Healthcare Funding Models: A Comparative Analysis of UTS Hospital Data
VerifiedAdded on 2019/10/30
|8
|1570
|197
Report
AI Summary
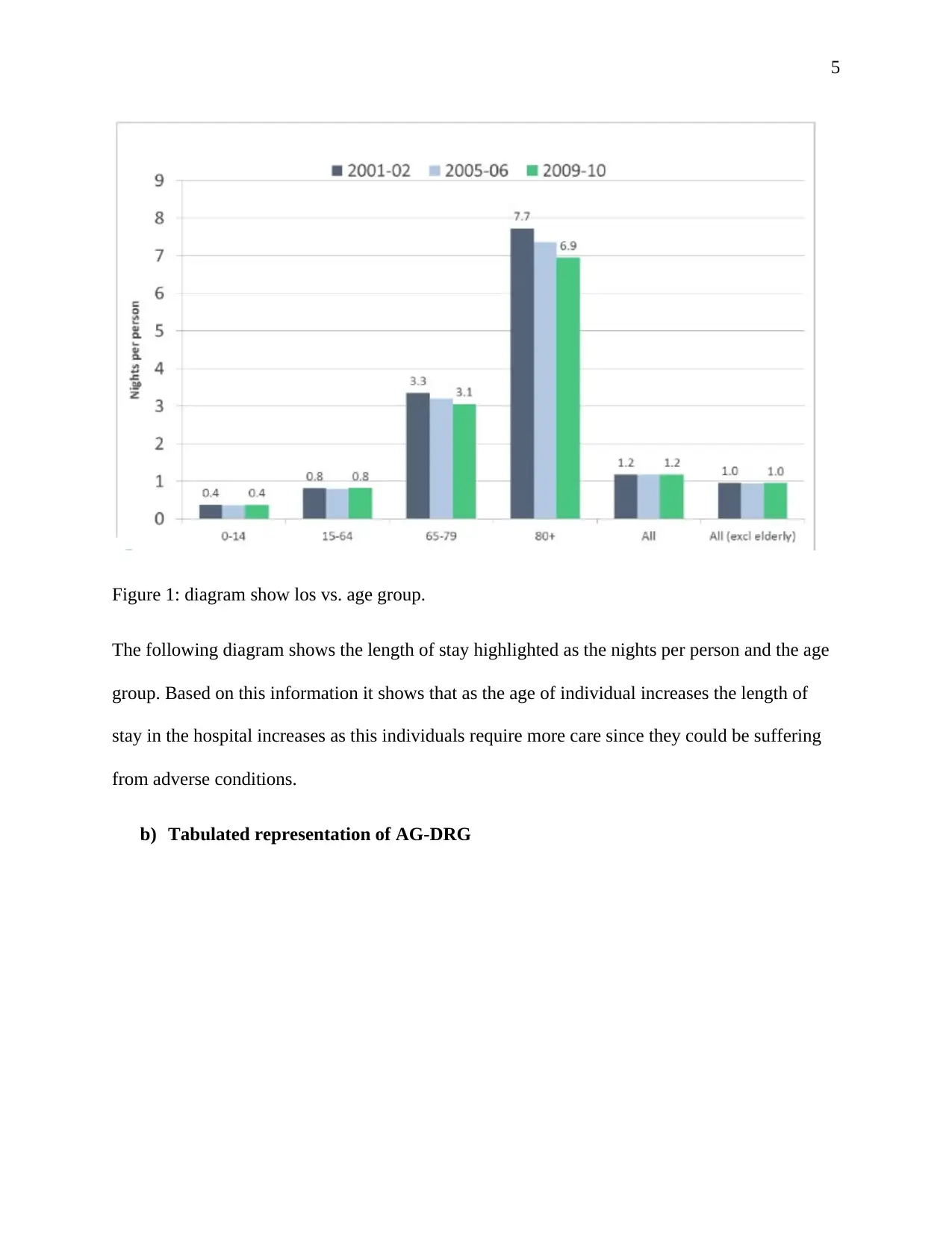
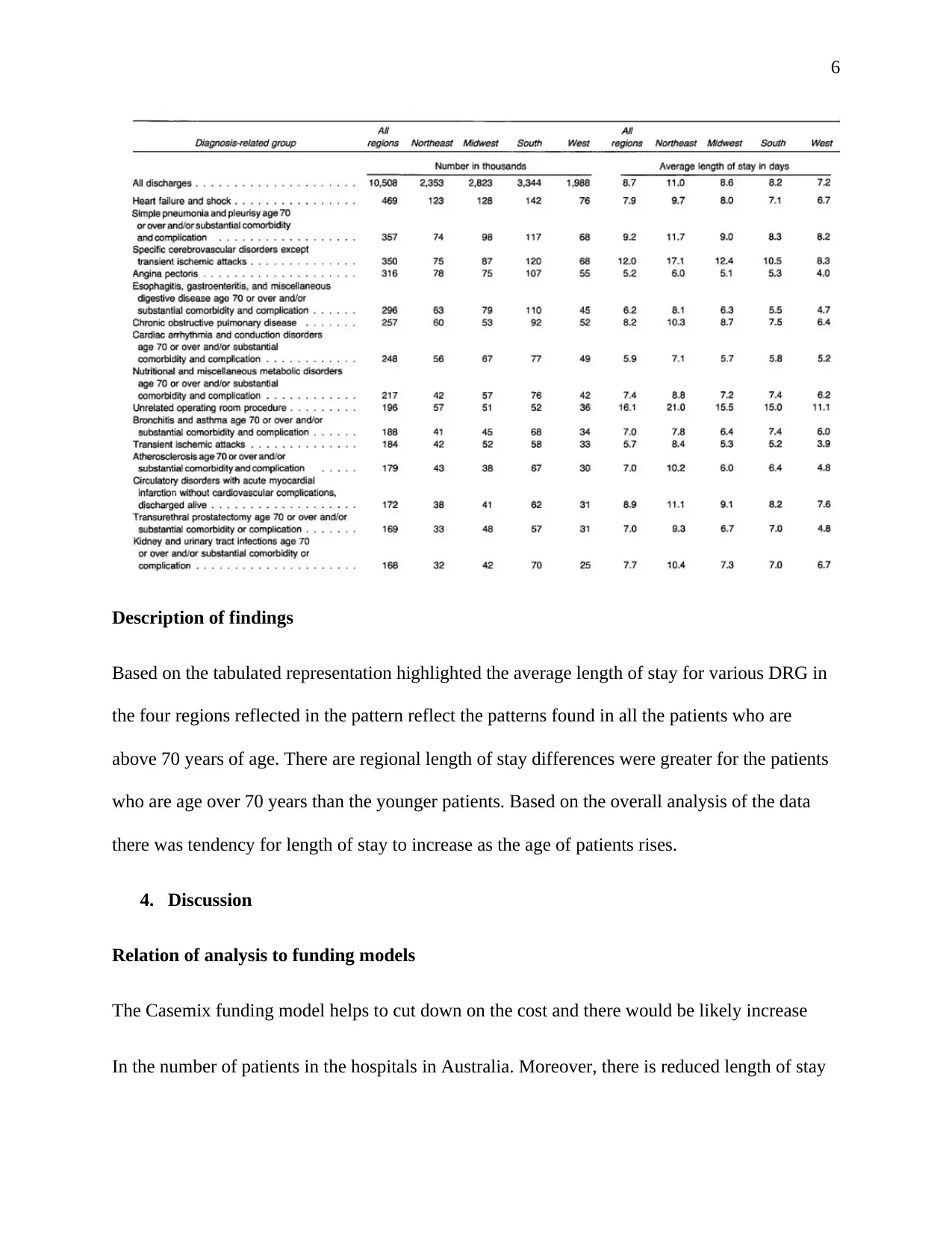
This report examines healthcare funding models, specifically comparing casemix and per-diem approaches using data from UTS Hospital. The analysis begins by defining these two funding models, with casemix funding being based on the activities and types of patients treated, and per-diem funding involving a fixed daily allowance. The report then details the pros and cons of each model, highlighting that casemix funding is useful for reimbursement and benchmarking, but may not suit older, more complex patient populations. Per-diem funding is easy to manage but can be less flexible. The analysis also covers how casemix funding is achieved in Australian hospitals using diagnosis-related groups (DRGs). The report analyzes UTS hospital data to visualize the relationship between patient age and length of stay, finding that older patients tend to have longer stays. The report concludes that UTS hospital should consider per-diem funding due to the nature of its patient population. The analysis is supported by cited references. This report contributes to the understanding of healthcare economics and resource management within hospital settings.

1 out of 8



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.