Case Study: CMAJ Analysis of Cannabis Legalization and Public Health
VerifiedAdded on 2023/06/14
|6
|6409
|266
Case Study
AI Summary
This case study analyzes cannabis legalization policies through a public health lens, drawing on experiences from countries like Uruguay, the Netherlands, and the United States. It uses a framework based on tobacco and alcohol regulation to assess the potential harms and benefits of different legalization approaches. The analysis emphasizes that the primary goal of cannabis legalization should be public health promotion and protection, including delaying youth use, reducing risky use, and minimizing addiction. The study also cautions against the rise of 'Big Cannabis' and advocates for government control over production, distribution, and marketing to prevent commercialization and prioritize public health objectives. Ultimately, the case study provides a resource for policymakers and researchers to evaluate cannabis policies and their outcomes, promoting evidence-based decision-making in the context of cannabis legalization.
AnalysisCMAJ
©2015 8872147 Canada Inc. or its licensors CMAJ, November 3, 2015, 187(16) 1211
According to the 2011 United Nations
World Drug Report, the prevalence of
cannabis use in the Netherlands, where
cannabis has been de facto legal for the last 40
years, is lower than in many other European
countries, the United States and Canada.1 Juris-
dictions that have recently legalized cannabis
(Uruguay and four US states) or redefined can-
nabis legalization policies (Catalonia) may be
expecting a similar result. However, if their poli-
cies governing cannabis are different, they may
see different outcomes.
In this article, we analyze cannabis legaliza-
tion policies through a public health lens using a
framework2 created from extensive data on to-
bacco3 and alcohol regulation.4 The aim of this
article, and indeed the framework, is to go be-
yond reduction in use and include minimization
of harms and realization of benefits.5 Cannabis
policy will be a topic of debate in Canada in the
lead-up to the federal election in October. The
governing party favours the status quo, one of
the competing political parties has promised
decriminalization, and another party supports le-
galization.6 Surveys have shown that most Can-
adians are looking for change.7,8 We provide a
resource for Canadian policy-makers looking to
reform cannabis laws and a tool for researchers
evaluating cannabis policies and their outcomes.
A broad picture of cannabis use
and legality
A 2013 UNICEF study found that the prevalence
of cannabis use among youth in the preceding
year was highest in Canada (28%) and lower in
Spain (24%), the US (22%) and the Netherlands
(17%).9 A 2014 survey in Uruguay found that
17% of secondary school children reported using
cannabis in the preceding year.10 According to the
2011 UN World Drug Report, cannabis use in the
general population was higher in Canada, the US
and Spain than in Uruguay and the Netherlands.1
There are an estimated 180.6 million cannabis
users worldwide,11 most living in jurisdictions
where cannabis is illegal.
In the past three years, Uruguay and four US
states have gone beyond the limited legalization
policies in Spain and the Netherlands to fully legal-
ize the possession, production and sale of cannabis.
Many other jurisdictions have removed criminal
penalties for possession or have legalized cannabis
for medical use, or both. Canada legalized the use
of cannabis for medical indications in 2001 and
implemented updated regulations for medical use
and production in 2014.12 Possession of cannabis
for nonmedical use remains a criminal offence, and
about 60 000 Canadians are charged yearly.13
Legalization of cannabis for nonmedical use
remains contrary to the 1961 UN Single Conven-
tion on Narcotic Drugs. Signatory countries can
address this by renegotiating, withdrawing from
or ignoring the treaty. Uruguay has chosen the
third approach, arguing that its legalization
framework follows the more important UN val-
ues of human rights, public health and safety.14
What are the harms from cannabis
use and its prohibition?
Policies that prohibit cannabis cause harm.15 They
funnel money into the illegal market and drive
criminal activity. They harm individuals through
imprisonment, marginalization and the creation of
barriers to treatment. This burden falls dispropor-
tionately on vulnerable groups; even though white
and black Americans use cannabis at about the
Cannabis legalization: adhering to public health best p
Sheryl Spithoff MD, Brian Emerson MD MHSc, Andrea Spithoff MA
Competing interests: None
declared.
This article has been peer
reviewed.
Correspondence to:
Sheryl Spithoff,
sheryl.spithoff@wchospital.ca
CMAJ 2015. DOI:10.1503
/cmaj.150657
• Prohibition of cannabis has failed to achieve its goal of reducing use
and causes substantial public health and societal harm.
• Two of Canada’s three main political parties promise to reform
cannabis policies if voted into power.
• If Canadian policy-makers move away from prohibitionist policies and
create a legal framework for cannabis, public health promotion and
protection must be the primary goals.
• Lessons learned from permissive alcohol and tobacco regulation can
guide public health–oriented policy-making; in particular, a ban on
promotion and advertising of cannabis to prevent commercialization
will be important.
• Policy-makers should look to jurisdictions with legalized cannabis that
prioritize public health and use evidence, not ideology, to guide policies.
Key points
CMAJ Podcasts: author interview at https://soundcloud.com/cmajpodcasts/150657-ana
©2015 8872147 Canada Inc. or its licensors CMAJ, November 3, 2015, 187(16) 1211
According to the 2011 United Nations
World Drug Report, the prevalence of
cannabis use in the Netherlands, where
cannabis has been de facto legal for the last 40
years, is lower than in many other European
countries, the United States and Canada.1 Juris-
dictions that have recently legalized cannabis
(Uruguay and four US states) or redefined can-
nabis legalization policies (Catalonia) may be
expecting a similar result. However, if their poli-
cies governing cannabis are different, they may
see different outcomes.
In this article, we analyze cannabis legaliza-
tion policies through a public health lens using a
framework2 created from extensive data on to-
bacco3 and alcohol regulation.4 The aim of this
article, and indeed the framework, is to go be-
yond reduction in use and include minimization
of harms and realization of benefits.5 Cannabis
policy will be a topic of debate in Canada in the
lead-up to the federal election in October. The
governing party favours the status quo, one of
the competing political parties has promised
decriminalization, and another party supports le-
galization.6 Surveys have shown that most Can-
adians are looking for change.7,8 We provide a
resource for Canadian policy-makers looking to
reform cannabis laws and a tool for researchers
evaluating cannabis policies and their outcomes.
A broad picture of cannabis use
and legality
A 2013 UNICEF study found that the prevalence
of cannabis use among youth in the preceding
year was highest in Canada (28%) and lower in
Spain (24%), the US (22%) and the Netherlands
(17%).9 A 2014 survey in Uruguay found that
17% of secondary school children reported using
cannabis in the preceding year.10 According to the
2011 UN World Drug Report, cannabis use in the
general population was higher in Canada, the US
and Spain than in Uruguay and the Netherlands.1
There are an estimated 180.6 million cannabis
users worldwide,11 most living in jurisdictions
where cannabis is illegal.
In the past three years, Uruguay and four US
states have gone beyond the limited legalization
policies in Spain and the Netherlands to fully legal-
ize the possession, production and sale of cannabis.
Many other jurisdictions have removed criminal
penalties for possession or have legalized cannabis
for medical use, or both. Canada legalized the use
of cannabis for medical indications in 2001 and
implemented updated regulations for medical use
and production in 2014.12 Possession of cannabis
for nonmedical use remains a criminal offence, and
about 60 000 Canadians are charged yearly.13
Legalization of cannabis for nonmedical use
remains contrary to the 1961 UN Single Conven-
tion on Narcotic Drugs. Signatory countries can
address this by renegotiating, withdrawing from
or ignoring the treaty. Uruguay has chosen the
third approach, arguing that its legalization
framework follows the more important UN val-
ues of human rights, public health and safety.14
What are the harms from cannabis
use and its prohibition?
Policies that prohibit cannabis cause harm.15 They
funnel money into the illegal market and drive
criminal activity. They harm individuals through
imprisonment, marginalization and the creation of
barriers to treatment. This burden falls dispropor-
tionately on vulnerable groups; even though white
and black Americans use cannabis at about the
Cannabis legalization: adhering to public health best p
Sheryl Spithoff MD, Brian Emerson MD MHSc, Andrea Spithoff MA
Competing interests: None
declared.
This article has been peer
reviewed.
Correspondence to:
Sheryl Spithoff,
sheryl.spithoff@wchospital.ca
CMAJ 2015. DOI:10.1503
/cmaj.150657
• Prohibition of cannabis has failed to achieve its goal of reducing use
and causes substantial public health and societal harm.
• Two of Canada’s three main political parties promise to reform
cannabis policies if voted into power.
• If Canadian policy-makers move away from prohibitionist policies and
create a legal framework for cannabis, public health promotion and
protection must be the primary goals.
• Lessons learned from permissive alcohol and tobacco regulation can
guide public health–oriented policy-making; in particular, a ban on
promotion and advertising of cannabis to prevent commercialization
will be important.
• Policy-makers should look to jurisdictions with legalized cannabis that
prioritize public health and use evidence, not ideology, to guide policies.
Key points
CMAJ Podcasts: author interview at https://soundcloud.com/cmajpodcasts/150657-ana
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Analysis
1212 CMAJ, November 3, 2015, 187(16)
same rate, the latter are 3.73 times more likely to
be arrested for possession.16 Finally, society pays
with high policing, court and prison costs.15,17
Harms from regular cannabis use may be less
than those associated with other psychoactive
substances,18 but they are still substantial at a pop-
ulation level. At higher doses, cannabis is a well-
established risk for motor vehicle crashes.19,20
Combining alcohol with cannabis results in
greater impairment than either substance alone.21
A recent study estimated that 6825–20 475 inju-
ries from cannabis-attributed motor vehicle
crashes occur in Canada annually.19 Each year in
Canada, 76 000–95 000 people undergo cannabis
addiction treatment and 219–547 cannabis-related
deaths occur (from injuries in motor vehicle
crashes and lung disease).19 Youth are particularly
vulnerable to the effects of cannabis: regular users
frequently report loss of control over their canna-
bis use,22 have lower educational attainment23 and
may have, according to one cohort study, a drop
in IQ that persists into adulthood.24
Often the harms from prohibition versus harms
from potential increased use of cannabis are
falsely pitted against each other. Evidence shows,
however, that cannabis prohibition has no effect
on rates of use, at least in developed countries.25–28
Some have advocated for the removal of crimi-
nal penalties for possession instead of legalization.
With Portugal’s experience in decriminalizing can-
nabis, users benefit from reduced marginalization,
imprisonment and barriers to treatment, and soci-
ety benefits from reduced policing, court and
prison costs.17 The illegal supply chain, however,
continues to fund criminal activity. In addition, be-
cause the government does not control the produc-
tion, processing, supply or price of cannabis, it has
a limited ability to achieve public health goals.
What objectives should underpin
legalization?
If policy-makers opt to legalize cannabis, careful
planning and comprehensive governmental con-
trols would provide the greatest likelihood of
minimizing harms and maximizing benefits. A
cannabis legalization framework should explic-
itly state that public health promotion and pro-
tection are its primary goals. It should list spe-
cific objectives,5,29,30
including delayed onset of
use by youth; reduced demand; reduced risky
use (e.g., reduced impaired driving); decreased
rates of problematic use, addiction and concur-
rent risky use of other substances; reduced con-
sumption of products with contaminants and un-
certain potency; increased public safety (e.g.,
reduced drug-related crime); reduced discrimina-
tion, stigmatization and marginalization of user
and realization of therapeutic benefits.
A frequently cited concern with legalization i
that it will allow the rise of Big Cannabis,31 simi-
lar to Big Tobacco and Big Alcohol. These pow-
erful multinational corporations have revenu
and market expansion as their primary goals, w
little consideration of the impact on public hea
They increase tobacco and alcohol use by lobb
ing for favourable regulations32 and funding huge
marketing campaigns.33 It is important that the
regulations actively work against the establish-
ment of Big Cannabis.
Evaluating cannabis regulations
through a public health lens
There is scant direct evidence to guide the cre-
ation of public health–oriented cannabis policie
Fortunately, there is an extensive evidence bas
for two other substances with potential for add
tion and other harms: tobacco3 and alcohol.4
With these data, researchers have proposed po
icy frameworks for cannabis.28–30,34
For our analysis, we built on previous
work,29,35–38
using a framework created by Can-
adian public health researchers2 that was based
on a report by the Health Officers Council
British Columbia.5 We included jurisdictions
with well-articulated cannabis policies and regu
lations, which we analyzed from a public health
perspective using a systematic method (Table
Uruguay
Uruguay follows the key public health best prac
tices.40 It has established a central, governmenta
arm’s length commission to purchase cannabis
from producers and sell to distributors. The com
mission will have control over production, qual
and prices, and the ability to undercut the illeg
market.41 Uruguay has banned cannabis-impaired
driving and has set the cut-off for impaired driv
ing to a serum tetrahydrocannabinol (THC) leve
of 10 ng/mL. Because of its zero-tolerance polic
for alcohol-impaired driving, the country has cr
ated a lower threshold for the combination of c
nabis and alcohol. Tax revenues will fund t
commission and a public health campaign. (Ca
nabis will initially be sold tax free to undercut t
illegal market.) Uruguay bans all promotion of
cannabis products. Pharmacies will sell bulk ca
nabis in plain bags, labelled only with the THC
percentage and warnings. (Sales are slated to
early in 2016.) Individuals are permitted to gro
their own cannabis and to form growing co
operatives. People who purchase or grow cann
bis will be registered and fingerprinted to preve
1212 CMAJ, November 3, 2015, 187(16)
same rate, the latter are 3.73 times more likely to
be arrested for possession.16 Finally, society pays
with high policing, court and prison costs.15,17
Harms from regular cannabis use may be less
than those associated with other psychoactive
substances,18 but they are still substantial at a pop-
ulation level. At higher doses, cannabis is a well-
established risk for motor vehicle crashes.19,20
Combining alcohol with cannabis results in
greater impairment than either substance alone.21
A recent study estimated that 6825–20 475 inju-
ries from cannabis-attributed motor vehicle
crashes occur in Canada annually.19 Each year in
Canada, 76 000–95 000 people undergo cannabis
addiction treatment and 219–547 cannabis-related
deaths occur (from injuries in motor vehicle
crashes and lung disease).19 Youth are particularly
vulnerable to the effects of cannabis: regular users
frequently report loss of control over their canna-
bis use,22 have lower educational attainment23 and
may have, according to one cohort study, a drop
in IQ that persists into adulthood.24
Often the harms from prohibition versus harms
from potential increased use of cannabis are
falsely pitted against each other. Evidence shows,
however, that cannabis prohibition has no effect
on rates of use, at least in developed countries.25–28
Some have advocated for the removal of crimi-
nal penalties for possession instead of legalization.
With Portugal’s experience in decriminalizing can-
nabis, users benefit from reduced marginalization,
imprisonment and barriers to treatment, and soci-
ety benefits from reduced policing, court and
prison costs.17 The illegal supply chain, however,
continues to fund criminal activity. In addition, be-
cause the government does not control the produc-
tion, processing, supply or price of cannabis, it has
a limited ability to achieve public health goals.
What objectives should underpin
legalization?
If policy-makers opt to legalize cannabis, careful
planning and comprehensive governmental con-
trols would provide the greatest likelihood of
minimizing harms and maximizing benefits. A
cannabis legalization framework should explic-
itly state that public health promotion and pro-
tection are its primary goals. It should list spe-
cific objectives,5,29,30
including delayed onset of
use by youth; reduced demand; reduced risky
use (e.g., reduced impaired driving); decreased
rates of problematic use, addiction and concur-
rent risky use of other substances; reduced con-
sumption of products with contaminants and un-
certain potency; increased public safety (e.g.,
reduced drug-related crime); reduced discrimina-
tion, stigmatization and marginalization of user
and realization of therapeutic benefits.
A frequently cited concern with legalization i
that it will allow the rise of Big Cannabis,31 simi-
lar to Big Tobacco and Big Alcohol. These pow-
erful multinational corporations have revenu
and market expansion as their primary goals, w
little consideration of the impact on public hea
They increase tobacco and alcohol use by lobb
ing for favourable regulations32 and funding huge
marketing campaigns.33 It is important that the
regulations actively work against the establish-
ment of Big Cannabis.
Evaluating cannabis regulations
through a public health lens
There is scant direct evidence to guide the cre-
ation of public health–oriented cannabis policie
Fortunately, there is an extensive evidence bas
for two other substances with potential for add
tion and other harms: tobacco3 and alcohol.4
With these data, researchers have proposed po
icy frameworks for cannabis.28–30,34
For our analysis, we built on previous
work,29,35–38
using a framework created by Can-
adian public health researchers2 that was based
on a report by the Health Officers Council
British Columbia.5 We included jurisdictions
with well-articulated cannabis policies and regu
lations, which we analyzed from a public health
perspective using a systematic method (Table
Uruguay
Uruguay follows the key public health best prac
tices.40 It has established a central, governmenta
arm’s length commission to purchase cannabis
from producers and sell to distributors. The com
mission will have control over production, qual
and prices, and the ability to undercut the illeg
market.41 Uruguay has banned cannabis-impaired
driving and has set the cut-off for impaired driv
ing to a serum tetrahydrocannabinol (THC) leve
of 10 ng/mL. Because of its zero-tolerance polic
for alcohol-impaired driving, the country has cr
ated a lower threshold for the combination of c
nabis and alcohol. Tax revenues will fund t
commission and a public health campaign. (Ca
nabis will initially be sold tax free to undercut t
illegal market.) Uruguay bans all promotion of
cannabis products. Pharmacies will sell bulk ca
nabis in plain bags, labelled only with the THC
percentage and warnings. (Sales are slated to
early in 2016.) Individuals are permitted to gro
their own cannabis and to form growing co
operatives. People who purchase or grow cann
bis will be registered and fingerprinted to preve
Analysis
CMAJ, November 3, 2015, 187(16) 1213
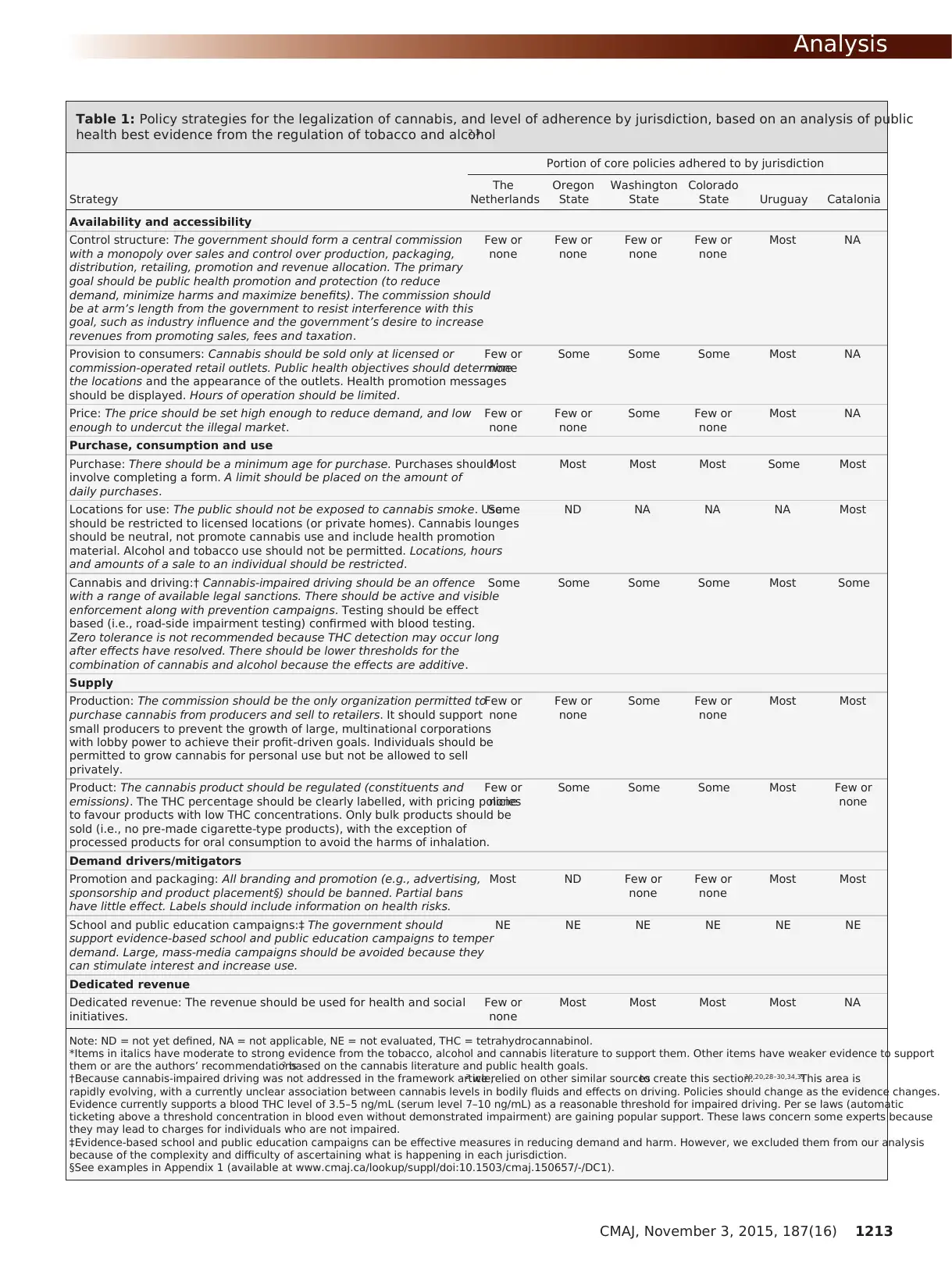
Table 1: Policy strategies for the legalization of cannabis, and level of adherence by jurisdiction, based on an analysis of public
health best evidence from the regulation of tobacco and alcohol2,3
Portion of core policies adhered to by jurisdiction
Strategy
The
Netherlands
Oregon
State
Washington
State
Colorado
State Uruguay Catalonia
Availability and accessibility
Control structure: The government should form a central commission
with a monopoly over sales and control over production, packaging,
distribution, retailing, promotion and revenue allocation. The primary
goal should be public health promotion and protection (to reduce
demand, minimize harms and maximize benefits). The commission should
be at arm’s length from the government to resist interference with this
goal, such as industry influence and the government’s desire to increase
revenues from promoting sales, fees and taxation.
Few or
none
Few or
none
Few or
none
Few or
none
Most NA
Provision to consumers: Cannabis should be sold only at licensed or
commission-operated retail outlets. Public health objectives should determine
the locations and the appearance of the outlets. Health promotion messages
should be displayed. Hours of operation should be limited.
Few or
none
Some Some Some Most NA
Price: The price should be set high enough to reduce demand, and low
enough to undercut the illegal market.
Few or
none
Few or
none
Some Few or
none
Most NA
Purchase, consumption and use
Purchase: There should be a minimum age for purchase. Purchases should
involve completing a form. A limit should be placed on the amount of
daily purchases.
Most Most Most Most Some Most
Locations for use: The public should not be exposed to cannabis smoke. Use
should be restricted to licensed locations (or private homes). Cannabis lounges
should be neutral, not promote cannabis use and include health promotion
material. Alcohol and tobacco use should not be permitted. Locations, hours
and amounts of a sale to an individual should be restricted.
Some ND NA NA NA Most
Cannabis and driving:† Cannabis-impaired driving should be an offence
with a range of available legal sanctions. There should be active and visible
enforcement along with prevention campaigns. Testing should be effect
based (i.e., road-side impairment testing) confirmed with blood testing.
Zero tolerance is not recommended because THC detection may occur long
after effects have resolved. There should be lower thresholds for the
combination of cannabis and alcohol because the effects are additive.
Some Some Some Some Most Some
Supply
Production: The commission should be the only organization permitted to
purchase cannabis from producers and sell to retailers. It should support
small producers to prevent the growth of large, multinational corporations
with lobby power to achieve their profit-driven goals. Individuals should be
permitted to grow cannabis for personal use but not be allowed to sell
privately.
Few or
none
Few or
none
Some Few or
none
Most Most
Product: The cannabis product should be regulated (constituents and
emissions). The THC percentage should be clearly labelled, with pricing policies
to favour products with low THC concentrations. Only bulk products should be
sold (i.e., no pre-made cigarette-type products), with the exception of
processed products for oral consumption to avoid the harms of inhalation.
Few or
none
Some Some Some Most Few or
none
Demand drivers/mitigators
Promotion and packaging: All branding and promotion (e.g., advertising,
sponsorship and product placement§) should be banned. Partial bans
have little effect. Labels should include information on health risks.
Most ND Few or
none
Few or
none
Most Most
School and public education campaigns:‡ The government should
support evidence-based school and public education campaigns to temper
demand. Large, mass-media campaigns should be avoided because they
can stimulate interest and increase use.
NE NE NE NE NE NE
Dedicated revenue
Dedicated revenue: The revenue should be used for health and social
initiatives.
Few or
none
Most Most Most Most NA
Note: ND = not yet defined, NA = not applicable, NE = not evaluated, THC = tetrahydrocannabinol.
*Items in italics have moderate to strong evidence from the tobacco, alcohol and cannabis literature to support them. Other items have weaker evidence to support
them or are the authors’ recommendations2 based on the cannabis literature and public health goals.
†Because cannabis-impaired driving was not addressed in the framework article,2 we relied on other similar sourcesto create this section.19,20,28–30,34,39
This area is
rapidly evolving, with a currently unclear association between cannabis levels in bodily fluids and effects on driving. Policies should change as the evidence changes.
Evidence currently supports a blood THC level of 3.5–5 ng/mL (serum level 7–10 ng/mL) as a reasonable threshold for impaired driving. Per se laws (automatic
ticketing above a threshold concentration in blood even without demonstrated impairment) are gaining popular support. These laws concern some experts because
they may lead to charges for individuals who are not impaired.
‡Evidence-based school and public education campaigns can be effective measures in reducing demand and harm. However, we excluded them from our analysis
because of the complexity and difficulty of ascertaining what is happening in each jurisdiction.
§See examples in Appendix 1 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150657/-/DC1).
CMAJ, November 3, 2015, 187(16) 1213
Table 1: Policy strategies for the legalization of cannabis, and level of adherence by jurisdiction, based on an analysis of public
health best evidence from the regulation of tobacco and alcohol2,3
Portion of core policies adhered to by jurisdiction
Strategy
The
Netherlands
Oregon
State
Washington
State
Colorado
State Uruguay Catalonia
Availability and accessibility
Control structure: The government should form a central commission
with a monopoly over sales and control over production, packaging,
distribution, retailing, promotion and revenue allocation. The primary
goal should be public health promotion and protection (to reduce
demand, minimize harms and maximize benefits). The commission should
be at arm’s length from the government to resist interference with this
goal, such as industry influence and the government’s desire to increase
revenues from promoting sales, fees and taxation.
Few or
none
Few or
none
Few or
none
Few or
none
Most NA
Provision to consumers: Cannabis should be sold only at licensed or
commission-operated retail outlets. Public health objectives should determine
the locations and the appearance of the outlets. Health promotion messages
should be displayed. Hours of operation should be limited.
Few or
none
Some Some Some Most NA
Price: The price should be set high enough to reduce demand, and low
enough to undercut the illegal market.
Few or
none
Few or
none
Some Few or
none
Most NA
Purchase, consumption and use
Purchase: There should be a minimum age for purchase. Purchases should
involve completing a form. A limit should be placed on the amount of
daily purchases.
Most Most Most Most Some Most
Locations for use: The public should not be exposed to cannabis smoke. Use
should be restricted to licensed locations (or private homes). Cannabis lounges
should be neutral, not promote cannabis use and include health promotion
material. Alcohol and tobacco use should not be permitted. Locations, hours
and amounts of a sale to an individual should be restricted.
Some ND NA NA NA Most
Cannabis and driving:† Cannabis-impaired driving should be an offence
with a range of available legal sanctions. There should be active and visible
enforcement along with prevention campaigns. Testing should be effect
based (i.e., road-side impairment testing) confirmed with blood testing.
Zero tolerance is not recommended because THC detection may occur long
after effects have resolved. There should be lower thresholds for the
combination of cannabis and alcohol because the effects are additive.
Some Some Some Some Most Some
Supply
Production: The commission should be the only organization permitted to
purchase cannabis from producers and sell to retailers. It should support
small producers to prevent the growth of large, multinational corporations
with lobby power to achieve their profit-driven goals. Individuals should be
permitted to grow cannabis for personal use but not be allowed to sell
privately.
Few or
none
Few or
none
Some Few or
none
Most Most
Product: The cannabis product should be regulated (constituents and
emissions). The THC percentage should be clearly labelled, with pricing policies
to favour products with low THC concentrations. Only bulk products should be
sold (i.e., no pre-made cigarette-type products), with the exception of
processed products for oral consumption to avoid the harms of inhalation.
Few or
none
Some Some Some Most Few or
none
Demand drivers/mitigators
Promotion and packaging: All branding and promotion (e.g., advertising,
sponsorship and product placement§) should be banned. Partial bans
have little effect. Labels should include information on health risks.
Most ND Few or
none
Few or
none
Most Most
School and public education campaigns:‡ The government should
support evidence-based school and public education campaigns to temper
demand. Large, mass-media campaigns should be avoided because they
can stimulate interest and increase use.
NE NE NE NE NE NE
Dedicated revenue
Dedicated revenue: The revenue should be used for health and social
initiatives.
Few or
none
Most Most Most Most NA
Note: ND = not yet defined, NA = not applicable, NE = not evaluated, THC = tetrahydrocannabinol.
*Items in italics have moderate to strong evidence from the tobacco, alcohol and cannabis literature to support them. Other items have weaker evidence to support
them or are the authors’ recommendations2 based on the cannabis literature and public health goals.
†Because cannabis-impaired driving was not addressed in the framework article,2 we relied on other similar sourcesto create this section.19,20,28–30,34,39
This area is
rapidly evolving, with a currently unclear association between cannabis levels in bodily fluids and effects on driving. Policies should change as the evidence changes.
Evidence currently supports a blood THC level of 3.5–5 ng/mL (serum level 7–10 ng/mL) as a reasonable threshold for impaired driving. Per se laws (automatic
ticketing above a threshold concentration in blood even without demonstrated impairment) are gaining popular support. These laws concern some experts because
they may lead to charges for individuals who are not impaired.
‡Evidence-based school and public education campaigns can be effective measures in reducing demand and harm. However, we excluded them from our analysis
because of the complexity and difficulty of ascertaining what is happening in each jurisdiction.
§See examples in Appendix 1 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150657/-/DC1).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Analysis
1214 CMAJ, November 3, 2015, 187(16)
consumers from buying more than 480 g per year.
This approach, however, gives rise to concerns
around privacy and may encourage some to pur-
chase cannabis from the illegal market.
The Netherlands
The Netherlands has a complex system gov-
erned by accepted practice rather than explicit
policy. It decriminalized cannabis almost 40
years ago. Around the same time, it started to
tolerate the buying and selling of small amounts
in strictly controlled locations (the production
and importing of cannabis remains illegal).42 As
long as these coffee shops sold small amounts,
did not advertise or market, did not sell to
minors and were “good neighbours,” they were
permitted to sell cannabis.43 This is still the
practice 40 years later, and the Netherlands con-
tinues to struggle with the “back door” problem
of an illegal supply chain.44 The government
does not control production, packaging or price,
nor is it able to legally tax cannabis products.
The illegal supply chain continues to fund the
illegal market. The government does, however,
ban all promotion. This ban may be an impor-
tant contributor to the low rates of use among
youth in the Netherlands.
Spain
Spain has taken a different approach: it permits
people to grow their own cannabis but prohibits
private for-profit cannabis enterprises.45 The coun-
try’s Supreme Court ruling in the 1970s opened
the door for nonprofit cannabis co-operatives, or
cannabis social clubs. The first such club opened
in Barcelona in 2001, and until recently, the clubs
were guided by voluntary adherence to a code of
practice. Many clubs, however, had lax enforce-
ment of the membership rules. As a result, the
government in Catalonia (an autonomous region in
Spain where most of the cannabis social clubs are
located) recently passed recommendations to
guide municipalities in licensing the clubs.46,47
These recommendations include limits on monthly
personal amounts of cannabis, hours of operation
and membership. They also ban all promotion.
Catalonia’s approach uses elements of a public
health framework and eliminates the risk of harms
associated with the involvement of profit-driven
corporations. However, because production and
use occur in private locations, the government has
limited ability to ensure safety and quality, and to
ensure that the focus remains on public health
promotion inside the club doors. In addition,
because the model restricts access to people who
grow cannabis for personal use or are invited into
a cannabis social club, some people may be
excluded from obtaining cannabis legally.
Oregon, Washington State, Colorado
The US states of Oregon, Washington and Colo
rado all have an arm’s-length commission to cr
and police cannabis policies, and to license pro
ducers and sellers.48–51The commissions control
the sellers’ locations and hours and amount of
sales, and they prohibit sales to people less tha
years old. The states ban cannabis-impaired dr
ing. Washington and Colorado have per se laws
with automatic ticketing for a blood THC conce
tration above 5 ng/mL. Colorado allows drivers
rebut the charges if they can show they were n
impaired. All three states control the product c
stituents and set labelling requirements. They
mit the sale of pre-made cigarette-type cannab
products, not just bulk products. Most revenue
earmarked for health and social programs.
The commissions do not have a monopoly on
supply. (This monopoly model has precedent in
the US: many states have a central governmen
monopoly for liquor). Instead, the states permi
rect sales from producers to retailers. Colorado
and Oregon go one step further and permit pro
ducers to be retailers. The commissions therefo
have little control over supply and prices. In ad
tion, they do not control cannabis taxation and
must appeal to the state legislature for change
Accordingly, Colorado and Washington State in
tially struggled with a price of legal cannabis th
was much higher than the price of illegal canna
bis. If the price of legal cannabis falls because
more efficient production, the opposite problem
may occur: cheap legal cannabis, a known de-
mand driver.52 Washington State has taken steps
to counteract the lack of control and the risk of
oversupply by limiting the number of producer
and total production capacity.53
The states have set few controls over other d
mand drivers. Washington and Colorado permi
forms of promotion (advertising, branding and
sponsorship) with few limits except on promoti
to youth. Colorado asks industry “to refrain fro
advertising where more than approximately 30
percent of the audience is reasonably expected
be under the age of 21.”50 Washington’s regula-
tions state that youth under age 21 should not
exposed to mass-media advertising, but they d
not explain how this is to be done.54 The states are
hampered in creating stricter regulations by co
tutional protection of commercial free speech.55,56
Because the states have limited control over
supply and price, and permit promotion, there
little to stop the rise of Big Cannabis and its as
ciated lobbying and marketing power. Washing
ton State may be somewhat protected with lim
it has placed on producer size and production.
states are at risk of an increase in cannabis use
over time. On the positive side, these states sh
1214 CMAJ, November 3, 2015, 187(16)
consumers from buying more than 480 g per year.
This approach, however, gives rise to concerns
around privacy and may encourage some to pur-
chase cannabis from the illegal market.
The Netherlands
The Netherlands has a complex system gov-
erned by accepted practice rather than explicit
policy. It decriminalized cannabis almost 40
years ago. Around the same time, it started to
tolerate the buying and selling of small amounts
in strictly controlled locations (the production
and importing of cannabis remains illegal).42 As
long as these coffee shops sold small amounts,
did not advertise or market, did not sell to
minors and were “good neighbours,” they were
permitted to sell cannabis.43 This is still the
practice 40 years later, and the Netherlands con-
tinues to struggle with the “back door” problem
of an illegal supply chain.44 The government
does not control production, packaging or price,
nor is it able to legally tax cannabis products.
The illegal supply chain continues to fund the
illegal market. The government does, however,
ban all promotion. This ban may be an impor-
tant contributor to the low rates of use among
youth in the Netherlands.
Spain
Spain has taken a different approach: it permits
people to grow their own cannabis but prohibits
private for-profit cannabis enterprises.45 The coun-
try’s Supreme Court ruling in the 1970s opened
the door for nonprofit cannabis co-operatives, or
cannabis social clubs. The first such club opened
in Barcelona in 2001, and until recently, the clubs
were guided by voluntary adherence to a code of
practice. Many clubs, however, had lax enforce-
ment of the membership rules. As a result, the
government in Catalonia (an autonomous region in
Spain where most of the cannabis social clubs are
located) recently passed recommendations to
guide municipalities in licensing the clubs.46,47
These recommendations include limits on monthly
personal amounts of cannabis, hours of operation
and membership. They also ban all promotion.
Catalonia’s approach uses elements of a public
health framework and eliminates the risk of harms
associated with the involvement of profit-driven
corporations. However, because production and
use occur in private locations, the government has
limited ability to ensure safety and quality, and to
ensure that the focus remains on public health
promotion inside the club doors. In addition,
because the model restricts access to people who
grow cannabis for personal use or are invited into
a cannabis social club, some people may be
excluded from obtaining cannabis legally.
Oregon, Washington State, Colorado
The US states of Oregon, Washington and Colo
rado all have an arm’s-length commission to cr
and police cannabis policies, and to license pro
ducers and sellers.48–51The commissions control
the sellers’ locations and hours and amount of
sales, and they prohibit sales to people less tha
years old. The states ban cannabis-impaired dr
ing. Washington and Colorado have per se laws
with automatic ticketing for a blood THC conce
tration above 5 ng/mL. Colorado allows drivers
rebut the charges if they can show they were n
impaired. All three states control the product c
stituents and set labelling requirements. They
mit the sale of pre-made cigarette-type cannab
products, not just bulk products. Most revenue
earmarked for health and social programs.
The commissions do not have a monopoly on
supply. (This monopoly model has precedent in
the US: many states have a central governmen
monopoly for liquor). Instead, the states permi
rect sales from producers to retailers. Colorado
and Oregon go one step further and permit pro
ducers to be retailers. The commissions therefo
have little control over supply and prices. In ad
tion, they do not control cannabis taxation and
must appeal to the state legislature for change
Accordingly, Colorado and Washington State in
tially struggled with a price of legal cannabis th
was much higher than the price of illegal canna
bis. If the price of legal cannabis falls because
more efficient production, the opposite problem
may occur: cheap legal cannabis, a known de-
mand driver.52 Washington State has taken steps
to counteract the lack of control and the risk of
oversupply by limiting the number of producer
and total production capacity.53
The states have set few controls over other d
mand drivers. Washington and Colorado permi
forms of promotion (advertising, branding and
sponsorship) with few limits except on promoti
to youth. Colorado asks industry “to refrain fro
advertising where more than approximately 30
percent of the audience is reasonably expected
be under the age of 21.”50 Washington’s regula-
tions state that youth under age 21 should not
exposed to mass-media advertising, but they d
not explain how this is to be done.54 The states are
hampered in creating stricter regulations by co
tutional protection of commercial free speech.55,56
Because the states have limited control over
supply and price, and permit promotion, there
little to stop the rise of Big Cannabis and its as
ciated lobbying and marketing power. Washing
ton State may be somewhat protected with lim
it has placed on producer size and production.
states are at risk of an increase in cannabis use
over time. On the positive side, these states sh
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Analysis
CMAJ, November 3, 2015, 187(16) 1215
see a reduction in crime, harms to cannabis users
(from incarceration and marginalization), and
policing, court and prison costs.17
How should Canada proceed?
Canada has started down the path to a regulated
market by implementing commercial production
of cannabis for therapeutic purposes. Concur-
rently, there is a proliferation of unregulated can-
nabis dispensaries, especially in Vancouver and
Victoria. Both municipalities are moving to regu-
late these operations.57,58
Given the evolving political and social land-
scape, and the upcoming federal election, Canada
may soon revisit its policy on nonmedical canna-
bis. The federal government could create regula-
tions or delegate this responsibility to provincial
governments, either through an exemption to the
Controlled Drugs and Substances Act (as was
done in British Columbia to permit a supervised
injection site) or through statute amendment (as
happened with gambling59,60
).
If Canadian policy-makers decide to create a
legal, regulatory framework for cannabis, it is criti-
cal that public health objectives be the foundation
of changes. Otherwise, Canada may experience the
same health and social harms that resulted from the
commercialization of alcohol and tobacco. The
Canadian public would likely support a model that
has public health as its primary goal.61,62
Policy-makers can use tobacco and alcohol
research and the frameworks for cannabis policy
created by public health researchers as a guide.
They can also learn from the experiences of other
jurisdictions. Spain and Uruguay have models
that could be adapted for use in Canada (without
the registration and fingerprinting of consumers
that Uruguay requires). The American models do
not put public health first and risk the rise of Big
Cannabis and increased harms, and the Dutch
model has not solved the “back door” illegal sup-
ply problem. With careful planning, Canada can
create its own policy framework for legalized
cannabis that achieves public health objectives.
References
1. World drug report 2011. Vienna: United Nations Office on Drugs
and Crime; 2011:209-40. Available: www.unodc.org/documents/
data-and -analysis/WDR2011/StatAnnex-consumption.pdf (ac-
cessed 2015 Sept. 2).
2. Haden M, Emerson BP. A vision of cannabis regulation: a pub-
lic health approach based on lessons learned from the regulation
of alcohol and tobacco. Open Medicine 2014;8:e73-80.
3. WHO framework convention on tobacco control. Geneva:
World Health Organization; 2003. Available: www.who.int/fctc/
text_download/en/ (accessed 2015 Apr. 30).
4. Babor TF, Caetano R, Casswell S, et al. Alcohol: no ordinary
commodity: research and public policy. Oxford (UK): Oxford
University Press; 2010. Available: www.oxfordscholarship.
com/view /10.1093 /acprof:oso/9780199551149.001.0001/acprof
-9780199551149 (accessed 2015 Apr. 30).
5. Public health perspectives for regulating psychoactive sub-
stances: What we can do about alcohol, tobacco, and other
drugs? Health Officers Council of British Columbia; 2011.
Available: https://healthofficerscouncil.files.wordpress.com
/2012/12/regulated-models-v8-final.pdf (accessed 2015 Apr. 30).
6. Health and safety, justice and law: where Canadian political par-
ties stand on marijuana [blog]. The Fifth Estate 2015 Jan. 29.
Available: www.cbc.ca/fifth/blog/where-canadian-political
-parties-stand-on-marijuana (accessed 2015 Aug. 5).
7. Six-in-ten Canadians support legalizing marijuana, but say it’s not
a top justice priority [Canada public opinion poll]. Angus Reid
Global 2014 Aug. 12. Available: http://angusreidglobal.com/wp
-content/uploads/2014/08/ARG-Marijuana-Opinions2.pdf (ac-
cessed 2015 Aug. 20).
8. Kennedy M. Government’s poll shows Canadians want marijuana
laws changed. Ottawa Citizen 2014 July 30. Available: http://ottawa
citizen.com/news/politics/conservative-governments-poll -shows
-canadians-want-marijuana-laws-changed (accessed 2015 Aug. 19).
9. Office of Research Innocenti report card 11: Child well-being in
rich countries: a comparative overview. Florence: UNICEF;
2013. Available: www.unicef.ca/sites/default/files/imce _
uploads/DISCOVER/OUR%20WORK/ADVOCACY/DOMESTIC
/POLICY %20ADVOCACY/DOCS/unicef_report_card_11.pdf (ac-
cessed 2015 June 12).
10. Boidi F, Maria JMC, Queirolo R, et al. Marijuana legalization in
Uruguay and beyond: executive summary. Insights Research
Group; Latin America and Caribbean Center, FIU; Universidad
Católica del Uruguay; 2015. Available: www.wilsoncenter.org/
sites/default/files/Marijuana%20Legalization%20in%20Uruguay
%20and%20Beyond_brief%20report_v3%20%282%29.pdf (ac-
cessed 2015 Aug. 17).
11. World Drug Report 2013. Vienna: United Nations Office on
Drugs and Crime; 2013. Available: https://www.unodc.org/
unodc/secured/wdr/wdr2013/World_Drug_Report_2013.pdf (ac-
cessed 2015 Sept. 2).
12. Marihuana for Medical Purposes Regulations. SOR/2013-119.
Available: http://laws-lois.justice.gc.ca/eng/regulations/SOR
-2013-119/index.html (accessed 2015 Sept. 6).
13. Police-reported crime for selected offences, Canada [Table 1].
Ottawa: Statistics Canada; 2014. Available: www.statcan.gc.ca/
daily -quotidien/140723/t140723b001-eng.htm (accessed 2015
July 10).
14. Hetzer H, Walsh J. Pioneering cannabis regulation in Uruguay.
New York: North American Congress on Latin America
(NACLA); 2014. Available: https://nacla.org/article/pioneering
-cannabis-regulation-uruguay (accessed 2015 Aug. 18).
15. War on drugs: report of the Global Commission on Drug Policy
June 2011. Rio de Janeiro: Global Commission on Drug Policy;
2011. Available: www.globalcommissionondrugs.org/wp-content/
themes/gcdp_v1/pdf/Global_Commission_Report_English.pdf (ac-
cessed 2015 Aug. 15).
16. The war on marijuana in black and white: billions of dollars
wasted on radically biased arrests. New York: American Civil
Liberties Union; 2013. Available: www.aclu.org/files/assets/
aclu-thewaronmarijuana-rel2.pdf (accessed 2015 June 23).
17. Hughes CE, Stevens A. What can we learn from the Portuguese
decriminalization of illicit drugs? Br J Criminol 2010;50:999-1022.
18. Nutt DJ, King LA, Philips LD. Drug harms in the UK: a multi-
criteria decision analysis. Lancet 2010;376:1558-65.
19. Fischer B, Imtiaz S, Rudzinski K, et al. Crude estimates of can-
nabis-attributable mortality and morbidity in Canada — implica-
tions for public health focused intervention priorities. J Public
Health (Oxf) 2015;Jan 28:pii: fdv005.
20. Drummer OH, Gerostamoulos J, Batziris H, et al. The involve-
ment of drugs in drivers of motor vehicles killed in Australian
road traffic crashes. Accid Anal Prev 2004;36:239-48.
21. Sewell R, Poling J, Sofuoglu M. The effect of cannabis com-
pared with alcohol on driving. Am J Addiction 2009;18:185-93.
22. Nocon A, Wittchen HU, Pfister H, et al. Dependence symptoms
in young cannabis users? A prospective epidemiological study.
J Psychiatr Res 2006;40:394-403.
23. Hall W. What has research over the past two decades revealed
about the adverse health effects of recreational cannabis use?
Addiction 2015;110:19-35.
24. Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users
show neuropsychological decline from childhood to midlife.
Proc Natl Acad Sci U S A 2012;40:E2657-2664.
25. MacCoun RJ, Reuter PH. Drug war heresies: learning from
other vices, time & places. Cambridge (UK): Cambridge Uni-
versity Press; 2001.
26. Simons-Morton B, Pickett W, Boyce W, et al. Cross-national com-
parison of adolescent drinking and cannabis use in the United States,
Canada, and the Netherlands. Int J Drug Policy 2010; 21:64-9.
27. Canadian Drug Policy Coalition. Getting to tomorrow: a report on
Canadian drug policy. Vancouver: Simon Fraser University; 2013.
CMAJ, November 3, 2015, 187(16) 1215
see a reduction in crime, harms to cannabis users
(from incarceration and marginalization), and
policing, court and prison costs.17
How should Canada proceed?
Canada has started down the path to a regulated
market by implementing commercial production
of cannabis for therapeutic purposes. Concur-
rently, there is a proliferation of unregulated can-
nabis dispensaries, especially in Vancouver and
Victoria. Both municipalities are moving to regu-
late these operations.57,58
Given the evolving political and social land-
scape, and the upcoming federal election, Canada
may soon revisit its policy on nonmedical canna-
bis. The federal government could create regula-
tions or delegate this responsibility to provincial
governments, either through an exemption to the
Controlled Drugs and Substances Act (as was
done in British Columbia to permit a supervised
injection site) or through statute amendment (as
happened with gambling59,60
).
If Canadian policy-makers decide to create a
legal, regulatory framework for cannabis, it is criti-
cal that public health objectives be the foundation
of changes. Otherwise, Canada may experience the
same health and social harms that resulted from the
commercialization of alcohol and tobacco. The
Canadian public would likely support a model that
has public health as its primary goal.61,62
Policy-makers can use tobacco and alcohol
research and the frameworks for cannabis policy
created by public health researchers as a guide.
They can also learn from the experiences of other
jurisdictions. Spain and Uruguay have models
that could be adapted for use in Canada (without
the registration and fingerprinting of consumers
that Uruguay requires). The American models do
not put public health first and risk the rise of Big
Cannabis and increased harms, and the Dutch
model has not solved the “back door” illegal sup-
ply problem. With careful planning, Canada can
create its own policy framework for legalized
cannabis that achieves public health objectives.
References
1. World drug report 2011. Vienna: United Nations Office on Drugs
and Crime; 2011:209-40. Available: www.unodc.org/documents/
data-and -analysis/WDR2011/StatAnnex-consumption.pdf (ac-
cessed 2015 Sept. 2).
2. Haden M, Emerson BP. A vision of cannabis regulation: a pub-
lic health approach based on lessons learned from the regulation
of alcohol and tobacco. Open Medicine 2014;8:e73-80.
3. WHO framework convention on tobacco control. Geneva:
World Health Organization; 2003. Available: www.who.int/fctc/
text_download/en/ (accessed 2015 Apr. 30).
4. Babor TF, Caetano R, Casswell S, et al. Alcohol: no ordinary
commodity: research and public policy. Oxford (UK): Oxford
University Press; 2010. Available: www.oxfordscholarship.
com/view /10.1093 /acprof:oso/9780199551149.001.0001/acprof
-9780199551149 (accessed 2015 Apr. 30).
5. Public health perspectives for regulating psychoactive sub-
stances: What we can do about alcohol, tobacco, and other
drugs? Health Officers Council of British Columbia; 2011.
Available: https://healthofficerscouncil.files.wordpress.com
/2012/12/regulated-models-v8-final.pdf (accessed 2015 Apr. 30).
6. Health and safety, justice and law: where Canadian political par-
ties stand on marijuana [blog]. The Fifth Estate 2015 Jan. 29.
Available: www.cbc.ca/fifth/blog/where-canadian-political
-parties-stand-on-marijuana (accessed 2015 Aug. 5).
7. Six-in-ten Canadians support legalizing marijuana, but say it’s not
a top justice priority [Canada public opinion poll]. Angus Reid
Global 2014 Aug. 12. Available: http://angusreidglobal.com/wp
-content/uploads/2014/08/ARG-Marijuana-Opinions2.pdf (ac-
cessed 2015 Aug. 20).
8. Kennedy M. Government’s poll shows Canadians want marijuana
laws changed. Ottawa Citizen 2014 July 30. Available: http://ottawa
citizen.com/news/politics/conservative-governments-poll -shows
-canadians-want-marijuana-laws-changed (accessed 2015 Aug. 19).
9. Office of Research Innocenti report card 11: Child well-being in
rich countries: a comparative overview. Florence: UNICEF;
2013. Available: www.unicef.ca/sites/default/files/imce _
uploads/DISCOVER/OUR%20WORK/ADVOCACY/DOMESTIC
/POLICY %20ADVOCACY/DOCS/unicef_report_card_11.pdf (ac-
cessed 2015 June 12).
10. Boidi F, Maria JMC, Queirolo R, et al. Marijuana legalization in
Uruguay and beyond: executive summary. Insights Research
Group; Latin America and Caribbean Center, FIU; Universidad
Católica del Uruguay; 2015. Available: www.wilsoncenter.org/
sites/default/files/Marijuana%20Legalization%20in%20Uruguay
%20and%20Beyond_brief%20report_v3%20%282%29.pdf (ac-
cessed 2015 Aug. 17).
11. World Drug Report 2013. Vienna: United Nations Office on
Drugs and Crime; 2013. Available: https://www.unodc.org/
unodc/secured/wdr/wdr2013/World_Drug_Report_2013.pdf (ac-
cessed 2015 Sept. 2).
12. Marihuana for Medical Purposes Regulations. SOR/2013-119.
Available: http://laws-lois.justice.gc.ca/eng/regulations/SOR
-2013-119/index.html (accessed 2015 Sept. 6).
13. Police-reported crime for selected offences, Canada [Table 1].
Ottawa: Statistics Canada; 2014. Available: www.statcan.gc.ca/
daily -quotidien/140723/t140723b001-eng.htm (accessed 2015
July 10).
14. Hetzer H, Walsh J. Pioneering cannabis regulation in Uruguay.
New York: North American Congress on Latin America
(NACLA); 2014. Available: https://nacla.org/article/pioneering
-cannabis-regulation-uruguay (accessed 2015 Aug. 18).
15. War on drugs: report of the Global Commission on Drug Policy
June 2011. Rio de Janeiro: Global Commission on Drug Policy;
2011. Available: www.globalcommissionondrugs.org/wp-content/
themes/gcdp_v1/pdf/Global_Commission_Report_English.pdf (ac-
cessed 2015 Aug. 15).
16. The war on marijuana in black and white: billions of dollars
wasted on radically biased arrests. New York: American Civil
Liberties Union; 2013. Available: www.aclu.org/files/assets/
aclu-thewaronmarijuana-rel2.pdf (accessed 2015 June 23).
17. Hughes CE, Stevens A. What can we learn from the Portuguese
decriminalization of illicit drugs? Br J Criminol 2010;50:999-1022.
18. Nutt DJ, King LA, Philips LD. Drug harms in the UK: a multi-
criteria decision analysis. Lancet 2010;376:1558-65.
19. Fischer B, Imtiaz S, Rudzinski K, et al. Crude estimates of can-
nabis-attributable mortality and morbidity in Canada — implica-
tions for public health focused intervention priorities. J Public
Health (Oxf) 2015;Jan 28:pii: fdv005.
20. Drummer OH, Gerostamoulos J, Batziris H, et al. The involve-
ment of drugs in drivers of motor vehicles killed in Australian
road traffic crashes. Accid Anal Prev 2004;36:239-48.
21. Sewell R, Poling J, Sofuoglu M. The effect of cannabis com-
pared with alcohol on driving. Am J Addiction 2009;18:185-93.
22. Nocon A, Wittchen HU, Pfister H, et al. Dependence symptoms
in young cannabis users? A prospective epidemiological study.
J Psychiatr Res 2006;40:394-403.
23. Hall W. What has research over the past two decades revealed
about the adverse health effects of recreational cannabis use?
Addiction 2015;110:19-35.
24. Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users
show neuropsychological decline from childhood to midlife.
Proc Natl Acad Sci U S A 2012;40:E2657-2664.
25. MacCoun RJ, Reuter PH. Drug war heresies: learning from
other vices, time & places. Cambridge (UK): Cambridge Uni-
versity Press; 2001.
26. Simons-Morton B, Pickett W, Boyce W, et al. Cross-national com-
parison of adolescent drinking and cannabis use in the United States,
Canada, and the Netherlands. Int J Drug Policy 2010; 21:64-9.
27. Canadian Drug Policy Coalition. Getting to tomorrow: a report on
Canadian drug policy. Vancouver: Simon Fraser University; 2013.
Analysis
1216 CMAJ, November 3, 2015, 187(16)
28. Room R, Fischer B, Hall W, et al. Cannabis policy: moving beyond
stalemate. Oxford (UK): Oxford University Press/Beckley Founda-
tion Press; 2010.
29. Rolles S, Murkin G. How to regulate cannabis: a practical guide.
Bristol (UK): Transform Drug Policy Foundation; 2013. Avail-
able: www.unodc.org/documents/ungass2016/Contributions/Civil/
Transform-Drug-Policy-Foundation/How-to-Regulate-Cannabis
-Guide.pdf (accessed 2015 Aug. 16).
30. Pacula RL, Kilmer B, Wagenaar AC, et al. Developing public
health regulations for marijuana: lessons from alcohol and
tobacco. Am J Public Health 2014;104:1021-8.
31. Carroll R. Big Cannabis: Will legal weed grow to be America’s
next corporate titan? The Guardian [UK] 2014 Jan. 3. Available:
www.theguardian.com/politics/2014/jan/03/legal-marijuana
-colorado-big-tobacco-lobbying (accessed 2015 Apr. 30).
32. Gornall J. Europe under the Influence. BMJ 2014;348:g1166.
33. Jernigan DH. The global alcohol industry: an overview. Addic-
tion 2009;104(Suppl 1):6-12.
34. Cannabis policy framework. Toronto: Centre for Addiction and
Mental Health; 2014. Available: www.camh.ca/en/hospital/about_
camh/influencing_public_policy/Documents/CAMHCannabis
PolicyFramework.pdf (accessed 2015 June 12).
35. Room R. Legalizing a market for cannabis for pleasure: Colorado,
Washington, Uruguay and beyond. Addiction 2014;109:345-51.
36. Pardo B. Cannabis policy reforms in the Americas: a compara-
tive analysis of Colorado, Washington, and Uruguay. Int J Drug
Policy 2014;25:727-35.
37. Kilmer B, Kruithof K, Pardal M, et al. Multinational overview of
cannabis production regimes. Research and Documentation
Centre (WODC), Dutch Ministry of Security and Justice; 2013.
Available: www.rand.org/pubs/research_reports/RR510.html
(accessed 2015 June 12).
38. Walsh J, Ramsey G. Uruguay’s drug policy: major innovations,
major challenges. Washington (DC): Brookings/WALA; 2015.
Available: www.brookings.edu/~/media/Research/Files/Papers
/2015/04/global-drug-policy/Walsh--Uruguay-final.pdf?la=en (ac-
cessed 2015 Aug. 14).
39. Grotenhermen F, Leson G, Berghaus G, et al. Developing limits
for driving under cannabis. Addiction 2007;102:1910-7.
40. Marihuana y sus derivados: control y regulación del estado de
la importación, producción, adquisición, almacenamiento, com-
ercialización y distribución. Law no. 19.172. Senate and House
of Representatives of the Oriental Republic of Uruguay, meeting
in Assembly General. Available: www.correo.com.uy/otrosdoc-
umentos/pdf/Ley_19.172.pdf (accessed 2015 June 2).
41. Castaldi M. Uruguay to sell marijuana tax-free to undercut
drug traffickers. Reuters 2014 May 19. Available: www.
reuters.com/article/2014/05/19/us-uruguay-marijuana
-idUSKBN0DZ17Z20140519 (accessed 2015 June 11).
42. Bieleman B, Nijkamp R, Reimer J, et al. Coffeeshops in Neder-
land 2012 [Dutch]. Groningen (the Netherlands): WODC, min-
isterie van Veiligheid en Justitie, Den Haag; 2013. Available:
http://voc-nederland.org/persberichten_pdf/rapport-coffeeshops
-in-nederland-2012-2.pdf (accessed 2015 Sept. 8).
43. Toleration policy regarding soft drugs and coffee shops. Govern-
ment of the Netherlands. Available: www.government.nl/topics/
drugs/contents/toleration-policy-regarding-soft-drugs-and-coffee
-shops (accessed 2015 June 4).
44. Police discover more marijuana plantations in Randstad region.
DutchNews.nl 2015 Jan. 15. Available: www.dutchnews.nl/news/
archives /2014/01/police_discover_more_marijuana/ (accessed
2015 May 29).
45. Murkin G. Cannabis social clubs in Spain: legalisation without
commercialization. Transform 2015 Jan. 6. Available: www.tdpf
.org .uk/blog/cannabis-social-clubs-spain-legalisation-without
-commercialisation #.VLeZjsGV5R8.twitter (accessed 2015
May 16).
46. Resolución Slt/32/2015, De 15 de enero, por la que se aprueban
criterios en materia de salud pública para orientar a las aso-
ciaciones cannábicas y sus clubes sociales y las condiciones del
ejercicio de su actividad para los ayuntamientos de Cataluña.
Diari Oficial de la Generalitat de Catalunya (Official Gazette of the
Autonomous Government of Catalonia]. 2015 Jan. 29. Available:
http://portaldogc.gencat.cat/utilsEADOP/PDF/6799/1402549.pdf
(accessed 2015 Aug. 31).
47. Taylor H. Legislation passed to formally license Catalonia’s
cannabis clubs for first time. TalkingDrugs 2015 Feb. 3. Avail-
able: www.talkingdrugs.org/catalonia-cannabis-clubs-gain-formal
-licensing (accessed 2015 May 16).
48. Measure 91: Control, regulation, and taxation of marijuana and
industrial hemp act. People of the State of Oregon; 2014. Avail-
able: www.oregon.gov/olcc/marijuana/Documents /Measure91.
pdf (accessed 2015 May 22).
49. Colorado Amendment 64: Use and regulation of marijuana.
People of the State of Colorado; 2011. Available: www.fcgov.
com/mmj/pdf/amendment64.pdf (accessed 2015 May 11).
50. Marijuana Enforcement Division 1 CCR 212-2: Permanent rules
related to the Colorado Retail Marijuana Code. Denver: Colorad
Department of Revenue: Marijuana Enforcement Division;
2013:109. Available: www.colorado.gov/pacific/sites/default/file
Retail%20Marijuana%20Rules,%20Adopted% 20090913,%20
Effective%20101513%5B1%5D_0.pdf (accessed 2015 May 12)
51. Initiative measure no. 502. People of the State of Washington;
2011. Available: http://sos.wa.gov/_assets/elections/initiatives/
i502.pdf (accessed 2015 May 23).
52. Caulkins JP, Kilmer B, MacCoun RJ, et al. Design consider-
ations for legalizing cannabis: lessons inspired by analysis of
California’s Proposition 19. Addiction 2012;107:865-71.
53. Liquor Control Board clarifies next steps in its preparation to is
sue marijuana licenses [press release]. Olympia (WA): Washing
ton State Liquor and Cannabis Board; 2014 Feb. 19. Available:
www.liq.wa.gov/content/liquor-control-board-clarifies -next-ste
-its-preparation-issue-marijuana-licenses (accessed 2015 May
54. Frequently asked questions about I-502 advertising. Olymp
(WA): Washington State Liquor and Cannabis Board; 2015.
Available: http://liq.wa.gov/marijuana/faq_i502_advertising
#advertisingrules (accessed 2015 May 11).
55. Trans-High Corporation, D.B.A. High Times Magazine, The Daily
Doobie, LLC a corporate entity; and The Hemp Connoisseur, LLC,
a corporate entity v.The state of Colorado and John Hickenlooper
[civil action suit] 2013 May 29. Available: http://kln -law.
com/images /news_images/Marijuana-Magazines-Complaint .pd
(accessed 2015 June 17).
56. Kilmer B. 7 key questions on marijuana legalization [blog]. San
Monica (CA): Rand; 2013. Available: www.rand.org/blog
/2013/04/7-key-questions-on-marijuana-legalization.html (ac-
cessed 2015 June 17).
57. Bula F. Vancouver to become first city to regulate medical pot
pensaries. The Globe and Mail [Toronto] 2015 Apr. 22. Availabl
www.theglobeandmail.com/news/british-columbia/vancouver-t
-become-first-city-to-regulate-medical-pot-dispensaries/article
24071461/%3b/ (accessed 2015 June 29).
58. Bailey I. Victoria mulling new bylaws for marijuana dispensarie
The Globe and Mail [Toronto] 2015 May 7. Available: www.
theglobeandmail.com/news/british-columbia/victoria-mulling-n
-bylaws-for-marijuana-dispensaries/article24324753/ (accessed
2015 June 23).
59. Campbell CS, Smith GJ. Gambling in Canada — from vice to
disease to responsibility: a negotiated history. Can Bull Me
Hist 2003;20:121-49.
60. Lower the stakes: a public health approach to gambling in Briti
Columbia: Provincial health officer’s 2009 annual report. Victo-
ria: Office of the Provincial Health Officer BC; 2013. Available:
www2.gov.bc.ca/gov/DownloadAsset?assetId=EB445906BC214
EB4A44C1A075E3733&filename=gambling-in-bc.pdf (accessed
2015 June 21.
61. Majority supports study to evaluate taxation and regulation of
marijuana. Vancouver: Stop the Violence BC; 2013. Avail-
able: http://stoptheviolencebc.org/2013/04/18/majority-of
-british -columbians-support-pilot-study-to-evaluate-taxation-a
-regulation-of-marijuana (accessed 2015 Aug. 13).
62. Majority supports safe-injection sites. The Gazette [Montréal]
2008 June 7. Available: www.canada.com/montrealgazette/
story.html?id=f585e4fe-c262-41a8-b79a-d8329c379f26 (ac-
cessed 2015 June 5).
Affiliations: Department of Familiy Medicine (S. Spithoff)
Women’s College Hospital, Toronto, Ont.; Division of Popu
lation and Public Health (Emerson), BC Ministry of Health,
Victoria, BC; Not For Sale — the Netherlands (A. Spithoff),
Amsterdam, the Netherlands.
Contributors: Sheryl Spithoff conceived of and designed
article and wrote the first draft. Andrea Spithoff did most o
the acquisition of data and critically revised the article. Br
Emerson contributed substantially to the analysis and inte
pretation of data and critically revised the article. All of th
authors approved the final version to be published and ag
to act as guarantors of the work.
Acknowledgments: The authors thank Raquel Peyrau
Rebecca Jesseman, Meldon Kahan and the Women’s Colleg
Academic Family Health Team Peer Support Writing Group
for reviewing and providing helpful suggestions on earlier
drafts of this paper. The authors also thank Pim Imenkamp
Laura Gutierrez and Rebecca Abavi for assisting in the bac
ground research for this paper.
Disclaimer: The opinions stated in this commentary
those of the authors and not of their affiliated organization
1216 CMAJ, November 3, 2015, 187(16)
28. Room R, Fischer B, Hall W, et al. Cannabis policy: moving beyond
stalemate. Oxford (UK): Oxford University Press/Beckley Founda-
tion Press; 2010.
29. Rolles S, Murkin G. How to regulate cannabis: a practical guide.
Bristol (UK): Transform Drug Policy Foundation; 2013. Avail-
able: www.unodc.org/documents/ungass2016/Contributions/Civil/
Transform-Drug-Policy-Foundation/How-to-Regulate-Cannabis
-Guide.pdf (accessed 2015 Aug. 16).
30. Pacula RL, Kilmer B, Wagenaar AC, et al. Developing public
health regulations for marijuana: lessons from alcohol and
tobacco. Am J Public Health 2014;104:1021-8.
31. Carroll R. Big Cannabis: Will legal weed grow to be America’s
next corporate titan? The Guardian [UK] 2014 Jan. 3. Available:
www.theguardian.com/politics/2014/jan/03/legal-marijuana
-colorado-big-tobacco-lobbying (accessed 2015 Apr. 30).
32. Gornall J. Europe under the Influence. BMJ 2014;348:g1166.
33. Jernigan DH. The global alcohol industry: an overview. Addic-
tion 2009;104(Suppl 1):6-12.
34. Cannabis policy framework. Toronto: Centre for Addiction and
Mental Health; 2014. Available: www.camh.ca/en/hospital/about_
camh/influencing_public_policy/Documents/CAMHCannabis
PolicyFramework.pdf (accessed 2015 June 12).
35. Room R. Legalizing a market for cannabis for pleasure: Colorado,
Washington, Uruguay and beyond. Addiction 2014;109:345-51.
36. Pardo B. Cannabis policy reforms in the Americas: a compara-
tive analysis of Colorado, Washington, and Uruguay. Int J Drug
Policy 2014;25:727-35.
37. Kilmer B, Kruithof K, Pardal M, et al. Multinational overview of
cannabis production regimes. Research and Documentation
Centre (WODC), Dutch Ministry of Security and Justice; 2013.
Available: www.rand.org/pubs/research_reports/RR510.html
(accessed 2015 June 12).
38. Walsh J, Ramsey G. Uruguay’s drug policy: major innovations,
major challenges. Washington (DC): Brookings/WALA; 2015.
Available: www.brookings.edu/~/media/Research/Files/Papers
/2015/04/global-drug-policy/Walsh--Uruguay-final.pdf?la=en (ac-
cessed 2015 Aug. 14).
39. Grotenhermen F, Leson G, Berghaus G, et al. Developing limits
for driving under cannabis. Addiction 2007;102:1910-7.
40. Marihuana y sus derivados: control y regulación del estado de
la importación, producción, adquisición, almacenamiento, com-
ercialización y distribución. Law no. 19.172. Senate and House
of Representatives of the Oriental Republic of Uruguay, meeting
in Assembly General. Available: www.correo.com.uy/otrosdoc-
umentos/pdf/Ley_19.172.pdf (accessed 2015 June 2).
41. Castaldi M. Uruguay to sell marijuana tax-free to undercut
drug traffickers. Reuters 2014 May 19. Available: www.
reuters.com/article/2014/05/19/us-uruguay-marijuana
-idUSKBN0DZ17Z20140519 (accessed 2015 June 11).
42. Bieleman B, Nijkamp R, Reimer J, et al. Coffeeshops in Neder-
land 2012 [Dutch]. Groningen (the Netherlands): WODC, min-
isterie van Veiligheid en Justitie, Den Haag; 2013. Available:
http://voc-nederland.org/persberichten_pdf/rapport-coffeeshops
-in-nederland-2012-2.pdf (accessed 2015 Sept. 8).
43. Toleration policy regarding soft drugs and coffee shops. Govern-
ment of the Netherlands. Available: www.government.nl/topics/
drugs/contents/toleration-policy-regarding-soft-drugs-and-coffee
-shops (accessed 2015 June 4).
44. Police discover more marijuana plantations in Randstad region.
DutchNews.nl 2015 Jan. 15. Available: www.dutchnews.nl/news/
archives /2014/01/police_discover_more_marijuana/ (accessed
2015 May 29).
45. Murkin G. Cannabis social clubs in Spain: legalisation without
commercialization. Transform 2015 Jan. 6. Available: www.tdpf
.org .uk/blog/cannabis-social-clubs-spain-legalisation-without
-commercialisation #.VLeZjsGV5R8.twitter (accessed 2015
May 16).
46. Resolución Slt/32/2015, De 15 de enero, por la que se aprueban
criterios en materia de salud pública para orientar a las aso-
ciaciones cannábicas y sus clubes sociales y las condiciones del
ejercicio de su actividad para los ayuntamientos de Cataluña.
Diari Oficial de la Generalitat de Catalunya (Official Gazette of the
Autonomous Government of Catalonia]. 2015 Jan. 29. Available:
http://portaldogc.gencat.cat/utilsEADOP/PDF/6799/1402549.pdf
(accessed 2015 Aug. 31).
47. Taylor H. Legislation passed to formally license Catalonia’s
cannabis clubs for first time. TalkingDrugs 2015 Feb. 3. Avail-
able: www.talkingdrugs.org/catalonia-cannabis-clubs-gain-formal
-licensing (accessed 2015 May 16).
48. Measure 91: Control, regulation, and taxation of marijuana and
industrial hemp act. People of the State of Oregon; 2014. Avail-
able: www.oregon.gov/olcc/marijuana/Documents /Measure91.
pdf (accessed 2015 May 22).
49. Colorado Amendment 64: Use and regulation of marijuana.
People of the State of Colorado; 2011. Available: www.fcgov.
com/mmj/pdf/amendment64.pdf (accessed 2015 May 11).
50. Marijuana Enforcement Division 1 CCR 212-2: Permanent rules
related to the Colorado Retail Marijuana Code. Denver: Colorad
Department of Revenue: Marijuana Enforcement Division;
2013:109. Available: www.colorado.gov/pacific/sites/default/file
Retail%20Marijuana%20Rules,%20Adopted% 20090913,%20
Effective%20101513%5B1%5D_0.pdf (accessed 2015 May 12)
51. Initiative measure no. 502. People of the State of Washington;
2011. Available: http://sos.wa.gov/_assets/elections/initiatives/
i502.pdf (accessed 2015 May 23).
52. Caulkins JP, Kilmer B, MacCoun RJ, et al. Design consider-
ations for legalizing cannabis: lessons inspired by analysis of
California’s Proposition 19. Addiction 2012;107:865-71.
53. Liquor Control Board clarifies next steps in its preparation to is
sue marijuana licenses [press release]. Olympia (WA): Washing
ton State Liquor and Cannabis Board; 2014 Feb. 19. Available:
www.liq.wa.gov/content/liquor-control-board-clarifies -next-ste
-its-preparation-issue-marijuana-licenses (accessed 2015 May
54. Frequently asked questions about I-502 advertising. Olymp
(WA): Washington State Liquor and Cannabis Board; 2015.
Available: http://liq.wa.gov/marijuana/faq_i502_advertising
#advertisingrules (accessed 2015 May 11).
55. Trans-High Corporation, D.B.A. High Times Magazine, The Daily
Doobie, LLC a corporate entity; and The Hemp Connoisseur, LLC,
a corporate entity v.The state of Colorado and John Hickenlooper
[civil action suit] 2013 May 29. Available: http://kln -law.
com/images /news_images/Marijuana-Magazines-Complaint .pd
(accessed 2015 June 17).
56. Kilmer B. 7 key questions on marijuana legalization [blog]. San
Monica (CA): Rand; 2013. Available: www.rand.org/blog
/2013/04/7-key-questions-on-marijuana-legalization.html (ac-
cessed 2015 June 17).
57. Bula F. Vancouver to become first city to regulate medical pot
pensaries. The Globe and Mail [Toronto] 2015 Apr. 22. Availabl
www.theglobeandmail.com/news/british-columbia/vancouver-t
-become-first-city-to-regulate-medical-pot-dispensaries/article
24071461/%3b/ (accessed 2015 June 29).
58. Bailey I. Victoria mulling new bylaws for marijuana dispensarie
The Globe and Mail [Toronto] 2015 May 7. Available: www.
theglobeandmail.com/news/british-columbia/victoria-mulling-n
-bylaws-for-marijuana-dispensaries/article24324753/ (accessed
2015 June 23).
59. Campbell CS, Smith GJ. Gambling in Canada — from vice to
disease to responsibility: a negotiated history. Can Bull Me
Hist 2003;20:121-49.
60. Lower the stakes: a public health approach to gambling in Briti
Columbia: Provincial health officer’s 2009 annual report. Victo-
ria: Office of the Provincial Health Officer BC; 2013. Available:
www2.gov.bc.ca/gov/DownloadAsset?assetId=EB445906BC214
EB4A44C1A075E3733&filename=gambling-in-bc.pdf (accessed
2015 June 21.
61. Majority supports study to evaluate taxation and regulation of
marijuana. Vancouver: Stop the Violence BC; 2013. Avail-
able: http://stoptheviolencebc.org/2013/04/18/majority-of
-british -columbians-support-pilot-study-to-evaluate-taxation-a
-regulation-of-marijuana (accessed 2015 Aug. 13).
62. Majority supports safe-injection sites. The Gazette [Montréal]
2008 June 7. Available: www.canada.com/montrealgazette/
story.html?id=f585e4fe-c262-41a8-b79a-d8329c379f26 (ac-
cessed 2015 June 5).
Affiliations: Department of Familiy Medicine (S. Spithoff)
Women’s College Hospital, Toronto, Ont.; Division of Popu
lation and Public Health (Emerson), BC Ministry of Health,
Victoria, BC; Not For Sale — the Netherlands (A. Spithoff),
Amsterdam, the Netherlands.
Contributors: Sheryl Spithoff conceived of and designed
article and wrote the first draft. Andrea Spithoff did most o
the acquisition of data and critically revised the article. Br
Emerson contributed substantially to the analysis and inte
pretation of data and critically revised the article. All of th
authors approved the final version to be published and ag
to act as guarantors of the work.
Acknowledgments: The authors thank Raquel Peyrau
Rebecca Jesseman, Meldon Kahan and the Women’s Colleg
Academic Family Health Team Peer Support Writing Group
for reviewing and providing helpful suggestions on earlier
drafts of this paper. The authors also thank Pim Imenkamp
Laura Gutierrez and Rebecca Abavi for assisting in the bac
ground research for this paper.
Disclaimer: The opinions stated in this commentary
those of the authors and not of their affiliated organization
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 6
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.