Case Study: Calcific Uremic Arteriolopathy, Haemodialysis & Treatment
VerifiedAdded on 2023/03/20
|5
|682
|59
Case Study
AI Summary
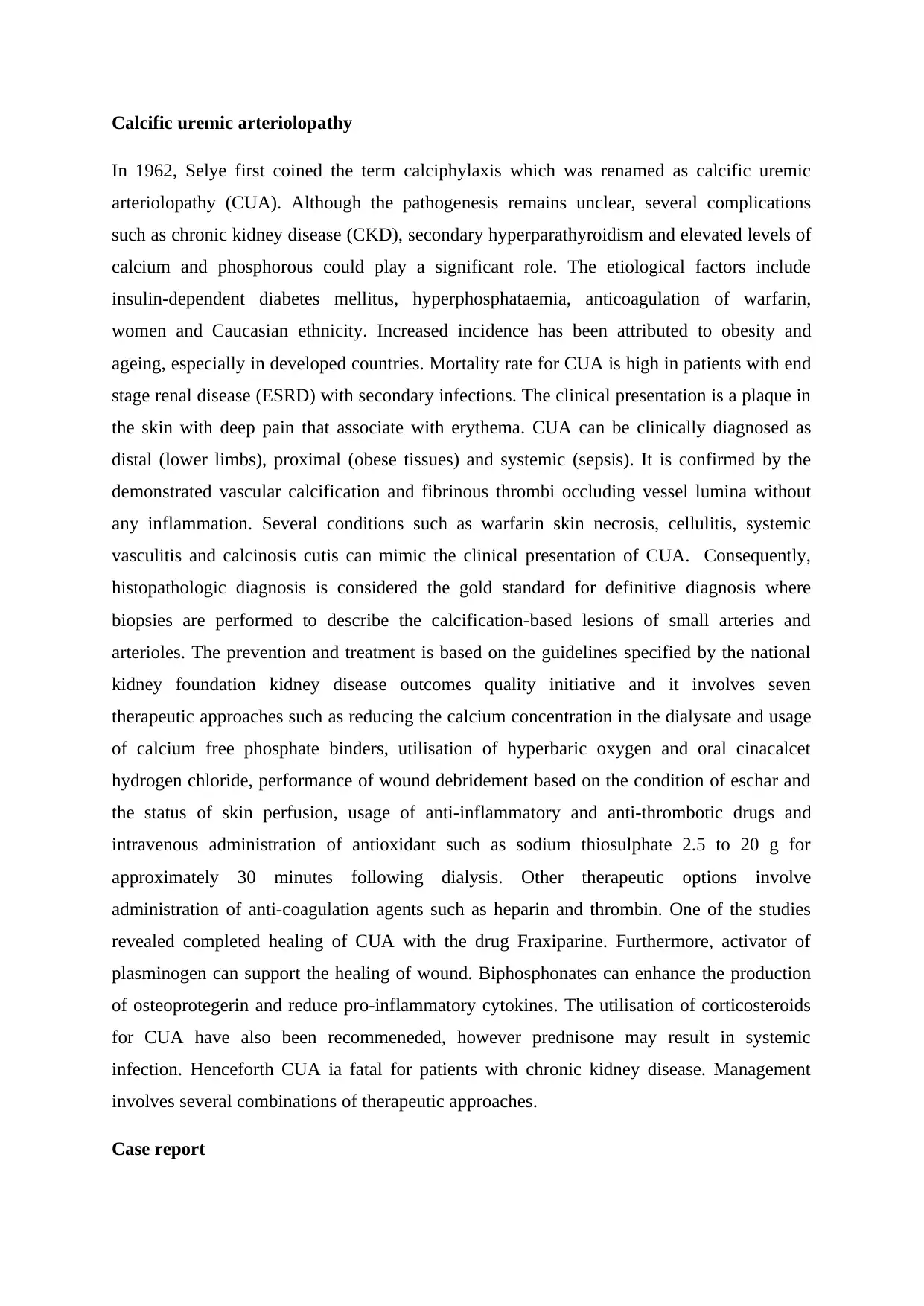
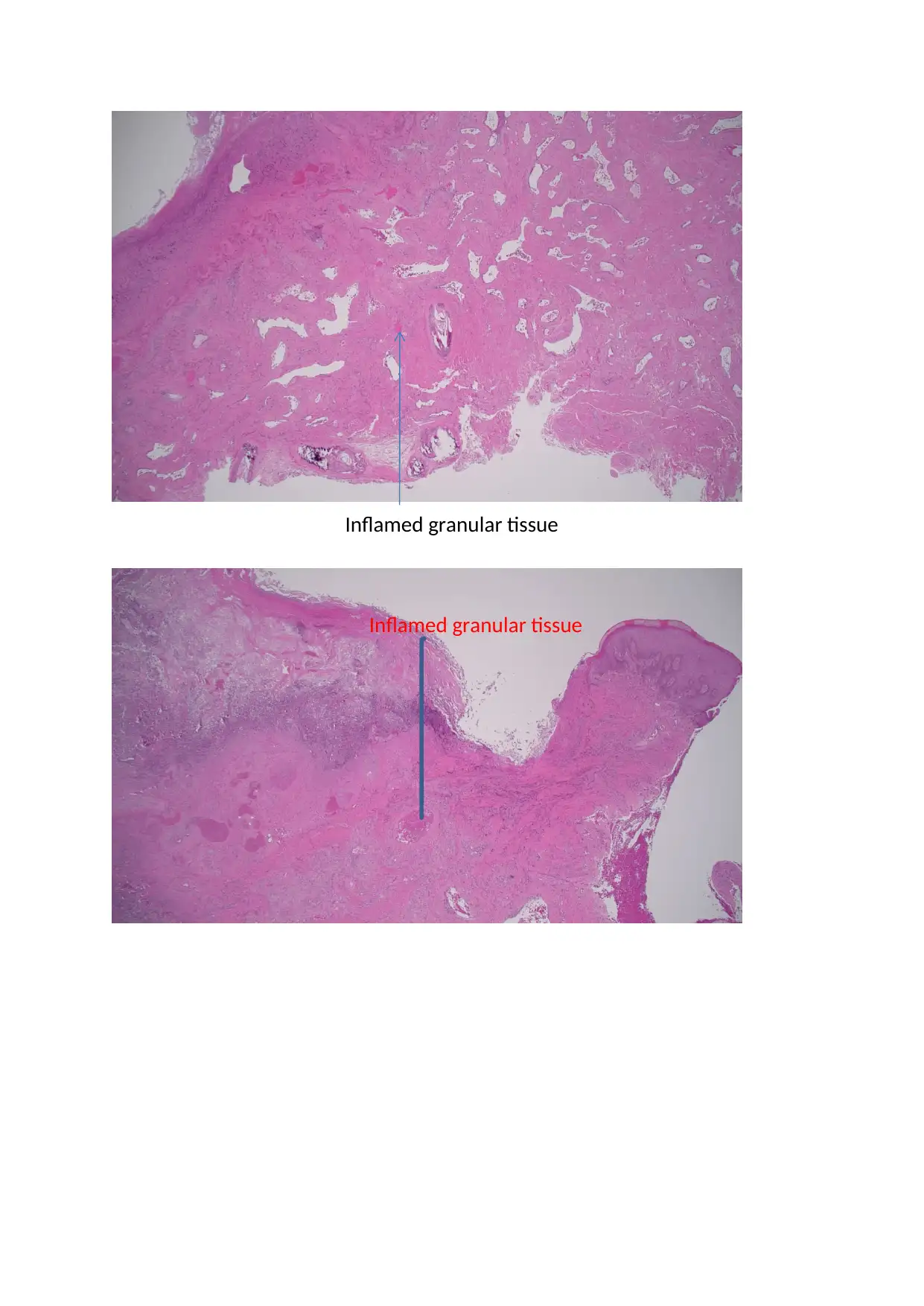
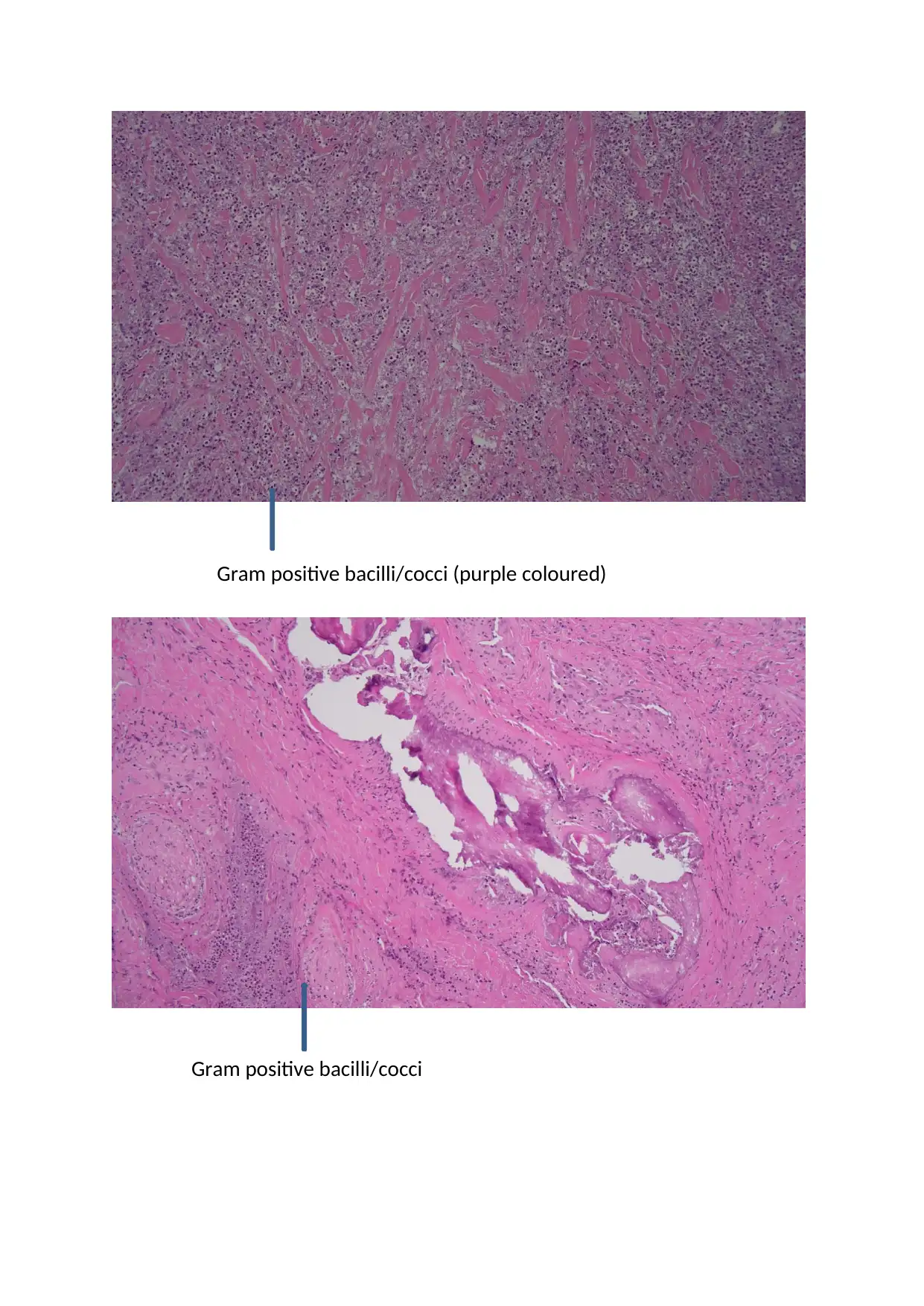
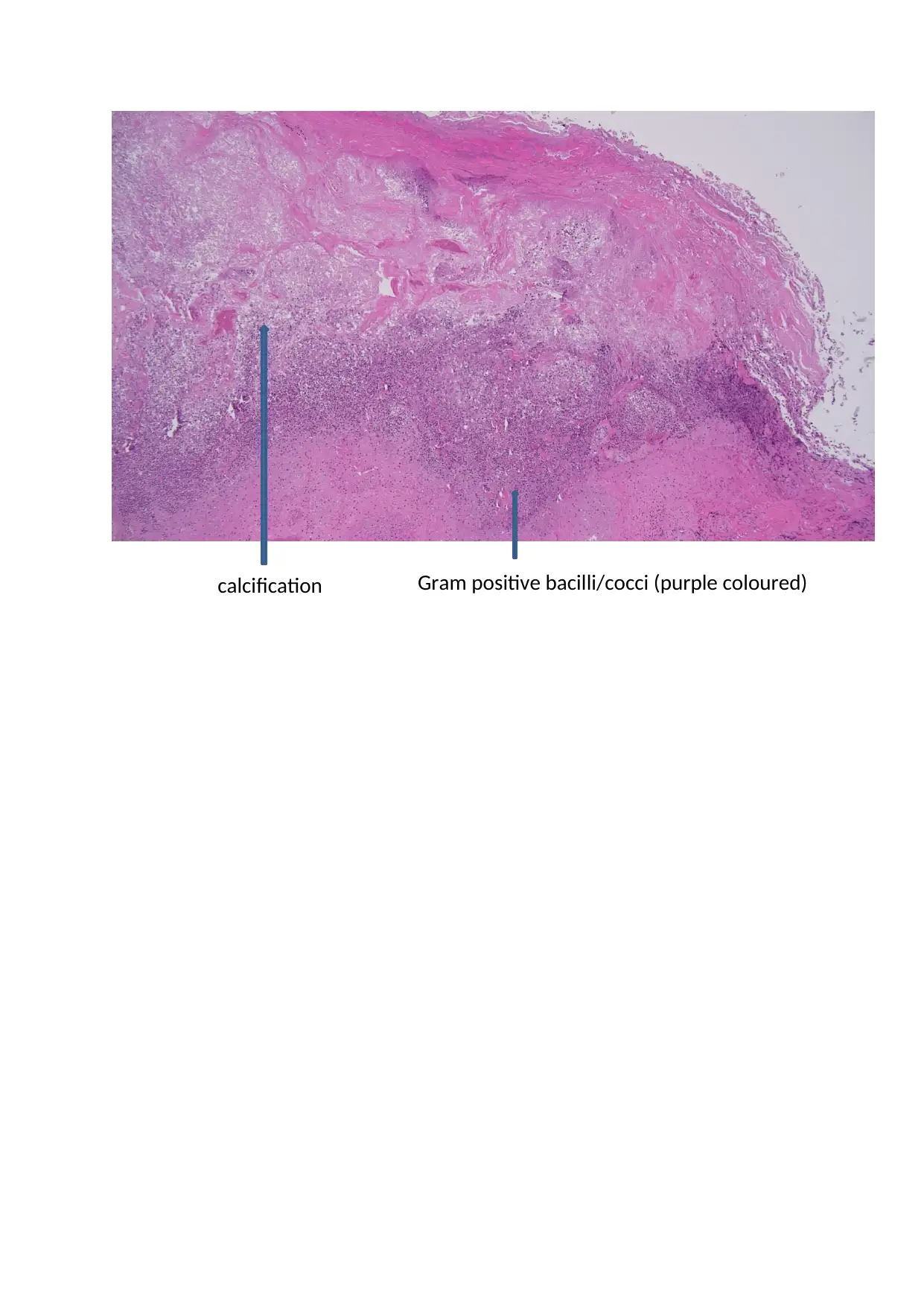
This case study examines a 62-year-old patient with end-stage renal failure (ESRF) on chronic haemodialysis who presented with a non-healing penile ulcer, ultimately diagnosed as calcific uremic arteriolopathy (CUA). The patient had a history of poor compliance with dialysis and medications, leading to multiple hospital visits. The presentation included severe pain and necrotic tissue, but the STD screen was negative. Treatment involved pain management with fentanyl and ketamine, wound debridement, and the administration of intravenous sodium thiosulphate and calcium-free phosphate binders. The patient responded positively to treatment, with pain reduction and ulcer healing. The case highlights the challenges of managing CUA, a condition associated with high mortality, and demonstrates the effectiveness of sodium thiosulphate in this context. The provided histology slides and the clinical presentation were consistent with the diagnosis of calciphylaxis.

1 out of 5


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.