Comprehensive Case Study: C2 Fracture Diagnosis and Management
VerifiedAdded on 2020/02/05
|17
|3326
|125
Case Study
AI Summary
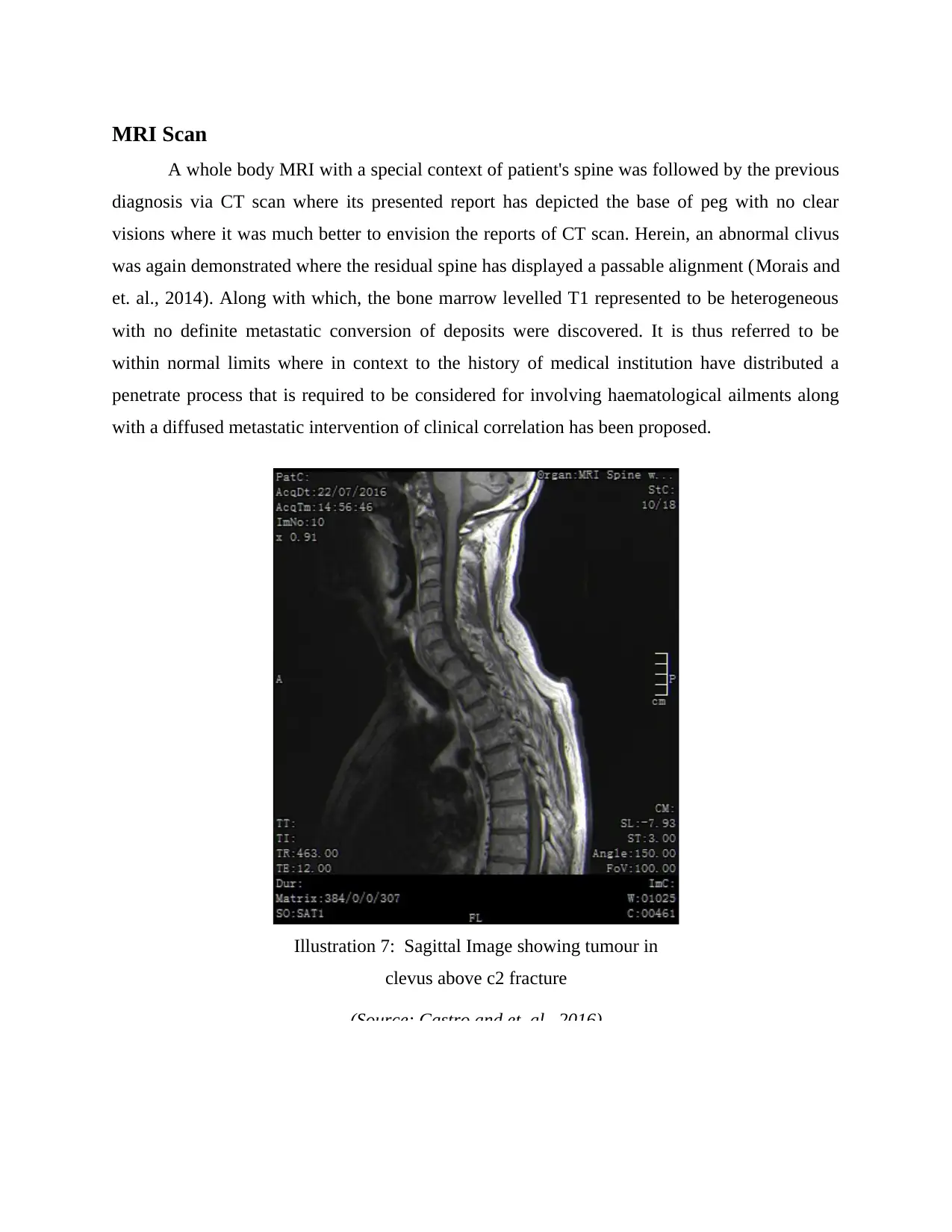
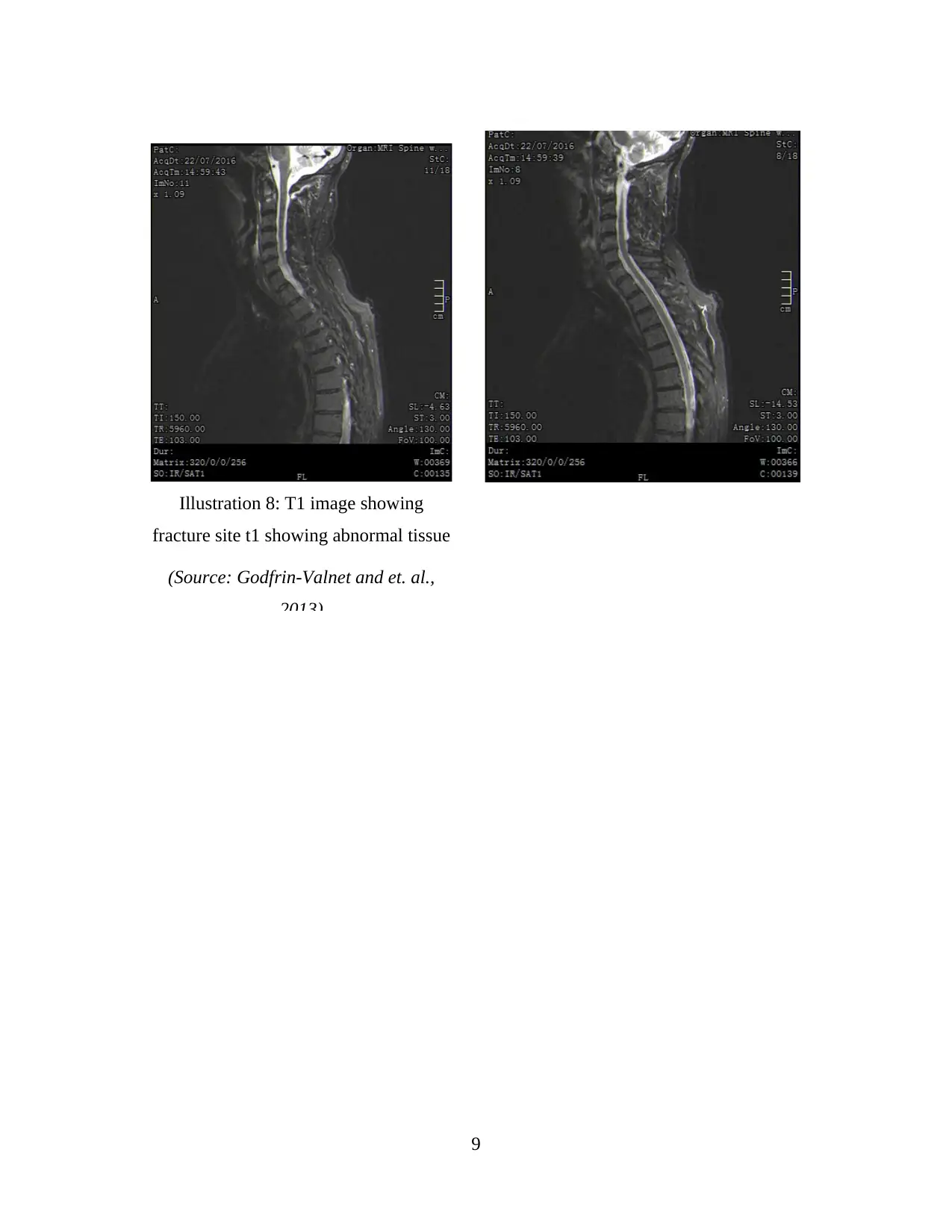
This case study examines the case of a 67-year-old male presenting with a C2 fracture, detailing the anatomy and physiology of the cervical spine. The assignment explores the aetiology of the injury, focusing on the patient's fall and subsequent symptoms like neck pain and numbness. It then delves into the diagnostic process, including non-imaging tests and detailed analysis of imaging results from X-rays, CT scans, and MRI scans, highlighting the findings of a pathological C2 fracture and cancerous penetration. The study further discusses treatment options, including palliative care, surgical methods (direct lateral mass screws), and follow-up procedures. Patient management pathways and relevant medical guidelines are also addressed to provide a comprehensive understanding of the case. The case study emphasizes the importance of prompt diagnosis and appropriate treatment for C2 fractures to prevent further complications and improve patient outcomes.


1 out of 17
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.