University: HSN702 Lifespan Nutrition - Calcium Intake Analysis Report
VerifiedAdded on 2022/10/10
|16
|4119
|231
Report
AI Summary
This report analyzes calcium intake among Australian children and adolescents, focusing on data from the National Nutrition and Physical Activity Survey (NNPAS). It examines the limitations of the Automated Multiple Pass Method (AMPM) used for dietary data collection, highlighting issues like underreporting and bias. The report compares calcium intake levels to Nutrient Reference Values (NRVs), revealing deficiencies, particularly in the 12-18 age group. The report discusses the health consequences of inadequate calcium intake, including bone health issues. The report then reviews peer-reviewed literature, including cross-sectional and cohort studies, to assess the relationship between calcium intake and health outcomes. Finally, the report provides evidence-based solutions, recommending calcium-rich foods, vitamin D intake, and physical activity to improve calcium absorption and overall health. The report also includes a discussion on alternative calcium sources for individuals with dietary restrictions and allergies. A one-minute audio transcript summarizing the health implications of current calcium intake levels is also included, along with a reflective journal upon completion of this task.

Running head: LIFESPAN NUTRITION
LIFESPAN NUTRITION
Name of the Student:
Name of the University:
Author note:
LIFESPAN NUTRITION
Name of the Student:
Name of the University:
Author note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1LIFESPAN NUTRITION
Part A: Written Assignment
Question 1
A 24 hour dietary recall has been used for collection of dietary data, which has been
emphasized as the Automated Multiple Pass Method (AMPM) [1]. Such dietary data collection
method is advantageous since it is easy to understand by individuals with non-clinical
backgrounds for whom complicated scientific terms may seem as medical jargon. Dietary recalls
like the AMPM are effective since they help individuals to select their patterns of food and
beverage consumption using multiple lists of food quantities, food product types and meal
consumption patterns [2].
However, 24 hour dietary recalls are prone to extensive limitations. A major disadvantage
of 24 hour dietary recalls is the high risk of participants forgetting their beverage and food
consumption. Due to forgetfulness, individuals are prone to providing incorrect details of their
consumption resulting in ‘underreporting’ [3]. It must be noted that dietary data on calcium
consumption of young populations like children in the age group of 2 years in the Australian
Health Survey are susceptible to inaccuracies as a result of underreporting and forgetfulness.
However, to prevent the possibilities of incorrect responses due to the same, the Australian
Bureau of Statistics, ensured that such children were accompanied by their parents. It was
however, also noted in the NNPAS report that even parents may be subject to forgetfulness of
their child’s intake of food and may also lack awareness of their children’s consumption of food
in external environments other than their home [4].
Part A: Written Assignment
Question 1
A 24 hour dietary recall has been used for collection of dietary data, which has been
emphasized as the Automated Multiple Pass Method (AMPM) [1]. Such dietary data collection
method is advantageous since it is easy to understand by individuals with non-clinical
backgrounds for whom complicated scientific terms may seem as medical jargon. Dietary recalls
like the AMPM are effective since they help individuals to select their patterns of food and
beverage consumption using multiple lists of food quantities, food product types and meal
consumption patterns [2].
However, 24 hour dietary recalls are prone to extensive limitations. A major disadvantage
of 24 hour dietary recalls is the high risk of participants forgetting their beverage and food
consumption. Due to forgetfulness, individuals are prone to providing incorrect details of their
consumption resulting in ‘underreporting’ [3]. It must be noted that dietary data on calcium
consumption of young populations like children in the age group of 2 years in the Australian
Health Survey are susceptible to inaccuracies as a result of underreporting and forgetfulness.
However, to prevent the possibilities of incorrect responses due to the same, the Australian
Bureau of Statistics, ensured that such children were accompanied by their parents. It was
however, also noted in the NNPAS report that even parents may be subject to forgetfulness of
their child’s intake of food and may also lack awareness of their children’s consumption of food
in external environments other than their home [4].
2LIFESPAN NUTRITION
However, considering the possibilities of all these errors, the ABS implemented a
comprehensive and specialized 24 dietary recall method known as the Automated Multiple Pass
Method (AMPM). The AMPM has been formulated by the United States Department of
Agriculture (USDA) and comprises of five sections or phases, requiring respondents to
remember their beverage and food consumption with the help of extensive lists of meal times,
quick and detailed food product databases along with repeated questioning and guidance by the
interviewer [1]. Incorporating specialized and comprehensive dietary recalls like the AMPM is
advantageous and was exclusively executed by the ABS to mitigate every possible limitation of
such dietary data collection methods [5].
Despite the efficiencies of the AMPM, there is no alternative to combat bias – an
additional major limitation of 24 hour dietary recalls. Families or adolescents are likely to
purposefully answer recalls questions incorrectly in order to project how ‘healthy’ their diets are
[6]. The ABS, in fact, has emphasizes that all the obtained dietary information are largely reliant
on participant answers and opinions and thus, may be still be highly bias, incorrect and
underreported. Thus, it can be postulated that the ABS’s usage of a 24 hour dietary recall in its
NNPAS survey may be subject to inaccuracies due to extensive possibility of underreporting,
bias and forgetfulness of its selected participants [4].
However, considering the possibilities of all these errors, the ABS implemented a
comprehensive and specialized 24 dietary recall method known as the Automated Multiple Pass
Method (AMPM). The AMPM has been formulated by the United States Department of
Agriculture (USDA) and comprises of five sections or phases, requiring respondents to
remember their beverage and food consumption with the help of extensive lists of meal times,
quick and detailed food product databases along with repeated questioning and guidance by the
interviewer [1]. Incorporating specialized and comprehensive dietary recalls like the AMPM is
advantageous and was exclusively executed by the ABS to mitigate every possible limitation of
such dietary data collection methods [5].
Despite the efficiencies of the AMPM, there is no alternative to combat bias – an
additional major limitation of 24 hour dietary recalls. Families or adolescents are likely to
purposefully answer recalls questions incorrectly in order to project how ‘healthy’ their diets are
[6]. The ABS, in fact, has emphasizes that all the obtained dietary information are largely reliant
on participant answers and opinions and thus, may be still be highly bias, incorrect and
underreported. Thus, it can be postulated that the ABS’s usage of a 24 hour dietary recall in its
NNPAS survey may be subject to inaccuracies due to extensive possibility of underreporting,
bias and forgetfulness of its selected participants [4].
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3LIFESPAN NUTRITION
Question 2
Table 1: Mean Intake of Calcium in Australian children and adolescents as compared to
Nutrient Reference Values (NRVs)
Mean Intake
of Calcium
(mg/day):
2-3 years
Mean Intake
of Calcium
(mg/day):
4-8 years
Mean Intake
of Calcium
(mg/day):
9-11 years
Mean
Intake of
Calcium
(mg/day):
12-13
years
Mean Intake
of Calcium
(mg/day):
14-18 years
Boys 775.0 805.1 866 945 924.6
Girls 768.3 675.8 805 907 740.7
Total (boys
and girls)
771.8 742.6 853.4 853.4 833.4
EAR value 360 (males
and females)
520 (males
and females)
800 (males
and females)
1050
(males
and
females)
1050 (males
and females)
RDI value 500 (males
and females)
700 (males
and females)
1000 (males
and females)
1300
(males
and
females)
1300 (males
and females)
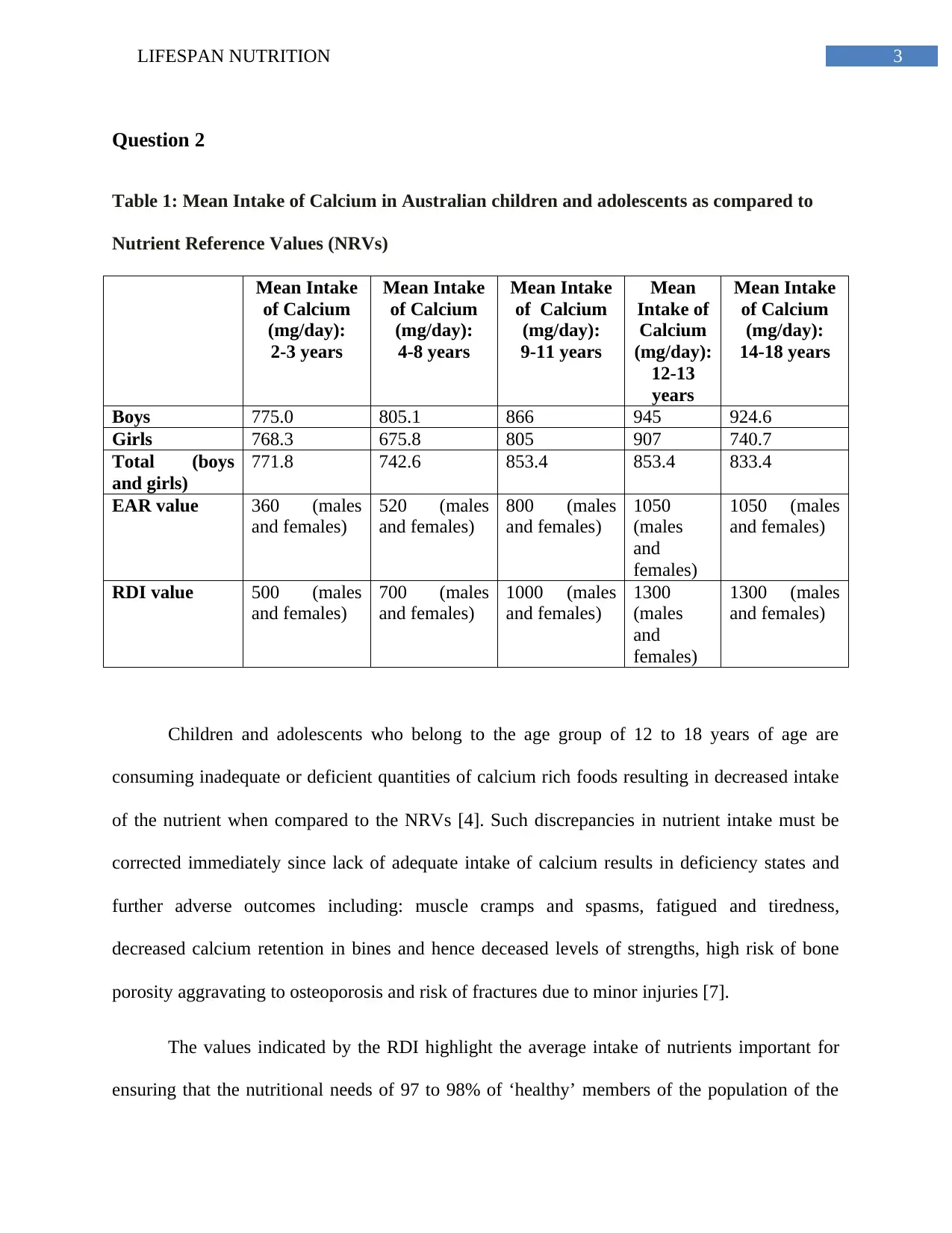
Children and adolescents who belong to the age group of 12 to 18 years of age are
consuming inadequate or deficient quantities of calcium rich foods resulting in decreased intake
of the nutrient when compared to the NRVs [4]. Such discrepancies in nutrient intake must be
corrected immediately since lack of adequate intake of calcium results in deficiency states and
further adverse outcomes including: muscle cramps and spasms, fatigued and tiredness,
decreased calcium retention in bines and hence deceased levels of strengths, high risk of bone
porosity aggravating to osteoporosis and risk of fractures due to minor injuries [7].
The values indicated by the RDI highlight the average intake of nutrients important for
ensuring that the nutritional needs of 97 to 98% of ‘healthy’ members of the population of the
Question 2
Table 1: Mean Intake of Calcium in Australian children and adolescents as compared to
Nutrient Reference Values (NRVs)
Mean Intake
of Calcium
(mg/day):
2-3 years
Mean Intake
of Calcium
(mg/day):
4-8 years
Mean Intake
of Calcium
(mg/day):
9-11 years
Mean
Intake of
Calcium
(mg/day):
12-13
years
Mean Intake
of Calcium
(mg/day):
14-18 years
Boys 775.0 805.1 866 945 924.6
Girls 768.3 675.8 805 907 740.7
Total (boys
and girls)
771.8 742.6 853.4 853.4 833.4
EAR value 360 (males
and females)
520 (males
and females)
800 (males
and females)
1050
(males
and
females)
1050 (males
and females)
RDI value 500 (males
and females)
700 (males
and females)
1000 (males
and females)
1300
(males
and
females)
1300 (males
and females)
Children and adolescents who belong to the age group of 12 to 18 years of age are
consuming inadequate or deficient quantities of calcium rich foods resulting in decreased intake
of the nutrient when compared to the NRVs [4]. Such discrepancies in nutrient intake must be
corrected immediately since lack of adequate intake of calcium results in deficiency states and
further adverse outcomes including: muscle cramps and spasms, fatigued and tiredness,
decreased calcium retention in bines and hence deceased levels of strengths, high risk of bone
porosity aggravating to osteoporosis and risk of fractures due to minor injuries [7].
The values indicated by the RDI highlight the average intake of nutrients important for
ensuring that the nutritional needs of 97 to 98% of ‘healthy’ members of the population of the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4LIFESPAN NUTRITION
country are met adequately. In comparison to the same, values indicated by the EAR demonstrate
requirements of nutrients which are optimal for addressing nutritional requirements of half of the
country’s ‘healthy’ population [8]. When nutrient intake values postulated as per EAR are not
accomplished, it indicates that the concerned individuals are at high risk of being deficient in that
nutrient and thus, demonstrates the need for improving or altering their respective diets. Values
emphasized by the EAR demonstrate far greater accuracy since they are indicative of the
minimal nutrient quantities required to ensure that a population is free from deficiency. In
comparison to the same, values represented by the RDI are indicative only of a mean value of
nutrient consumption which must be maintained to ensure adequate health status of the entire
population of the nation [9].
Question 3
For the purpose of obtaining of peer reviewed, scholarly and academic literature on the
intake of calcium and outcomes of health among children and adolescents in Australia, an
electronic screening of literature was performed with the assistance of keywords like
‘adolescents’, ‘children’, ‘health’, ‘calcium’ and ‘outcomes’ along with Boolean operators [10].
1. The cross sectional study by [11] researched on the impact of calcium consumption on
links between concentrations of parathyroid hormone (PTH) and serum 25-
hydroxyvitamin D3 (250HD) across 181 Indian adolescents (10 to 14 years) from 2012 to
2014. A 24 hour dietary recall was utilized for reporting calcium intake while
microparticle immunoassays were used to investigate 250HD and PTH concentrations.
Lower PTH and 250HD concentrations were observed across adolescents with calcium
consumption above median of 520 mg/day and vice versa for calcium intake below the
median. While this study provided key insights on the effects of PTH due to calcium
country are met adequately. In comparison to the same, values indicated by the EAR demonstrate
requirements of nutrients which are optimal for addressing nutritional requirements of half of the
country’s ‘healthy’ population [8]. When nutrient intake values postulated as per EAR are not
accomplished, it indicates that the concerned individuals are at high risk of being deficient in that
nutrient and thus, demonstrates the need for improving or altering their respective diets. Values
emphasized by the EAR demonstrate far greater accuracy since they are indicative of the
minimal nutrient quantities required to ensure that a population is free from deficiency. In
comparison to the same, values represented by the RDI are indicative only of a mean value of
nutrient consumption which must be maintained to ensure adequate health status of the entire
population of the nation [9].
Question 3
For the purpose of obtaining of peer reviewed, scholarly and academic literature on the
intake of calcium and outcomes of health among children and adolescents in Australia, an
electronic screening of literature was performed with the assistance of keywords like
‘adolescents’, ‘children’, ‘health’, ‘calcium’ and ‘outcomes’ along with Boolean operators [10].
1. The cross sectional study by [11] researched on the impact of calcium consumption on
links between concentrations of parathyroid hormone (PTH) and serum 25-
hydroxyvitamin D3 (250HD) across 181 Indian adolescents (10 to 14 years) from 2012 to
2014. A 24 hour dietary recall was utilized for reporting calcium intake while
microparticle immunoassays were used to investigate 250HD and PTH concentrations.
Lower PTH and 250HD concentrations were observed across adolescents with calcium
consumption above median of 520 mg/day and vice versa for calcium intake below the
median. While this study provided key insights on the effects of PTH due to calcium
5LIFESPAN NUTRITION
consumption, the low sample size and usage of cross sectional design and dietary recalls
are a major limitation in terms of bias. An additional limitation was the lack of usage of
tandem mass spectrometry – the gold standard in measurement of vitamin D.
2. The cross sectional study by [12] evidenced the association between calcium
consumption and body mass index (BMI) across 1570 children from Thailand, aged 6 to
12 years. Calcium intake was assessed using food frequency and 24 hour dietary recall
questionnaires. Skinfold thickness, body height and weight and sitting height were
measured. A low consumption of calcium was linked with higher BMI and skinfold
thickness using General Linear Model. The large sample size and wide range of age
group can be considered major strengths of this study. However the lack of blinding due
to cross sectional designs along with usage of dietary recalls was a major limitation in
terms of high prevalence of bias.
3. The cross sectional study by [13] assessed the relationship calcium consumption and
blood pressure across 347 children from Brazil within ages 8 to 9. Blood pressure was
recorded along with calcium intake using three dietary recalls. An estimated 93.6% were
deficient in calcium intake. Higher diastolic (p = 0.047) and systolic (p = 0.041 blood
pressures were observed across children with inadequate calcium intake. A cross
sectional research design with small sample size and without blinding is a major
limitation in terms of reliability and validity. The usage of a dietary recall further
increases susceptibility of bias. However, repeated dietary recalls along with
comprehensive information on the impact of calcium on blood pressures were major
strengths of this study.
consumption, the low sample size and usage of cross sectional design and dietary recalls
are a major limitation in terms of bias. An additional limitation was the lack of usage of
tandem mass spectrometry – the gold standard in measurement of vitamin D.
2. The cross sectional study by [12] evidenced the association between calcium
consumption and body mass index (BMI) across 1570 children from Thailand, aged 6 to
12 years. Calcium intake was assessed using food frequency and 24 hour dietary recall
questionnaires. Skinfold thickness, body height and weight and sitting height were
measured. A low consumption of calcium was linked with higher BMI and skinfold
thickness using General Linear Model. The large sample size and wide range of age
group can be considered major strengths of this study. However the lack of blinding due
to cross sectional designs along with usage of dietary recalls was a major limitation in
terms of high prevalence of bias.
3. The cross sectional study by [13] assessed the relationship calcium consumption and
blood pressure across 347 children from Brazil within ages 8 to 9. Blood pressure was
recorded along with calcium intake using three dietary recalls. An estimated 93.6% were
deficient in calcium intake. Higher diastolic (p = 0.047) and systolic (p = 0.041 blood
pressures were observed across children with inadequate calcium intake. A cross
sectional research design with small sample size and without blinding is a major
limitation in terms of reliability and validity. The usage of a dietary recall further
increases susceptibility of bias. However, repeated dietary recalls along with
comprehensive information on the impact of calcium on blood pressures were major
strengths of this study.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6LIFESPAN NUTRITION
4. The cohort study by [14] researched links between calcium consumption and adult height
and z scores height-for-age (HAZ) across 2019 Chinese adolescents. Mean calcium
intake was 355 mg/day in girls and 426mg/day in boys. After a 7 year follow up, girls
achieved 158.5 cm and boys 169 cm of height. Methods of non-linear regression revealed
shorter statures across boys with calcium consumption less than 327 mg/day. The large
sample size and extensive follow up period are major strengths of this study in terms of
reliability and validity. However, the lack of information on younger populations and
effect of calcium on additional anthropometric parameter hinder the applicability of this
study in terms of lack of information on calcium intake and anthropometric
measurements for growth.
5. The systematic review of randomized controlled trials by [15] investigated relationship
between mineral content in bones and consumption of dairy products in children. A total
of 13 randomized controlled trials were reviewed. A significant enhancement in bone
mineral content due to dairy product intake was observed by the authors. There was
inconclusive details on links between linear growth and dairy intake. Performing a
systematic review of randomized controlled trials was a major strength of this paper since
such a research design has been implicated to be one of the strongest forms of evidence.
However the lack of primary data collection and presence of inconclusive papers hinders
the validity of this paper in terms of publication bias. Further, the lack of information on
non-dairy calcium sources on bone mineral health is a limitation in terms of applicability.
Question 4
A number of evidence based solutions have been recommended:
4. The cohort study by [14] researched links between calcium consumption and adult height
and z scores height-for-age (HAZ) across 2019 Chinese adolescents. Mean calcium
intake was 355 mg/day in girls and 426mg/day in boys. After a 7 year follow up, girls
achieved 158.5 cm and boys 169 cm of height. Methods of non-linear regression revealed
shorter statures across boys with calcium consumption less than 327 mg/day. The large
sample size and extensive follow up period are major strengths of this study in terms of
reliability and validity. However, the lack of information on younger populations and
effect of calcium on additional anthropometric parameter hinder the applicability of this
study in terms of lack of information on calcium intake and anthropometric
measurements for growth.
5. The systematic review of randomized controlled trials by [15] investigated relationship
between mineral content in bones and consumption of dairy products in children. A total
of 13 randomized controlled trials were reviewed. A significant enhancement in bone
mineral content due to dairy product intake was observed by the authors. There was
inconclusive details on links between linear growth and dairy intake. Performing a
systematic review of randomized controlled trials was a major strength of this paper since
such a research design has been implicated to be one of the strongest forms of evidence.
However the lack of primary data collection and presence of inconclusive papers hinders
the validity of this paper in terms of publication bias. Further, the lack of information on
non-dairy calcium sources on bone mineral health is a limitation in terms of applicability.
Question 4
A number of evidence based solutions have been recommended:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7LIFESPAN NUTRITION
Adolescents and children of Australia are recommended to consume foods rich in
calcium which include, cheese, low fat milk and associated dairy products or beverages.
For families with intolerances and allergies associated with dairy, alternatives for dairy
must be consumed such as cereal of soy beverages and milk products, as well as seeds,
nuts and soy products like tofu. Consuming these food products must be aligned with
recommended serving sizes as per the Australian Dietary Guidelines, that is, 3.5 servings.
This serving size is equal to half cup of evaporated milk and low fat yoghurt, 2 slices of
cheese or 250ml or 1 cup of low fat dairy or alternatives like cereals and soy products
[16].
It has been researched that optimum intake of Vitamin D improves internal calcium
absorption. Thus, children and adolescents across Australia are recommended to ingest
products with commendable Vitamin D amount, which include leafy greens, seeds,
beans, legumes, fishes like salmon and sardine, liver oils of these fishes and nuts [17].
Consumption of dairy will not be feasible solution for families who are engaging in
special dietary practices like veganism, lactose intolerance or allergies. Hence, such
families can choose alternative dairy products equally rich in calcium such as, legumes,
leafy green vegetables, pulses, whole grains or juices which have been fortified, nuts,
seeds and fatty fishes such as salmons and sardines [18].
Engaging in optimum physical activity results in improved absorption of calcium such as
enhanced calcium retention in bones, improved strength of the skeletal system and hence
prevention of fracture and bone injuries in the future [11].It is recommended that
Australian adolescents and children participate in moderate levels of resistance of aerobic
Adolescents and children of Australia are recommended to consume foods rich in
calcium which include, cheese, low fat milk and associated dairy products or beverages.
For families with intolerances and allergies associated with dairy, alternatives for dairy
must be consumed such as cereal of soy beverages and milk products, as well as seeds,
nuts and soy products like tofu. Consuming these food products must be aligned with
recommended serving sizes as per the Australian Dietary Guidelines, that is, 3.5 servings.
This serving size is equal to half cup of evaporated milk and low fat yoghurt, 2 slices of
cheese or 250ml or 1 cup of low fat dairy or alternatives like cereals and soy products
[16].
It has been researched that optimum intake of Vitamin D improves internal calcium
absorption. Thus, children and adolescents across Australia are recommended to ingest
products with commendable Vitamin D amount, which include leafy greens, seeds,
beans, legumes, fishes like salmon and sardine, liver oils of these fishes and nuts [17].
Consumption of dairy will not be feasible solution for families who are engaging in
special dietary practices like veganism, lactose intolerance or allergies. Hence, such
families can choose alternative dairy products equally rich in calcium such as, legumes,
leafy green vegetables, pulses, whole grains or juices which have been fortified, nuts,
seeds and fatty fishes such as salmons and sardines [18].
Engaging in optimum physical activity results in improved absorption of calcium such as
enhanced calcium retention in bones, improved strength of the skeletal system and hence
prevention of fracture and bone injuries in the future [11].It is recommended that
Australian adolescents and children participate in moderate levels of resistance of aerobic
8LIFESPAN NUTRITION
exercise of approximately 60 minutes every day, as per the recommendations postulated
by the Department of Health [20].
Part B: Audio Transcript
Taking note of the recent findings of the National Nutrition and Physical Activity Survey
(NNPAS), Australia’s youth are predicted to be susceptible for acquiring bone associated injuries
in the future.
With the help of the Automated Multiple Pass Method, the ABS, obtained a
comprehensive information on the food and beverage consumption patterns followed by
Australian households, especially children and families. The average intake of calcium among
the children and adolescents of Australia, within the age group of 12 to 18 years, were found to
be grossly deficient (853.4 – 833.4 mg/day) in comparison to the Department of Health’s
Nutrient Reference Values (Estimated Average Requirement: 1050 mg/day, Recommended
Daily Intake: 1300 mg/day).
Calcium deficiencies can contribute to fractures, muscle spasms and bone diseases like
osteoporosis during adulthood. Australian families must follow the Australia Dietary Guidelines
and consume dairy and non-dairy foods rich in calcium like yoghurt, cheese, milk, seeds, leafy
greens, seeds and soy as well as food rich in Vitamin D like fatty fish, fortified cereals and juices
and yolks. Engaging in daily, moderate levels of exercise will further enhance long term calcium
absorption.
exercise of approximately 60 minutes every day, as per the recommendations postulated
by the Department of Health [20].
Part B: Audio Transcript
Taking note of the recent findings of the National Nutrition and Physical Activity Survey
(NNPAS), Australia’s youth are predicted to be susceptible for acquiring bone associated injuries
in the future.
With the help of the Automated Multiple Pass Method, the ABS, obtained a
comprehensive information on the food and beverage consumption patterns followed by
Australian households, especially children and families. The average intake of calcium among
the children and adolescents of Australia, within the age group of 12 to 18 years, were found to
be grossly deficient (853.4 – 833.4 mg/day) in comparison to the Department of Health’s
Nutrient Reference Values (Estimated Average Requirement: 1050 mg/day, Recommended
Daily Intake: 1300 mg/day).
Calcium deficiencies can contribute to fractures, muscle spasms and bone diseases like
osteoporosis during adulthood. Australian families must follow the Australia Dietary Guidelines
and consume dairy and non-dairy foods rich in calcium like yoghurt, cheese, milk, seeds, leafy
greens, seeds and soy as well as food rich in Vitamin D like fatty fish, fortified cereals and juices
and yolks. Engaging in daily, moderate levels of exercise will further enhance long term calcium
absorption.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9LIFESPAN NUTRITION
Part C: Reflection
Skill Development
Performing this assignment was an enriching and enlightening experience for me since it
paved the way for my development and learning of key skills and experiences. Questioning and
critically evaluating evidence based research was a key skill which I leaned while covering the
various sections of this assignment. Critical appraisal is a key skill which must be possessed by
students since evidence based research is subject to limitations which may affect validity and
learning for future data collection practice. Learning this skill is of key importance since taught
me to not be reliant only on dietary recalls for data collection during future nutrition practice
[21]. Additionally, this assignment me to acquire skills of data evaluation and analysis. Data
evaluation is a key skill which must be administered by health professionals for critical
interpretation public health data and health outcomes. Hence, such skills of critical appraisal and
data evaluation will prove to be useful in implementing evidence based research in my future
professional practice [22].
What surprised me most was the prevalent inadequacies in calcium consumption across
the Australian population despite the wide availability of public health educational resources
which are available at present. This has motivated me to work actively towards improvement of
public health outcomes in my future professional practice. The variety of limitations prevalent in
dietary recalls are what further surprised me which has prompted me further to explore
alternative dietary data collection methods in my future professional practice. A combination of
dietary data collection methods like FoodWorks software and food frequency questionnaire have
been implicated to yield better outcomes in comparison to only dietary recalls for data collection
[23].
Part C: Reflection
Skill Development
Performing this assignment was an enriching and enlightening experience for me since it
paved the way for my development and learning of key skills and experiences. Questioning and
critically evaluating evidence based research was a key skill which I leaned while covering the
various sections of this assignment. Critical appraisal is a key skill which must be possessed by
students since evidence based research is subject to limitations which may affect validity and
learning for future data collection practice. Learning this skill is of key importance since taught
me to not be reliant only on dietary recalls for data collection during future nutrition practice
[21]. Additionally, this assignment me to acquire skills of data evaluation and analysis. Data
evaluation is a key skill which must be administered by health professionals for critical
interpretation public health data and health outcomes. Hence, such skills of critical appraisal and
data evaluation will prove to be useful in implementing evidence based research in my future
professional practice [22].
What surprised me most was the prevalent inadequacies in calcium consumption across
the Australian population despite the wide availability of public health educational resources
which are available at present. This has motivated me to work actively towards improvement of
public health outcomes in my future professional practice. The variety of limitations prevalent in
dietary recalls are what further surprised me which has prompted me further to explore
alternative dietary data collection methods in my future professional practice. A combination of
dietary data collection methods like FoodWorks software and food frequency questionnaire have
been implicated to yield better outcomes in comparison to only dietary recalls for data collection
[23].
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

10LIFESPAN NUTRITION
Resource Use and Time Planning
Academic, scholarly and peer review studies were the key resources which I resorted for
this assignment. Peer reviewed studies have been evidenced to yield data of commendable
validity and rigor and is helpful for enhancing the significance of one’s research [24]. A key
personal limitation is procrastination and inadequate time management which compelled me to
rush through the assignment at the final hours. Engaging in a personal time frame or routine will
be a useful coping strategy to prevent the same in the future [25].
Peer Learning
This assignment taught me calcium consumption not only enhances musculoskeletal
functioning but also is associated with positive anthropometric measurements and metabolic
outcomes. Such information is not only useful for my personal knowledge enhancement but also
paves the way for new treatment possibilities for children and adolescents who may have poor
cardiovascular and metabolic health [26]. A combination of evidence based research as well as
continuous personal mindfulness and reflection are useful for potential public health nutritionists
like me for improved understanding of future community health outcomes. If met with a
situation requiring calcium assessment in the future with a group of adolescents, children or their
families, I wish to implement multiple dietary methods of data collection such as software of
food frequency questionnaires along with dietary recall. Along with these, I also wish to evaluate
metabolic and cardiovascular outcomes during such a situation considering the research links
between obesity and calcium intake.
Resource Use and Time Planning
Academic, scholarly and peer review studies were the key resources which I resorted for
this assignment. Peer reviewed studies have been evidenced to yield data of commendable
validity and rigor and is helpful for enhancing the significance of one’s research [24]. A key
personal limitation is procrastination and inadequate time management which compelled me to
rush through the assignment at the final hours. Engaging in a personal time frame or routine will
be a useful coping strategy to prevent the same in the future [25].
Peer Learning
This assignment taught me calcium consumption not only enhances musculoskeletal
functioning but also is associated with positive anthropometric measurements and metabolic
outcomes. Such information is not only useful for my personal knowledge enhancement but also
paves the way for new treatment possibilities for children and adolescents who may have poor
cardiovascular and metabolic health [26]. A combination of evidence based research as well as
continuous personal mindfulness and reflection are useful for potential public health nutritionists
like me for improved understanding of future community health outcomes. If met with a
situation requiring calcium assessment in the future with a group of adolescents, children or their
families, I wish to implement multiple dietary methods of data collection such as software of
food frequency questionnaires along with dietary recall. Along with these, I also wish to evaluate
metabolic and cardiovascular outcomes during such a situation considering the research links
between obesity and calcium intake.
11LIFESPAN NUTRITION
References
1. Australian Bureau of Statistics. 4363.0.55.001 - Australian Health Survey: Users' Guide,
2011-13 [Internet]. Abs.gov.au. 2019 [cited 7 August 2019]. Available from:
https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4363.0.55.001Chapter65022011-13.
2. Thompson FE, Dixit-Joshi S, Potischman N, Dodd KW, Kirkpatrick SI, Kushi LH,
Alexander GL, Coleman LA, Zimmerman TP, Sundaram ME, Clancy HA. Comparison
of interviewer-administered and automated self-administered 24-hour dietary recalls in 3
diverse integrated health systems. American journal of epidemiology. 2015 May
10;181(12):970-8.
3. Gemming L, Mhurchu CN. Dietary under-reporting: what foods and which meals are
typically under-reported?. European journal of clinical nutrition. 2016 May;70(5):640.
4. Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results – Food
and Nutrients, 2011-12 [Internet]. Ausstats.abs.gov.au. 2019 [cited 7 August 2019].
Available from:
https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/4683FD7315DFDFDBCA257D
080014F9E0/$File/australian%20health%20survey%20nutrition%20first%20results%20-
%20food%20and%20nutrients,%202011-12.pdf.
5. Steinfeldt LC, Moshfegh AJ. Collecting Brand and Product Names in the USDA
Automated Multiple Pass Method (AMPM) 24-hour Dietary Recall. The FASEB Journal.
2016 Apr;30(1_supplement):677-9.
References
1. Australian Bureau of Statistics. 4363.0.55.001 - Australian Health Survey: Users' Guide,
2011-13 [Internet]. Abs.gov.au. 2019 [cited 7 August 2019]. Available from:
https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4363.0.55.001Chapter65022011-13.
2. Thompson FE, Dixit-Joshi S, Potischman N, Dodd KW, Kirkpatrick SI, Kushi LH,
Alexander GL, Coleman LA, Zimmerman TP, Sundaram ME, Clancy HA. Comparison
of interviewer-administered and automated self-administered 24-hour dietary recalls in 3
diverse integrated health systems. American journal of epidemiology. 2015 May
10;181(12):970-8.
3. Gemming L, Mhurchu CN. Dietary under-reporting: what foods and which meals are
typically under-reported?. European journal of clinical nutrition. 2016 May;70(5):640.
4. Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results – Food
and Nutrients, 2011-12 [Internet]. Ausstats.abs.gov.au. 2019 [cited 7 August 2019].
Available from:
https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/4683FD7315DFDFDBCA257D
080014F9E0/$File/australian%20health%20survey%20nutrition%20first%20results%20-
%20food%20and%20nutrients,%202011-12.pdf.
5. Steinfeldt LC, Moshfegh AJ. Collecting Brand and Product Names in the USDA
Automated Multiple Pass Method (AMPM) 24-hour Dietary Recall. The FASEB Journal.
2016 Apr;30(1_supplement):677-9.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.