ESA50 - Capability for Work Questionnaire for Health Assessment
VerifiedAdded on 2022/12/29
|28
|7382
|1
Homework Assignment
AI Summary
This document represents a completed ESA50 questionnaire, which is used by the Health Assessment Advisory Service to determine an individual's capability for work and eligibility for Employment and Support Allowance (ESA). The questionnaire covers various aspects, including personal details, medical history, and the impact of health conditions on daily activities. It includes sections on general practitioner information, other healthcare professionals involved, and details about disabilities, illnesses, and health conditions, including long-term effects of coronavirus (long COVID) and post-COVID-19 syndrome. The document also addresses medication, hospital treatments, and cancer treatment, providing a comprehensive overview of the individual's health and its effects on their ability to work. The completed questionnaire is to be returned with supporting medical information to aid in the assessment process. The individual has been in hospital for over 28 days in the last 12 months, and is also experiencing bone pain. This assignment is a part of a health assessment process.
Capability for Work questionna
We have many ways we can communicate with you.
If you would like braille, British Sign Language, email, a hearing loop,
translations, large print, audio or something else please call us on
0800 169 0310 or textphone 0800 169 0314 and tell us which you need.
If you live in Wales and want this questionnaire in Welsh please call us
on 0800 328 1744.
Calls to 0800 numbers are free from landlines and mobiles.
Equality and diversity
We are committed to treating people fairly, regardless of their disability, ethnicity,
sex, sexual orientation, transgender status, marital or civil partnership status, age,
religion or beliefs. Please contact us if you have any concerns.
What you need to do:
• please fill in this questionnaire and send it back to the Health Assessment
Advisory Service by the date on the letter that it came with. The Health
Assessment Advisory Service will use the information you provide to decide
if you need to come for a face-to-face assessment or not. We will use this
information to give you the best support we can and pay you the right amount
of benefit.
• you must send it back by the date we have asked you to in the enclosed letter.
• read this questionnaire carefully and make sure you answer all the questions
in full.
• write in black ink and use CAPITAL LETTERS. If you want to, you can download
a copy of the questionnaire to your computer and fill it in. Go to www.gov.uk
and search for ESA50.
• return the completed questionnaire using the enclosed envelope. It does not
need a stamp. Do not send it or take it to your Jobcentre Plus office.
• send copies of all your medical or other information back with your
questionnaire. We do not always contact your medical professionals so this
information is important, and should let us know how your disability, illness
or health condition affect how you can do things on a daily basis. A list of
information we find helpful is on page 5.
• only send us copies of medical or other information if you already have them.
Do not ask or pay for new information or send us original documents. Please
write your National Insurance Number on each piece of information you send
to us.
• make sure you fill in the ‘About you’ section on page 2 in full.
01/21 1 ESA50
We have many ways we can communicate with you.
If you would like braille, British Sign Language, email, a hearing loop,
translations, large print, audio or something else please call us on
0800 169 0310 or textphone 0800 169 0314 and tell us which you need.
If you live in Wales and want this questionnaire in Welsh please call us
on 0800 328 1744.
Calls to 0800 numbers are free from landlines and mobiles.
Equality and diversity
We are committed to treating people fairly, regardless of their disability, ethnicity,
sex, sexual orientation, transgender status, marital or civil partnership status, age,
religion or beliefs. Please contact us if you have any concerns.
What you need to do:
• please fill in this questionnaire and send it back to the Health Assessment
Advisory Service by the date on the letter that it came with. The Health
Assessment Advisory Service will use the information you provide to decide
if you need to come for a face-to-face assessment or not. We will use this
information to give you the best support we can and pay you the right amount
of benefit.
• you must send it back by the date we have asked you to in the enclosed letter.
• read this questionnaire carefully and make sure you answer all the questions
in full.
• write in black ink and use CAPITAL LETTERS. If you want to, you can download
a copy of the questionnaire to your computer and fill it in. Go to www.gov.uk
and search for ESA50.
• return the completed questionnaire using the enclosed envelope. It does not
need a stamp. Do not send it or take it to your Jobcentre Plus office.
• send copies of all your medical or other information back with your
questionnaire. We do not always contact your medical professionals so this
information is important, and should let us know how your disability, illness
or health condition affect how you can do things on a daily basis. A list of
information we find helpful is on page 5.
• only send us copies of medical or other information if you already have them.
Do not ask or pay for new information or send us original documents. Please
write your National Insurance Number on each piece of information you send
to us.
• make sure you fill in the ‘About you’ section on page 2 in full.
01/21 1 ESA50
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
If you need help filling in the questionnaire, you can:
• ask a friend, relative, carer or support worker to help you
• call Jobcentre Plus on 0800 169 0310 to arrange for a trained advisor to talk
you through the questions over the phone. Please do not go into your local
Jobcentre Plus.
In some cases, your answers can be written down for you. You can ask for your
questionnaire to be sent to you by post to check.
Your Employment and Support Allowance (ESA) payments may
stop if you do not fill in this questionnaire and send it to the Health
Assessment Advisory Service by the date we have asked you to.
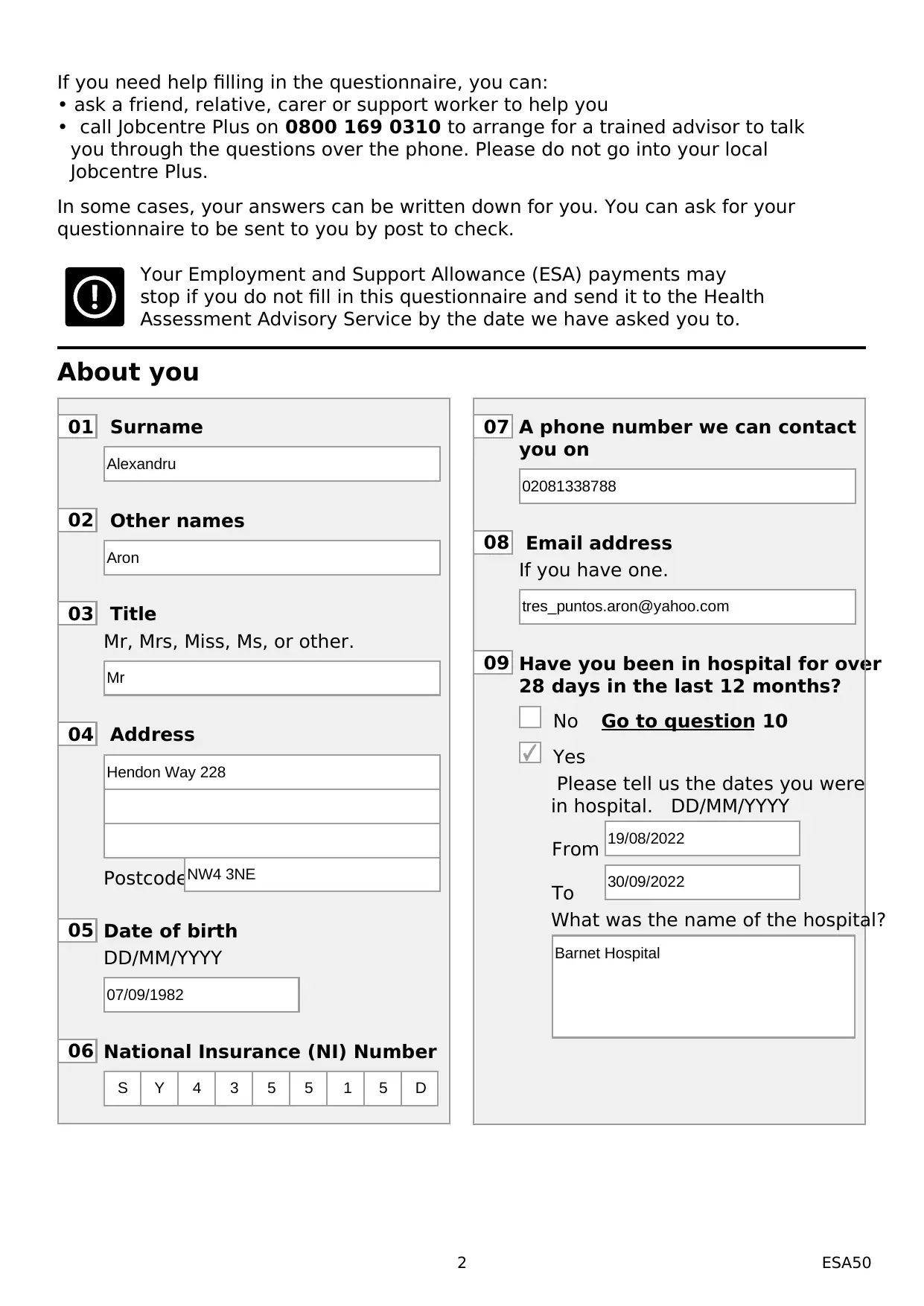
About you
01 Surname
02 Other names
03 Title
Mr, Mrs, Miss, Ms, or other.
04 Address
Postcode
05 Date of birth
DD/MM/YYYY
06 National Insurance (NI) Number
07 A phone number we can contact
you on
08 Email address
If you have one.
09 Have you been in hospital for over
28 days in the last 12 months?
No Go to question 10
Yes
Please tell us the dates you were
in hospital. DD/MM/YYYY
From
To
What was the name of the hospital?
2 ESA50
Alexandru
Aron
Mr
Hendon Way 228
NW4 3NE
07/09/1982
S Y 4 3 5 5 1 5 D
02081338788
tres_puntos.aron@yahoo.com
19/08/2022
30/09/2022
Barnet Hospital
• ask a friend, relative, carer or support worker to help you
• call Jobcentre Plus on 0800 169 0310 to arrange for a trained advisor to talk
you through the questions over the phone. Please do not go into your local
Jobcentre Plus.
In some cases, your answers can be written down for you. You can ask for your
questionnaire to be sent to you by post to check.
Your Employment and Support Allowance (ESA) payments may
stop if you do not fill in this questionnaire and send it to the Health
Assessment Advisory Service by the date we have asked you to.
About you
01 Surname
02 Other names
03 Title
Mr, Mrs, Miss, Ms, or other.
04 Address
Postcode
05 Date of birth
DD/MM/YYYY
06 National Insurance (NI) Number
07 A phone number we can contact
you on
08 Email address
If you have one.
09 Have you been in hospital for over
28 days in the last 12 months?
No Go to question 10
Yes
Please tell us the dates you were
in hospital. DD/MM/YYYY
From
To
What was the name of the hospital?
2 ESA50
Alexandru
Aron
Mr
Hendon Way 228
NW4 3NE
07/09/1982
S Y 4 3 5 5 1 5 D
02081338788
tres_puntos.aron@yahoo.com
19/08/2022
30/09/2022
Barnet Hospital
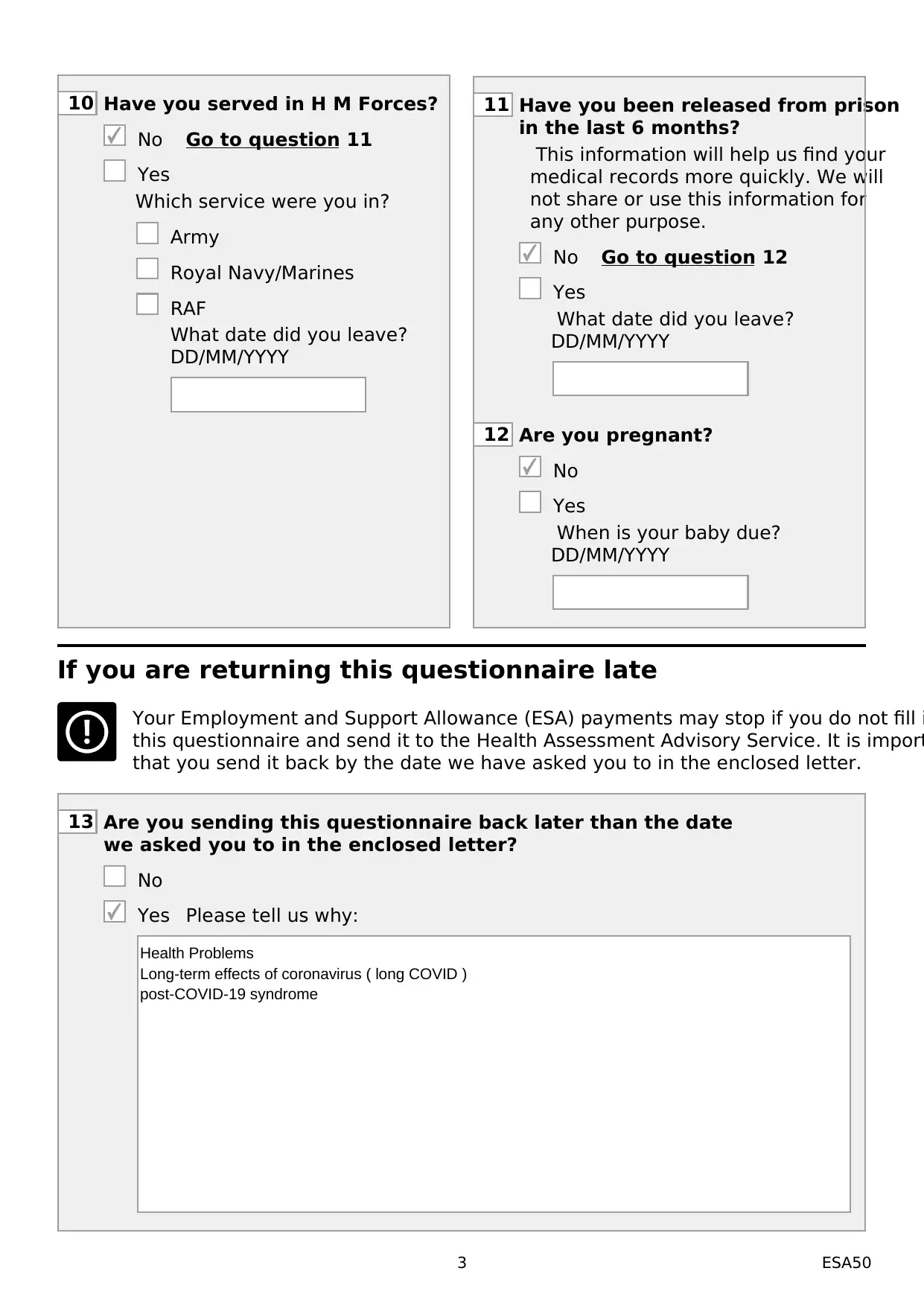
10 Have you served in H M Forces?
No Go to question 11
Yes
Which service were you in?
Army
Royal Navy/Marines
RAF
What date did you leave?
DD/MM/YYYY
11 Have you been released from prison
in the last 6 months?
This information will help us find your
medical records more quickly. We will
not share or use this information for
any other purpose.
No Go to question 12
Yes
What date did you leave?
DD/MM/YYYY
12 Are you pregnant?
No
Yes
When is your baby due?
DD/MM/YYYY
If you are returning this questionnaire late
Your Employment and Support Allowance (ESA) payments may stop if you do not fill i
this questionnaire and send it to the Health Assessment Advisory Service. It is import
that you send it back by the date we have asked you to in the enclosed letter.
13 Are you sending this questionnaire back later than the date
we asked you to in the enclosed letter?
No
Yes Please tell us why:
3 ESA50
Health Problems
Long-term effects of coronavirus ( long COVID )
post-COVID-19 syndrome
No Go to question 11
Yes
Which service were you in?
Army
Royal Navy/Marines
RAF
What date did you leave?
DD/MM/YYYY
11 Have you been released from prison
in the last 6 months?
This information will help us find your
medical records more quickly. We will
not share or use this information for
any other purpose.
No Go to question 12
Yes
What date did you leave?
DD/MM/YYYY
12 Are you pregnant?
No
Yes
When is your baby due?
DD/MM/YYYY
If you are returning this questionnaire late
Your Employment and Support Allowance (ESA) payments may stop if you do not fill i
this questionnaire and send it to the Health Assessment Advisory Service. It is import
that you send it back by the date we have asked you to in the enclosed letter.
13 Are you sending this questionnaire back later than the date
we asked you to in the enclosed letter?
No
Yes Please tell us why:
3 ESA50
Health Problems
Long-term effects of coronavirus ( long COVID )
post-COVID-19 syndrome
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
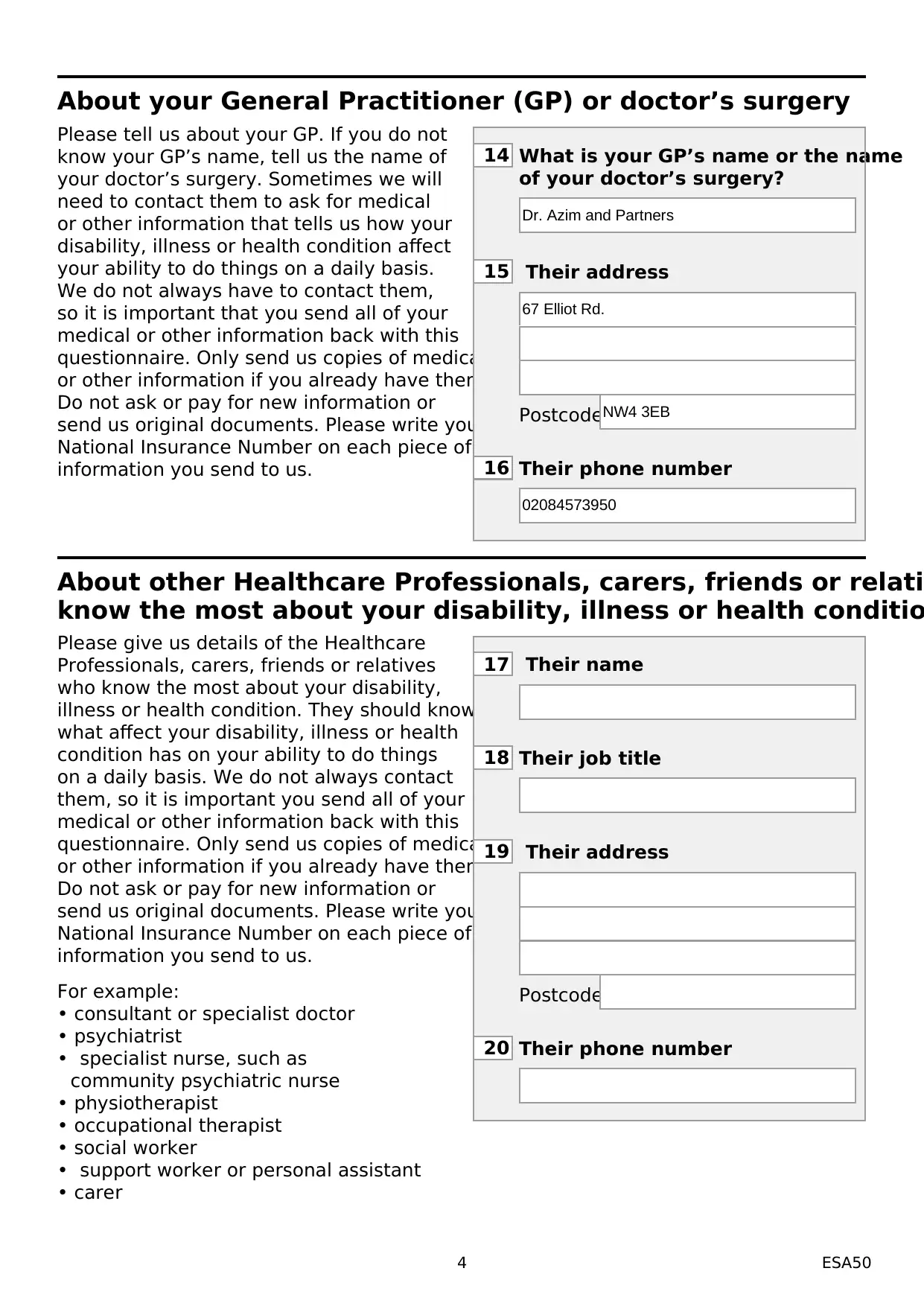
About your General Practitioner (GP) or doctor’s surgery
Please tell us about your GP. If you do not
know your GP’s name, tell us the name of
your doctor’s surgery. Sometimes we will
need to contact them to ask for medical
or other information that tells us how your
disability, illness or health condition affect
your ability to do things on a daily basis.
We do not always have to contact them,
so it is important that you send all of your
medical or other information back with this
questionnaire. Only send us copies of medical
or other information if you already have them.
Do not ask or pay for new information or
send us original documents. Please write your
National Insurance Number on each piece of
information you send to us.
14 What is your GP’s name or the name
of your doctor’s surgery?
15 Their address
Postcode
16 Their phone number
About other Healthcare Professionals, carers, friends or relati
know the most about your disability, illness or health conditio
Please give us details of the Healthcare
Professionals, carers, friends or relatives
who know the most about your disability,
illness or health condition. They should know
what affect your disability, illness or health
condition has on your ability to do things
on a daily basis. We do not always contact
them, so it is important you send all of your
medical or other information back with this
questionnaire. Only send us copies of medical
or other information if you already have them.
Do not ask or pay for new information or
send us original documents. Please write your
National Insurance Number on each piece of
information you send to us.
For example:
• consultant or specialist doctor
• psychiatrist
• specialist nurse, such as
community psychiatric nurse
• physiotherapist
• occupational therapist
• social worker
• support worker or personal assistant
• carer
17 Their name
18 Their job title
19 Their address
Postcode
20 Their phone number
4 ESA50
Dr. Azim and Partners
67 Elliot Rd.
NW4 3EB
02084573950
Please tell us about your GP. If you do not
know your GP’s name, tell us the name of
your doctor’s surgery. Sometimes we will
need to contact them to ask for medical
or other information that tells us how your
disability, illness or health condition affect
your ability to do things on a daily basis.
We do not always have to contact them,
so it is important that you send all of your
medical or other information back with this
questionnaire. Only send us copies of medical
or other information if you already have them.
Do not ask or pay for new information or
send us original documents. Please write your
National Insurance Number on each piece of
information you send to us.
14 What is your GP’s name or the name
of your doctor’s surgery?
15 Their address
Postcode
16 Their phone number
About other Healthcare Professionals, carers, friends or relati
know the most about your disability, illness or health conditio
Please give us details of the Healthcare
Professionals, carers, friends or relatives
who know the most about your disability,
illness or health condition. They should know
what affect your disability, illness or health
condition has on your ability to do things
on a daily basis. We do not always contact
them, so it is important you send all of your
medical or other information back with this
questionnaire. Only send us copies of medical
or other information if you already have them.
Do not ask or pay for new information or
send us original documents. Please write your
National Insurance Number on each piece of
information you send to us.
For example:
• consultant or specialist doctor
• psychiatrist
• specialist nurse, such as
community psychiatric nurse
• physiotherapist
• occupational therapist
• social worker
• support worker or personal assistant
• carer
17 Their name
18 Their job title
19 Their address
Postcode
20 Their phone number
4 ESA50
Dr. Azim and Partners
67 Elliot Rd.
NW4 3EB
02084573950
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
About medical or other information you may already have
Things the Health Assessment
Advisory Service would like to see,
if you already have them –
Reports, care or treatment plans
about you from:
• GPs
• hospital doctors
• specialist nurses
• community psychiatric nurses
• occupational therapists
• physiotherapists
• social workers
• support workers
• learning disability support teams
• counsellors or carers.
Medical test results including:
• scans
• audiology
• the results of x-rays, but not
the x-rays themselves.
Things like:
• your current prescription list
• your statement of special educational needs
• epilepsy seizure diary
• your certificate of visual impairment.
Other information:
• Hospital Passports, this is a written record
kept by people with learning disabilities
to provide hospital staff with important
information about them and their health
when they are admitted to hospital
• a diary of your symptoms if your disability,
illness or health condition varies from day to
day
• long-stay hospital information including date
of admission, length of stay and the hospital
name and address.
Remember – only send us copies of medical
or other information if you already have them.
Do not ask or pay for new information or
send us original documents. Please write your
National Insurance Number on each piece of
information you send to us.
Things the Health Assessment
Advisory Service do not need to see
General information about your medical
conditions that are not about you personally.
Such as:
• photographs
• letters about other benefits
• fact sheets about your medication
• internet printouts
• statement of Fitness for Work, otherwise
known as fit notes, medical certificates,
doctor’s statements or sick notes
• appointment letters.
3
5
5 ESA50
Things the Health Assessment
Advisory Service would like to see,
if you already have them –
Reports, care or treatment plans
about you from:
• GPs
• hospital doctors
• specialist nurses
• community psychiatric nurses
• occupational therapists
• physiotherapists
• social workers
• support workers
• learning disability support teams
• counsellors or carers.
Medical test results including:
• scans
• audiology
• the results of x-rays, but not
the x-rays themselves.
Things like:
• your current prescription list
• your statement of special educational needs
• epilepsy seizure diary
• your certificate of visual impairment.
Other information:
• Hospital Passports, this is a written record
kept by people with learning disabilities
to provide hospital staff with important
information about them and their health
when they are admitted to hospital
• a diary of your symptoms if your disability,
illness or health condition varies from day to
day
• long-stay hospital information including date
of admission, length of stay and the hospital
name and address.
Remember – only send us copies of medical
or other information if you already have them.
Do not ask or pay for new information or
send us original documents. Please write your
National Insurance Number on each piece of
information you send to us.
Things the Health Assessment
Advisory Service do not need to see
General information about your medical
conditions that are not about you personally.
Such as:
• photographs
• letters about other benefits
• fact sheets about your medication
• internet printouts
• statement of Fitness for Work, otherwise
known as fit notes, medical certificates,
doctor’s statements or sick notes
• appointment letters.
3
5
5 ESA50
Cancer treatment
IMPORTANT: if your cancer treatment is affecting you and you have no
other health conditions, you do not have to answer all the questions on
this questionnaire.
21 Do you have cancer?
No Go to ‘About your disabilities,
illnesses or health conditions’
on page 7
Yes Go to question 22
22 Are you having, waiting for or
recovering from chemotherapy or
radiotherapy treatment for cancer?
No Go to ‘About your disabilities,
illnesses or health conditions’
on page 7
Yes Please make sure page 27 is
filled in and signed by your
Healthcare Professional. This
may include a GP, hospital
doctor or clinical nurse who
is aware of your cancer
treatment. When your
Healthcare Professional has
signed page 28 and you have
signed page 25 you can then
return this questionnaire using
the enclosed envelope.
23 Do you have other health problems,
as well as cancer and the problems
resulting from your cancer treatment?
No Please make sure page 27 has
been filled in and signed by
your Healthcare Professional
and you have signed page
25. You can then return
this questionnaire using the
enclosed envelope.
Yes Please fill in the rest of this
questionnaire.
6 ESA50
IMPORTANT: if your cancer treatment is affecting you and you have no
other health conditions, you do not have to answer all the questions on
this questionnaire.
21 Do you have cancer?
No Go to ‘About your disabilities,
illnesses or health conditions’
on page 7
Yes Go to question 22
22 Are you having, waiting for or
recovering from chemotherapy or
radiotherapy treatment for cancer?
No Go to ‘About your disabilities,
illnesses or health conditions’
on page 7
Yes Please make sure page 27 is
filled in and signed by your
Healthcare Professional. This
may include a GP, hospital
doctor or clinical nurse who
is aware of your cancer
treatment. When your
Healthcare Professional has
signed page 28 and you have
signed page 25 you can then
return this questionnaire using
the enclosed envelope.
23 Do you have other health problems,
as well as cancer and the problems
resulting from your cancer treatment?
No Please make sure page 27 has
been filled in and signed by
your Healthcare Professional
and you have signed page
25. You can then return
this questionnaire using the
enclosed envelope.
Yes Please fill in the rest of this
questionnaire.
6 ESA50
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
About your disabilities, illnesses or health conditions
We will ask you specific questions about how your disability, illness or health condition
affect your ability to do things on a daily basis in the rest of this questionnaire.
24 What are your disabilities, illnesses or health conditions?
Tell us how they affect you, when they started and if you think any of your
conditions are linked to drugs or alcohol.
Also tell us about any aids you use, such as a wheelchair or hearing aid and anything
else you think we should know about your disabilities, illnesses or health conditions.
If you need more space, please use page 24 or a separate sheet of paper with your
National Insurance Number written on it.
7 ESA50
Long-term effects of coronavirus ( long COVID )
post-COVID-19 syndrome
Bone pain, I can barely move
We will ask you specific questions about how your disability, illness or health condition
affect your ability to do things on a daily basis in the rest of this questionnaire.
24 What are your disabilities, illnesses or health conditions?
Tell us how they affect you, when they started and if you think any of your
conditions are linked to drugs or alcohol.
Also tell us about any aids you use, such as a wheelchair or hearing aid and anything
else you think we should know about your disabilities, illnesses or health conditions.
If you need more space, please use page 24 or a separate sheet of paper with your
National Insurance Number written on it.
7 ESA50
Long-term effects of coronavirus ( long COVID )
post-COVID-19 syndrome
Bone pain, I can barely move
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
25 What tablets, liquids, inhalers or other medication are you taking and
are there any side effects?
You can find a list of your medications on your latest prescription. If you need more spac
please use page 24 or a separate sheet of paper with your National Insurance Number
written on it.
Hospital, clinic or special treatment like dialysis or rehabilitat
treatment
Use this section to tell us about any:
• hospital or clinic treatment you are having
• hospital or clinic treatment you expect to have in the near future
• special treatment you are having such as dialysis or rehabilitation treatment.
Please also tell us about any special treatment you have which you may not
go to a hospital or clinic for.
26 What hospital, clinic or special treatments are you getting?
For example, the treatment you are having, where you get it and how often.
If you are expecting to have treatment in the near future, tell us what the
treatment will be and the date it is due to start.
If you need more space, please use page 24 or a separate sheet of paper with
your National Insurance Number written on it.
8 ESA50
are there any side effects?
You can find a list of your medications on your latest prescription. If you need more spac
please use page 24 or a separate sheet of paper with your National Insurance Number
written on it.
Hospital, clinic or special treatment like dialysis or rehabilitat
treatment
Use this section to tell us about any:
• hospital or clinic treatment you are having
• hospital or clinic treatment you expect to have in the near future
• special treatment you are having such as dialysis or rehabilitation treatment.
Please also tell us about any special treatment you have which you may not
go to a hospital or clinic for.
26 What hospital, clinic or special treatments are you getting?
For example, the treatment you are having, where you get it and how often.
If you are expecting to have treatment in the near future, tell us what the
treatment will be and the date it is due to start.
If you need more space, please use page 24 or a separate sheet of paper with
your National Insurance Number written on it.
8 ESA50
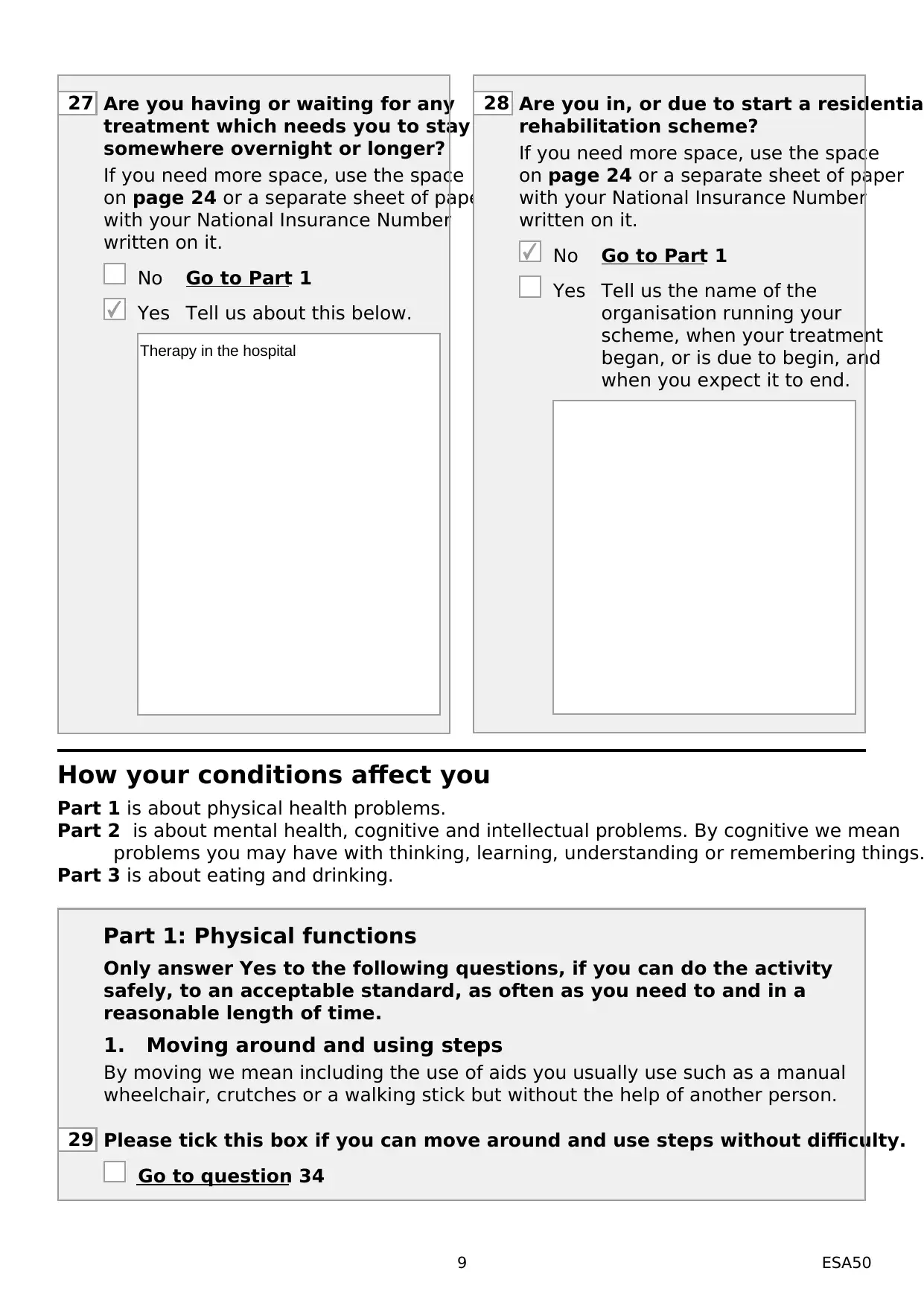
27 Are you having or waiting for any
treatment which needs you to stay
somewhere overnight or longer?
If you need more space, use the space
on page 24 or a separate sheet of paper
with your National Insurance Number
written on it.
No Go to Part 1
Yes Tell us about this below.
28 Are you in, or due to start a residentia
rehabilitation scheme?
If you need more space, use the space
on page 24 or a separate sheet of paper
with your National Insurance Number
written on it.
No Go to Part 1
Yes Tell us the name of the
organisation running your
scheme, when your treatment
began, or is due to begin, and
when you expect it to end.
How your conditions affect you
Part 1 is about physical health problems.
Part 2 is about mental health, cognitive and intellectual problems. By cognitive we mean
problems you may have with thinking, learning, understanding or remembering things.
Part 3 is about eating and drinking.
Part 1: Physical functions
Only answer Yes to the following questions, if you can do the activity
safely, to an acceptable standard, as often as you need to and in a
reasonable length of time.
1. Moving around and using steps
By moving we mean including the use of aids you usually use such as a manual
wheelchair, crutches or a walking stick but without the help of another person.
29 Please tick this box if you can move around and use steps without difficulty.
Go to question 34
9 ESA50
Therapy in the hospital
treatment which needs you to stay
somewhere overnight or longer?
If you need more space, use the space
on page 24 or a separate sheet of paper
with your National Insurance Number
written on it.
No Go to Part 1
Yes Tell us about this below.
28 Are you in, or due to start a residentia
rehabilitation scheme?
If you need more space, use the space
on page 24 or a separate sheet of paper
with your National Insurance Number
written on it.
No Go to Part 1
Yes Tell us the name of the
organisation running your
scheme, when your treatment
began, or is due to begin, and
when you expect it to end.
How your conditions affect you
Part 1 is about physical health problems.
Part 2 is about mental health, cognitive and intellectual problems. By cognitive we mean
problems you may have with thinking, learning, understanding or remembering things.
Part 3 is about eating and drinking.
Part 1: Physical functions
Only answer Yes to the following questions, if you can do the activity
safely, to an acceptable standard, as often as you need to and in a
reasonable length of time.
1. Moving around and using steps
By moving we mean including the use of aids you usually use such as a manual
wheelchair, crutches or a walking stick but without the help of another person.
29 Please tick this box if you can move around and use steps without difficulty.
Go to question 34
9 ESA50
Therapy in the hospital
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
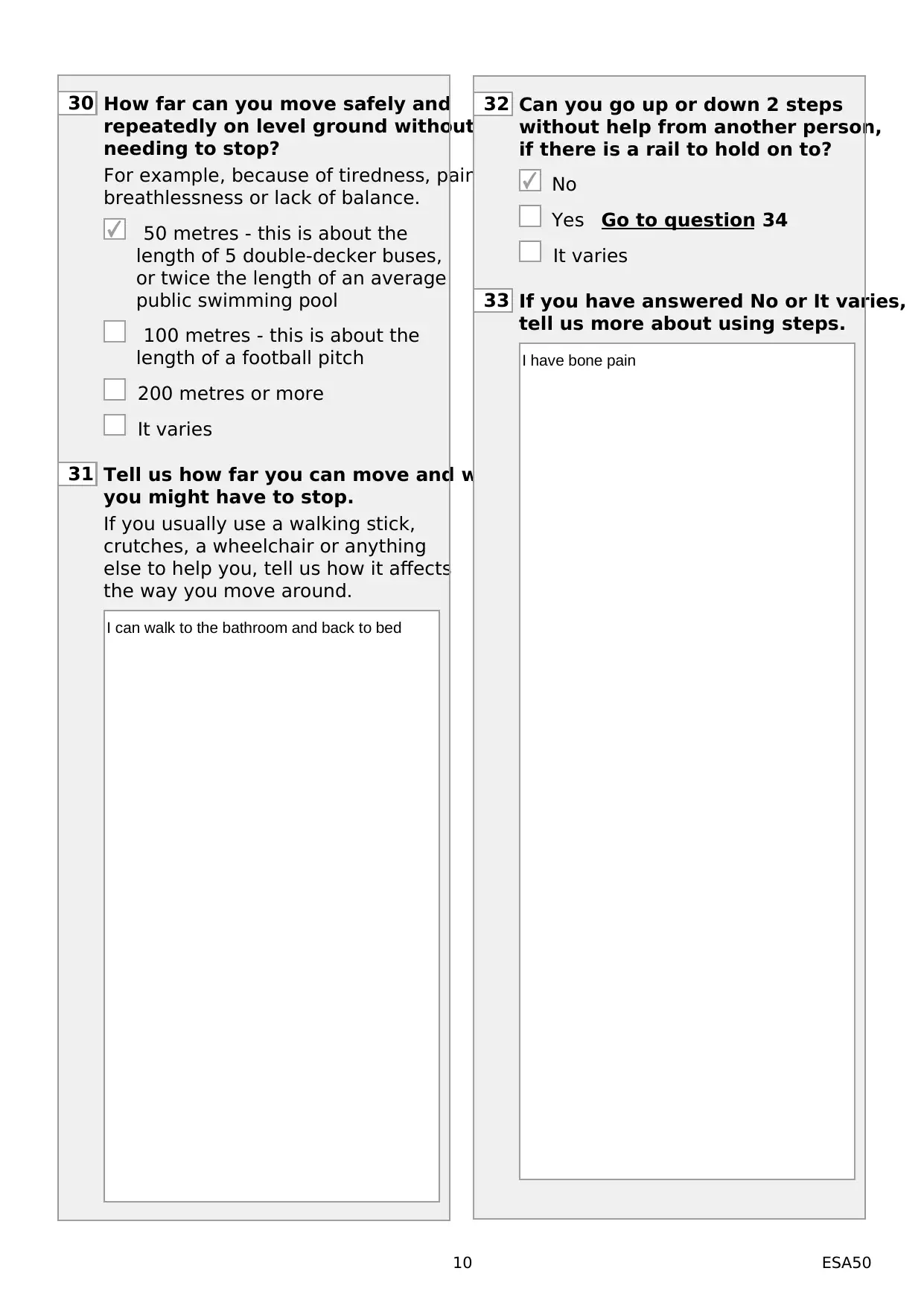
30 How far can you move safely and
repeatedly on level ground without
needing to stop?
For example, because of tiredness, pain,
breathlessness or lack of balance.
50 metres - this is about the
length of 5 double-decker buses,
or twice the length of an average
public swimming pool
100 metres - this is about the
length of a football pitch
200 metres or more
It varies
31 Tell us how far you can move and why
you might have to stop.
If you usually use a walking stick,
crutches, a wheelchair or anything
else to help you, tell us how it affects
the way you move around.
32 Can you go up or down 2 steps
without help from another person,
if there is a rail to hold on to?
No
Yes Go to question 34
It varies
33 If you have answered No or It varies,
tell us more about using steps.
10 ESA50
I can walk to the bathroom and back to bed
I have bone pain
repeatedly on level ground without
needing to stop?
For example, because of tiredness, pain,
breathlessness or lack of balance.
50 metres - this is about the
length of 5 double-decker buses,
or twice the length of an average
public swimming pool
100 metres - this is about the
length of a football pitch
200 metres or more
It varies
31 Tell us how far you can move and why
you might have to stop.
If you usually use a walking stick,
crutches, a wheelchair or anything
else to help you, tell us how it affects
the way you move around.
32 Can you go up or down 2 steps
without help from another person,
if there is a rail to hold on to?
No
Yes Go to question 34
It varies
33 If you have answered No or It varies,
tell us more about using steps.
10 ESA50
I can walk to the bathroom and back to bed
I have bone pain
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
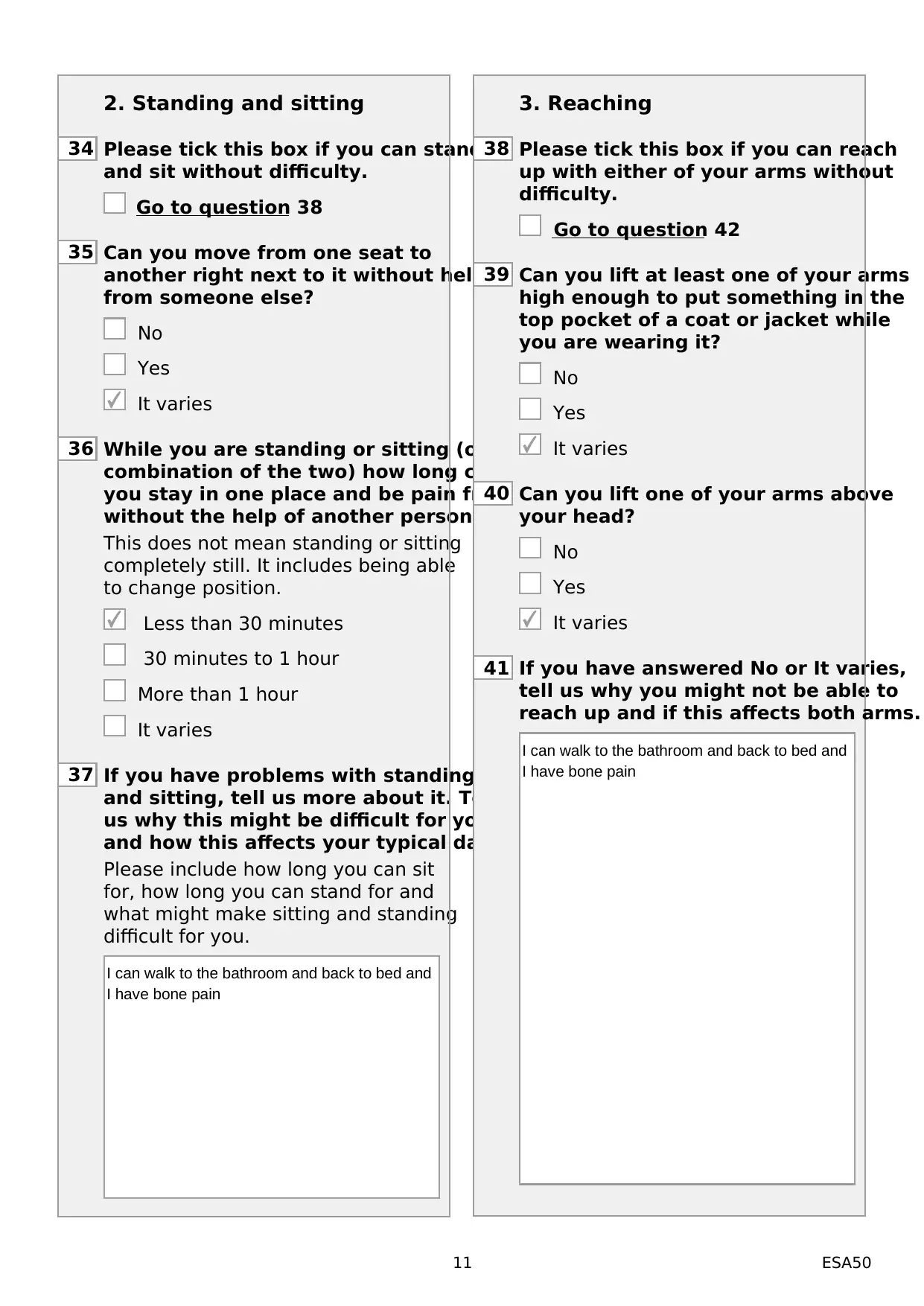
2. Standing and sitting
34 Please tick this box if you can stand
and sit without difficulty.
Go to question 38
35 Can you move from one seat to
another right next to it without help
from someone else?
No
Yes
It varies
36 While you are standing or sitting (or a
combination of the two) how long can
you stay in one place and be pain free
without the help of another person?
This does not mean standing or sitting
completely still. It includes being able
to change position.
Less than 30 minutes
30 minutes to 1 hour
More than 1 hour
It varies
37 If you have problems with standing
and sitting, tell us more about it. Tell
us why this might be difficult for you
and how this affects your typical day.
Please include how long you can sit
for, how long you can stand for and
what might make sitting and standing
difficult for you.
3. Reaching
38 Please tick this box if you can reach
up with either of your arms without
difficulty.
Go to question 42
39 Can you lift at least one of your arms
high enough to put something in the
top pocket of a coat or jacket while
you are wearing it?
No
Yes
It varies
40 Can you lift one of your arms above
your head?
No
Yes
It varies
41 If you have answered No or It varies,
tell us why you might not be able to
reach up and if this affects both arms.
11 ESA50
I can walk to the bathroom and back to bed and
I have bone pain
I can walk to the bathroom and back to bed and
I have bone pain
34 Please tick this box if you can stand
and sit without difficulty.
Go to question 38
35 Can you move from one seat to
another right next to it without help
from someone else?
No
Yes
It varies
36 While you are standing or sitting (or a
combination of the two) how long can
you stay in one place and be pain free
without the help of another person?
This does not mean standing or sitting
completely still. It includes being able
to change position.
Less than 30 minutes
30 minutes to 1 hour
More than 1 hour
It varies
37 If you have problems with standing
and sitting, tell us more about it. Tell
us why this might be difficult for you
and how this affects your typical day.
Please include how long you can sit
for, how long you can stand for and
what might make sitting and standing
difficult for you.
3. Reaching
38 Please tick this box if you can reach
up with either of your arms without
difficulty.
Go to question 42
39 Can you lift at least one of your arms
high enough to put something in the
top pocket of a coat or jacket while
you are wearing it?
No
Yes
It varies
40 Can you lift one of your arms above
your head?
No
Yes
It varies
41 If you have answered No or It varies,
tell us why you might not be able to
reach up and if this affects both arms.
11 ESA50
I can walk to the bathroom and back to bed and
I have bone pain
I can walk to the bathroom and back to bed and
I have bone pain
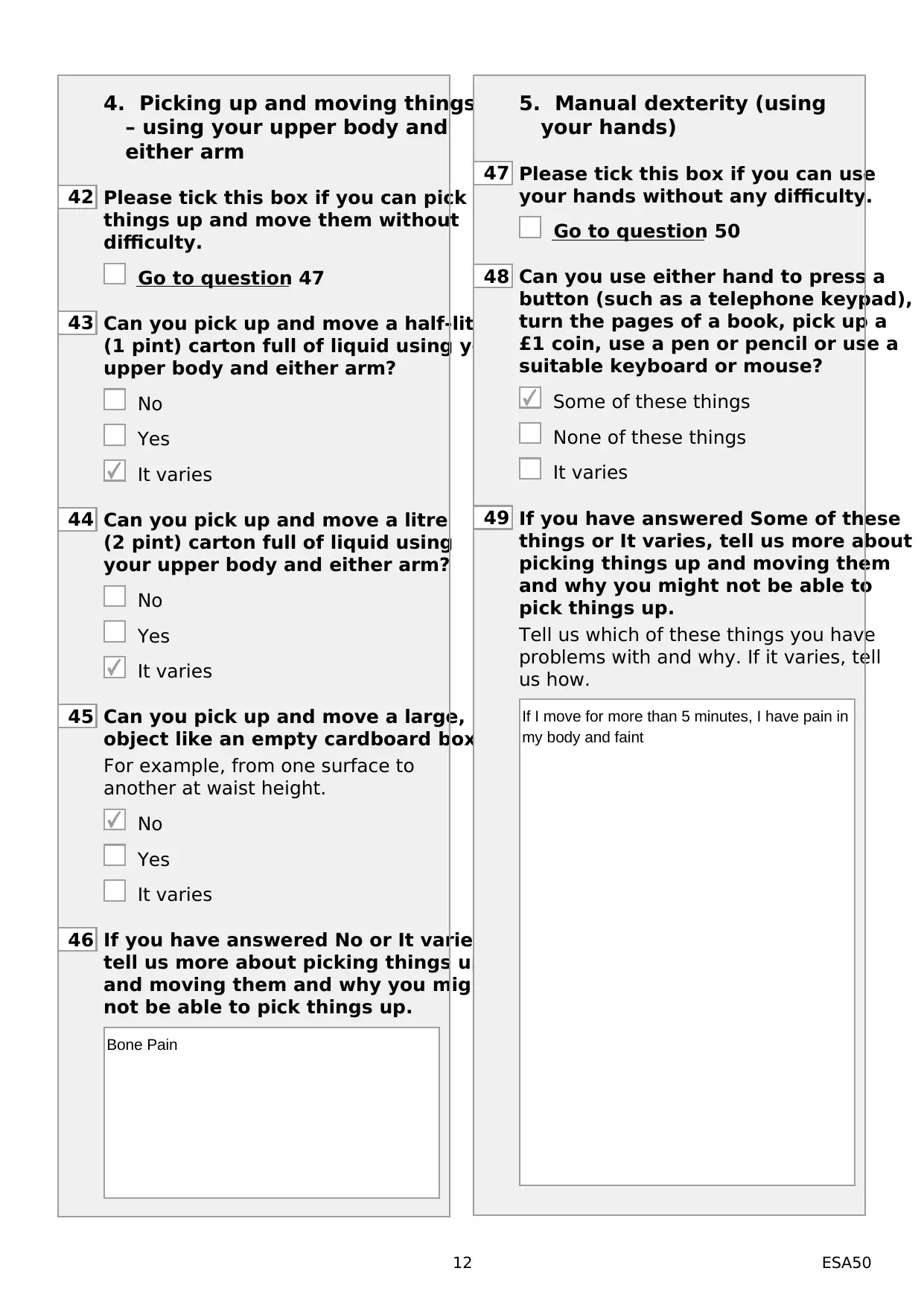
4. Picking up and moving things
– using your upper body and
either arm
42 Please tick this box if you can pick
things up and move them without
difficulty.
Go to question 47
43 Can you pick up and move a half-litre
(1 pint) carton full of liquid using your
upper body and either arm?
No
Yes
It varies
44 Can you pick up and move a litre
(2 pint) carton full of liquid using
your upper body and either arm?
No
Yes
It varies
45 Can you pick up and move a large, light
object like an empty cardboard box?
For example, from one surface to
another at waist height.
No
Yes
It varies
46 If you have answered No or It varies,
tell us more about picking things up
and moving them and why you might
not be able to pick things up.
5. Manual dexterity (using
your hands)
47 Please tick this box if you can use
your hands without any difficulty.
Go to question 50
48 Can you use either hand to press a
button (such as a telephone keypad),
turn the pages of a book, pick up a
£1 coin, use a pen or pencil or use a
suitable keyboard or mouse?
Some of these things
None of these things
It varies
49 If you have answered Some of these
things or It varies, tell us more about
picking things up and moving them
and why you might not be able to
pick things up.
Tell us which of these things you have
problems with and why. If it varies, tell
us how.
12 ESA50
Bone Pain
If I move for more than 5 minutes, I have pain in
my body and faint
– using your upper body and
either arm
42 Please tick this box if you can pick
things up and move them without
difficulty.
Go to question 47
43 Can you pick up and move a half-litre
(1 pint) carton full of liquid using your
upper body and either arm?
No
Yes
It varies
44 Can you pick up and move a litre
(2 pint) carton full of liquid using
your upper body and either arm?
No
Yes
It varies
45 Can you pick up and move a large, light
object like an empty cardboard box?
For example, from one surface to
another at waist height.
No
Yes
It varies
46 If you have answered No or It varies,
tell us more about picking things up
and moving them and why you might
not be able to pick things up.
5. Manual dexterity (using
your hands)
47 Please tick this box if you can use
your hands without any difficulty.
Go to question 50
48 Can you use either hand to press a
button (such as a telephone keypad),
turn the pages of a book, pick up a
£1 coin, use a pen or pencil or use a
suitable keyboard or mouse?
Some of these things
None of these things
It varies
49 If you have answered Some of these
things or It varies, tell us more about
picking things up and moving them
and why you might not be able to
pick things up.
Tell us which of these things you have
problems with and why. If it varies, tell
us how.
12 ESA50
Bone Pain
If I move for more than 5 minutes, I have pain in
my body and faint
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 28
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.