 2003) was excluded because ER-
nurseswere only a smallsubsample(n =20) of the study,for
which insufficientdatawere provided.From the remaining
41 studies seventeenfocused on burnout as an outcome
measure.Two of these were related to the same study
sample(Escriba`-Agu¨ir et al.,2006;Escriba-Agu¨ir and Pe´rez-
Hoyos,2007)and two studiespresentedcross-sectionaland
longitudinalresultsof the samesample(Van der Ploegand
Kleber, 2001; Van der Ploeg and Kleber, 2003). For the
purposeof this systematicreview,focusingon determinants
of burnout,all 17 remainingstudieswere included(Fig. 1).
Thesecan be found in alphabeticalorder in Table 1.
3. Results
3.1. Studypopulationand studydesign
All of the 17 reviewed studies, except one (Van der
Ploegand Kleber,2003),had a cross-sectionaldesign.Self-
reportquestionnaireswere usedfor everystudy.The initial
samplesizes rangedfrom 57 to 945 respondents(Median:
228) with responseratesvaryingfrom 25.8%to 100%.Most
of the researchersapproachedentire emergencycareunits.
Two authors collected their data at conferences(Walsh
et al.,1998; Browninget al.,2007).The meanpercentageof
female respondentsin the studies was 61.6%(SD 29.7).
Women worked significantly less in ambulanceservices
than in in-hospital emergency services (Mn: 13.8%vs.
77.5%t =6.21 p < .001).One study did not mention gender
nor age of the respondents (Walsh et al., 1998). The
majority of the respondentswere between35 and 40 years
old (range 18 to 67), with the exception of an Egyptian
study that included younger ER-nurses (Sorour and El-
Maksoud, 2012). The majority of the respondentswere
holder of a bachelordegree,and about 7%had a Master’s
degree. The mean seniority of the respondents in the
different studies rangedfrom 6.5 to 13 years.Walsh et al.
(1998) did not mention seniority.
3.2. Globalburnoutscoresof the respondents
Fifteen out of 17 studies used the Maslach Burnout
Inventory to quantify the level of emotional exhaustion,
depersonalizationand lack of personal accomplishment.
Twelvestudiesusedthe MBI for humanservices(MBI-HSS)
(Maslachet al.,1996).Van der Ploegand Kleber (2001)and
Garcia-Izquierdoand Rios-Risquez(2012) both used the
16-item MBI-GS (Schaufeli et al., 1996). The MBI-HSS
primarily focuses on professions,in which contact with
other people is an essentialpart of the work content.The
items explicitly refer to contactswith clients (Taris et al.,
1999).The MBI-GS is an MBI-HSS basedinstrumentfor the
measurementof burnout in non-contactualprofessions.
Severalitems of the GS-versionare identical to the HSS-
version, but for other items the source of the surveyed
feelingsis morerelatedto the contentof the work insteadof
the professionalinterpersonalcontacts(Taris et al., 1999).
Maslach et al. (1997) statethat the MBI-HSS and MBI-HSS
measurethe sameconceptin differentoccupationalgroups,
based on the same theoretical considerations.For the
purpose of the second measurementof the longitudinal
studyby Van der Ploegand Kleber(2003)a 15-itemUBOS-A
was used (Schaufeliand Van Dierendonck,2000).Hooper
et al. (2010) and Ariapooran(2014) used the Professional
Quality of Life: Compassion Satisfaction and Fatigue
Subscales(ProQOLR-IV) (Stamm,2010).This is a 30-item
instrumentusing a 6-point Likert scale(0 =never,5 =very
often).The total score of this instrumentis used to define
burnout,3 sub-scoresare distinguished.
The MBI-HSS cut-off scoresfor mental health workers
(Maslachand Jackson,1986)and for nursesand physicians
(Maslachet al.,1996)can be found in Table2. Cut off points
of the MBI (levels designatedas limits for the different
dimensionsof burnout) were set arbitrary at the 33rd and
66th percentileby Maslachand Jackson(1986).The cut-off
scores for the MBI-GS (Brenninkmeijerand Van Yperen,
Table 2
cut-off scoresfor the MBI-HSS, MBI-GS and UBOS-A for human servicesoccupations.
MBI-HSS Targetrespondents Cut off Normativevalues
Emotional exhaustion Mental Health personnela
Nurses & physiciansb
21
26
Mn(SD) =23.80 (11.80)
a
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx6
paperswere excludedbecausetherewere no separatedata
for a subgroupof ER-nursesand five were excludedbecause
the response rates were lower than 25%. One study
(Gillespie and Melby, 2003) was excluded because ER-
nurseswere only a smallsubsample(n =20) of the study,for
which insufficientdatawere provided.From the remaining
41 studies seventeenfocused on burnout as an outcome
measure.Two of these were related to the same study
sample(Escriba`-Agu¨ir et al.,2006;Escriba-Agu¨ir and Pe´rez-
Hoyos,2007)and two studiespresentedcross-sectionaland
longitudinalresultsof the samesample(Van der Ploegand
Kleber, 2001; Van der Ploeg and Kleber, 2003). For the
purposeof this systematicreview,focusingon determinants
of burnout,all 17 remainingstudieswere included(Fig. 1).
Thesecan be found in alphabeticalorder in Table 1.
3. Results
3.1. Studypopulationand studydesign
All of the 17 reviewed studies, except one (Van der
Ploegand Kleber,2003),had a cross-sectionaldesign.Self-
reportquestionnaireswere usedfor everystudy.The initial
samplesizes rangedfrom 57 to 945 respondents(Median:
228) with responseratesvaryingfrom 25.8%to 100%.Most
of the researchersapproachedentire emergencycareunits.
Two authors collected their data at conferences(Walsh
et al.,1998; Browninget al.,2007).The meanpercentageof
female respondentsin the studies was 61.6%(SD 29.7).
Women worked significantly less in ambulanceservices
than in in-hospital emergency services (Mn: 13.8%vs.
77.5%t =6.21 p < .001).One study did not mention gender
nor age of the respondents (Walsh et al., 1998). The
majority of the respondentswere between35 and 40 years
old (range 18 to 67), with the exception of an Egyptian
study that included younger ER-nurses (Sorour and El-
Maksoud, 2012). The majority of the respondentswere
holder of a bachelordegree,and about 7%had a Master’s
degree. The mean seniority of the respondents in the
different studies rangedfrom 6.5 to 13 years.Walsh et al.
(1998) did not mention seniority.
3.2. Globalburnoutscoresof the respondents
Fifteen out of 17 studies used the Maslach Burnout
Inventory to quantify the level of emotional exhaustion,
depersonalizationand lack of personal accomplishment.
Twelvestudiesusedthe MBI for humanservices(MBI-HSS)
(Maslachet al.,1996).Van der Ploegand Kleber (2001)and
Garcia-Izquierdoand Rios-Risquez(2012) both used the
16-item MBI-GS (Schaufeli et al., 1996). The MBI-HSS
primarily focuses on professions,in which contact with
other people is an essentialpart of the work content.The
items explicitly refer to contactswith clients (Taris et al.,
1999).The MBI-GS is an MBI-HSS basedinstrumentfor the
measurementof burnout in non-contactualprofessions.
Severalitems of the GS-versionare identical to the HSS-
version, but for other items the source of the surveyed
feelingsis morerelatedto the contentof the work insteadof
the professionalinterpersonalcontacts(Taris et al., 1999).
Maslach et al. (1997) statethat the MBI-HSS and MBI-HSS
measurethe sameconceptin differentoccupationalgroups,
based on the same theoretical considerations.For the
purpose of the second measurementof the longitudinal
studyby Van der Ploegand Kleber(2003)a 15-itemUBOS-A
was used (Schaufeliand Van Dierendonck,2000).Hooper
et al. (2010) and Ariapooran(2014) used the Professional
Quality of Life: Compassion Satisfaction and Fatigue
Subscales(ProQOLR-IV) (Stamm,2010).This is a 30-item
instrumentusing a 6-point Likert scale(0 =never,5 =very
often).The total score of this instrumentis used to define
burnout,3 sub-scoresare distinguished.
The MBI-HSS cut-off scoresfor mental health workers
(Maslachand Jackson,1986)and for nursesand physicians
(Maslachet al.,1996)can be found in Table2. Cut off points
of the MBI (levels designatedas limits for the different
dimensionsof burnout) were set arbitrary at the 33rd and
66th percentileby Maslachand Jackson(1986).The cut-off
scores for the MBI-GS (Brenninkmeijerand Van Yperen,
Table 2
cut-off scoresfor the MBI-HSS, MBI-GS and UBOS-A for human servicesoccupations.
MBI-HSS Targetrespondents Cut off Normativevalues
Emotional exhaustion Mental Health personnela
Nurses & physiciansb
21
26
Mn(SD) =23.80 (11.80)
a
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
2003), its Dutch version UBOS-A (Schaufeli and Van
Dierendonck,2000) and the ProQOL R-IV (Stamm,2010)
are also describedin Table 2. Normative values (Mn and
SD) for nurses for the MBI-HSS (samplesize 1542 nurses)
were publishedby Schaufeliand Enzmann(1998).Norma-
tive values for MBI-GS and UBOS-A for human services
occupations (sample size 13076 respondents) were
publishedby Schaufeliand Van Dierendonck(2000).Nor-
mative data for the ProQOL R-IV were provided in the
manual of the instrument (Stamm,2010).
The means, SD’s and percentages of caseness for
of Van der Ploeg and Kleber (2001),that used the MBI-GS
and UBOS-A, reported 11.7%,17.7%and 16.3%of respon-
dents exceeding the cut off for emotional exhaustion,
depersonalizationand lack of personal accomplishment,
respectively.Hooper et al. (2010) and Ariapooran (2014)
found 22.4%and 19.2%of respondentswith high levels of
burnout, respectively.
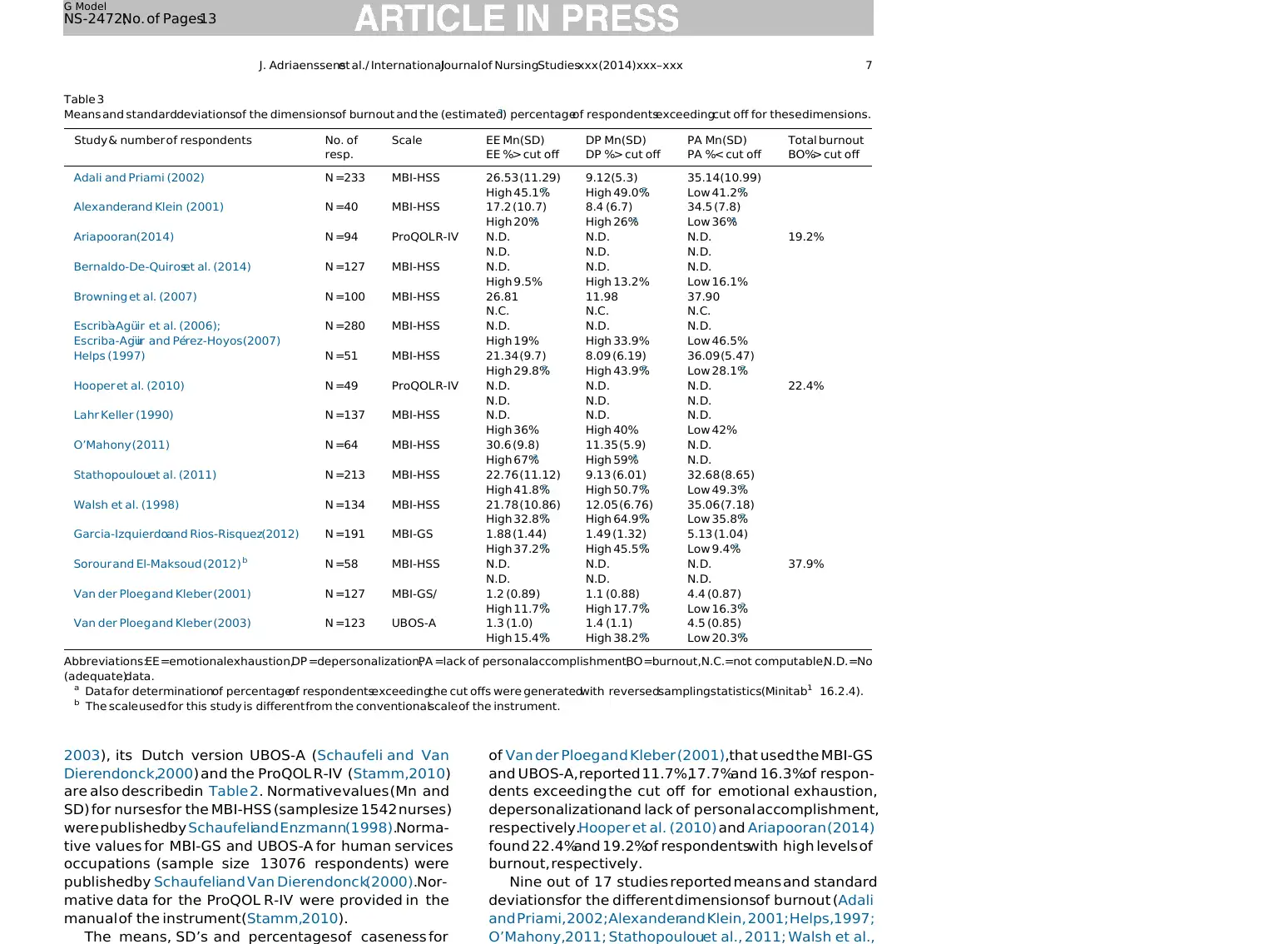
Nine out of 17 studies reported means and standard
deviationsfor the different dimensionsof burnout (Adali
and Priami, 2002; Alexanderand Klein, 2001; Helps,1997;
O’Mahony,2011; Stathopoulouet al., 2011; Walsh et al.,
Table 3
Means and standarddeviationsof the dimensionsof burnout and the (estimateda
) percentageof respondentsexceedingcut off for these dimensions.
Study & number of respondents No. of
resp.
Scale EE Mn(SD)
EE %> cut off
DP Mn(SD)
DP %> cut off
PA Mn(SD)
PA %< cut off
Total burnout
BO%> cut off
Adali and Priami (2002) N =233 MBI-HSS 26.53 (11.29) 9.12(5.3) 35.14(10.99)
High 45.1%a High 49.0%a Low 41.2%a
Alexanderand Klein (2001) N =40 MBI-HSS 17.2 (10.7) 8.4 (6.7) 34.5 (7.8)
High 20%a High 26%a Low 36%a
Ariapooran(2014) N =94 ProQOL R-IV N.D. N.D. N.D. 19.2%
N.D. N.D. N.D.
Bernaldo-De-Quiroset al. (2014) N =127 MBI-HSS N.D. N.D. N.D.
High 9.5% High 13.2% Low 16.1%
Browning et al. (2007) N =100 MBI-HSS 26.81 11.98 37.90
N.C. N.C. N.C.
Escriba`-Agu¨ir et al. (2006);
Escriba-Agu¨ir and Pe´rez-Hoyos (2007)
N =280 MBI-HSS N.D. N.D. N.D.
High 19% High 33.9% Low 46.5%
Helps (1997) N =51 MBI-HSS 21.34 (9.7) 8.09 (6.19) 36.09 (5.47)
High 29.8%a High 43.9%a Low 28.1%a
Hooper et al. (2010) N =49 ProQOL R-IV N.D. N.D. N.D. 22.4%
N.D. N.D. N.D.
Lahr Keller (1990) N =137 MBI-HSS N.D. N.D. N.D.
High 36% High 40% Low 42%
O’Mahony (2011) N =64 MBI-HSS 30.6 (9.8) 11.35 (5.9) N.D.
High 67%a High 59%a N.D.
Stathopoulouet al. (2011) N =213 MBI-HSS 22.76 (11.12) 9.13 (6.01) 32.68 (8.65)
High 41.8%a High 50.7%a Low 49.3%a
Walsh et al. (1998) N =134 MBI-HSS 21.78 (10.86) 12.05 (6.76) 35.06 (7.18)
High 32.8%a High 64.9%a Low 35.8%a
Garcia-Izquierdoand Rios-Risquez(2012) N =191 MBI-GS 1.88 (1.44) 1.49 (1.32) 5.13 (1.04)
High 37.2%a High 45.5%a Low 9.4%a
Sorour and El-Maksoud (2012) b N =58 MBI-HSS N.D. N.D. N.D. 37.9%
N.D. N.D. N.D.
Van der Ploeg and Kleber (2001) N =127 MBI-GS/ 1.2 (0.89) 1.1 (0.88) 4.4 (0.87)
High 11.7%a High 17.7%a Low 16.3%a
Van der Ploeg and Kleber (2003) N =123 UBOS-A 1.3 (1.0) 1.4 (1.1) 4.5 (0.85)
High 15.4%a High 38.2%a Low 20.3%a
Abbreviations:EE =emotionalexhaustion,DP =depersonalization,PA =lack of personalaccomplishment,BO =burnout,N.C.=not computable,N.D. =No
(adequate)data.
a Data for determinationof percentageof respondentsexceedingthe cut offs were generatedwith reversedsamplingstatistics(Minitab1 16.2.4).
b The scale used for this study is different from the conventionalscale of the instrument.
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 7
Dierendonck,2000) and the ProQOL R-IV (Stamm,2010)
are also describedin Table 2. Normative values (Mn and
SD) for nurses for the MBI-HSS (samplesize 1542 nurses)
were publishedby Schaufeliand Enzmann(1998).Norma-
tive values for MBI-GS and UBOS-A for human services
occupations (sample size 13076 respondents) were
publishedby Schaufeliand Van Dierendonck(2000).Nor-
mative data for the ProQOL R-IV were provided in the
manual of the instrument (Stamm,2010).
The means, SD’s and percentages of caseness for
of Van der Ploeg and Kleber (2001),that used the MBI-GS
and UBOS-A, reported 11.7%,17.7%and 16.3%of respon-
dents exceeding the cut off for emotional exhaustion,
depersonalizationand lack of personal accomplishment,
respectively.Hooper et al. (2010) and Ariapooran (2014)
found 22.4%and 19.2%of respondentswith high levels of
burnout, respectively.
Nine out of 17 studies reported means and standard
deviationsfor the different dimensionsof burnout (Adali
and Priami, 2002; Alexanderand Klein, 2001; Helps,1997;
O’Mahony,2011; Stathopoulouet al., 2011; Walsh et al.,
Table 3
Means and standarddeviationsof the dimensionsof burnout and the (estimateda
) percentageof respondentsexceedingcut off for these dimensions.
Study & number of respondents No. of
resp.
Scale EE Mn(SD)
EE %> cut off
DP Mn(SD)
DP %> cut off
PA Mn(SD)
PA %< cut off
Total burnout
BO%> cut off
Adali and Priami (2002) N =233 MBI-HSS 26.53 (11.29) 9.12(5.3) 35.14(10.99)
High 45.1%a High 49.0%a Low 41.2%a
Alexanderand Klein (2001) N =40 MBI-HSS 17.2 (10.7) 8.4 (6.7) 34.5 (7.8)
High 20%a High 26%a Low 36%a
Ariapooran(2014) N =94 ProQOL R-IV N.D. N.D. N.D. 19.2%
N.D. N.D. N.D.
Bernaldo-De-Quiroset al. (2014) N =127 MBI-HSS N.D. N.D. N.D.
High 9.5% High 13.2% Low 16.1%
Browning et al. (2007) N =100 MBI-HSS 26.81 11.98 37.90
N.C. N.C. N.C.
Escriba`-Agu¨ir et al. (2006);
Escriba-Agu¨ir and Pe´rez-Hoyos (2007)
N =280 MBI-HSS N.D. N.D. N.D.
High 19% High 33.9% Low 46.5%
Helps (1997) N =51 MBI-HSS 21.34 (9.7) 8.09 (6.19) 36.09 (5.47)
High 29.8%a High 43.9%a Low 28.1%a
Hooper et al. (2010) N =49 ProQOL R-IV N.D. N.D. N.D. 22.4%
N.D. N.D. N.D.
Lahr Keller (1990) N =137 MBI-HSS N.D. N.D. N.D.
High 36% High 40% Low 42%
O’Mahony (2011) N =64 MBI-HSS 30.6 (9.8) 11.35 (5.9) N.D.
High 67%a High 59%a N.D.
Stathopoulouet al. (2011) N =213 MBI-HSS 22.76 (11.12) 9.13 (6.01) 32.68 (8.65)
High 41.8%a High 50.7%a Low 49.3%a
Walsh et al. (1998) N =134 MBI-HSS 21.78 (10.86) 12.05 (6.76) 35.06 (7.18)
High 32.8%a High 64.9%a Low 35.8%a
Garcia-Izquierdoand Rios-Risquez(2012) N =191 MBI-GS 1.88 (1.44) 1.49 (1.32) 5.13 (1.04)
High 37.2%a High 45.5%a Low 9.4%a
Sorour and El-Maksoud (2012) b N =58 MBI-HSS N.D. N.D. N.D. 37.9%
N.D. N.D. N.D.
Van der Ploeg and Kleber (2001) N =127 MBI-GS/ 1.2 (0.89) 1.1 (0.88) 4.4 (0.87)
High 11.7%a High 17.7%a Low 16.3%a
Van der Ploeg and Kleber (2003) N =123 UBOS-A 1.3 (1.0) 1.4 (1.1) 4.5 (0.85)
High 15.4%a High 38.2%a Low 20.3%a
Abbreviations:EE =emotionalexhaustion,DP =depersonalization,PA =lack of personalaccomplishment,BO =burnout,N.C.=not computable,N.D. =No
(adequate)data.
a Data for determinationof percentageof respondentsexceedingthe cut offs were generatedwith reversedsamplingstatistics(Minitab1 16.2.4).
b The scale used for this study is different from the conventionalscale of the instrument.
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
while Van der Ploegand Kleber (2001)reportedthe lowest
values for all these dimensions.
For the purpose of this study and with the aim to
estimatethe prevalenceof burnout amongER-nurses,we
used reverse sampling statistics (Minitabß 16.2.4,Penn-
sylvania) to generaterandom data for the seven studies
that reportedonly meansand standarddeviationsfor the
MBI-dimensions. For this reverse sampling method we
assumed,based on previous findings, that the reported
data of the burnout dimensionshad a normal distribution
(Schaufeliet al., 2002; Langelaanet al., 2007; Camposand
Maroco, 2012). The cut off scores for the respective
instruments were used to determine the percentageof
respondentswith high emotionalexhaustion,high deper-
sonalization and low personal accomplishment. The
results of these analyses are reported in Table 3. A
weighted averagepercentageof casenessfor emotional
exhaustion, depersonalizationand lack of personal ac-
complishmentwas calculated.Basedupon the scores for
the reversely generated samples and the originally
reported cut off percentages,on average 25.9% of the
respondents exceededthe cut off scores for emotional
exhaustion,34.8%exceededthe cut offs for depersonali-
zation and 27.2%exceededthe cut off for lack of personal
accomplishment.Consideringthe generalconsensusthat
emotional exhaustion is the core dimension of burnout,
this review shows that 26% of the respondents in the
selectedstudies suffered from burnout.
3.3. Determinantsfor burnoutin emergencynurses
The studies that were included in this review used a
varietyof determinants.For the purposeof this review we
categorized these determinants in terms of ‘individual
factors’and ‘job related factors’,basedon an overview of
burnout by Maslach et al. (2001). For each category,a
generalintroduction is given,followed by the description
of the results for the selected studies on burnout in
emergency nurses. The results of these studies can be
found in Table 1.
3.3.1.Individualfactors
3.3.1.1.Demographiccharacteristics.In general popula-
tions, younger age was found to be related to a higher
risk of burnout.Genderwas also found to be predictiveof
burnout in several studies but the results were not
nor Hooper et al. (2010) found significant relationships
betweenage,seniorityor genderand burnout dimensions.
3.3.1.2.Personalitycharacteristics.In the job stress litera-
ture on a broad set of populations,personalitycharacter-
istics, such as neuroticism, extraversion,agreeableness,
conscientiousnessand openness,also called ‘The Big Five’
personalitytraits (McCraeand Costa,1987),were found to
be associatedwith burnout (Zellars et al., 2000; Bakker
et al., 2006; Swider and Zimmerman,2010; Shimizutani
et al., 2008; Maslach et al., 2001).Low levels of hardiness
(less involvement in daily activities, a lower sense of
control overevents,and lessopennessto change)were also
related to higher levels of emotionalexhaustion(Maslach
et al., 2001).
In the ER-nursesstudies,includedin the presentreview,
personalitycharacteristicswere not frequentlyreportedas
potential determinantsof burnout. Alexanderet al. found
personswith a hardy personalityto view eventsmore as
meaningful (leading to higher levels of commitment),
challengingand under their control than their colleagues.
This studyreportsa strongnegativecorrelationbetweenthe
level of commitment,perceivedcontrol,job challengeand
emotionalexhaustion.Also for depersonalizationnegative
relationshipswere found with commitment and control.
Personal accomplishmentwas positively related to com-
mitment,controlandchallenge(AlexanderandKlein,2001).
Lack of flexibility, stubbornness,judgmentalbehaviorand
difficulty in adaptation were also reported as potential
determinantsof burnout (Walsh et al., 1998).
3.3.1.3.Copingstrategies.In studies on occupationalwell-
being in nurses,copingstrategieswere found to be related
to well-being and performance.Active problem focused
copingwas found to be relatedto lower levelsof emotional
exhaustionand depersonalizationand to higher personal
accomplishment.Passiveavoidant and emotional coping
strategies,especially when used alone or as a dominant
mode of coping, were found to be ineffectivein dealing
with stress(Shirey,2006;Shimizutaniet al.,2008;Maslach
et al., 2001; Semmer,2003).
In the selectedstudiesin ER-nurses,Van der Ploeg and
Kleber (2001) found significant positive correlationsbe-
tween avoidant behavior and emotional exhaustionand
depersonalization and reported a negative correlation
with personal accomplishment.They state that avoidant
behavior after exposureto traumatic eventsis not a good
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx8
values for all these dimensions.
For the purpose of this study and with the aim to
estimatethe prevalenceof burnout amongER-nurses,we
used reverse sampling statistics (Minitabß 16.2.4,Penn-
sylvania) to generaterandom data for the seven studies
that reportedonly meansand standarddeviationsfor the
MBI-dimensions. For this reverse sampling method we
assumed,based on previous findings, that the reported
data of the burnout dimensionshad a normal distribution
(Schaufeliet al., 2002; Langelaanet al., 2007; Camposand
Maroco, 2012). The cut off scores for the respective
instruments were used to determine the percentageof
respondentswith high emotionalexhaustion,high deper-
sonalization and low personal accomplishment. The
results of these analyses are reported in Table 3. A
weighted averagepercentageof casenessfor emotional
exhaustion, depersonalizationand lack of personal ac-
complishmentwas calculated.Basedupon the scores for
the reversely generated samples and the originally
reported cut off percentages,on average 25.9% of the
respondents exceededthe cut off scores for emotional
exhaustion,34.8%exceededthe cut offs for depersonali-
zation and 27.2%exceededthe cut off for lack of personal
accomplishment.Consideringthe generalconsensusthat
emotional exhaustion is the core dimension of burnout,
this review shows that 26% of the respondents in the
selectedstudies suffered from burnout.
3.3. Determinantsfor burnoutin emergencynurses
The studies that were included in this review used a
varietyof determinants.For the purposeof this review we
categorized these determinants in terms of ‘individual
factors’and ‘job related factors’,basedon an overview of
burnout by Maslach et al. (2001). For each category,a
generalintroduction is given,followed by the description
of the results for the selected studies on burnout in
emergency nurses. The results of these studies can be
found in Table 1.
3.3.1.Individualfactors
3.3.1.1.Demographiccharacteristics.In general popula-
tions, younger age was found to be related to a higher
risk of burnout.Genderwas also found to be predictiveof
burnout in several studies but the results were not
nor Hooper et al. (2010) found significant relationships
betweenage,seniorityor genderand burnout dimensions.
3.3.1.2.Personalitycharacteristics.In the job stress litera-
ture on a broad set of populations,personalitycharacter-
istics, such as neuroticism, extraversion,agreeableness,
conscientiousnessand openness,also called ‘The Big Five’
personalitytraits (McCraeand Costa,1987),were found to
be associatedwith burnout (Zellars et al., 2000; Bakker
et al., 2006; Swider and Zimmerman,2010; Shimizutani
et al., 2008; Maslach et al., 2001).Low levels of hardiness
(less involvement in daily activities, a lower sense of
control overevents,and lessopennessto change)were also
related to higher levels of emotionalexhaustion(Maslach
et al., 2001).
In the ER-nursesstudies,includedin the presentreview,
personalitycharacteristicswere not frequentlyreportedas
potential determinantsof burnout. Alexanderet al. found
personswith a hardy personalityto view eventsmore as
meaningful (leading to higher levels of commitment),
challengingand under their control than their colleagues.
This studyreportsa strongnegativecorrelationbetweenthe
level of commitment,perceivedcontrol,job challengeand
emotionalexhaustion.Also for depersonalizationnegative
relationshipswere found with commitment and control.
Personal accomplishmentwas positively related to com-
mitment,controlandchallenge(AlexanderandKlein,2001).
Lack of flexibility, stubbornness,judgmentalbehaviorand
difficulty in adaptation were also reported as potential
determinantsof burnout (Walsh et al., 1998).
3.3.1.3.Copingstrategies.In studies on occupationalwell-
being in nurses,copingstrategieswere found to be related
to well-being and performance.Active problem focused
copingwas found to be relatedto lower levelsof emotional
exhaustionand depersonalizationand to higher personal
accomplishment.Passiveavoidant and emotional coping
strategies,especially when used alone or as a dominant
mode of coping, were found to be ineffectivein dealing
with stress(Shirey,2006;Shimizutaniet al.,2008;Maslach
et al., 2001; Semmer,2003).
In the selectedstudiesin ER-nurses,Van der Ploeg and
Kleber (2001) found significant positive correlationsbe-
tween avoidant behavior and emotional exhaustionand
depersonalization and reported a negative correlation
with personal accomplishment.They state that avoidant
behavior after exposureto traumatic eventsis not a good
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx8

In none of the studies in ER-nurses,included in this
review, job attitudesand goal settingwere investigatedas
a predictor of burnout in ER nurses.
3.3.2.Work relatedfactors
3.3.2.1.Exposureto traumatic events.Repetitive profes-
sional exposureto traumaticevents,such as confrontation
with severe injuries, death, suicide, aggression and
suffering,was reported to be related to the development
of post-traumaticstress syndrome(PTSD) and burnout in
various nurses’populations (Donnelly and Siebert,2009;
Mealer et al., 2009; Collins and Long, 2003).
In one of the studies included in the present review,
Alexanderand Klein (2001) reported that ER-nurseswho
were exposedto traumaticeventsin the previous6 months
had higher levels of casenessfor high emotional exhaus-
tion (23%vs. 5%,p =.03) and high depersonalization(32%
vs. 0%,p =.003)but they found no differencesfor caseness
of low personal accomplishment(33% vs. 35%,p =.89),
comparedto non-exposedER-nurses.They reported that
69%of the exposedER-nursesmentionedthat they ‘never’
had sufficient time to recover emotionally between
traumatic events (Alexander and Klein, 2001). Van der
Ploeg and Kleber (2001) found the number of traumatic
eventsto be positively correlatedto posttraumaticstress
symptoms,emotional exhaustionand depersonalization.
In their longitudinal study (2003) they found a positive
long term relationshipbetween frequencyof exposureat
baselineand emotionalexhaustionand depersonalization
at follow up. Garcia-Izquierdo and Rios-Risquez (2012)
reported a positive correlation between frequency of
confrontation with death and suffering and emotional
exhaustion.Bernaldo-De-Quiroset al. (2014)found nurses
who were exposed more frequently to violence (insults,
threats and physical violence) to report higher levels of
emotional exhaustionand depersonalization.
3.3.2.2.Job characteristics.One of the most popular theo-
retical occupational stress models is the Job Demand
Control Support Model (JDCS),developedby Karasekand
Theorell (1990). This model defines three dimensions as
predictorsof occupationalstress:‘job demand’as a burden
and ‘job control’and ‘socialsupport’as potentialresources
or buffers.Job demandis definedas the psychologicalwork
load in terms of time pressure,role conflict and quantita-
tive workload. Job control, also called decision latitude,is
sub-dimensions:socialsupportprovidedby the colleagues
or co-workers and social support provided by the
supervisor. Previous research in multiple occupational
groups showed relationshipsbetween JDCS-variablesand
burnout (Mark and Smith, 2008). Researchin nurses also
revealedrelationshipsbetween JDCS-variablesand burn-
out (Ha¨usser et al., 2010; Gelsemaet al., 2006). In those
studies,burnout was seen as an end-stageof adaptation
failure resulting from the long-term imbalance between
job demandsand resources(McSherry et al., 2012).
A number of studies, included in this review on ER-
nursesreport JCDS-variablesto be relatedto burnout.The
results are describedby JDCS-variable.
Psychologicaldemands(work/time pressure)was found
to be related to burnout and its dimensions. Adali and
Priami (2002) found work pressure to be a significant
positivepredictorfor emotionalexhaustion.Escriba-Agu¨ir
and Pe´rez-Hoyos (2007) found high psychological
demands to be predictive of high levels of emotional
exhaustion. Garcia-Izquierdo and Rios-Risquez (2012)
found excessive workload to be related to higher
emotional exhaustion and depersonalizationbut found
no relationship with personal accomplishment.Van der
Ploeg and Kleber (2001) report positive correlations
between emotional demands and emotional exhaustion
and depersonalizationbut did not find any relationship
with personalaccomplishment.In their longitudinalstudy
emotionaldemandsat baselinewere positively related to
emotional exhaustionand depersonalizationat follow-up
(Van der Ploeg and Kleber, 2003). One study reported an
inverserelationship:an increasein the job demandscore
was related to a decreasein the general burnout score
(r =0.34,p < .01) (Sorour and El-Maksoud,2012).Physical
demandsin ER-nurses showed no relationship (dynamic
nor static) with burnout in the study of Escriba-Agu¨ir and
Pe´rez-Hoyos (2007).However, this variable was found to
be predictivefor higher emotional exhaustionin longitu-
dinal analysis(Van der Ploeg and Kleber, 2003).
Thelevelof JobControlwas foundto be negativelyrelated
to emotional exhaustionand depersonalizationand posi-
tively relatedto personalaccomplishment(Alexanderand
Klein, 2001). In the study of Browning et al. (2007),
perceived control moderated the relationship between
work stressorson the one hand and emotionalexhaustion
and depersonalizationon the otherhand.Escriba-Agu¨ir and
Pe´rez-Hoyos (2007) did not find a relationship between
controland emotionalexhaustion.Van der Ploegand Kleber
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 9
review, job attitudesand goal settingwere investigatedas
a predictor of burnout in ER nurses.
3.3.2.Work relatedfactors
3.3.2.1.Exposureto traumatic events.Repetitive profes-
sional exposureto traumaticevents,such as confrontation
with severe injuries, death, suicide, aggression and
suffering,was reported to be related to the development
of post-traumaticstress syndrome(PTSD) and burnout in
various nurses’populations (Donnelly and Siebert,2009;
Mealer et al., 2009; Collins and Long, 2003).
In one of the studies included in the present review,
Alexanderand Klein (2001) reported that ER-nurseswho
were exposedto traumaticeventsin the previous6 months
had higher levels of casenessfor high emotional exhaus-
tion (23%vs. 5%,p =.03) and high depersonalization(32%
vs. 0%,p =.003)but they found no differencesfor caseness
of low personal accomplishment(33% vs. 35%,p =.89),
comparedto non-exposedER-nurses.They reported that
69%of the exposedER-nursesmentionedthat they ‘never’
had sufficient time to recover emotionally between
traumatic events (Alexander and Klein, 2001). Van der
Ploeg and Kleber (2001) found the number of traumatic
eventsto be positively correlatedto posttraumaticstress
symptoms,emotional exhaustionand depersonalization.
In their longitudinal study (2003) they found a positive
long term relationshipbetween frequencyof exposureat
baselineand emotionalexhaustionand depersonalization
at follow up. Garcia-Izquierdo and Rios-Risquez (2012)
reported a positive correlation between frequency of
confrontation with death and suffering and emotional
exhaustion.Bernaldo-De-Quiroset al. (2014)found nurses
who were exposed more frequently to violence (insults,
threats and physical violence) to report higher levels of
emotional exhaustionand depersonalization.
3.3.2.2.Job characteristics.One of the most popular theo-
retical occupational stress models is the Job Demand
Control Support Model (JDCS),developedby Karasekand
Theorell (1990). This model defines three dimensions as
predictorsof occupationalstress:‘job demand’as a burden
and ‘job control’and ‘socialsupport’as potentialresources
or buffers.Job demandis definedas the psychologicalwork
load in terms of time pressure,role conflict and quantita-
tive workload. Job control, also called decision latitude,is
sub-dimensions:socialsupportprovidedby the colleagues
or co-workers and social support provided by the
supervisor. Previous research in multiple occupational
groups showed relationshipsbetween JDCS-variablesand
burnout (Mark and Smith, 2008). Researchin nurses also
revealedrelationshipsbetween JDCS-variablesand burn-
out (Ha¨usser et al., 2010; Gelsemaet al., 2006). In those
studies,burnout was seen as an end-stageof adaptation
failure resulting from the long-term imbalance between
job demandsand resources(McSherry et al., 2012).
A number of studies, included in this review on ER-
nursesreport JCDS-variablesto be relatedto burnout.The
results are describedby JDCS-variable.
Psychologicaldemands(work/time pressure)was found
to be related to burnout and its dimensions. Adali and
Priami (2002) found work pressure to be a significant
positivepredictorfor emotionalexhaustion.Escriba-Agu¨ir
and Pe´rez-Hoyos (2007) found high psychological
demands to be predictive of high levels of emotional
exhaustion. Garcia-Izquierdo and Rios-Risquez (2012)
found excessive workload to be related to higher
emotional exhaustion and depersonalizationbut found
no relationship with personal accomplishment.Van der
Ploeg and Kleber (2001) report positive correlations
between emotional demands and emotional exhaustion
and depersonalizationbut did not find any relationship
with personalaccomplishment.In their longitudinalstudy
emotionaldemandsat baselinewere positively related to
emotional exhaustionand depersonalizationat follow-up
(Van der Ploeg and Kleber, 2003). One study reported an
inverserelationship:an increasein the job demandscore
was related to a decreasein the general burnout score
(r =0.34,p < .01) (Sorour and El-Maksoud,2012).Physical
demandsin ER-nurses showed no relationship (dynamic
nor static) with burnout in the study of Escriba-Agu¨ir and
Pe´rez-Hoyos (2007).However, this variable was found to
be predictivefor higher emotional exhaustionin longitu-
dinal analysis(Van der Ploeg and Kleber, 2003).
Thelevelof JobControlwas foundto be negativelyrelated
to emotional exhaustionand depersonalizationand posi-
tively relatedto personalaccomplishment(Alexanderand
Klein, 2001). In the study of Browning et al. (2007),
perceived control moderated the relationship between
work stressorson the one hand and emotionalexhaustion
and depersonalizationon the otherhand.Escriba-Agu¨ir and
Pe´rez-Hoyos (2007) did not find a relationship between
controland emotionalexhaustion.Van der Ploegand Kleber
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
exhaustion.Van der Ploeg and Kleber (2001)found lack of
supervisor social support to be positively related to
emotional exhaustion,depersonalizationand negatively
to personal accomplishment.Lack of social support from
colleagues was also positively related to emotional
exhaustion,depersonalizationand negativelyto personal
accomplishment.In contrast, Adali and Priami (2002)
found a rise in supervisorsocial supportto be relatedto an
increasein depersonalization.In their longitudinal study,
Van der Ploeg and Kleber (2003) found lack of supervisor
socialsupportat baselineto be relatedto higheremotional
exhaustionand depersonalizationand to lower personal
accomplishmentat follow up. Also lack of social support
from colleaguesat baselineshowedsignificantcorrelations
with higher emotional exhaustionand depersonalization
and lower personal accomplishmentat follow up. Inter-
personally conflicts, that can be very disturbing for the
team cohesion, were found to be positively related to
emotionalexhaustion,depersonalizationand negativelyto
personal accomplishmentin ER-nurses(Garcia-Izquierdo
and Rios-Risquez,2012). Ariapooran (2014) found higher
levelsof social supportfrom peersand family to be related
to lower levels of burnout.
3.3.2.3.Organizationalfactors.Next to job characteristics,
organizationaland environmentalcharacteristics,such as
personnel and material resources, procedures,policies,
organizationalcultureand reward,provedto be associated
with the employees’wellnessin severalstudy populations
(Maslach et al., 2001; Poncet et al., 2007).
In one of the studies included in the present review
(O’Mahony,2011) 53%of the ER-nursesrated their work
environmentas unfavorable.In another study (Alexander
and Klein, 2001)dissatisfactionwas associatedwith higher
scores on emotional exhaustion and depersonalization.
The existing literature on ER-nurses mentions various
organizationalfactors as determinantsfor burnout. These
are describedbelow.
Communicationandcollaborationwith other profession-
al disciplines was taken into account in a number of
studies. O’Mahony (2011) reported nurse/physiciancol-
laboration to have a negativecorrelation with emotional
exhaustion and depersonalization. The experience of
working as a team was also negatively related to
depersonalization(O’Mahony,2011).Another study found
the level of interpersonalconflictsto be positively related
to emotional exhaustion and depersonalization and
Staffingissueswere taken into accountin two studies:
quality of staffing,adequacyof work schedulesand shift
work were significantly correlated with fatigue and
decreased concentration, what in turn was related to
burnout(Walsh et al.,1998).Understaffingwas mentioned
as an important predictor of stress and burnout in ER-
nurses(Helps,1997).Permanentnight shift was relatedto
a decreasein feelings of personal accomplishment(F(3,
185)=3.06 p < .05) (Garcia-Izquierdoand Rios-Risquez,
2012).Lackof materialresourceswas found to be relatedto
higheremotionalexhaustionand depersonalization(Garcia-
Izquierdoand Rios-Risquez,2012).Organizationalculturewas
alsotakeninto account.A moreinnovativecultureon theward
was found to be related to lower levels of emotional
exhaustion (Adali and Priami, 2002). O’Mahony (2011)
reported that a perceived lack of quality assurance
initiatives in the institution was associatedwith higher
levels emotional exhaustion. Financial reward was not
found to be predictive of any dimension of burnout in ER
nurses (Van der Ploeg and Kleber, 2003).
4. Discussion
In the present study the research on burnout, con-
ducted in the past 25 years in ER-nurses,was examined.
This review focuses on (1) the prevalenceof burnout in
nursesworking in ER-settingsand (2) the identificationof
the determinantsof burnout in terms of individual factors
(demographiccharacteristics,personality factors, coping
strategies and job attitudes) and work related factors
(exposureto traumatic incidents, job characteristicsand
organizational factors). We analyzed the results of 17
empiricalstudiespublishedbetween1987 and 2012.All of
these quantitativestudies had a study sample of at least
40 ER-nurses,with a responserate higher than 25%and
burnout as an outcomemeasure.
The weighted average percentage of respondents
exceeding the cut-off for the different dimensions of
burnout was 26% for emotional exhaustion, 35% for
depersonalizationand 27% for lack of personal accom-
plishment.Theseresults are alarming and need attention
of all stakeholders.The broad range of casenessbetween
the selectedstudies can be partly explainedby the small
sample sizes in several studies. However, previous
research in other nursing populations also showed
significantcross-nationaldifferencesin the scoreson the
MBI-dimensions. North-American nurses were found to
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx10
supervisor social support to be positively related to
emotional exhaustion,depersonalizationand negatively
to personal accomplishment.Lack of social support from
colleagues was also positively related to emotional
exhaustion,depersonalizationand negativelyto personal
accomplishment.In contrast, Adali and Priami (2002)
found a rise in supervisorsocial supportto be relatedto an
increasein depersonalization.In their longitudinal study,
Van der Ploeg and Kleber (2003) found lack of supervisor
socialsupportat baselineto be relatedto higheremotional
exhaustionand depersonalizationand to lower personal
accomplishmentat follow up. Also lack of social support
from colleaguesat baselineshowedsignificantcorrelations
with higher emotional exhaustionand depersonalization
and lower personal accomplishmentat follow up. Inter-
personally conflicts, that can be very disturbing for the
team cohesion, were found to be positively related to
emotionalexhaustion,depersonalizationand negativelyto
personal accomplishmentin ER-nurses(Garcia-Izquierdo
and Rios-Risquez,2012). Ariapooran (2014) found higher
levelsof social supportfrom peersand family to be related
to lower levels of burnout.
3.3.2.3.Organizationalfactors.Next to job characteristics,
organizationaland environmentalcharacteristics,such as
personnel and material resources, procedures,policies,
organizationalcultureand reward,provedto be associated
with the employees’wellnessin severalstudy populations
(Maslach et al., 2001; Poncet et al., 2007).
In one of the studies included in the present review
(O’Mahony,2011) 53%of the ER-nursesrated their work
environmentas unfavorable.In another study (Alexander
and Klein, 2001)dissatisfactionwas associatedwith higher
scores on emotional exhaustion and depersonalization.
The existing literature on ER-nurses mentions various
organizationalfactors as determinantsfor burnout. These
are describedbelow.
Communicationandcollaborationwith other profession-
al disciplines was taken into account in a number of
studies. O’Mahony (2011) reported nurse/physiciancol-
laboration to have a negativecorrelation with emotional
exhaustion and depersonalization. The experience of
working as a team was also negatively related to
depersonalization(O’Mahony,2011).Another study found
the level of interpersonalconflictsto be positively related
to emotional exhaustion and depersonalization and
Staffingissueswere taken into accountin two studies:
quality of staffing,adequacyof work schedulesand shift
work were significantly correlated with fatigue and
decreased concentration, what in turn was related to
burnout(Walsh et al.,1998).Understaffingwas mentioned
as an important predictor of stress and burnout in ER-
nurses(Helps,1997).Permanentnight shift was relatedto
a decreasein feelings of personal accomplishment(F(3,
185)=3.06 p < .05) (Garcia-Izquierdoand Rios-Risquez,
2012).Lackof materialresourceswas found to be relatedto
higheremotionalexhaustionand depersonalization(Garcia-
Izquierdoand Rios-Risquez,2012).Organizationalculturewas
alsotakeninto account.A moreinnovativecultureon theward
was found to be related to lower levels of emotional
exhaustion (Adali and Priami, 2002). O’Mahony (2011)
reported that a perceived lack of quality assurance
initiatives in the institution was associatedwith higher
levels emotional exhaustion. Financial reward was not
found to be predictive of any dimension of burnout in ER
nurses (Van der Ploeg and Kleber, 2003).
4. Discussion
In the present study the research on burnout, con-
ducted in the past 25 years in ER-nurses,was examined.
This review focuses on (1) the prevalenceof burnout in
nursesworking in ER-settingsand (2) the identificationof
the determinantsof burnout in terms of individual factors
(demographiccharacteristics,personality factors, coping
strategies and job attitudes) and work related factors
(exposureto traumatic incidents, job characteristicsand
organizational factors). We analyzed the results of 17
empiricalstudiespublishedbetween1987 and 2012.All of
these quantitativestudies had a study sample of at least
40 ER-nurses,with a responserate higher than 25%and
burnout as an outcomemeasure.
The weighted average percentage of respondents
exceeding the cut-off for the different dimensions of
burnout was 26% for emotional exhaustion, 35% for
depersonalizationand 27% for lack of personal accom-
plishment.Theseresults are alarming and need attention
of all stakeholders.The broad range of casenessbetween
the selectedstudies can be partly explainedby the small
sample sizes in several studies. However, previous
research in other nursing populations also showed
significantcross-nationaldifferencesin the scoreson the
MBI-dimensions. North-American nurses were found to
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
be different between cultures and nationalities.Schaufeli
and Van Dierendonck (1995) advised therefore to be
cautious with cross-national comparison of burnout
results. Poghosyan et al. (2009) also showed significant
differences in the factor loadings and inter-correlations
of the MBI-items across countries. Transnational differ-
ences in the perception and scoring of the MBI-items
might have resulted in differences in the composite
scores on the burnout dimensions (Poghosyan et al.,
2009).All theseissuespoint at important methodological
flaws in cross-culturalresearch.As pointed out by Squires
et al. (2013) even translation/back-translation of an
instrument such as e.g. the MBI, is not a sufficient
guaranteefor the comparability of the results. Character-
istics of the health care system, mastery of professional
language,relevance to health care workers in different
countries, and quality of professional research infra-
structure are other sourcesof instrumental bias. Another
aspect that may hamper the comparison of the burnout
scores for the selected studies in this review is the fact
that three different instruments were used (MBI-HSS,
MBI-GS and ProQOL R-IV).
In this review,the limit of the samplesizefor inclusionof
a studywas set at 25%.Despitethis,the samplesize of some
studiesincludedin this review is still low, which may have
influenced the results. Differencesin composition of the
studysamplesmayalsohaveconsequencesfor the results.It
is remarkablethat the two highestand the two lowest rates
of casenessfor emotionalexhaustionand depersonalization
are, respectively,reportedby the study sampleswith the
highestand the lowest proportionsof femalenurses.Two
authorscollectedtheir data at conferencesbecauseof the
availability of potential respondents(Walsh et al., 1998;
Browning et al., 2007).This can have causedbias (healthy
worker effect)since people who go to congressesare less
likely to suffer from burnout. Finally, the study of Sorour
and El-Maksoud (2012) used a different scale than the
conventionalMBI-HSS instrument,making comparisonof
the prevalence results with other studies impossible.
Nevertheless,the averagecasenessfor burnoutin ER-nurses
is high and requiresthe attentionof hospital management
and policy makers, as burnout is directly related to job
satisfaction(Rheajaneet al.,2013)nurses’well-being(Burke
et al., 2010), nurse turnover (Leiter and Maslach, 2009),
patientsafety(Halbeslebenet al., 2008)and quality of care
(Poghosyanet al.,2010b).High ratesof casenessfor burnout
were also found in studies in non-ER nursing disciplines:
work stressorsand some outcomes,without taking into
account the perception of the stressor by the ER-nurse.
Additionally,oftendifferentmeasureswere usedto assessa
commonconcept.The lack of similarity acrossthe different
studiesin termsof determinants,instrumentsandoutcomes
is an obstacleto conducta meta-regressionanalysis,what
makesa proper statisticalsummaryimpossible.Moreover,
16 out of 17 studieshad a cross-sectionaldesign.All these
issuesare quite unfortunatebecause(1) only small partsof
variancecan be explained,(2) interrelationshipsbetween
determinantscannotbe adequatelyinvestigated,(3) results
from different studies on the same concept cannot be
comparedand (4) causal relationshipsbetween determi-
nants and outcomescannot be drawn. A more preferable
approachis the use of a longitudinal design based on an
informationprocessingapproachwhich takesinto account
the consequencesover time of individual appraisal and
coping of work stress(Perrewe´ and Zellars,1999; Mackin-
tosh, 2007).
Starting from the abovementioned methodological
strengths and weaknesses,the results of Van der Ploeg
and Kleber (2001, 2003), Escriba-Agu¨ir and Pe´rez-Hoyos
(2007) and Garcia-Izquierdo and Rios-Risquez (2012)
provide the strongest evidence concerning burnout and
its determinants in ER-nurses. These studies show that
the JDCS-variablesare strong determinantsof burnout in
ER-nurses. Van der Ploeg and Kleber (2001, 2003) and
Garcia-Izquierdo and Rios-Risquez (2012) also showed
the deleterious (long term) effect of repetitive exposure
to traumatic events on the development of burnout in
ER-nurses. Finally, seven out of 17 studies indicate the
importance of good communication, interdisciplinary
collaboration and team spirit to prevent burnout (Adali
and Priami, 2002; Escriba-Agu¨ir and Pe´rez-Hoyos, 2007;
Escriba`-Agu¨ir et al., 2006; Garcia-Izquierdo and Rios-
Risquez, 2012; O’Mahony, 2011; Van der Ploeg and
Kleber, 2001; Van der Ploeg and Kleber, 2003). On the
other hand, personality characteristics,coping strategies
and job attitudes (goal orientation) were underinvesti-
gatedin the selectedstudies.Future researchshould take
these aspects into account.
5. Implications for nursing
Although several studies suffer from methodological
weaknessesand flaws,the presentsystematicreview offers
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 11
and Van Dierendonck (1995) advised therefore to be
cautious with cross-national comparison of burnout
results. Poghosyan et al. (2009) also showed significant
differences in the factor loadings and inter-correlations
of the MBI-items across countries. Transnational differ-
ences in the perception and scoring of the MBI-items
might have resulted in differences in the composite
scores on the burnout dimensions (Poghosyan et al.,
2009).All theseissuespoint at important methodological
flaws in cross-culturalresearch.As pointed out by Squires
et al. (2013) even translation/back-translation of an
instrument such as e.g. the MBI, is not a sufficient
guaranteefor the comparability of the results. Character-
istics of the health care system, mastery of professional
language,relevance to health care workers in different
countries, and quality of professional research infra-
structure are other sourcesof instrumental bias. Another
aspect that may hamper the comparison of the burnout
scores for the selected studies in this review is the fact
that three different instruments were used (MBI-HSS,
MBI-GS and ProQOL R-IV).
In this review,the limit of the samplesizefor inclusionof
a studywas set at 25%.Despitethis,the samplesize of some
studiesincludedin this review is still low, which may have
influenced the results. Differencesin composition of the
studysamplesmayalsohaveconsequencesfor the results.It
is remarkablethat the two highestand the two lowest rates
of casenessfor emotionalexhaustionand depersonalization
are, respectively,reportedby the study sampleswith the
highestand the lowest proportionsof femalenurses.Two
authorscollectedtheir data at conferencesbecauseof the
availability of potential respondents(Walsh et al., 1998;
Browning et al., 2007).This can have causedbias (healthy
worker effect)since people who go to congressesare less
likely to suffer from burnout. Finally, the study of Sorour
and El-Maksoud (2012) used a different scale than the
conventionalMBI-HSS instrument,making comparisonof
the prevalence results with other studies impossible.
Nevertheless,the averagecasenessfor burnoutin ER-nurses
is high and requiresthe attentionof hospital management
and policy makers, as burnout is directly related to job
satisfaction(Rheajaneet al.,2013)nurses’well-being(Burke
et al., 2010), nurse turnover (Leiter and Maslach, 2009),
patientsafety(Halbeslebenet al., 2008)and quality of care
(Poghosyanet al.,2010b).High ratesof casenessfor burnout
were also found in studies in non-ER nursing disciplines:
work stressorsand some outcomes,without taking into
account the perception of the stressor by the ER-nurse.
Additionally,oftendifferentmeasureswere usedto assessa
commonconcept.The lack of similarity acrossthe different
studiesin termsof determinants,instrumentsandoutcomes
is an obstacleto conducta meta-regressionanalysis,what
makesa proper statisticalsummaryimpossible.Moreover,
16 out of 17 studieshad a cross-sectionaldesign.All these
issuesare quite unfortunatebecause(1) only small partsof
variancecan be explained,(2) interrelationshipsbetween
determinantscannotbe adequatelyinvestigated,(3) results
from different studies on the same concept cannot be
comparedand (4) causal relationshipsbetween determi-
nants and outcomescannot be drawn. A more preferable
approachis the use of a longitudinal design based on an
informationprocessingapproachwhich takesinto account
the consequencesover time of individual appraisal and
coping of work stress(Perrewe´ and Zellars,1999; Mackin-
tosh, 2007).
Starting from the abovementioned methodological
strengths and weaknesses,the results of Van der Ploeg
and Kleber (2001, 2003), Escriba-Agu¨ir and Pe´rez-Hoyos
(2007) and Garcia-Izquierdo and Rios-Risquez (2012)
provide the strongest evidence concerning burnout and
its determinants in ER-nurses. These studies show that
the JDCS-variablesare strong determinantsof burnout in
ER-nurses. Van der Ploeg and Kleber (2001, 2003) and
Garcia-Izquierdo and Rios-Risquez (2012) also showed
the deleterious (long term) effect of repetitive exposure
to traumatic events on the development of burnout in
ER-nurses. Finally, seven out of 17 studies indicate the
importance of good communication, interdisciplinary
collaboration and team spirit to prevent burnout (Adali
and Priami, 2002; Escriba-Agu¨ir and Pe´rez-Hoyos, 2007;
Escriba`-Agu¨ir et al., 2006; Garcia-Izquierdo and Rios-
Risquez, 2012; O’Mahony, 2011; Van der Ploeg and
Kleber, 2001; Van der Ploeg and Kleber, 2003). On the
other hand, personality characteristics,coping strategies
and job attitudes (goal orientation) were underinvesti-
gatedin the selectedstudies.Future researchshould take
these aspects into account.
5. Implications for nursing
Although several studies suffer from methodological
weaknessesand flaws,the presentsystematicreview offers
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx 11

ER-nurses,futureinterventionresearchshouldexaminethe
validity of thesesuggestions.
Conflict of interest
No conflict of interest has been declared by the
author(s).
Funding statement
This research received no specific grant from any
fundingagencyin the public, commercial,or not-for-profit
sectors.
References
Adali, E., Priami, M., 2002.Burnout amongnursesin intensivecare units,
internal medicinewards and emergencydepartmentsin Greek hos-
pitals. ICUs Nurs. Web J. 1–19 (ISSN 1108-7366).
Ahola, K., Toppinen-Tanner,S., Huuhtanen,P., Koskinen,A., Va¨na¨nen, A.,
2009. Occupationalburnout and chronic work disability: an eight
year cohort study on pensioningamongFinish forest industry work-
ers. J. AffectiveDis. 115, 150–159.
Aiken,L., Clarke,S.,Sloane,D., Sochalski,J., Silber,J., 2002.Hospital nurse
staffing and patient mortality, nurse burnout, and job satisfaction.
JAMA 288, 1987–1993.
Alexander,D., Klein, S.,2001.Impact of accidentand emergencywork on
mentalhealthand emotionalwell-being.Br. J. Psychiatry178, 76–81.
Ariapooran,S., 2014. Compassionfatigueand burnout in Iranian nurses:
the role of perceivedsocialsupport.Iran. J. Nurs.Midwifery Res.19 (3)
279–284.
Aromaa,A., Koskinen,S.,2004.Health and FunctionalCapacityin Finland:
BaselineResults of the Health 2000 ExaminationsSurvey. KTL-Na-
tional Public Health Institute,Helsinki.
Bakker, A., Demerouti, E., Euwema, M., 2005. Job resources buffer
the impact of job demands on burnout. J. Occup. Health Psychol.
10, 170–180.
Bakker,A., Van der Zee,K., Lewig, K., Dollard, M., 2006. The relationship
betweenthe big five personalityfactorsand burnout: a study among
volunteercounselors.J. Soc. Psychol.146, 31–50.
Ball,J., Pike,G.,Griffiths,P., Rafferty,A., Murrells, T.,2012.RN4CASTNurse
Surveyin England.King’s CollegeLondon,London.
Bernaldo-De-Quiros,M., Piccini, A.T., Gomez,M.M., Cerdeira,J.C., 2014.
Psychologicalconsequencedof aggressionin pre-hospitalemergency
care: cross sectionalsurvey.Int. J. Nurs. Stud.,[Epub aheadof print].
Borritz,M., Rugulies,R.,Christensen,K., Villadsen,E., Kristensen,T., 2006.
Burnout as a predictor of self-reported sickness absence among
human serviceworkers: prospectivefindings from three year follow
up of the PUMA study. Occup.Environ. Med. 63, 98–106.
Brenninkmeijer,V., Van Yperen, N., 2003. How to conduct researchon
burnout: advantages and disadvantages of an unidimensional
approachto burnout. Occup.Environ. Med. 60, 16–21.
Browning, L., Ryan, C., Thomas, S., Greenberg,M., Rolniak, S., 2007.
Escriba`-Agu¨ir, V., Martin-Baena,D., Pe´rez-Hoyos, S., 2006. Psychosocial
work environment and burnout among emergency medical and
nursing staff. Int. Arch. Occup.Environ. Health 80, 127–133.
Escriba-Agu¨ir, V., Pe´rez-Hoyos, S., 2007. Psychologicalwell-being and
psychosocialwork environment characteristicsamong emergency
medical and nursing staff. StressHealth 23, 153–160.
Flynn, L., Thomas-Hawkins,C., Clarke,S.,2009.Organizationaltraits,care
processes,and burnout amongchronic hemodialysisnurses.West. J.
Nurs. Res. 31, 569–582.
Freudenberger,H., 1974. Staff burn-out. J. Soc. Issues30, 159–165.
Gaines,J., Jermier,J., 1983.Emotionalexhaustionin a high stressorgani-
zation. Acad. Manage.J. 26, 567–586.
Garcia-Izquierdo,M., Rios-Risquez,M., 2012. The relationship between
psychosocialjob stress and burnout in emergencydepartment:an
exploratorystudy. Nurs. Outlook 60, 322–329.
Gates,D., Gillespie, G., Succop,P., 2011. Violence againstnurses and its
impact on stressand productivity.Nurs. Econ. 29, 59–67.
Gelsema, T., Van der Doef, M., Maes, S., Janssen, M., Akerboom, S.,
Verhoeven, C., 2006. A longitudinal study of job stress in the
nursing profession: causesand consequences.J. Nurs. Manage. 14,
289–299.
Gillespie, M., Melby, V., 2003. Burnout among nursing staff in accident
and emergencyand acute medicine: a comparativestudy. J. Clin.
Nurs. 12, 842–851.
Goalder,N., Schultz, L., 2008. Mental health nurse burnout and stress:
options for prevention.Handover1, 35–38.
Halbesleben,J.R.B., Wakefield, B.J., Wakefield, D.S., Cooper, L.B., 2008.
Nurse burnout and patientsafetyoutcomes:nurse safetyperception
versusreporting behavior.West. J. Nurs. Res.30, 560–577.
Hasselhorn,H., Tackenberg,P., Mu¨ller, B., 2003.Working Conditionsand
Intent to Leavethe Professionamong Nursing Staff in Europe. Na-
tional Institute for Working Life, Stockholm.
Ha¨usser,J., Mojzisch, A., Niesel,M., Schulz-Hardt,S.,2010.Ten yearson: a
review of recent research on the Job Demand-Control(-Support)
Model and psychologicalwell-being. Work Stress24, 1–35.
Helps, S., 1997. Experiencesof stressin accidentand emergencynurses.
Accid. Emerg.Nurs. 5, 48–53.
Hooper,C.,Craig,J., Janvrin, D., Wetsel,M., Reimels,E., 2010.Compassion
satisfaction, burnout, and compassion fatigue among emergency
nursescomparedwith nurses in other selectedinpatient specialties.
J. Emerg.Nurs. 36, 420–427.
Houtman, I., Schaufeli,W., Taris, T., 2000. PsychischeVermoeidheiden
Werk. Samson,Alphen a/d Rijn.
Iacovides, A., Fountoulakis, K., Moysidou, C., Ierodiakonou, C., 1999.
Burnout in nursing staff: is there a relationshipbetweendepression
and burnout? Int. J. PsychiatryMed. 29, 421–433.
Imai, H., Nakao,H., Tsuchiya,M., Kuroda,Y., Katoh,T., 2004.Burnout and
work environmentsof public healthnursesinvolvedin mentalhealth
care.Occup.Environ. Med. 61, 764–768.
Kant, I., Jansen, N., Van Amelsfoort, L., Mohren, D., Swaen, G., 2004.
Burnout in de werkendebevolking? resultatenvan de Maastrichtse
Cohort Studie. (Burnout Among the Working Population.Results of
the Maastricht Cohort Study). Gedragen Organisatie17, 5–17.
Karasek,R.,Theorell,T., 1990.HealthyWork: Stress,Productivity,and the
Reconstructionof Working Life. Basic Books,New-York, NY.
Kipping, C., 2000. Stressin mental health nursing. Int. J. Nurs. Stud. 37,
207–218.
LahrKeller,K., 1990.The managementof stressand preventionof burnout
in emergencynurses.J. Emerg.Nurs. 16, 90–96.
Langelaan,S.,Bakker,A.B.,Schaufeli,W., Van Rhenen,W., Van Doornen,L.,
2007.Is butnoutrelatedto allostaticload? Int. J. Behav.Med. 14, 213–
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx12
validity of thesesuggestions.
Conflict of interest
No conflict of interest has been declared by the
author(s).
Funding statement
This research received no specific grant from any
fundingagencyin the public, commercial,or not-for-profit
sectors.
References
Adali, E., Priami, M., 2002.Burnout amongnursesin intensivecare units,
internal medicinewards and emergencydepartmentsin Greek hos-
pitals. ICUs Nurs. Web J. 1–19 (ISSN 1108-7366).
Ahola, K., Toppinen-Tanner,S., Huuhtanen,P., Koskinen,A., Va¨na¨nen, A.,
2009. Occupationalburnout and chronic work disability: an eight
year cohort study on pensioningamongFinish forest industry work-
ers. J. AffectiveDis. 115, 150–159.
Aiken,L., Clarke,S.,Sloane,D., Sochalski,J., Silber,J., 2002.Hospital nurse
staffing and patient mortality, nurse burnout, and job satisfaction.
JAMA 288, 1987–1993.
Alexander,D., Klein, S.,2001.Impact of accidentand emergencywork on
mentalhealthand emotionalwell-being.Br. J. Psychiatry178, 76–81.
Ariapooran,S., 2014. Compassionfatigueand burnout in Iranian nurses:
the role of perceivedsocialsupport.Iran. J. Nurs.Midwifery Res.19 (3)
279–284.
Aromaa,A., Koskinen,S.,2004.Health and FunctionalCapacityin Finland:
BaselineResults of the Health 2000 ExaminationsSurvey. KTL-Na-
tional Public Health Institute,Helsinki.
Bakker, A., Demerouti, E., Euwema, M., 2005. Job resources buffer
the impact of job demands on burnout. J. Occup. Health Psychol.
10, 170–180.
Bakker,A., Van der Zee,K., Lewig, K., Dollard, M., 2006. The relationship
betweenthe big five personalityfactorsand burnout: a study among
volunteercounselors.J. Soc. Psychol.146, 31–50.
Ball,J., Pike,G.,Griffiths,P., Rafferty,A., Murrells, T.,2012.RN4CASTNurse
Surveyin England.King’s CollegeLondon,London.
Bernaldo-De-Quiros,M., Piccini, A.T., Gomez,M.M., Cerdeira,J.C., 2014.
Psychologicalconsequencedof aggressionin pre-hospitalemergency
care: cross sectionalsurvey.Int. J. Nurs. Stud.,[Epub aheadof print].
Borritz,M., Rugulies,R.,Christensen,K., Villadsen,E., Kristensen,T., 2006.
Burnout as a predictor of self-reported sickness absence among
human serviceworkers: prospectivefindings from three year follow
up of the PUMA study. Occup.Environ. Med. 63, 98–106.
Brenninkmeijer,V., Van Yperen, N., 2003. How to conduct researchon
burnout: advantages and disadvantages of an unidimensional
approachto burnout. Occup.Environ. Med. 60, 16–21.
Browning, L., Ryan, C., Thomas, S., Greenberg,M., Rolniak, S., 2007.
Escriba`-Agu¨ir, V., Martin-Baena,D., Pe´rez-Hoyos, S., 2006. Psychosocial
work environment and burnout among emergency medical and
nursing staff. Int. Arch. Occup.Environ. Health 80, 127–133.
Escriba-Agu¨ir, V., Pe´rez-Hoyos, S., 2007. Psychologicalwell-being and
psychosocialwork environment characteristicsamong emergency
medical and nursing staff. StressHealth 23, 153–160.
Flynn, L., Thomas-Hawkins,C., Clarke,S.,2009.Organizationaltraits,care
processes,and burnout amongchronic hemodialysisnurses.West. J.
Nurs. Res. 31, 569–582.
Freudenberger,H., 1974. Staff burn-out. J. Soc. Issues30, 159–165.
Gaines,J., Jermier,J., 1983.Emotionalexhaustionin a high stressorgani-
zation. Acad. Manage.J. 26, 567–586.
Garcia-Izquierdo,M., Rios-Risquez,M., 2012. The relationship between
psychosocialjob stress and burnout in emergencydepartment:an
exploratorystudy. Nurs. Outlook 60, 322–329.
Gates,D., Gillespie, G., Succop,P., 2011. Violence againstnurses and its
impact on stressand productivity.Nurs. Econ. 29, 59–67.
Gelsema, T., Van der Doef, M., Maes, S., Janssen, M., Akerboom, S.,
Verhoeven, C., 2006. A longitudinal study of job stress in the
nursing profession: causesand consequences.J. Nurs. Manage. 14,
289–299.
Gillespie, M., Melby, V., 2003. Burnout among nursing staff in accident
and emergencyand acute medicine: a comparativestudy. J. Clin.
Nurs. 12, 842–851.
Goalder,N., Schultz, L., 2008. Mental health nurse burnout and stress:
options for prevention.Handover1, 35–38.
Halbesleben,J.R.B., Wakefield, B.J., Wakefield, D.S., Cooper, L.B., 2008.
Nurse burnout and patientsafetyoutcomes:nurse safetyperception
versusreporting behavior.West. J. Nurs. Res.30, 560–577.
Hasselhorn,H., Tackenberg,P., Mu¨ller, B., 2003.Working Conditionsand
Intent to Leavethe Professionamong Nursing Staff in Europe. Na-
tional Institute for Working Life, Stockholm.
Ha¨usser,J., Mojzisch, A., Niesel,M., Schulz-Hardt,S.,2010.Ten yearson: a
review of recent research on the Job Demand-Control(-Support)
Model and psychologicalwell-being. Work Stress24, 1–35.
Helps, S., 1997. Experiencesof stressin accidentand emergencynurses.
Accid. Emerg.Nurs. 5, 48–53.
Hooper,C.,Craig,J., Janvrin, D., Wetsel,M., Reimels,E., 2010.Compassion
satisfaction, burnout, and compassion fatigue among emergency
nursescomparedwith nurses in other selectedinpatient specialties.
J. Emerg.Nurs. 36, 420–427.
Houtman, I., Schaufeli,W., Taris, T., 2000. PsychischeVermoeidheiden
Werk. Samson,Alphen a/d Rijn.
Iacovides, A., Fountoulakis, K., Moysidou, C., Ierodiakonou, C., 1999.
Burnout in nursing staff: is there a relationshipbetweendepression
and burnout? Int. J. PsychiatryMed. 29, 421–433.
Imai, H., Nakao,H., Tsuchiya,M., Kuroda,Y., Katoh,T., 2004.Burnout and
work environmentsof public healthnursesinvolvedin mentalhealth
care.Occup.Environ. Med. 61, 764–768.
Kant, I., Jansen, N., Van Amelsfoort, L., Mohren, D., Swaen, G., 2004.
Burnout in de werkendebevolking? resultatenvan de Maastrichtse
Cohort Studie. (Burnout Among the Working Population.Results of
the Maastricht Cohort Study). Gedragen Organisatie17, 5–17.
Karasek,R.,Theorell,T., 1990.HealthyWork: Stress,Productivity,and the
Reconstructionof Working Life. Basic Books,New-York, NY.
Kipping, C., 2000. Stressin mental health nursing. Int. J. Nurs. Stud. 37,
207–218.
LahrKeller,K., 1990.The managementof stressand preventionof burnout
in emergencynurses.J. Emerg.Nurs. 16, 90–96.
Langelaan,S.,Bakker,A.B.,Schaufeli,W., Van Rhenen,W., Van Doornen,L.,
2007.Is butnoutrelatedto allostaticload? Int. J. Behav.Med. 14, 213–
G Model
NS-2472;No. of Pages13
J. Adriaenssenset al./ InternationalJournal of NursingStudiesxxx (2014)xxx–xxx12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.