Addressing Postnatal Depression: A Case Study of Ms. Brown
VerifiedAdded on 2020/05/04
|20
|5404
|72
AI Summary
Postnatal depression is a significant mental health concern affecting mothers during pregnancy and after childbirth, with implications for both maternal and child well-being. This assignment focuses on understanding postnatal depression through clinical assessment and intervention strategies. It highlights the use of tools like the Edinburgh Postnatal Depression Scale (EPDS) for accurate diagnosis and discusses evidence-based therapeutic interventions to support affected individuals. The aim is to provide a comprehensive overview of current practices in managing postnatal depression, drawing on recent research and clinical guidelines.

Title Page
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

Contents
Assessment Task Number Two:
A Comprehensive Consumer Assessment
Introduction
Psychiatric Nurse Assessing: Delia
Date:
Consumer Name (in full): Rachel Edison
Date of Birth:
Sex: Male Female
Address:
Telephone Home:
Telephone Work:
UR Number _ _ _ _ _ _
Next of Kin Contact Person:
Name:
Relationship to the Consumer:
Address:
Contact Telephone Number Home:
Contact Telephone Number Work:
REFERRAL SOURCE:
OTHER WORKERS / AGENCIES INVOLVED
A Comprehensive Consumer Assessment
Introduction
Psychiatric Nurse Assessing: Delia
Date:
Consumer Name (in full): Rachel Edison
Date of Birth:
Sex: Male Female
Address:
Telephone Home:
Telephone Work:
UR Number _ _ _ _ _ _
Next of Kin Contact Person:
Name:
Relationship to the Consumer:
Address:
Contact Telephone Number Home:
Contact Telephone Number Work:
REFERRAL SOURCE:
OTHER WORKERS / AGENCIES INVOLVED
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Assessment Task Two Example Format (Cont…)
PRESENTING COMPLAINT:
The reviewed case is one of a 28-year-old female who has been suffering from the
effects of post-natal depression in the immediate aftermath of having a three-month-
old baby. For the sake of confidentiality of personal information and the
maintenance of anonymity, the patient in question shall henceforth be referred to
with the pseudonym ‘Mary’. Mary has been admitted to the Inpatient Perinatal
Mental Health Unit following the signs and symptoms of severe depression and
emotional upheaval. The depressive state of the patient, in particular, has reached a
severe state, wherein she feels extremely depressed and reported that she wanted to
‘escape’ from all the trials and challenges of her life. Despite several reassurances,
the patient still believes that everything that is happening is having a severe
negative impact on her life, which is a sign of the advent of clinical depression
(Albert, Vahid-Ansari & Luckhart, 2014).
PAST PSYCHIATRIC TREATMENT:
Mary has had several depression issues in the past as well, with periods of normal
behaviour followed by phases of depression where almost nothing seemed to cheer
her up. While the conditions were never severe enough to warrant admission to the
hospitals or healthcare organisations of the nearby vicinity of her home, certain
medications were definitely needed for improving her mental condition during such
phases. However, the symptoms often got worse over a long period of time, with the
periods of depression often increasing in length and magnitude (Bauer et al. 2015).
She was finally taken for checkups at the age of twenty, which revealed that the
signs and symptoms which she has displayed are those of Persistent Depressive
Disorder (dysthymia). The recommended anti-depressants and therapy sessions did
manage to help her get back on her feet in a satisfactory manner, though the
specialist warned of the possible relapse in conditions such as those of hardship and
discomfort. Indeed, her previous history of depression has resulted in the onset of
her postnatal depression to an appreciable degree (Borra, Iacovou & Sevilla, 2015).
CURRENT PSYCHIATRIC TREATMENT:
PRESENTING COMPLAINT:
The reviewed case is one of a 28-year-old female who has been suffering from the
effects of post-natal depression in the immediate aftermath of having a three-month-
old baby. For the sake of confidentiality of personal information and the
maintenance of anonymity, the patient in question shall henceforth be referred to
with the pseudonym ‘Mary’. Mary has been admitted to the Inpatient Perinatal
Mental Health Unit following the signs and symptoms of severe depression and
emotional upheaval. The depressive state of the patient, in particular, has reached a
severe state, wherein she feels extremely depressed and reported that she wanted to
‘escape’ from all the trials and challenges of her life. Despite several reassurances,
the patient still believes that everything that is happening is having a severe
negative impact on her life, which is a sign of the advent of clinical depression
(Albert, Vahid-Ansari & Luckhart, 2014).
PAST PSYCHIATRIC TREATMENT:
Mary has had several depression issues in the past as well, with periods of normal
behaviour followed by phases of depression where almost nothing seemed to cheer
her up. While the conditions were never severe enough to warrant admission to the
hospitals or healthcare organisations of the nearby vicinity of her home, certain
medications were definitely needed for improving her mental condition during such
phases. However, the symptoms often got worse over a long period of time, with the
periods of depression often increasing in length and magnitude (Bauer et al. 2015).
She was finally taken for checkups at the age of twenty, which revealed that the
signs and symptoms which she has displayed are those of Persistent Depressive
Disorder (dysthymia). The recommended anti-depressants and therapy sessions did
manage to help her get back on her feet in a satisfactory manner, though the
specialist warned of the possible relapse in conditions such as those of hardship and
discomfort. Indeed, her previous history of depression has resulted in the onset of
her postnatal depression to an appreciable degree (Borra, Iacovou & Sevilla, 2015).
CURRENT PSYCHIATRIC TREATMENT:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Mary has been admitted to the Inpatient Perinatal Mental Health Unit, with the
admission procedure deeming her to be a non-compulsory client diagnosed with
Postnatal Depression. The used medications have included:
A daily dose of Sertraline (Previous Dose – 100 mg, Current Dose – 150 mg)
Diazepam thrice per day (Maximum dose not going past 15 mg, with the maximum number
of doses not exceeding three per day; the range of Diazepam has to be at least 2.5 mg – 5
mg) (Clarici et al. 2015)
ACCOMMODATION:
The present medical accommodation is the rented ward of the Inpatient Perinatal
Mental Health Unit, with her husband being one of the regular visitors. Their house
is a five-minute walk away from the healthcare facility, which ensures the ease of
comfort in ensuring proper communication.
FINANCIAL ARRANGEMENTS:
The patient in question has been supported financially by her husband, who is an
engineer working in a reputed firm. The main financial arrangements as decreed and
decided by her husband have ensured the continued implementation of the treatment
without any kind of inhibitions.
HISTORY AS REPORTED BY OTHERS:
Her husband (to be referred with the pseudonym ‘Mark’) has referred to her as a
moody person, with her mood sometimes swinging from one extreme to the other
within a considerably short period of time. She has also been described as ‘fairly
shy’, who generally remains quiet during visits to gatherings and places with a
higher number of people. Her husband has also revealed that she may have inherited
the traits of depression from her parents, whom he said are similar in nature to her
(Cox, Holden & Henshaw, 2014). Mark has also stated that the traits of depression
admission procedure deeming her to be a non-compulsory client diagnosed with
Postnatal Depression. The used medications have included:
A daily dose of Sertraline (Previous Dose – 100 mg, Current Dose – 150 mg)
Diazepam thrice per day (Maximum dose not going past 15 mg, with the maximum number
of doses not exceeding three per day; the range of Diazepam has to be at least 2.5 mg – 5
mg) (Clarici et al. 2015)
ACCOMMODATION:
The present medical accommodation is the rented ward of the Inpatient Perinatal
Mental Health Unit, with her husband being one of the regular visitors. Their house
is a five-minute walk away from the healthcare facility, which ensures the ease of
comfort in ensuring proper communication.
FINANCIAL ARRANGEMENTS:
The patient in question has been supported financially by her husband, who is an
engineer working in a reputed firm. The main financial arrangements as decreed and
decided by her husband have ensured the continued implementation of the treatment
without any kind of inhibitions.
HISTORY AS REPORTED BY OTHERS:
Her husband (to be referred with the pseudonym ‘Mark’) has referred to her as a
moody person, with her mood sometimes swinging from one extreme to the other
within a considerably short period of time. She has also been described as ‘fairly
shy’, who generally remains quiet during visits to gatherings and places with a
higher number of people. Her husband has also revealed that she may have inherited
the traits of depression from her parents, whom he said are similar in nature to her
(Cox, Holden & Henshaw, 2014). Mark has also stated that the traits of depression
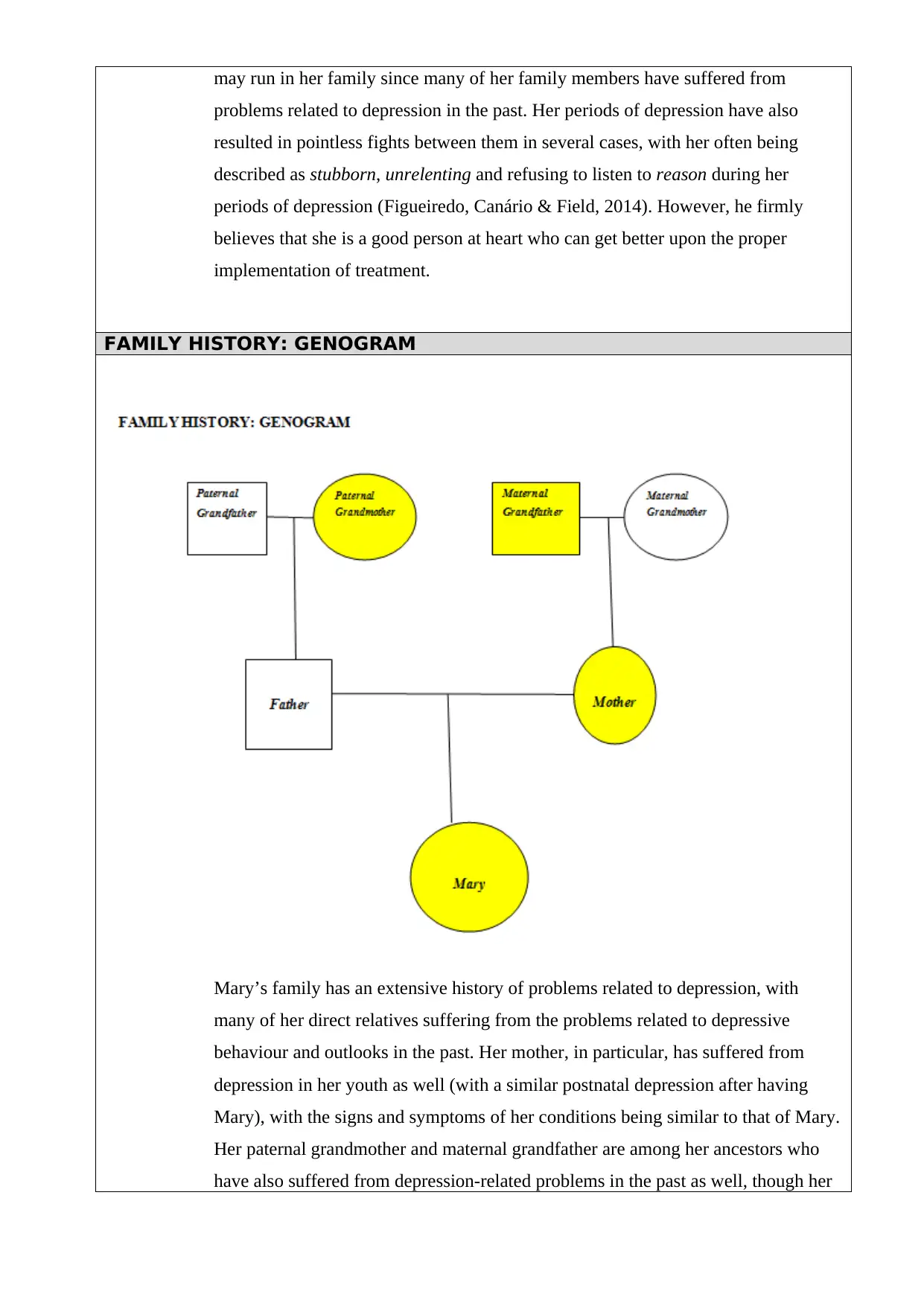
may run in her family since many of her family members have suffered from
problems related to depression in the past. Her periods of depression have also
resulted in pointless fights between them in several cases, with her often being
described as stubborn, unrelenting and refusing to listen to reason during her
periods of depression (Figueiredo, Canário & Field, 2014). However, he firmly
believes that she is a good person at heart who can get better upon the proper
implementation of treatment.
FAMILY HISTORY: GENOGRAM
Mary’s family has an extensive history of problems related to depression, with
many of her direct relatives suffering from the problems related to depressive
behaviour and outlooks in the past. Her mother, in particular, has suffered from
depression in her youth as well (with a similar postnatal depression after having
Mary), with the signs and symptoms of her conditions being similar to that of Mary.
Her paternal grandmother and maternal grandfather are among her ancestors who
have also suffered from depression-related problems in the past as well, though her
problems related to depression in the past. Her periods of depression have also
resulted in pointless fights between them in several cases, with her often being
described as stubborn, unrelenting and refusing to listen to reason during her
periods of depression (Figueiredo, Canário & Field, 2014). However, he firmly
believes that she is a good person at heart who can get better upon the proper
implementation of treatment.
FAMILY HISTORY: GENOGRAM
Mary’s family has an extensive history of problems related to depression, with
many of her direct relatives suffering from the problems related to depressive
behaviour and outlooks in the past. Her mother, in particular, has suffered from
depression in her youth as well (with a similar postnatal depression after having
Mary), with the signs and symptoms of her conditions being similar to that of Mary.
Her paternal grandmother and maternal grandfather are among her ancestors who
have also suffered from depression-related problems in the past as well, though her
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
paternal grandparents had passed away before she was fully grown up. Being an
only child, she was prone to being alone for certain periods of time on account of
both of her parents being working professionals in her youth. The members of her
family who suffered from depression problems have been coloured in yellow in the
given genogram of family history.
RECOVERY ENGAGEMENT / RESOURCES / RELATIONSHIPS:
Mary has been gifted with a high level of intelligence and thinking ability, with her
intellect being of a considerably high level. She always wishes to engage in
different kinds of productive activities, with her main motivation being occupying
her mind and body with useful and creative work. Her desire to live a normal life
and spend her days without too much stress highlights the main desires of a high
percentage of the people, especially those belonging to the middle classes (Franck et
al. 2016). She is generally a good person to talk to, as is evident by her relatively
good relationship with her husband and the fact that her husband understands her
condition (and its potential effects on her behaviour). She is aware of her problems
related to depression, with her seeking to get rid of them as soon as possible. Her
general good nature has ensured that her friends understand her bouts of depression
and outburst as well. Her protective factors include her relatives, family members
and close friends.
Assessment Task Two Example Format (Cont…)
PERSONAL HISTORY:
EARLY CHILDHOOD DEVELOPMENT
Her mother has described her pregnancy with Mary as being unremarkable and not
different from a normal full term of pregnancy. She was born after a normal term of
nine months without the need of cesarean section, having a normal birth. However,
her mother did feel post natal depression for a couple of months after having her as
well. Being an only child, she was fairly close to both of her parents, though their
only child, she was prone to being alone for certain periods of time on account of
both of her parents being working professionals in her youth. The members of her
family who suffered from depression problems have been coloured in yellow in the
given genogram of family history.
RECOVERY ENGAGEMENT / RESOURCES / RELATIONSHIPS:
Mary has been gifted with a high level of intelligence and thinking ability, with her
intellect being of a considerably high level. She always wishes to engage in
different kinds of productive activities, with her main motivation being occupying
her mind and body with useful and creative work. Her desire to live a normal life
and spend her days without too much stress highlights the main desires of a high
percentage of the people, especially those belonging to the middle classes (Franck et
al. 2016). She is generally a good person to talk to, as is evident by her relatively
good relationship with her husband and the fact that her husband understands her
condition (and its potential effects on her behaviour). She is aware of her problems
related to depression, with her seeking to get rid of them as soon as possible. Her
general good nature has ensured that her friends understand her bouts of depression
and outburst as well. Her protective factors include her relatives, family members
and close friends.
Assessment Task Two Example Format (Cont…)
PERSONAL HISTORY:
EARLY CHILDHOOD DEVELOPMENT
Her mother has described her pregnancy with Mary as being unremarkable and not
different from a normal full term of pregnancy. She was born after a normal term of
nine months without the need of cesarean section, having a normal birth. However,
her mother did feel post natal depression for a couple of months after having her as
well. Being an only child, she was fairly close to both of her parents, though their
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
work in her pre-teen and teenage years often left her alone in their house for a
considerable period of time. The loneliness that she experienced during that time is
a crucial factor to be noted, as it can be an indication of the origin of her depression
problems (Gutierrez-Galve et al. 2015).
SCHOOL PROGRESSION:
Mary has always been an above-average student on account of her intelligence,
though nerves often dampened her results in certain examinations during high
school. Her teachers often described her as having results that did not reflect her
true potential, on account of panicking during the times of the examinations (due to
excessive nervousness) (Hiscock et al. 2014). Despite these inhibitions, she passed
out of high school with above average grades, with her family being fairly proud of
her results. She also enrolled in management diploma courses, in order to learn
about the aspects of marketing, with her passing out of the same with fairly good
results as well.
OCCUPATIONAL HISTORY:
Mary is currently a housewife, with her main attention being the full-time care of
her three-month-old baby. Despite this, Mary also held several part-time jobs in
order to manage enough money to get by her daily expenses, in order to depend on
her parents on an excessive manner (during the days before she was married). She
was also a participant in awareness campaigns pertaining to the importance of
cleanliness in ensuring the effective management of the diseases when she was 22.
Her first job was as a staff member of the Wal-Mart branch of Melbourne, with her
payment being on a monthly basis. She started when she was 18 and held the job for
a period of almost two years. She has stated that she was fairly happy during her
time there, with her increasingly busy schedule as a result of being the student of
the management diploma course being her main reason for departure.
She also worked as a receptionist of a Child Care Center at the age of 25, with her
marketing knowledge and speaking skills helping her tremendously in her job. She
held the job for almost a year before quitting on account of her impending marriage
considerable period of time. The loneliness that she experienced during that time is
a crucial factor to be noted, as it can be an indication of the origin of her depression
problems (Gutierrez-Galve et al. 2015).
SCHOOL PROGRESSION:
Mary has always been an above-average student on account of her intelligence,
though nerves often dampened her results in certain examinations during high
school. Her teachers often described her as having results that did not reflect her
true potential, on account of panicking during the times of the examinations (due to
excessive nervousness) (Hiscock et al. 2014). Despite these inhibitions, she passed
out of high school with above average grades, with her family being fairly proud of
her results. She also enrolled in management diploma courses, in order to learn
about the aspects of marketing, with her passing out of the same with fairly good
results as well.
OCCUPATIONAL HISTORY:
Mary is currently a housewife, with her main attention being the full-time care of
her three-month-old baby. Despite this, Mary also held several part-time jobs in
order to manage enough money to get by her daily expenses, in order to depend on
her parents on an excessive manner (during the days before she was married). She
was also a participant in awareness campaigns pertaining to the importance of
cleanliness in ensuring the effective management of the diseases when she was 22.
Her first job was as a staff member of the Wal-Mart branch of Melbourne, with her
payment being on a monthly basis. She started when she was 18 and held the job for
a period of almost two years. She has stated that she was fairly happy during her
time there, with her increasingly busy schedule as a result of being the student of
the management diploma course being her main reason for departure.
She also worked as a receptionist of a Child Care Center at the age of 25, with her
marketing knowledge and speaking skills helping her tremendously in her job. She
held the job for almost a year before quitting on account of her impending marriage
(to concentrate on being a housewife).
RELATIONSHIP / MARTIAL HISTORY:
Mary has been married to Mark for almost two years, with her relationship with him
being fairly decent. While they have managed their house quite well, her depression
problems often cause them to have fights (which Mark often describes to be
pointless) quite frequently. Her husband has been fairly understanding of her
condition, with him trying to cater to her needs during her bouts of depression.
Despite the fairly high frequency of disputes and fights, their marriage has been one
of the sources of strength for Mary during her worst times.
DRUG AND ALCOHOL USE:
Mary does not have any kind of history of drug use, with her being completely
drug-free with no history of illicit drug use or substance abuse. She has managed to
ensure that she does not get addicted to any of the strong medications which have
been prescribed to her over the years. She is also an occasional drinker, though her
alcohol intake increases during her times of depression (Kozinszky & Dudas, 2015).
She is also a non-smoker, with her excess alcohol consumption during certain times
being the only major problem in this regard.
FORENSIC HISTORY / LEGAL MATTERS:
Despite her mental troubles, Mary has not been involved with any kind of
altercations which have resulted in legal procedures and enquiries. However, one of
the fights that she had with her husband resulted in her yelling in a manner which
prompted their neighbours to threaten them with police warnings. Other than the
aforementioned, the patient in question has been reportedly free from legal
inquisitions and altercations.
MEDICAL HISTORY:
RELATIONSHIP / MARTIAL HISTORY:
Mary has been married to Mark for almost two years, with her relationship with him
being fairly decent. While they have managed their house quite well, her depression
problems often cause them to have fights (which Mark often describes to be
pointless) quite frequently. Her husband has been fairly understanding of her
condition, with him trying to cater to her needs during her bouts of depression.
Despite the fairly high frequency of disputes and fights, their marriage has been one
of the sources of strength for Mary during her worst times.
DRUG AND ALCOHOL USE:
Mary does not have any kind of history of drug use, with her being completely
drug-free with no history of illicit drug use or substance abuse. She has managed to
ensure that she does not get addicted to any of the strong medications which have
been prescribed to her over the years. She is also an occasional drinker, though her
alcohol intake increases during her times of depression (Kozinszky & Dudas, 2015).
She is also a non-smoker, with her excess alcohol consumption during certain times
being the only major problem in this regard.
FORENSIC HISTORY / LEGAL MATTERS:
Despite her mental troubles, Mary has not been involved with any kind of
altercations which have resulted in legal procedures and enquiries. However, one of
the fights that she had with her husband resulted in her yelling in a manner which
prompted their neighbours to threaten them with police warnings. Other than the
aforementioned, the patient in question has been reportedly free from legal
inquisitions and altercations.
MEDICAL HISTORY:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
A lack of a proper amount of diet during times of depression led to malnutrition and
the patient in question being underweight during certain times. Her lack of weight
often led to her being recommended a proper diet pattern, following which she has
been restored to almost-normal health (Matthey, Fisher & Rowe, 2013). She also
gained a bit of weight in the immediate aftermath of parturition, with her being a bit
overweight for a couple of months after the birth of her baby.
PERSONALITY:
Mary is generally a quiet and shy woman, who nonetheless has good qualities and a
gentle personality which enables her to interact with her peers in a desirable and
satisfactory manner. Her tendency of thinking stuff through often leads to her over-
thinking certain matters, which causes her to be depressed and frustrated in several
situations (Massoudi, Hwang & Wickberg, 2013).
Assessment Task Two Example Format (Cont…)
CULTURAL BACKGROUND:
Mary was born and brought up in Melbourne, Victoria (Australia) and has spent
virtually her entire life there. She has relatives in other parts of Australia, with her
visiting them in her childhood on several occasions.
SPIRITUAL CONSIDERATIONS:
Mary is recognized to closely associate with the spiritual beliefs and concepts. Her
views in relation to the certain rituals, ceremonies determine her being spiritual.
Spirituality is one of the aspects that are often neglected by health care system
the patient in question being underweight during certain times. Her lack of weight
often led to her being recommended a proper diet pattern, following which she has
been restored to almost-normal health (Matthey, Fisher & Rowe, 2013). She also
gained a bit of weight in the immediate aftermath of parturition, with her being a bit
overweight for a couple of months after the birth of her baby.
PERSONALITY:
Mary is generally a quiet and shy woman, who nonetheless has good qualities and a
gentle personality which enables her to interact with her peers in a desirable and
satisfactory manner. Her tendency of thinking stuff through often leads to her over-
thinking certain matters, which causes her to be depressed and frustrated in several
situations (Massoudi, Hwang & Wickberg, 2013).
Assessment Task Two Example Format (Cont…)
CULTURAL BACKGROUND:
Mary was born and brought up in Melbourne, Victoria (Australia) and has spent
virtually her entire life there. She has relatives in other parts of Australia, with her
visiting them in her childhood on several occasions.
SPIRITUAL CONSIDERATIONS:
Mary is recognized to closely associate with the spiritual beliefs and concepts. Her
views in relation to the certain rituals, ceremonies determine her being spiritual.
Spirituality is one of the aspects that are often neglected by health care system
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
(Milgrom, Martin & Negri, 2015). Therefore, in case of Mary it is essential that she
be treated for her diagnosis by undertaking the spiritual considerations. Mary
considers crystal healing, traditional medicines and folk medicines to be the real
concepts of treatment. Specific customs, traditional therapies are among the spiritual
aspects her beliefs is largely.
GENERAL PRESENTATION:
Mary is a 28-year-old Australian woman. She is average weighted and in appearance
is observed to care have a average self care. She is a first time mother of 3-Month-old
baby because of whom she seems to have undergone postnatal depression
(Murgatroyd, Quinn, Sharp, Pickles & Hill, 2015). With a height of 5 feet 10 inches,
she is observed to be well dressed and tries to maintain a good eye contact. Her
behavior seems to be quiet inclusive and she does not involve herself into any kind
activity at all. Therefore, it is difficult to engage with her.
ORIENTATION:
Mary was alert and well acknowledged the place and position in which she was in
THOUGHT
Content:
Experiences guilt, rejected and irritable all the time. She even determines that she has
thoughts of harming her baby and herself as well. In addition to this she feels that
there is nobody to support her and her husband Mark is not concerned about her at all
instead he is more concerned about the baby. Feeling lonely and unsupported is one
of the major characteristic symptoms of Postnatal Depression. In addition to this, her
thoughts relating to harming herself and the baby as well clearly identifies her state of
be treated for her diagnosis by undertaking the spiritual considerations. Mary
considers crystal healing, traditional medicines and folk medicines to be the real
concepts of treatment. Specific customs, traditional therapies are among the spiritual
aspects her beliefs is largely.
GENERAL PRESENTATION:
Mary is a 28-year-old Australian woman. She is average weighted and in appearance
is observed to care have a average self care. She is a first time mother of 3-Month-old
baby because of whom she seems to have undergone postnatal depression
(Murgatroyd, Quinn, Sharp, Pickles & Hill, 2015). With a height of 5 feet 10 inches,
she is observed to be well dressed and tries to maintain a good eye contact. Her
behavior seems to be quiet inclusive and she does not involve herself into any kind
activity at all. Therefore, it is difficult to engage with her.
ORIENTATION:
Mary was alert and well acknowledged the place and position in which she was in
THOUGHT
Content:
Experiences guilt, rejected and irritable all the time. She even determines that she has
thoughts of harming her baby and herself as well. In addition to this she feels that
there is nobody to support her and her husband Mark is not concerned about her at all
instead he is more concerned about the baby. Feeling lonely and unsupported is one
of the major characteristic symptoms of Postnatal Depression. In addition to this, her
thoughts relating to harming herself and the baby as well clearly identifies her state of
depression after pregnancy (Murray, Fearon, & Cooper, 2015)
Stream:
The thoughts related to unsupportive husband and harming herself is observed to be
in her mind every time. Therefore, because of this she seems to have detached herself
from her husband largely. Therefore, this continuous unblocked thought describes her
state of being in postnatal depression (O’Connor, Rossom, Henninger, Groom &
Burda, 2016). In post natal depression the emotional detachment of the women from
their husband and loved ones and the continuous blaming oneself and tending to harm
one are one of the characteristics features of the concerned mental issue in question.
MOOD & AFFECT:
Mary’s mood as observed is always low and irritable. She feels least bothered and
interested about her newborn baby. Low mood and persistent guilt are not uncommon
among women suffering from postnatal depression. Under this mental issue, the
women undergo a phase where they lose the motivation of engaging into any kind
activities and is often feeling tearful (O’Higgins, Roberts, Glover & Taylor, 2013). In
Mary’s case her low mood has not only made it difficult for her to cope up with
anything but has also hampered her concentration power and decision making
abilities.
PERCEPTUAL ABNORMALITIES:
Experiencing sleep deprivation and that self blaming were among the common
abnormalities in case of Mary. Denial of her being a mother of a baby and the
emotional detachment from her husband presented the key features of Postnatal
depression. Persistence of low mood, frightening thoughts of harming the baby and
Stream:
The thoughts related to unsupportive husband and harming herself is observed to be
in her mind every time. Therefore, because of this she seems to have detached herself
from her husband largely. Therefore, this continuous unblocked thought describes her
state of being in postnatal depression (O’Connor, Rossom, Henninger, Groom &
Burda, 2016). In post natal depression the emotional detachment of the women from
their husband and loved ones and the continuous blaming oneself and tending to harm
one are one of the characteristics features of the concerned mental issue in question.
MOOD & AFFECT:
Mary’s mood as observed is always low and irritable. She feels least bothered and
interested about her newborn baby. Low mood and persistent guilt are not uncommon
among women suffering from postnatal depression. Under this mental issue, the
women undergo a phase where they lose the motivation of engaging into any kind
activities and is often feeling tearful (O’Higgins, Roberts, Glover & Taylor, 2013). In
Mary’s case her low mood has not only made it difficult for her to cope up with
anything but has also hampered her concentration power and decision making
abilities.
PERCEPTUAL ABNORMALITIES:
Experiencing sleep deprivation and that self blaming were among the common
abnormalities in case of Mary. Denial of her being a mother of a baby and the
emotional detachment from her husband presented the key features of Postnatal
depression. Persistence of low mood, frightening thoughts of harming the baby and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 20
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.