CHCPRP003 Case Study: Reflecting on Medication Error & Patient Safety
VerifiedAdded on 2023/04/21
|7
|2606
|406
Case Study
AI Summary
This assignment presents a case study involving a 23-year-old woman admitted to the ICU with flu-like symptoms, ultimately resulting in a medication error and patient death. The solution involves a reflection on the case using Gibbs’ Reflective Cycle. The reflection covers the nurse's feelings, evaluation of the situation, analysis of key concepts such as documentation and communication, conclusions about improving practice, and an action plan for future similar situations. Key areas of improvement identified include thorough documentation, effective communication with physicians, and vigilant patient monitoring to prevent adverse outcomes. The reflection emphasizes the importance of learning from mistakes and continuously improving clinical practice to ensure patient safety. Desklib offers similar case studies and assignments for students.
Student Name:
Student Signature:
Trainer Name:
Trainer Signature:
Student Outcome: Satisfactory Not Satisfactory
CHCPRP003 Reflect on and improve
own clinical practice
Case Study
Student Signature:
Trainer Name:
Trainer Signature:
Student Outcome: Satisfactory Not Satisfactory
CHCPRP003 Reflect on and improve
own clinical practice
Case Study
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Assessment Instructions
Achieving competency
This assessment task contains 1 Case Study. In order for you to meet the requirements of this assessment
task you are complete the case study by providing satisfactory answer to the related questions.
The task is to be completed in your own time using available reliable sources such as the course text books
provided to you at orientation, credible internet sources such as the department of health and other text
and online journals available to you through the online library service offered to all students and discussed
at orientation.
It is important that you reference all sources of information that you use to obtain information used in your
answers. Referencing must be included and failure to adhere to this requirement will result in a not
satisfactory outcome for the assessment.
The case study is available in the Student Portal. You will need to download the case study and complete it
then submit it through the Student Portal
Plagiarism will result in an immediate Not yet Competent – all copied material MUST be referenced
accordingly. See you Student Handbook for more information.
Reassessment
If you receive a Not Yet Satisfactory result for this Assessment Task, it will be due to you not satisfying the
requirements of one, multiple or all aspects of the task. Your Assessor will provide you with feedback as to
where you did not meet the requirement. You will have another opportunity to resubmit your assessment
work addressing the areas as identified in your assessor feedback.
Should the student wish to appeal any decision relating to outcome of this assessment task, the student
should follow the Academic-Non Academic Grievance policy and procedure available in the Student
Handbook and Skills Training Australia website.
Assessment Extension Request:
All assessments are due on the assessment due date as identified on the assessment task document and
confirmed by your Trainer/Assessor on the first day of the unit.
If you are unable, due to exceptional circumstances, to submit your assessment tasks on the required due
date, you MUST submit a completed Assessment Extension Form to your Trainer/Assessor.
Extensions may be granted by your trainer under exceptional circumstances and will only be granted for a
maximum of 2 weeks.
Adjustment in assessment
Flexibility in assessment will be considered where the integrity of the assessment and learning outcome is
maintained. For example, a written assessment may be administered as a verbal assessment and recorded
by a STA staff member where a student has sustained an injury preventing them from writing. Any
agreement for an adjustment to assessment must be documented in the space provided in the assessment
task document (or in writing to the program manager in the event of an electronically submitted
assessment task and placed in your student file).
Please type your responses in the spaces provided below each question and submit as per the instructions
in the assessment document.
Please note: The space below is not indicative to the required length of the response; you are to ensure
that you thoroughly answer the question.
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 2
Achieving competency
This assessment task contains 1 Case Study. In order for you to meet the requirements of this assessment
task you are complete the case study by providing satisfactory answer to the related questions.
The task is to be completed in your own time using available reliable sources such as the course text books
provided to you at orientation, credible internet sources such as the department of health and other text
and online journals available to you through the online library service offered to all students and discussed
at orientation.
It is important that you reference all sources of information that you use to obtain information used in your
answers. Referencing must be included and failure to adhere to this requirement will result in a not
satisfactory outcome for the assessment.
The case study is available in the Student Portal. You will need to download the case study and complete it
then submit it through the Student Portal
Plagiarism will result in an immediate Not yet Competent – all copied material MUST be referenced
accordingly. See you Student Handbook for more information.
Reassessment
If you receive a Not Yet Satisfactory result for this Assessment Task, it will be due to you not satisfying the
requirements of one, multiple or all aspects of the task. Your Assessor will provide you with feedback as to
where you did not meet the requirement. You will have another opportunity to resubmit your assessment
work addressing the areas as identified in your assessor feedback.
Should the student wish to appeal any decision relating to outcome of this assessment task, the student
should follow the Academic-Non Academic Grievance policy and procedure available in the Student
Handbook and Skills Training Australia website.
Assessment Extension Request:
All assessments are due on the assessment due date as identified on the assessment task document and
confirmed by your Trainer/Assessor on the first day of the unit.
If you are unable, due to exceptional circumstances, to submit your assessment tasks on the required due
date, you MUST submit a completed Assessment Extension Form to your Trainer/Assessor.
Extensions may be granted by your trainer under exceptional circumstances and will only be granted for a
maximum of 2 weeks.
Adjustment in assessment
Flexibility in assessment will be considered where the integrity of the assessment and learning outcome is
maintained. For example, a written assessment may be administered as a verbal assessment and recorded
by a STA staff member where a student has sustained an injury preventing them from writing. Any
agreement for an adjustment to assessment must be documented in the space provided in the assessment
task document (or in writing to the program manager in the event of an electronically submitted
assessment task and placed in your student file).
Please type your responses in the spaces provided below each question and submit as per the instructions
in the assessment document.
Please note: The space below is not indicative to the required length of the response; you are to ensure
that you thoroughly answer the question.
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 2
Case Study 1:
Medication Administration Error and Failure to Monitor
A 23-year-old woman with no significant medical history presented to ED with flu-like symptoms. She complained of
generalized body ache and had a fever of 38.8. For the past two weeks, she self-administered over- the-counter
medications with no relief. Instead, her condition deteriorated and she developed both shortness of breath and a
cough.
Following an abnormal CT Scan of the chest, an elevated white blood count and abnormal liver function test results,
the emergency department physician admitted the patient to ICU.
The patient was started on oxygen and antibiotic therapy. Blood cultures were drawn and showed Streptococcus
Pneumoniae and antibiotics were appropriately adjusted per recommendation of the infectious disease specialist.
The attending physician first saw the patient in the ICU. At the time of his initial exam, the patient was not in
significant respiratory distress, was responding well to the oxygen and antibiotic therapy, and was subsequently
continued on the same therapy. The attending physician noted that while the patient was not in acute distress, her
blood chemistry was abnormal with a potassium level of 2.9 (normal range is 3.5 to 5.0).
The physician ordered 30mEq of potassium to be added to each bag of the patient’s intravenous fluid, infused at 80
millilitres per hour. The order was to be maintained through the remainder of her course of treatment. Two days
later and despite the potassium added to her intravenous fluids, the patient’s potassium level was noted to be 3.0
and the attending physician ordered 80 mEq of potassium to be administered by mouth.
The patient vomited the medication (amount retained undetermined). The attending physician then ordered two
doses of 40 mEq of intravenous potassium to infuse over a four-hour time period.
Documentation is problematic. It appears that despite the order for two doses of potassium 40 mEq to be infused
over four hours, the nurse administered two intravenous potassium doses of 20 mEq over approximately one hour
(documentation regarding this is inconclusive).
Throughout the day the nurse documented the patient’s heart rate in the patient care record. At 7:30 a.m. it was 72
beats per minute, at 1:30 p.m. it was 96 beats per minute and at 4:30 p.m. it was 116 beats per minute. The
patient’s blood pressure remained stable at 120/80. The nurse did not specifically notify the physician of the
pattern of rising heart rate. When the physician saw the patient that day, he noted that the patient’s white blood
cell and platelet counts remained higher than normal but were dropping.
In addition, her vital signs were within normal range and she was not in respiratory distress. He ordered a
pulmonary consult for possible bronchoscopy but deemed that she was stable, and that vasopressors and
aggressive pulmonary treatment were not necessary at that time. He ordered the patient to be transferred to the
High Dependency Unit. The nurse’s documentation fails to provide the exact time of transfer from the ICU to HDU
although it appears to have been between 7:15 p.m. and 7:30 p.m. The documentation also fails to validate the
nurse’s statement that the patient was on a cardiac monitor during her intensive care stay and that she was
transferred to the HDU with a cardiac monitor and oxygen therapy. The HDU nurse stated the patient did not arrive
with a monitor. Other HDU staff indicated that the unit was in an overflow situation when the patient was
transferred and the central monitoring station was not functioning. Shortly after the transfer, the patient became
unconscious and unresponsive. A MET was called and the critical response team attempted to resuscitate the
patient with no success. The patient had gone into cardiac arrest and died.
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 3
Medication Administration Error and Failure to Monitor
A 23-year-old woman with no significant medical history presented to ED with flu-like symptoms. She complained of
generalized body ache and had a fever of 38.8. For the past two weeks, she self-administered over- the-counter
medications with no relief. Instead, her condition deteriorated and she developed both shortness of breath and a
cough.
Following an abnormal CT Scan of the chest, an elevated white blood count and abnormal liver function test results,
the emergency department physician admitted the patient to ICU.
The patient was started on oxygen and antibiotic therapy. Blood cultures were drawn and showed Streptococcus
Pneumoniae and antibiotics were appropriately adjusted per recommendation of the infectious disease specialist.
The attending physician first saw the patient in the ICU. At the time of his initial exam, the patient was not in
significant respiratory distress, was responding well to the oxygen and antibiotic therapy, and was subsequently
continued on the same therapy. The attending physician noted that while the patient was not in acute distress, her
blood chemistry was abnormal with a potassium level of 2.9 (normal range is 3.5 to 5.0).
The physician ordered 30mEq of potassium to be added to each bag of the patient’s intravenous fluid, infused at 80
millilitres per hour. The order was to be maintained through the remainder of her course of treatment. Two days
later and despite the potassium added to her intravenous fluids, the patient’s potassium level was noted to be 3.0
and the attending physician ordered 80 mEq of potassium to be administered by mouth.
The patient vomited the medication (amount retained undetermined). The attending physician then ordered two
doses of 40 mEq of intravenous potassium to infuse over a four-hour time period.
Documentation is problematic. It appears that despite the order for two doses of potassium 40 mEq to be infused
over four hours, the nurse administered two intravenous potassium doses of 20 mEq over approximately one hour
(documentation regarding this is inconclusive).
Throughout the day the nurse documented the patient’s heart rate in the patient care record. At 7:30 a.m. it was 72
beats per minute, at 1:30 p.m. it was 96 beats per minute and at 4:30 p.m. it was 116 beats per minute. The
patient’s blood pressure remained stable at 120/80. The nurse did not specifically notify the physician of the
pattern of rising heart rate. When the physician saw the patient that day, he noted that the patient’s white blood
cell and platelet counts remained higher than normal but were dropping.
In addition, her vital signs were within normal range and she was not in respiratory distress. He ordered a
pulmonary consult for possible bronchoscopy but deemed that she was stable, and that vasopressors and
aggressive pulmonary treatment were not necessary at that time. He ordered the patient to be transferred to the
High Dependency Unit. The nurse’s documentation fails to provide the exact time of transfer from the ICU to HDU
although it appears to have been between 7:15 p.m. and 7:30 p.m. The documentation also fails to validate the
nurse’s statement that the patient was on a cardiac monitor during her intensive care stay and that she was
transferred to the HDU with a cardiac monitor and oxygen therapy. The HDU nurse stated the patient did not arrive
with a monitor. Other HDU staff indicated that the unit was in an overflow situation when the patient was
transferred and the central monitoring station was not functioning. Shortly after the transfer, the patient became
unconscious and unresponsive. A MET was called and the critical response team attempted to resuscitate the
patient with no success. The patient had gone into cardiac arrest and died.
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1. Research one of the models of reflective practice (Example: Kolb- Learning Cycle, Gibbs- Reflective
Cycle, Schon- Reflective Practice) and outline the model.
Gibbs’ Reflective Cycle
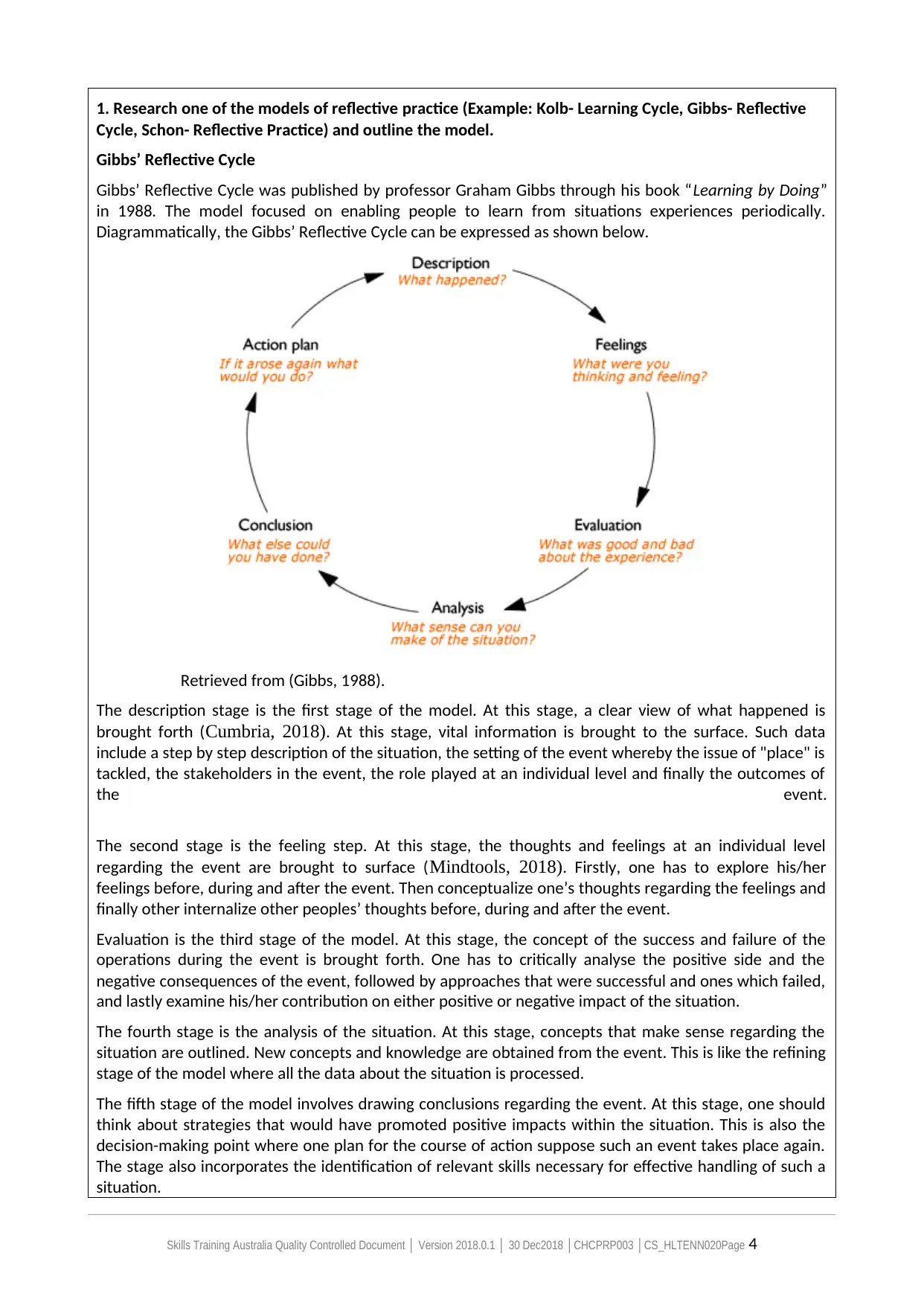
Gibbs’ Reflective Cycle was published by professor Graham Gibbs through his book “Learning by Doing”
in 1988. The model focused on enabling people to learn from situations experiences periodically.
Diagrammatically, the Gibbs’ Reflective Cycle can be expressed as shown below.
Retrieved from (Gibbs, 1988).
The description stage is the first stage of the model. At this stage, a clear view of what happened is
brought forth (Cumbria, 2018). At this stage, vital information is brought to the surface. Such data
include a step by step description of the situation, the setting of the event whereby the issue of "place" is
tackled, the stakeholders in the event, the role played at an individual level and finally the outcomes of
the event.
The second stage is the feeling step. At this stage, the thoughts and feelings at an individual level
regarding the event are brought to surface (Mindtools, 2018). Firstly, one has to explore his/her
feelings before, during and after the event. Then conceptualize one’s thoughts regarding the feelings and
finally other internalize other peoples’ thoughts before, during and after the event.
Evaluation is the third stage of the model. At this stage, the concept of the success and failure of the
operations during the event is brought forth. One has to critically analyse the positive side and the
negative consequences of the event, followed by approaches that were successful and ones which failed,
and lastly examine his/her contribution on either positive or negative impact of the situation.
The fourth stage is the analysis of the situation. At this stage, concepts that make sense regarding the
situation are outlined. New concepts and knowledge are obtained from the event. This is like the refining
stage of the model where all the data about the situation is processed.
The fifth stage of the model involves drawing conclusions regarding the event. At this stage, one should
think about strategies that would have promoted positive impacts within the situation. This is also the
decision-making point where one plan for the course of action suppose such an event takes place again.
The stage also incorporates the identification of relevant skills necessary for effective handling of such a
situation.
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 4
Cycle, Schon- Reflective Practice) and outline the model.
Gibbs’ Reflective Cycle
Gibbs’ Reflective Cycle was published by professor Graham Gibbs through his book “Learning by Doing”
in 1988. The model focused on enabling people to learn from situations experiences periodically.
Diagrammatically, the Gibbs’ Reflective Cycle can be expressed as shown below.
Retrieved from (Gibbs, 1988).
The description stage is the first stage of the model. At this stage, a clear view of what happened is
brought forth (Cumbria, 2018). At this stage, vital information is brought to the surface. Such data
include a step by step description of the situation, the setting of the event whereby the issue of "place" is
tackled, the stakeholders in the event, the role played at an individual level and finally the outcomes of
the event.
The second stage is the feeling step. At this stage, the thoughts and feelings at an individual level
regarding the event are brought to surface (Mindtools, 2018). Firstly, one has to explore his/her
feelings before, during and after the event. Then conceptualize one’s thoughts regarding the feelings and
finally other internalize other peoples’ thoughts before, during and after the event.
Evaluation is the third stage of the model. At this stage, the concept of the success and failure of the
operations during the event is brought forth. One has to critically analyse the positive side and the
negative consequences of the event, followed by approaches that were successful and ones which failed,
and lastly examine his/her contribution on either positive or negative impact of the situation.
The fourth stage is the analysis of the situation. At this stage, concepts that make sense regarding the
situation are outlined. New concepts and knowledge are obtained from the event. This is like the refining
stage of the model where all the data about the situation is processed.
The fifth stage of the model involves drawing conclusions regarding the event. At this stage, one should
think about strategies that would have promoted positive impacts within the situation. This is also the
decision-making point where one plan for the course of action suppose such an event takes place again.
The stage also incorporates the identification of relevant skills necessary for effective handling of such a
situation.
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

The sixth and final step of the model is the action stage. This stage involves execution of the suggested
strategies in the conclusion stage. As the name suggests, this stage circumnavigates the implementation
process. It is also at this stage where a monitoring and evaluation plan is designed.
Trainer comments: S NYS
☐ ☒
/10
2. Using the model you have outlined above, reflect on the case study as if you were the nurse
involved. Describe the steps you might go through as you reflect on this event and the conclusions you
came to in relation to improvements to your practice.
Step 1. Description
The description is as entailed in the case study provided
Step 2. Feeling
Just before the event, I was optimistic that the patient shall be well. Such feelings were vivid even within
the other medical practitioners as expressed through the medical physician who realized that the patient
was not in significant respiratory distress and responded excellently to antibiotic and oxygen therapy.
The abnormal potassium level in the blood despite having added in the intravenous fluid made me
worried. I think a similar feeling rose through other medical practitioners as the physician tried her level
best to settle the condition. After the event, I felt too bad to have not secured the life of the patient. I
thought I was the one to be blamed. I think a similar feeling of incompetence was felt by the physician
who didn't make a follow up on her delivery of healthcare services.
Step 3. Evaluation
The good thing is that the patient responded very well to oxygen and antibiotic therapy. Also, the patient
was free from significant respiratory distress. Furthermore, the diagnosis process was successful whereby
abnormalities were successfully identified while their courses of action are present. However, some
things didn't occur as expected. For instance, the abnormal potassium level in the body blood was a huge
issue. The patient could not respond despite administering potassium in the intravenous fluid. The
patient vomits the second dosage and documentation lacks clarity on how to administer the third
dosage. The patient also presents increasing heartbeats despite all the other body conditions being
normal. As a result, the patient went into a cardiac arrest and died.
Step 4. Analysis
Two major concepts made sense to me. Firstly, I realized the importance and significance of proper
documentation in the work-place. Documentation failure was a real issue in the entire crisis. Secondly, I
opened up my senses against assumptions. Every variation has to be undertaken seriously. For instance, I
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 5
strategies in the conclusion stage. As the name suggests, this stage circumnavigates the implementation
process. It is also at this stage where a monitoring and evaluation plan is designed.
Trainer comments: S NYS
☐ ☒
/10
2. Using the model you have outlined above, reflect on the case study as if you were the nurse
involved. Describe the steps you might go through as you reflect on this event and the conclusions you
came to in relation to improvements to your practice.
Step 1. Description
The description is as entailed in the case study provided
Step 2. Feeling
Just before the event, I was optimistic that the patient shall be well. Such feelings were vivid even within
the other medical practitioners as expressed through the medical physician who realized that the patient
was not in significant respiratory distress and responded excellently to antibiotic and oxygen therapy.
The abnormal potassium level in the blood despite having added in the intravenous fluid made me
worried. I think a similar feeling rose through other medical practitioners as the physician tried her level
best to settle the condition. After the event, I felt too bad to have not secured the life of the patient. I
thought I was the one to be blamed. I think a similar feeling of incompetence was felt by the physician
who didn't make a follow up on her delivery of healthcare services.
Step 3. Evaluation
The good thing is that the patient responded very well to oxygen and antibiotic therapy. Also, the patient
was free from significant respiratory distress. Furthermore, the diagnosis process was successful whereby
abnormalities were successfully identified while their courses of action are present. However, some
things didn't occur as expected. For instance, the abnormal potassium level in the body blood was a huge
issue. The patient could not respond despite administering potassium in the intravenous fluid. The
patient vomits the second dosage and documentation lacks clarity on how to administer the third
dosage. The patient also presents increasing heartbeats despite all the other body conditions being
normal. As a result, the patient went into a cardiac arrest and died.
Step 4. Analysis
Two major concepts made sense to me. Firstly, I realized the importance and significance of proper
documentation in the work-place. Documentation failure was a real issue in the entire crisis. Secondly, I
opened up my senses against assumptions. Every variation has to be undertaken seriously. For instance, I
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 5

failed to take the increasing heartbeats seriously assuming the patient was faring well as everything else
was normal.
Step 5. Conclusion
Apart from what I did in this situation, I feel it was vital to acknowledge the physician about the rising
heartbeats in the patient. Additionally, proper documentation and clarification regarding the
administering of prescribed medicine were essential. This situation required nursing skills and knowledge
across all the body variations and the appropriate means of settling the abnormalities. Suppose such
happens again in future, I will be kin and prepared to tackle each and every abnormality effectively while
promoting efficient monitoring and evaluation of the situation.
Ste 6. Action
Since this situation resulted from incompetence at the workplace, Implementation action starts from
incorporating an electronic system to replace our manual documentation process within the workplace.
Additionally, a training and development program shall be initiated to promote proper communication
within the workplace, to enhance clarification on doctors’ prescriptions. Furthermore, an action plan
which is policy oriented shall be initiated against cases involving reporting incompetence among the
nursing staff. Monitoring and evaluation shall be done every week whereby the outcomes of the courses
of action shall be compared to the plan to identify the gaps and incorporate appropriate corrective
actions.
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 6
was normal.
Step 5. Conclusion
Apart from what I did in this situation, I feel it was vital to acknowledge the physician about the rising
heartbeats in the patient. Additionally, proper documentation and clarification regarding the
administering of prescribed medicine were essential. This situation required nursing skills and knowledge
across all the body variations and the appropriate means of settling the abnormalities. Suppose such
happens again in future, I will be kin and prepared to tackle each and every abnormality effectively while
promoting efficient monitoring and evaluation of the situation.
Ste 6. Action
Since this situation resulted from incompetence at the workplace, Implementation action starts from
incorporating an electronic system to replace our manual documentation process within the workplace.
Additionally, a training and development program shall be initiated to promote proper communication
within the workplace, to enhance clarification on doctors’ prescriptions. Furthermore, an action plan
which is policy oriented shall be initiated against cases involving reporting incompetence among the
nursing staff. Monitoring and evaluation shall be done every week whereby the outcomes of the courses
of action shall be compared to the plan to identify the gaps and incorporate appropriate corrective
actions.
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
References
Cumbria (2018). Gibbs’ reflective Cycle [online]. Retrieved from:
https://my.cumbria.ac.uk/media/MyCumbria/Documents/ReflectiveCycleGibbs.pdf (Accessed on
30 March 2019)
Gibbs G (1988) Learning by Doing: A guide to teaching and learning methods. Further Education
Unit. Oxford Polytechnic: Oxford. Retrieved from:
https://www.brookes.ac.uk/students/upgrade/study-skills/reflective-writing-gibbs/ (Accessed on
30 March 2019).
Mindtools (2018). Gibbs’ Reflective Cycle: Helping people learn from experience [online].
Retrieved from: https://www.mindtools.com/pages/article/reflective-cycle.htm (Accessed on 30
March 2019).
Trainer comments: S NYS
☐ ☐
/10
Outcome S ☐ NS ☐
Grade /20
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 7
Cumbria (2018). Gibbs’ reflective Cycle [online]. Retrieved from:
https://my.cumbria.ac.uk/media/MyCumbria/Documents/ReflectiveCycleGibbs.pdf (Accessed on
30 March 2019)
Gibbs G (1988) Learning by Doing: A guide to teaching and learning methods. Further Education
Unit. Oxford Polytechnic: Oxford. Retrieved from:
https://www.brookes.ac.uk/students/upgrade/study-skills/reflective-writing-gibbs/ (Accessed on
30 March 2019).
Mindtools (2018). Gibbs’ Reflective Cycle: Helping people learn from experience [online].
Retrieved from: https://www.mindtools.com/pages/article/reflective-cycle.htm (Accessed on 30
March 2019).
Trainer comments: S NYS
☐ ☐
/10
Outcome S ☐ NS ☐
Grade /20
Skills Training Australia Quality Controlled Document │ Version 2018.0.1 │ 30 Dec2018 │CHCPRP003 │CS_HLTENN020Page 7
1 out of 7
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.