NUR241 Case Study: Cervical Cancer Screening and Guidelines
VerifiedAdded on 2022/09/15
|5
|863
|21
Case Study
AI Summary
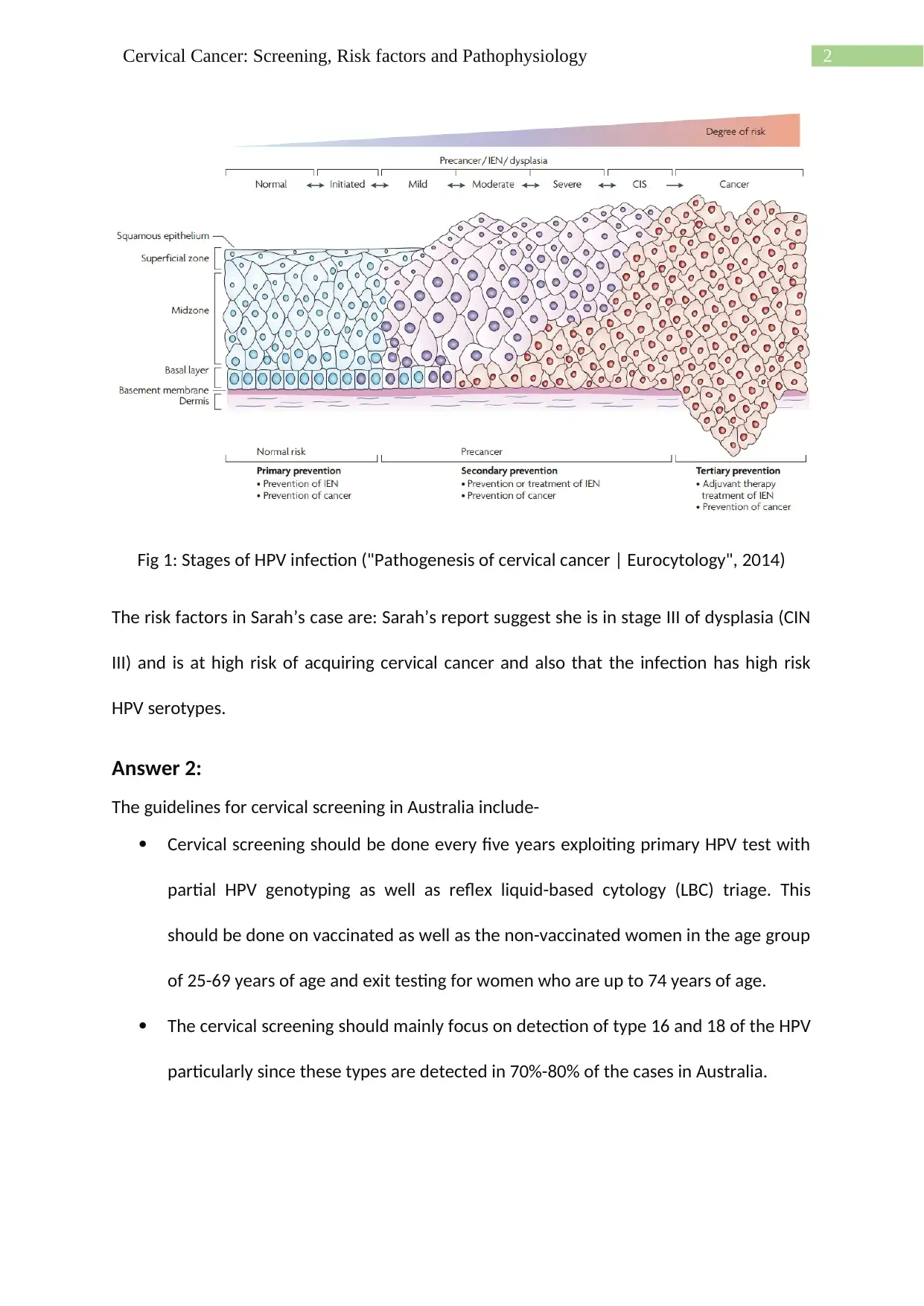
This case study examines the pathophysiology of cervical cancer, focusing on the role of HPV infection and the progression from CIN stages to invasive cancer. The risk factors in Sarah's case, including high-risk HPV serotypes and a CIN III diagnosis, are identified. The assignment also outlines the latest cervical screening guidelines in Australia, emphasizing primary HPV testing, genotyping, and the recommended screening intervals for vaccinated and unvaccinated women. The rationale behind these guidelines, supported by scientific literature, is presented, highlighting the effectiveness of the screening process in reducing cervical cancer incidence. The study also mentions the introduction of the National Cancer Screening Registry and the delisting of existing cervical screening test items.

1 out of 5
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.