University Nursing Practice: Cardiogenic Shock Case Study Analysis
VerifiedAdded on 2020/04/07
|9
|2143
|177
Report
AI Summary
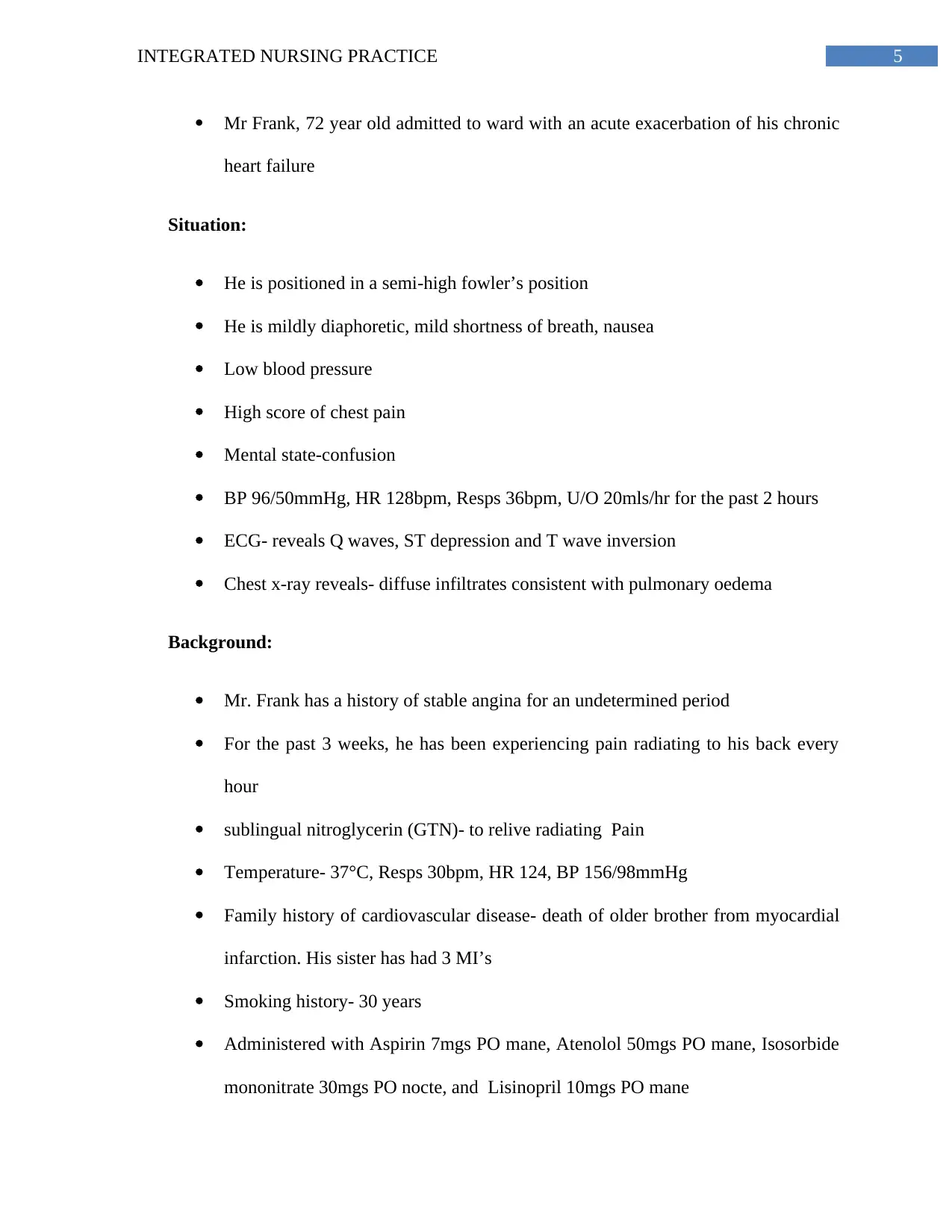
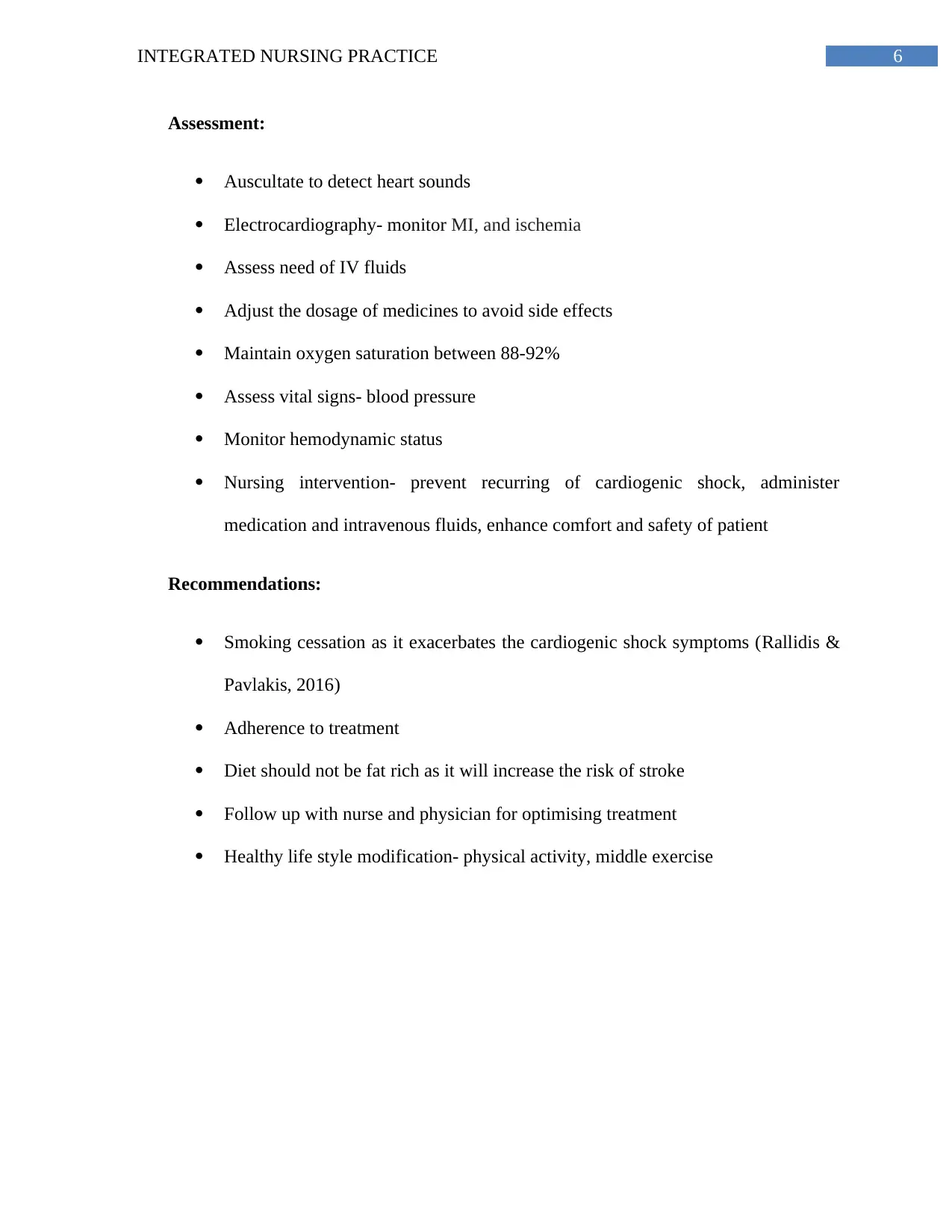
This report presents a comprehensive analysis of a nursing case study involving a 72-year-old patient, Frank James, admitted with an acute exacerbation of chronic heart failure leading to cardiogenic shock. The report meticulously examines the patient's presentation, including signs and symptoms associated with the ABCDE approach (Airway, Breathing, Circulation, Disability, and Exposure). It delves into the pathophysiology of cardiogenic shock, discussing the underlying causes and manifestations, such as changes in vital signs, respiratory distress, and altered mental status. The report also outlines the nursing interventions, including medication management, fluid administration, and patient positioning to alleviate symptoms and improve outcomes. Furthermore, the report incorporates an ISBAR (Identify, Situation, Background, Assessment, Recommendation) handover format to demonstrate effective communication in a clinical setting. The report also highlights the importance of smoking cessation and lifestyle modifications for long-term patient management. The case study includes references to support the analysis.

1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.