Healthcare Work Placement Report: Canadian and African Systems
VerifiedAdded on 2023/01/13
|25
|5964
|1
Report
AI Summary
This report, a product of a student's work placement, delves into the primary care reforms in Ontario, Canada, detailing the various models and their operational mechanisms. It includes an interview and analyzes the healthcare systems of Canada and Angola, highlighting similarities and differences in funding, access, and infrastructure. The report identifies problems such as inadequate staffing and lack of resources, and proposes solutions, including increased government funding and the adoption of e-health technologies. Furthermore, it offers recommendations for change and personal opinions on the issues, along with insights on health office layouts, aiming to improve healthcare delivery and patient care. The report is complete with appendices that include interview forms and confidentiality statements.

Running Head: WORK PLACEMENT
Topic- Report on work placement
Student name
University name
Author notes
Topic- Report on work placement
Student name
University name
Author notes
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

WORK PLACEMENT
TABLE OF CONTENTS
Answer to question 1.......................................................................................................................3
Research of Primary Care (PC) reform in Ontario province.......................................................3
Number of PC groups operating..................................................................................................4
Description of the setting up of PC groups and their mode of operations...................................4
Interview session and other underway PC reforms......................................................................7
Answer to question 2.......................................................................................................................8
Interview with a different cultural people....................................................................................8
Comparison of healthcare system in Canada and Africa.............................................................8
Identification and resolution of problems....................................................................................9
Recommendations for change and personal opinions................................................................10
Answer to question 3.....................................................................................................................11
Layout of office and reception areas..........................................................................................11
Change required in the layout....................................................................................................12
Designing an ideal health office layout......................................................................................12
References......................................................................................................................................17
Appendices....................................................................................................................................19
A sample interview form of clients/ patients.............................................................................19
Thank you letter to interviewees................................................................................................20
Confidentiality statement...........................................................................................................21
Agreement and personal information.........................................................................................22
Interview session with an African origin people.......................................................................23
2
TABLE OF CONTENTS
Answer to question 1.......................................................................................................................3
Research of Primary Care (PC) reform in Ontario province.......................................................3
Number of PC groups operating..................................................................................................4
Description of the setting up of PC groups and their mode of operations...................................4
Interview session and other underway PC reforms......................................................................7
Answer to question 2.......................................................................................................................8
Interview with a different cultural people....................................................................................8
Comparison of healthcare system in Canada and Africa.............................................................8
Identification and resolution of problems....................................................................................9
Recommendations for change and personal opinions................................................................10
Answer to question 3.....................................................................................................................11
Layout of office and reception areas..........................................................................................11
Change required in the layout....................................................................................................12
Designing an ideal health office layout......................................................................................12
References......................................................................................................................................17
Appendices....................................................................................................................................19
A sample interview form of clients/ patients.............................................................................19
Thank you letter to interviewees................................................................................................20
Confidentiality statement...........................................................................................................21
Agreement and personal information.........................................................................................22
Interview session with an African origin people.......................................................................23
2
WORK PLACEMENT
PROJECT A
Answer to question 1
Research of Primary Care (PC) reform in Ontario province
Ontario is one of the most innovative provinces in pursuing primary care reform in
Canada. A number of primary care reform models are introduced to improve overall primacy
care support in Ontario. The multi-dimensional and complex structures created inconveniences
in many areas (Chatwood, 2018). The PC framework is based on three governing bodies namely
Primary Health Care, professional autonomy and neo-institutionalism. The PCR models fail to
balance structural and institutional relationships simultaneously. As a result, there is difficulty in
control areas of political, economic and clinical care aspects (Freund et al., 2015). Thus, greatest
amount of reform is required in altering the structural relationship between the medical
associations and the state. Power balance need to be emphasized more in reform areas. The
Ontario government has already invested in huge amount in regard to PC in the province but
deteriorating fiscal position has increased conflicts in regard to organized medicine and
physician budgets and a radical restructuring of the PC was hindered greatly (Hutchison &
Glazier, 2013). But Ontario still stands out among other Canadian provinces and the single-
minded focus of the government on PC is worth praising. The flexibility of the Universal
Medical Care coverage and Saskatoon Agreement has been increased by the PC reform in
Ontario (Jeffords & Jones, 2019). The PC in areas of care transition funding, home care and
coverage of catastrophic drugs has also been reformed greatly. To support reforms in PC changes
in physician remuneration was focused along with additional provinces of bonuses and other
performance-based incentives providence (Marchildon, 2013). This change has direct positive
impact on the number of graduates entering into Primary Care and there is a sharp increase in
3
PROJECT A
Answer to question 1
Research of Primary Care (PC) reform in Ontario province
Ontario is one of the most innovative provinces in pursuing primary care reform in
Canada. A number of primary care reform models are introduced to improve overall primacy
care support in Ontario. The multi-dimensional and complex structures created inconveniences
in many areas (Chatwood, 2018). The PC framework is based on three governing bodies namely
Primary Health Care, professional autonomy and neo-institutionalism. The PCR models fail to
balance structural and institutional relationships simultaneously. As a result, there is difficulty in
control areas of political, economic and clinical care aspects (Freund et al., 2015). Thus, greatest
amount of reform is required in altering the structural relationship between the medical
associations and the state. Power balance need to be emphasized more in reform areas. The
Ontario government has already invested in huge amount in regard to PC in the province but
deteriorating fiscal position has increased conflicts in regard to organized medicine and
physician budgets and a radical restructuring of the PC was hindered greatly (Hutchison &
Glazier, 2013). But Ontario still stands out among other Canadian provinces and the single-
minded focus of the government on PC is worth praising. The flexibility of the Universal
Medical Care coverage and Saskatoon Agreement has been increased by the PC reform in
Ontario (Jeffords & Jones, 2019). The PC in areas of care transition funding, home care and
coverage of catastrophic drugs has also been reformed greatly. To support reforms in PC changes
in physician remuneration was focused along with additional provinces of bonuses and other
performance-based incentives providence (Marchildon, 2013). This change has direct positive
impact on the number of graduates entering into Primary Care and there is a sharp increase in
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
WORK PLACEMENT
their numbers in recent times. Though the reform is still in work-in-process stage in regard to
quality of care providence.
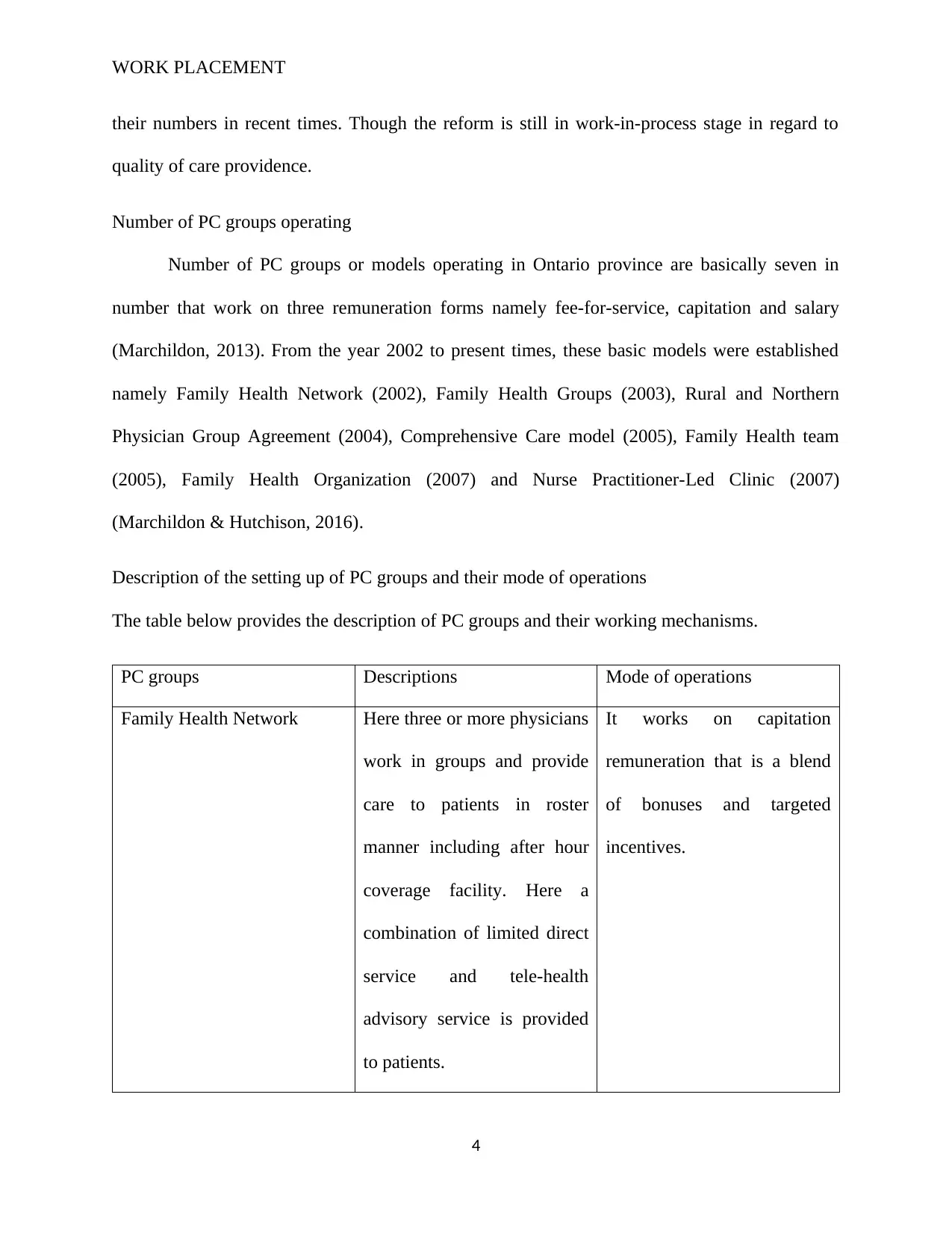
Number of PC groups operating
Number of PC groups or models operating in Ontario province are basically seven in
number that work on three remuneration forms namely fee-for-service, capitation and salary
(Marchildon, 2013). From the year 2002 to present times, these basic models were established
namely Family Health Network (2002), Family Health Groups (2003), Rural and Northern
Physician Group Agreement (2004), Comprehensive Care model (2005), Family Health team
(2005), Family Health Organization (2007) and Nurse Practitioner-Led Clinic (2007)
(Marchildon & Hutchison, 2016).
Description of the setting up of PC groups and their mode of operations
The table below provides the description of PC groups and their working mechanisms.
PC groups Descriptions Mode of operations
Family Health Network Here three or more physicians
work in groups and provide
care to patients in roster
manner including after hour
coverage facility. Here a
combination of limited direct
service and tele-health
advisory service is provided
to patients.
It works on capitation
remuneration that is a blend
of bonuses and targeted
incentives.
4
their numbers in recent times. Though the reform is still in work-in-process stage in regard to
quality of care providence.
Number of PC groups operating
Number of PC groups or models operating in Ontario province are basically seven in
number that work on three remuneration forms namely fee-for-service, capitation and salary
(Marchildon, 2013). From the year 2002 to present times, these basic models were established
namely Family Health Network (2002), Family Health Groups (2003), Rural and Northern
Physician Group Agreement (2004), Comprehensive Care model (2005), Family Health team
(2005), Family Health Organization (2007) and Nurse Practitioner-Led Clinic (2007)
(Marchildon & Hutchison, 2016).
Description of the setting up of PC groups and their mode of operations
The table below provides the description of PC groups and their working mechanisms.
PC groups Descriptions Mode of operations
Family Health Network Here three or more physicians
work in groups and provide
care to patients in roster
manner including after hour
coverage facility. Here a
combination of limited direct
service and tele-health
advisory service is provided
to patients.
It works on capitation
remuneration that is a blend
of bonuses and targeted
incentives.
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
WORK PLACEMENT
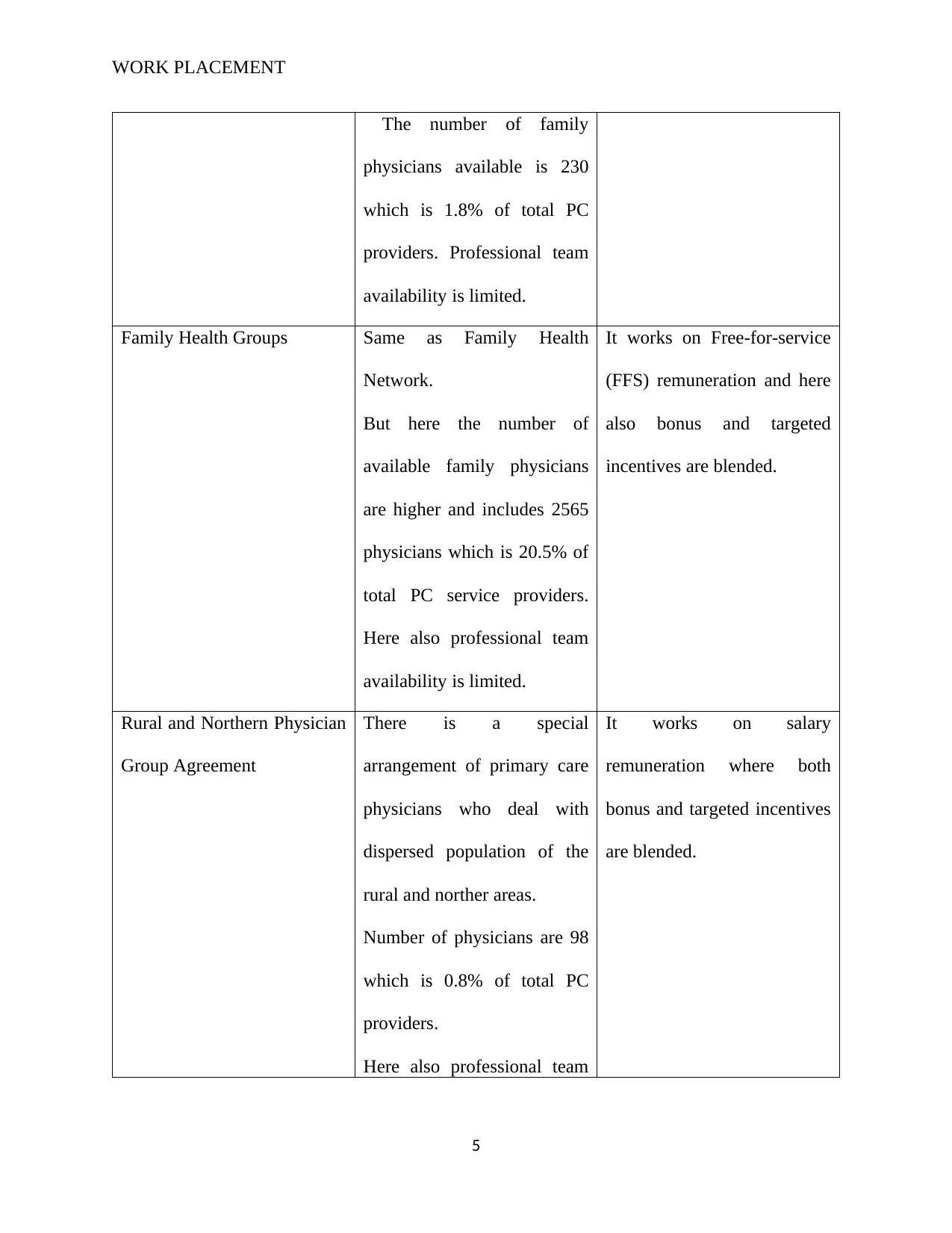
The number of family
physicians available is 230
which is 1.8% of total PC
providers. Professional team
availability is limited.
Family Health Groups Same as Family Health
Network.
But here the number of
available family physicians
are higher and includes 2565
physicians which is 20.5% of
total PC service providers.
Here also professional team
availability is limited.
It works on Free-for-service
(FFS) remuneration and here
also bonus and targeted
incentives are blended.
Rural and Northern Physician
Group Agreement
There is a special
arrangement of primary care
physicians who deal with
dispersed population of the
rural and norther areas.
Number of physicians are 98
which is 0.8% of total PC
providers.
Here also professional team
It works on salary
remuneration where both
bonus and targeted incentives
are blended.
5
The number of family
physicians available is 230
which is 1.8% of total PC
providers. Professional team
availability is limited.
Family Health Groups Same as Family Health
Network.
But here the number of
available family physicians
are higher and includes 2565
physicians which is 20.5% of
total PC service providers.
Here also professional team
availability is limited.
It works on Free-for-service
(FFS) remuneration and here
also bonus and targeted
incentives are blended.
Rural and Northern Physician
Group Agreement
There is a special
arrangement of primary care
physicians who deal with
dispersed population of the
rural and norther areas.
Number of physicians are 98
which is 0.8% of total PC
providers.
Here also professional team
It works on salary
remuneration where both
bonus and targeted incentives
are blended.
5
WORK PLACEMENT
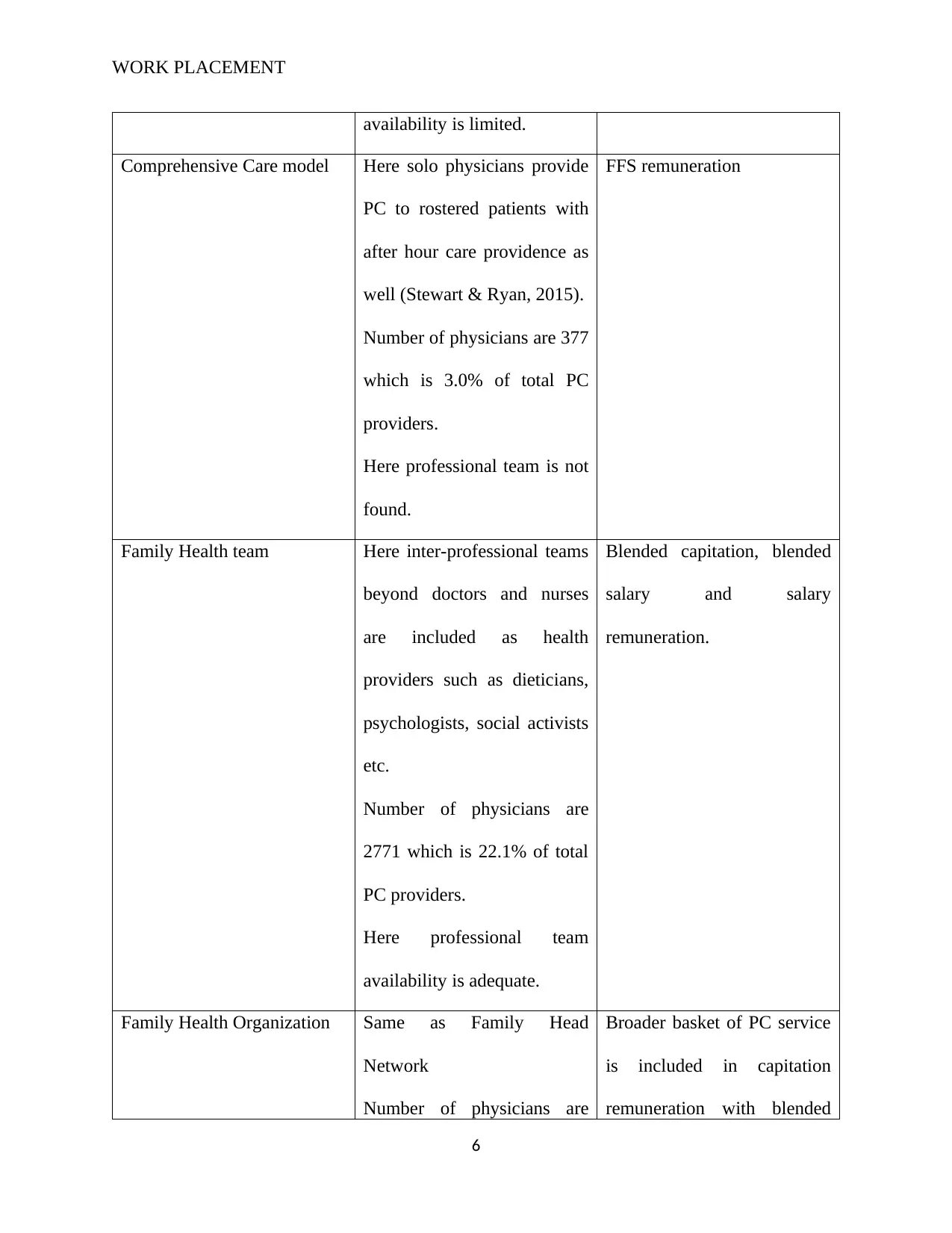
availability is limited.
Comprehensive Care model Here solo physicians provide
PC to rostered patients with
after hour care providence as
well (Stewart & Ryan, 2015).
Number of physicians are 377
which is 3.0% of total PC
providers.
Here professional team is not
found.
FFS remuneration
Family Health team Here inter-professional teams
beyond doctors and nurses
are included as health
providers such as dieticians,
psychologists, social activists
etc.
Number of physicians are
2771 which is 22.1% of total
PC providers.
Here professional team
availability is adequate.
Blended capitation, blended
salary and salary
remuneration.
Family Health Organization Same as Family Head
Network
Number of physicians are
Broader basket of PC service
is included in capitation
remuneration with blended
6
availability is limited.
Comprehensive Care model Here solo physicians provide
PC to rostered patients with
after hour care providence as
well (Stewart & Ryan, 2015).
Number of physicians are 377
which is 3.0% of total PC
providers.
Here professional team is not
found.
FFS remuneration
Family Health team Here inter-professional teams
beyond doctors and nurses
are included as health
providers such as dieticians,
psychologists, social activists
etc.
Number of physicians are
2771 which is 22.1% of total
PC providers.
Here professional team
availability is adequate.
Blended capitation, blended
salary and salary
remuneration.
Family Health Organization Same as Family Head
Network
Number of physicians are
Broader basket of PC service
is included in capitation
remuneration with blended
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
WORK PLACEMENT
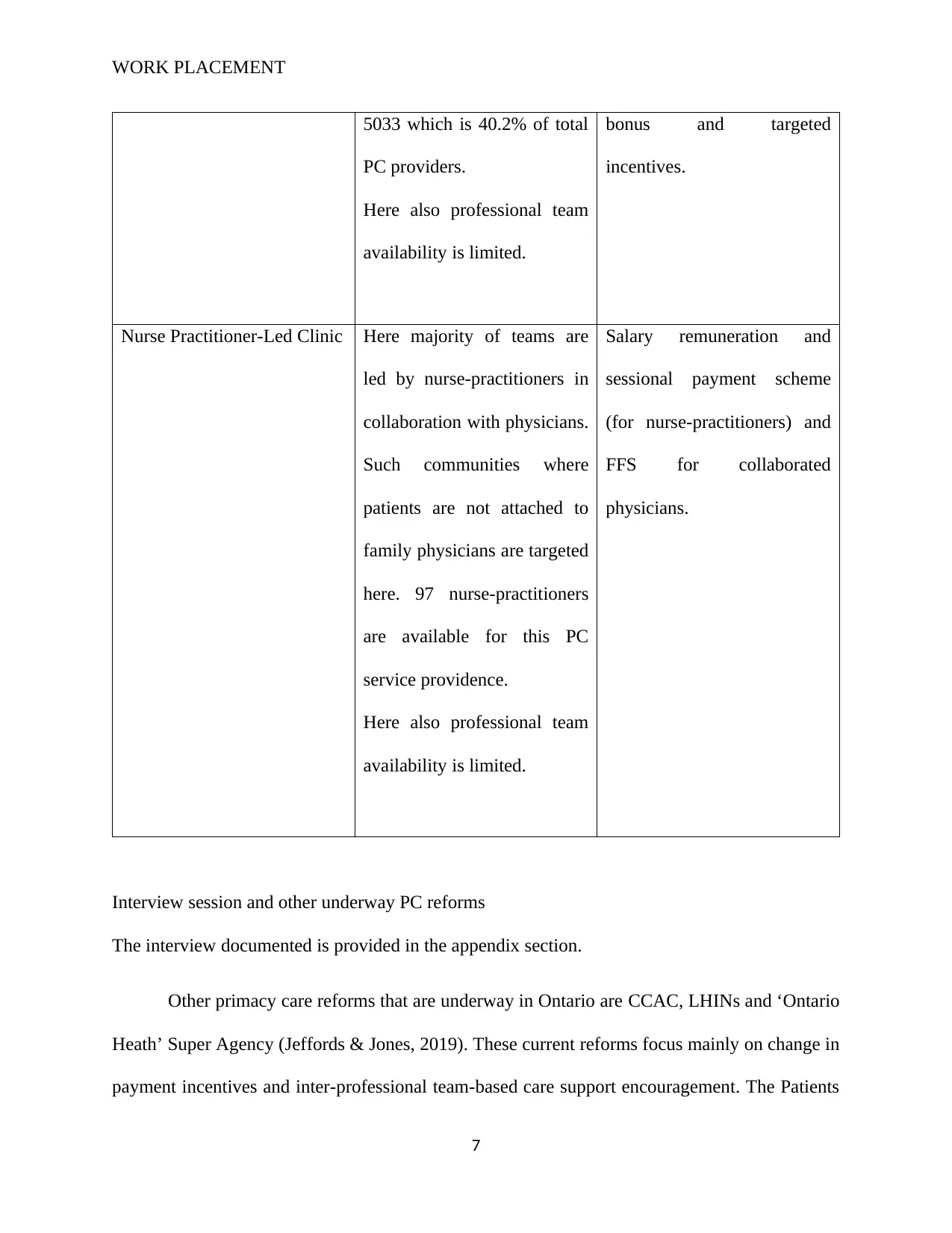
5033 which is 40.2% of total
PC providers.
Here also professional team
availability is limited.
bonus and targeted
incentives.
Nurse Practitioner-Led Clinic Here majority of teams are
led by nurse-practitioners in
collaboration with physicians.
Such communities where
patients are not attached to
family physicians are targeted
here. 97 nurse-practitioners
are available for this PC
service providence.
Here also professional team
availability is limited.
Salary remuneration and
sessional payment scheme
(for nurse-practitioners) and
FFS for collaborated
physicians.
Interview session and other underway PC reforms
The interview documented is provided in the appendix section.
Other primacy care reforms that are underway in Ontario are CCAC, LHINs and ‘Ontario
Heath’ Super Agency (Jeffords & Jones, 2019). These current reforms focus mainly on change in
payment incentives and inter-professional team-based care support encouragement. The Patients
7
5033 which is 40.2% of total
PC providers.
Here also professional team
availability is limited.
bonus and targeted
incentives.
Nurse Practitioner-Led Clinic Here majority of teams are
led by nurse-practitioners in
collaboration with physicians.
Such communities where
patients are not attached to
family physicians are targeted
here. 97 nurse-practitioners
are available for this PC
service providence.
Here also professional team
availability is limited.
Salary remuneration and
sessional payment scheme
(for nurse-practitioners) and
FFS for collaborated
physicians.
Interview session and other underway PC reforms
The interview documented is provided in the appendix section.
Other primacy care reforms that are underway in Ontario are CCAC, LHINs and ‘Ontario
Heath’ Super Agency (Jeffords & Jones, 2019). These current reforms focus mainly on change in
payment incentives and inter-professional team-based care support encouragement. The Patients
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

WORK PLACEMENT
first Act has also been recently implemented which widened the role of the Local Health
Integration Networks (LHINs) (Young et al., 2016).
Answer to question 2
Interview with a different cultural people
Details of interview session is provided in appendix. Here an African original, inhabitant
of Angola is interviewed for having knowledge on the African Healthcare system.
Comparison of healthcare system in Canada and Africa
Angola has a relatively higher population than Canada although the healthcare system is
not fully resilient to support the diverse needs of patients. While Canada is ranked 115th global
population wise, Angola enjoys a 55th global population ranking. It is important to note that the
Canadian healthcare system has tight guidelines. For instance, healthcare is not interested in
fraud but spending. The Canada Health Transfer is a fund set aside to finance citizens' medical
and healthcare needs – and it is distributed to municipal hospitals and local clinics. However, the
Angola government has a selected set of government hospitals that they fund. As a result, a key
discrepancy is that while the Canadian healthcare system is fully government sponsored, the
African healthcare system tends to receive funding from private players, foreign aid, and internal
funding.
Canada is a developed economy and as a result, most people enjoy relatively stable
healthcare. Over 75% of the population has access to quality healthcare, and an additional 15%
have private health insurance. The Canadian healthcare system further shows that all citizens
may access publicly available healthcare services in diverse settings; clinics, dispensaries, public
care facilities, and medical centers (Samuels, 2013). Angola, on the other hand, does not have a
8
first Act has also been recently implemented which widened the role of the Local Health
Integration Networks (LHINs) (Young et al., 2016).
Answer to question 2
Interview with a different cultural people
Details of interview session is provided in appendix. Here an African original, inhabitant
of Angola is interviewed for having knowledge on the African Healthcare system.
Comparison of healthcare system in Canada and Africa
Angola has a relatively higher population than Canada although the healthcare system is
not fully resilient to support the diverse needs of patients. While Canada is ranked 115th global
population wise, Angola enjoys a 55th global population ranking. It is important to note that the
Canadian healthcare system has tight guidelines. For instance, healthcare is not interested in
fraud but spending. The Canada Health Transfer is a fund set aside to finance citizens' medical
and healthcare needs – and it is distributed to municipal hospitals and local clinics. However, the
Angola government has a selected set of government hospitals that they fund. As a result, a key
discrepancy is that while the Canadian healthcare system is fully government sponsored, the
African healthcare system tends to receive funding from private players, foreign aid, and internal
funding.
Canada is a developed economy and as a result, most people enjoy relatively stable
healthcare. Over 75% of the population has access to quality healthcare, and an additional 15%
have private health insurance. The Canadian healthcare system further shows that all citizens
may access publicly available healthcare services in diverse settings; clinics, dispensaries, public
care facilities, and medical centers (Samuels, 2013). Angola, on the other hand, does not have a
8
WORK PLACEMENT
stable healthcare environment and only 40% of the population is covered by available insurance
plans. Lack of an integrated state system to secure user information, identify healthcare needs,
source, and deliver funding and financing makes it challenging for Angola and Africa in general
to have equitable access to healthcare services to the citizens. As a result, this analysis
establishes that a fully secure insurance plan will expand access to insurance services, and in the
process enable Angola and African, in general, realize better healthcare standards.
The problems experienced by the Canadian healthcare system are similarly reflected in
Angola. For instance, inadequate staff and lack of well-trained practitioners ails many clinics,
hospitals, and care centers. Similarly, poorly developed infrastructure and lack of adequate
clinical resources and equipment inhibits the quality of care and impedes the delivery of clinical
care. Angola and Africa suffer from similar problems although little has been invested to remedy
the situation. This analysis observes that in the comparison of the healthcare system of the two
nations, there are common problems that need re-evaluation.
Identification and resolution of problems
Well, the African healthcare system ails from the lack of a strong support structure. Poor
government funding leads to inadequate staffing suppressing the level of care. This problem can
be solved by strengthening the education system, provision of government sponsorships for
medical courses, and investment into healthcare research and vocational training.
A stark shortage of medical facilities ails most healthcare institutions. In Angola,
machines and equipment to diagnose and treat chronic illnesses are noticeably lacking, and in the
process undermining the quality and speed of clinical delivery. An important solution is to adopt
better management principles, to change the governance of public hospitals, and conduct
accountability as part of assessing and quantifying the utilizing of public healthcare resources.
9
stable healthcare environment and only 40% of the population is covered by available insurance
plans. Lack of an integrated state system to secure user information, identify healthcare needs,
source, and deliver funding and financing makes it challenging for Angola and Africa in general
to have equitable access to healthcare services to the citizens. As a result, this analysis
establishes that a fully secure insurance plan will expand access to insurance services, and in the
process enable Angola and African, in general, realize better healthcare standards.
The problems experienced by the Canadian healthcare system are similarly reflected in
Angola. For instance, inadequate staff and lack of well-trained practitioners ails many clinics,
hospitals, and care centers. Similarly, poorly developed infrastructure and lack of adequate
clinical resources and equipment inhibits the quality of care and impedes the delivery of clinical
care. Angola and Africa suffer from similar problems although little has been invested to remedy
the situation. This analysis observes that in the comparison of the healthcare system of the two
nations, there are common problems that need re-evaluation.
Identification and resolution of problems
Well, the African healthcare system ails from the lack of a strong support structure. Poor
government funding leads to inadequate staffing suppressing the level of care. This problem can
be solved by strengthening the education system, provision of government sponsorships for
medical courses, and investment into healthcare research and vocational training.
A stark shortage of medical facilities ails most healthcare institutions. In Angola,
machines and equipment to diagnose and treat chronic illnesses are noticeably lacking, and in the
process undermining the quality and speed of clinical delivery. An important solution is to adopt
better management principles, to change the governance of public hospitals, and conduct
accountability as part of assessing and quantifying the utilizing of public healthcare resources.
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
WORK PLACEMENT
The emergence of chronic conditions and new epidemiological patterns continues to put
healthcare systems in shambles. In Africa for example, chronic conditions are accountable for
80% healthcare expenditure. This means that the government spends significantly to deal with
specific illnesses and ailments. In this realization, there is a need to conduct market targeting to
determine ways to fight a certain group of ailments.
For instance, HIV/AIDS, Cancer, and diabetes cost 65% of the population and
approximated 47% of their income expenditure (Thompson, 2015). This means that individuals
suffering from such ailments are likely to spend a significant sum for diagnosis, treatment, and
self-management. This means that specific targeting of epidemiological conditions will help to
identify lasting solutions.
Finally, a major problem is that hospitals are yet to adopt new technologies to streamline
processes and enhance the quality of care. Nowadays, technologies provide a viable model to
secure patient data, integrate systems and networks, and streamline clinical care processes (Tony,
Brace, & Lois, 2018). This means that a major solution is to support a national-wide campaign to
build transparency on the potential and impact of new e-health technologies. Such resources will
help improve the speed and quality of care in local, national, and international jurisdictions.
Recommendations for change and personal opinions
Personally, I agree that low funding from the government affects most healthcare systems
in the developing world. Lack of transparency and accountability has led to misallocation and
misappropriate of public health funding, and in the process undermined the quality and the speed
of care. I also agree with the fact that most hospitals are yet to adopt e-health resources as
substitutes for quality care. This means that African cap taps into the emerging technologies to
boost their level and scale of service delivery. This recommendation adds insight into the fact
10
The emergence of chronic conditions and new epidemiological patterns continues to put
healthcare systems in shambles. In Africa for example, chronic conditions are accountable for
80% healthcare expenditure. This means that the government spends significantly to deal with
specific illnesses and ailments. In this realization, there is a need to conduct market targeting to
determine ways to fight a certain group of ailments.
For instance, HIV/AIDS, Cancer, and diabetes cost 65% of the population and
approximated 47% of their income expenditure (Thompson, 2015). This means that individuals
suffering from such ailments are likely to spend a significant sum for diagnosis, treatment, and
self-management. This means that specific targeting of epidemiological conditions will help to
identify lasting solutions.
Finally, a major problem is that hospitals are yet to adopt new technologies to streamline
processes and enhance the quality of care. Nowadays, technologies provide a viable model to
secure patient data, integrate systems and networks, and streamline clinical care processes (Tony,
Brace, & Lois, 2018). This means that a major solution is to support a national-wide campaign to
build transparency on the potential and impact of new e-health technologies. Such resources will
help improve the speed and quality of care in local, national, and international jurisdictions.
Recommendations for change and personal opinions
Personally, I agree that low funding from the government affects most healthcare systems
in the developing world. Lack of transparency and accountability has led to misallocation and
misappropriate of public health funding, and in the process undermined the quality and the speed
of care. I also agree with the fact that most hospitals are yet to adopt e-health resources as
substitutes for quality care. This means that African cap taps into the emerging technologies to
boost their level and scale of service delivery. This recommendation adds insight into the fact
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
WORK PLACEMENT
that governments and states must invest exhaustively in financing public and private health
facilities.
Such efforts will go a long way to ensure that citizens have equitable access to quality
and affordable healthcare. However, I disagree with the fact that targeting of epidemiological
conditions will help alleviate the prevalence of most diseases and illnesses. What should be
adopted is a complete change in lifestyle, including nutritional and dietary habits. Governments
must establish cross-tier partnerships with hospitals to fund community educational campaigns
that act as agents for positive lifestyle changes. This initiative will go a long way to ensure that
populations lead healthier lives and are immune to lifestyle chronic conditions such as cancer,
diabetes, obesity, heart disease, and cardiopulmonary diseases.
Answer to question 3
Layout of office and reception areas
The setting of health care offices may not be stunning examples of architectural designs
but are designed in a convenient manner so that patients can be put at ease and their healing
process can be accelerated (Yu, 2014). A number of health care offices are been reviewed and a
general discussion of their office and reception center layout is provided here. Most offices are
designed based on a single direction traffic flow. Total space availability is less important in
regard to layout design where in most cases the reception counter is located just after the main
entrance gate. This facilitates patients to clarify their queries in regard to various health issues. A
standardized layout map is also provided in the reception counter wall to guide patient parties to
the exact place they need to go. Traffic in most offices flows in a loop where both starting point
and ending point is same, that is the reception area (Gunn et al., 2015). Directional flow placards
are provided in intervals to guide patients conveniently. Various doctor consultancy rooms, lab
11
that governments and states must invest exhaustively in financing public and private health
facilities.
Such efforts will go a long way to ensure that citizens have equitable access to quality
and affordable healthcare. However, I disagree with the fact that targeting of epidemiological
conditions will help alleviate the prevalence of most diseases and illnesses. What should be
adopted is a complete change in lifestyle, including nutritional and dietary habits. Governments
must establish cross-tier partnerships with hospitals to fund community educational campaigns
that act as agents for positive lifestyle changes. This initiative will go a long way to ensure that
populations lead healthier lives and are immune to lifestyle chronic conditions such as cancer,
diabetes, obesity, heart disease, and cardiopulmonary diseases.
Answer to question 3
Layout of office and reception areas
The setting of health care offices may not be stunning examples of architectural designs
but are designed in a convenient manner so that patients can be put at ease and their healing
process can be accelerated (Yu, 2014). A number of health care offices are been reviewed and a
general discussion of their office and reception center layout is provided here. Most offices are
designed based on a single direction traffic flow. Total space availability is less important in
regard to layout design where in most cases the reception counter is located just after the main
entrance gate. This facilitates patients to clarify their queries in regard to various health issues. A
standardized layout map is also provided in the reception counter wall to guide patient parties to
the exact place they need to go. Traffic in most offices flows in a loop where both starting point
and ending point is same, that is the reception area (Gunn et al., 2015). Directional flow placards
are provided in intervals to guide patients conveniently. Various doctor consultancy rooms, lab
11
WORK PLACEMENT
testing rooms and other specialized treatment providence rooms are generally located in the
perimeter of the layout and open work stations are in the central location. The pod design system
of patient flow management use round robin pattern in many cases (Yu, 2014). Color also plays
crucial role in designing of the reception halls and other areas. Use of bright color is avoided and
eye-soothing colors like green, light blue etc. is used in most cases. The reception area is open
with an arch shaped desk in most cases where one or two receptionists are available 24 hours.
The emergency casualty and pharmacy departments are also present near to the reception.
Change required in the layout
The change layout is quite functional and the interviewees agree to the fact. Sitting
arrangement facility in the reception is fine but in many cases patients’ condition are more
serious and for that separate waiting room with bed-facility is highly recommended on their
behalf. Also, personal space of keeping belongings should be improved. Rest things are fine with
them.
Designing an ideal health office layout
An ideal health office should be designed in a manner so that quality care providence is
maximized. The design should be done keeping these major aspects in consideration namely
safety, employee comfort and patient flow (Gunn et al., 2015). Safety can be in terms of injury
safety, fire safety and safety from various stress related injuries. Furnitures in relation to a health
care office may include chairs, tables, desks, benches, single beds, stretchers, wardrobes and
wheelchairs for physically challenged patients (Carayon et al., 2014). The diagrammatic
representation of an ideal office layout is provided below. Here physician availability is limited
to two but it can be more than that where the same floor planning may be applicable.
12
testing rooms and other specialized treatment providence rooms are generally located in the
perimeter of the layout and open work stations are in the central location. The pod design system
of patient flow management use round robin pattern in many cases (Yu, 2014). Color also plays
crucial role in designing of the reception halls and other areas. Use of bright color is avoided and
eye-soothing colors like green, light blue etc. is used in most cases. The reception area is open
with an arch shaped desk in most cases where one or two receptionists are available 24 hours.
The emergency casualty and pharmacy departments are also present near to the reception.
Change required in the layout
The change layout is quite functional and the interviewees agree to the fact. Sitting
arrangement facility in the reception is fine but in many cases patients’ condition are more
serious and for that separate waiting room with bed-facility is highly recommended on their
behalf. Also, personal space of keeping belongings should be improved. Rest things are fine with
them.
Designing an ideal health office layout
An ideal health office should be designed in a manner so that quality care providence is
maximized. The design should be done keeping these major aspects in consideration namely
safety, employee comfort and patient flow (Gunn et al., 2015). Safety can be in terms of injury
safety, fire safety and safety from various stress related injuries. Furnitures in relation to a health
care office may include chairs, tables, desks, benches, single beds, stretchers, wardrobes and
wheelchairs for physically challenged patients (Carayon et al., 2014). The diagrammatic
representation of an ideal office layout is provided below. Here physician availability is limited
to two but it can be more than that where the same floor planning may be applicable.
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 25

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.