Clinical Virology: DENV & CHIKV Infection Comparison & Arthralgia
VerifiedAdded on 2023/06/12
|5
|5572
|94
Journal and Reflective Writing
AI Summary
This study, conducted in Kuala Lumpur, Malaysia, retrospectively compares Chikungunya virus (CHIKV) and Dengue virus (DENV) infections in adult patients to identify differentiating clinical and laboratory factors and to determine predictors of persistent arthralgia in CHIKV patients. The study included 53 CHIKV and 113 DENV patients, finding that CHIKV patients were older and more likely to be female, with arthralgia and rash being independently associated with CHIKV, while myalgia, raised aspartate transaminase, and leucopaenia were associated with DENV. Follow-up interviews with CHIKV patients revealed that 45% experienced persistent arthralgia beyond 4 months, with age >40 years being an independent predictor. The research concludes that specific clinical and laboratory findings can help distinguish between DENV and CHIKV infections, and persistent arthralgia is a frequent sequel of CHIKV infection. Find more solved assignments on our website.

Journal of Clinical Virology 56 (2013) 141–145
Contentslists available at SciVerse ScienceDirect
Journal of Clinical Virology
j o u r n al h om e p a g e :w w w . e l s e v i e r . c o m / l o c a t e / j c v
Chikungunya infection in Malaysia: Comparison with dengueinfection in adults
and predictors of persistent arthralgia
M.A. Mohd Zima, I.-C. Samb,∗, S.F.Syed Omarc, Y.F. Chanb, S. AbuBakarb, A. Kamarulzamanc
a Departmentof Medicine,Facultyof Medicine,UniversitiTeknologiMARA, ShahAlam,Malaysia
b TropicalInfectiousDiseasesResearchand EducationCentre,Departmentof Medical Microbiology,Facultyof Medicine,UniversityMalaya, Kuala Lumpur,Malaysia
c InfectiousDiseasesUnit, Departmentof Medicine,Facultyof Medicine,UniversityMalaya, Kuala Lumpur,Malaysia
a r t i c l e i n f o
Articlehistory:
Received10 April 2012
Receivedin revised form 2 October 2012
Accepted30 October 2012
Keywords:
Chikungunyavirus
Denguevirus
Malaysia
Arthralgia
Rash
Differential diagnosis
a b s t r a c t
Background:Chikungunya virus (CHIKV) and dengue virus (DENV) co-circulate in areas endemic with
the Aedesmosquito vectors. Both viruses cause similar illnesses which may be difficult to distinguish
clinically. CHIKV is also associatedwith persistent arthralgia.
Objectives:To compare and describefactors which differentiatebetween DENV and CHIKV infections on
presentation;and to describepredictors of persistent arthralgiain CHIKV patients.
Studydesign:Patients aged>14yearsdiagnosedwith acuteCHIKV and DENV infections in Kuala Lumpur,
Malaysia were retrospectively identified. Clinical and laboratory data were obtained from medical
records, and compared. CHIKV patients were telephoned 15–24 months later and interviewed about
persistent symptoms.Logistic regressionanalysiswas performed.
Results:A total of 53 CHIKV and 113 DENV patients were included. CHIKV patients were older and more
likely to be female.CHIKV was independentlyassociatedwith arthralgiaand rash,while DENV was asso-
ciatedwith myalgia,raised aspartatetransaminase,and leucopaenia.Forty CHIKV patientswere followed
up, with a median duration of self-reportedarthralgiaof 3 months (range,0–24 months). Eighteen(45%)
had persistent arthralgia beyond 4 months, for which age >40years was an independent predictor. At 1
year,9 (22.5%)patients had arthralgia.
Conclusion:In Kuala Lumpur, selected clinical and laboratory predictors help to distinguish between
DENV and CHIKV infections.Persistentarthralgiawas a frequent sequelof CHIKV infection in this cohort.
© 2012 Elsevier B.V. All rights reserved.
1. Background
Chikungunyavirus (CHIKV) is a mosquito-borne alphavirus that
has caused large outbreaks affecting millions around the world in
recentyears,particularly in the Indian Ocean,1 Asia,2 and Africa.3 In
Malaysia, there have been sporadic limited outbreaksin the past,4,5
prior to the largest reported outbreak affecting the whole country
in 2008–2010.6 Denguevirus (DENV) is endemic in Malaysia.
Both CHIKV and DENV are transmitted by the mosquito vec-
tors Aedesaegyptiand Ae. albopictus.Both diseases cause similar
presentations,with fever, myalgia, headache,arthralgia, and rash.
Both viruses potentially co-circulate in the same Aedes-endemic
areas.7 As these are mainly developing countries where facilities
for virological diagnosis are often limited, the ability to clinically
Abbreviations:AST, aspartatetransaminase;CHIKV, Chikungunyavirus; CI, con-
fidence intervals; DENV, denguevirus; OR, odds ratio.
∗ Correspondingauthor. Tel.: +603 79492184;fax: +603 79675752.
E-mail address:jicsam@ummc.edu.my (I.-C.Sam).
differentiate between the two diseases assumes greater impor-
tance, in view of their different clinical courses and outcomes.
Comparativeclinical studies betweenthe two diseasesin adults are
scarce,often limited by small numbers, and differences in clinical
presentationsin one country may not be applicable to another.
Although the acute symptoms of CHIKV generally last about a
week and are self-limiting, an earlier study from South Africa sug-
gestedthat some patients do experiencechronic arthralgia lasting
for months to years.8 The recentglobal outbreakshave brought this
potential burden of long-term morbidity into focus.9.10 As there are
conflicting reports on how common persistentarthralgia is, further
follow-up data from different cohorts would be useful.
2. Objectives
This study aimed to compare and describefactors which would
help differentiate between DENV and CHIKV infections on presen-
tation. A secondaryobjective was to ascertainthe rate and describe
predictors of persistent arthralgia in CHIKV patients.
1386-6532/$– see front matter ©2012 Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.jcv.2012.10.019
Contentslists available at SciVerse ScienceDirect
Journal of Clinical Virology
j o u r n al h om e p a g e :w w w . e l s e v i e r . c o m / l o c a t e / j c v
Chikungunya infection in Malaysia: Comparison with dengueinfection in adults
and predictors of persistent arthralgia
M.A. Mohd Zima, I.-C. Samb,∗, S.F.Syed Omarc, Y.F. Chanb, S. AbuBakarb, A. Kamarulzamanc
a Departmentof Medicine,Facultyof Medicine,UniversitiTeknologiMARA, ShahAlam,Malaysia
b TropicalInfectiousDiseasesResearchand EducationCentre,Departmentof Medical Microbiology,Facultyof Medicine,UniversityMalaya, Kuala Lumpur,Malaysia
c InfectiousDiseasesUnit, Departmentof Medicine,Facultyof Medicine,UniversityMalaya, Kuala Lumpur,Malaysia
a r t i c l e i n f o
Articlehistory:
Received10 April 2012
Receivedin revised form 2 October 2012
Accepted30 October 2012
Keywords:
Chikungunyavirus
Denguevirus
Malaysia
Arthralgia
Rash
Differential diagnosis
a b s t r a c t
Background:Chikungunya virus (CHIKV) and dengue virus (DENV) co-circulate in areas endemic with
the Aedesmosquito vectors. Both viruses cause similar illnesses which may be difficult to distinguish
clinically. CHIKV is also associatedwith persistent arthralgia.
Objectives:To compare and describefactors which differentiatebetween DENV and CHIKV infections on
presentation;and to describepredictors of persistent arthralgiain CHIKV patients.
Studydesign:Patients aged>14yearsdiagnosedwith acuteCHIKV and DENV infections in Kuala Lumpur,
Malaysia were retrospectively identified. Clinical and laboratory data were obtained from medical
records, and compared. CHIKV patients were telephoned 15–24 months later and interviewed about
persistent symptoms.Logistic regressionanalysiswas performed.
Results:A total of 53 CHIKV and 113 DENV patients were included. CHIKV patients were older and more
likely to be female.CHIKV was independentlyassociatedwith arthralgiaand rash,while DENV was asso-
ciatedwith myalgia,raised aspartatetransaminase,and leucopaenia.Forty CHIKV patientswere followed
up, with a median duration of self-reportedarthralgiaof 3 months (range,0–24 months). Eighteen(45%)
had persistent arthralgia beyond 4 months, for which age >40years was an independent predictor. At 1
year,9 (22.5%)patients had arthralgia.
Conclusion:In Kuala Lumpur, selected clinical and laboratory predictors help to distinguish between
DENV and CHIKV infections.Persistentarthralgiawas a frequent sequelof CHIKV infection in this cohort.
© 2012 Elsevier B.V. All rights reserved.
1. Background
Chikungunyavirus (CHIKV) is a mosquito-borne alphavirus that
has caused large outbreaks affecting millions around the world in
recentyears,particularly in the Indian Ocean,1 Asia,2 and Africa.3 In
Malaysia, there have been sporadic limited outbreaksin the past,4,5
prior to the largest reported outbreak affecting the whole country
in 2008–2010.6 Denguevirus (DENV) is endemic in Malaysia.
Both CHIKV and DENV are transmitted by the mosquito vec-
tors Aedesaegyptiand Ae. albopictus.Both diseases cause similar
presentations,with fever, myalgia, headache,arthralgia, and rash.
Both viruses potentially co-circulate in the same Aedes-endemic
areas.7 As these are mainly developing countries where facilities
for virological diagnosis are often limited, the ability to clinically
Abbreviations:AST, aspartatetransaminase;CHIKV, Chikungunyavirus; CI, con-
fidence intervals; DENV, denguevirus; OR, odds ratio.
∗ Correspondingauthor. Tel.: +603 79492184;fax: +603 79675752.
E-mail address:jicsam@ummc.edu.my (I.-C.Sam).
differentiate between the two diseases assumes greater impor-
tance, in view of their different clinical courses and outcomes.
Comparativeclinical studies betweenthe two diseasesin adults are
scarce,often limited by small numbers, and differences in clinical
presentationsin one country may not be applicable to another.
Although the acute symptoms of CHIKV generally last about a
week and are self-limiting, an earlier study from South Africa sug-
gestedthat some patients do experiencechronic arthralgia lasting
for months to years.8 The recentglobal outbreakshave brought this
potential burden of long-term morbidity into focus.9.10 As there are
conflicting reports on how common persistentarthralgia is, further
follow-up data from different cohorts would be useful.
2. Objectives
This study aimed to compare and describefactors which would
help differentiate between DENV and CHIKV infections on presen-
tation. A secondaryobjective was to ascertainthe rate and describe
predictors of persistent arthralgia in CHIKV patients.
1386-6532/$– see front matter ©2012 Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.jcv.2012.10.019
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

142 M.A. Mohd Zim et al. / Journal of Clinical Virology56 (2013) 141–145
3. Study design
This study was conductedat the University Malaya Medical Cen-
tre, in Kuala Lumpur, Malaysia. Patients aged >14years with acute
CHIKV and DENV infections confirmed by the diagnostic virology
laboratory from April 2008 to July 2009 were retrospectivelyiden-
tified. Two DENV caseswere randomly selectedfor eachCHIKV case
identified. Confirmed CHIKV infections had a positive culture, pos-
itive PCR detection of the E1 gene,11 or positive IgM by indirect
immunofluorescence.4 As serum samples were taken at different
time-points after onset of symptoms for each patient,not all CHIKV
patients were tested by all three methods.We used a positive viral
culture as specific confirmation of acute DENV infection, as a sin-
gle positive dengue IgM may also indicate infection up to several
months ago. Cultures were performed using Vero (African green
monkey kidney) and C6/36 (Ae. albopictus) cells, and identified
with polyclonal anti-CHIKV or monoclonal anti-DENV antibodies.
The medical records of the identified patients were reviewed for
demographic,clinical and laboratory data on initial presentationat
the hospital. Ethical approval for the study was obtained from the
hospital’s Medical Ethics Committee.
For follow-up, CHIKV patients were contacted by telephone in
2011.Informed consent was first obtained.The interview was con-
ducted using a predefinedstructured questionnaire.Data collected
included duration of symptoms, the intensity of self-reported pain
during the initial attack and chronic phases,and impact of symp-
toms on activitiesof daily living. Declarativenumerical rating scales
(NRS) were used to evaluate the pain intensity during the acute
and chronic phases.The pain score ranges between 0 and 10, and
were categorized into pain-free (0), mild (1–3), moderate (4–6)
and severe (7–10).12 In two previous studies, including one from
Malaysia, >95%of patients were pain-free by 3 months.3,5 For this
study, persistent arthralgia was defined as the presence of self-
reported pain more than 4 months after the acute illness.
Data were analyzed using SPSS15.0 (SPSSInc., Chicago,IL). For
univariate analysis, Mann–Whitney U tests were used for contin-
uous variables, and Fisher’s exact or chi-squared tests were used
for categorical variables. Logistic regression analysis was carried
out for two separate outcomes: first, to predict either DENV or
CHIKV infection; and second,to predict CHIKV patientswith persis-
tent arthralgia. Univariate logistic regression was initially carried
out for selectedvariables,basedon previous studies and biological
plausibility. Odds ratio (OR) and 95%confidenceintervals (CI) were
calculated.Those variables significant at p <0.2 were entered into
the multivariate regressionmodel, and retainedbasedon the likeli-
hood ratio test. Final values of p <0.05 were consideredsignificant.
The final model was then tested for collinearity, and assessedwith
the Hosmer and Lemeshow goodness-of-fit test and calculation of
the area under the receiver operating characteristiccurve.
4. Results
A total of 60 patients with confirmed CHIKV and 120 patients
with confirmed DENV were identified from laboratory records, for
which medical records could not be located for 7 CHIKV and 7
DENV patients.A total of 53 CHIKV patients and 113 DENV patients
were therefore included in the study. For CHIKV, 35 patients were
diagnosed by IgM, 12 by PCR, and 17 by culture, or a combina-
tion of these. The predominant DENV serotypes were DENV1 (46,
40.7%)and DENV2 (46, 40.7%),followed by DENV3 (20, 17.7%)and
DENV4 (1, 0.9%).The patients’ demographic details are shown in
Table 1. Compared to DENV patients, CHIKV patients were signifi-
cantly older and more likely to be female. There was a significant
difference in ethnicity, due to a greater number of non-Malaysian
nationals (n =28, 24.8%)diagnosed with DENV. These comprised
patients from Bangladesh(n =12), Nepal (n =11), Indonesia (n =4),
and Vietnam (n =1). There were 82 (72.6%)admissions in the DENV
group, and only 12 (22.6%)in the CHIKV group ( 2 =36.6,p <0.001).
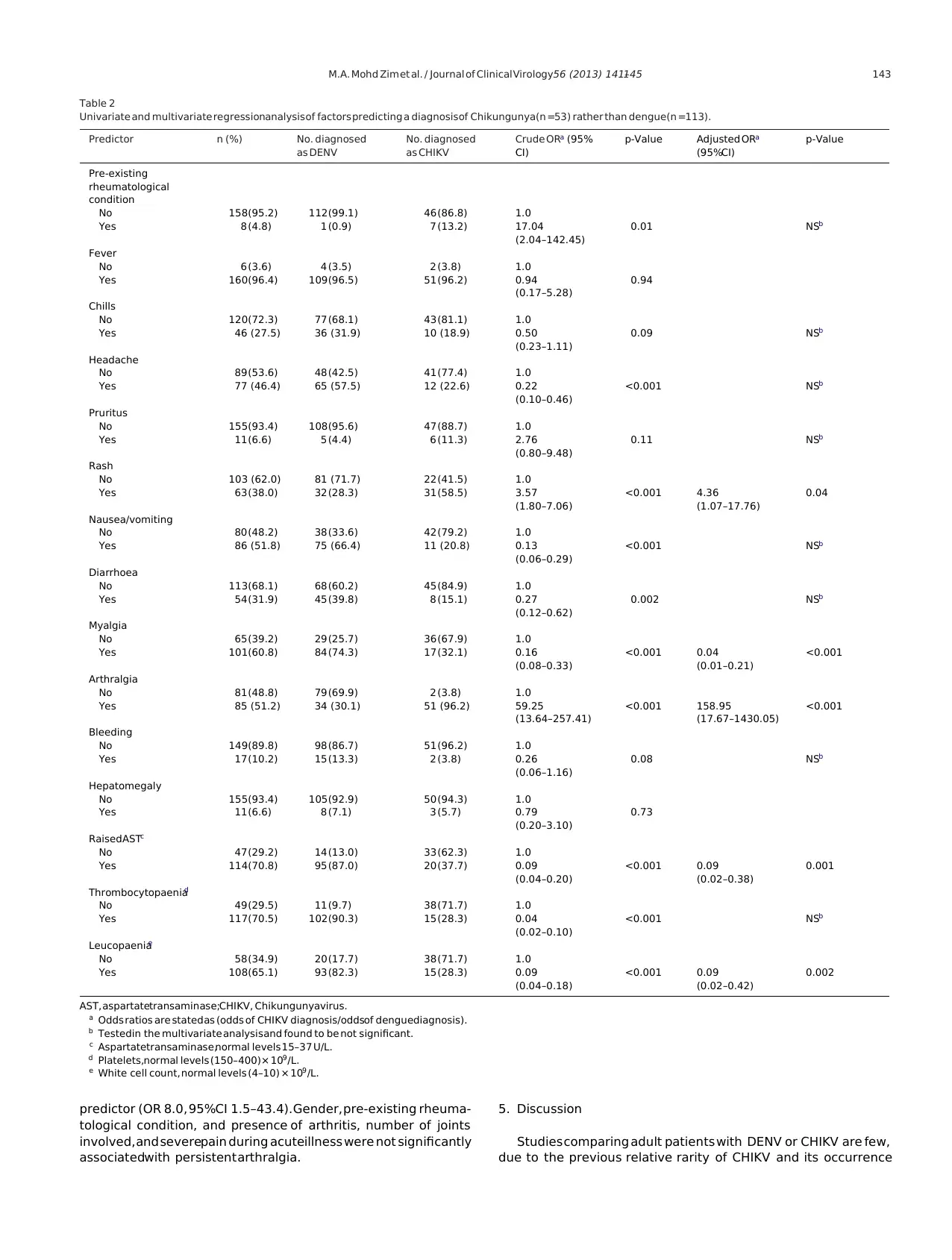
Clinical and biochemical test comparisons between CHIKV and
DENV patients at presentation are shown in Table 2. The 5 most
frequently reported presenting symptoms in CHIKV patients were
fever (96.2%),arthralgia (96.2%),rash (58.5%),myalgia (32.1%),and
headache(22.6%).DENV patientscommonly reported fever (96.4%),
myalgia (74.3%),nausea/vomiting (66.4%),headache (57.5%),and
diarrhoea(39.8%).On univariate analysis,DENV patientswere more
likely to have headache,nausea/vomiting,diarrhoea, and myalgia;
while CHIKV patients were more likely to report rash and arthral-
gia. CHIKV patients had significantly lower aspartatetransaminase
levels (AST; 114.0 vs. 144.9U/L, p <0.001),higher white cell counts
(5.9 vs. 2.9 × 109/L, p <0.001),and higher platelet counts (200.9 vs.
78.5× 109/L, p =0.001).
On multivariate analysis, CHIKV was associatedwith arthralgia
(OR 159.0,95%CI 17.7–1430.1)and rash (OR 4.4, 95%CI 1.1–17.8);
and absenceof myalgia (OR 0.04,95%CI 0.01–0.2),absenceof raised
AST (OR 0.09,95%CI 0.02–0.4),and absenceof leucopaenia(OR 0.09,
95%CI 0.02–0.4).This model had satisfactory fit ( 2 =5.3, p =0.72)
and discrimination (area under the curve =0.97, 95%CI 0.95–0.99,
p <0.001).At a predicted probability cut-off value of 0.5,this model
had a sensitivity of 88.7%,specificity of 96.3%,positive predictive
value of 92.2%,negative predictive value of 94.5%,positive likeli-
hood ratio of 24.0, and negativelikelihood ratio of 0.12.
Patients with CHIKV were then telephoned for follow-up inter-
views, a mean duration of 20 ± 2 months (range, 15–24 months)
after the initial illness. Out of 53 CHIKV patients, 40 patients
were interviewed. Of the 13 patients not interviewed, 10 had the
incorrect contact numbers in their medical records, 1 patient had
migrated,and 2 patients had died – one death was associatedwith
CHIKV, as previously described,13 while the other death was due to
unrelated causes.At the time of interview, 31 (77.5%)were pain-
free, while 9 (22.5%)still had arthralgia, of which 6 had mild pain
and 3 had moderatepain. In 17 (42.5%)patients,arthralgia affected
at least one daily activity for <30 days, 20 (50%) patients were
affectedfor 30–90 days,and 3 (7.5%)were affectedfor >90days.The
median self-reported duration of arthralgia was 3 months (range,
0–24 months), with 18 (45.0%)of the patients reporting persistent
arthralgia beyond 4 months, and 9/40 (22.5%)beyond 1 year.
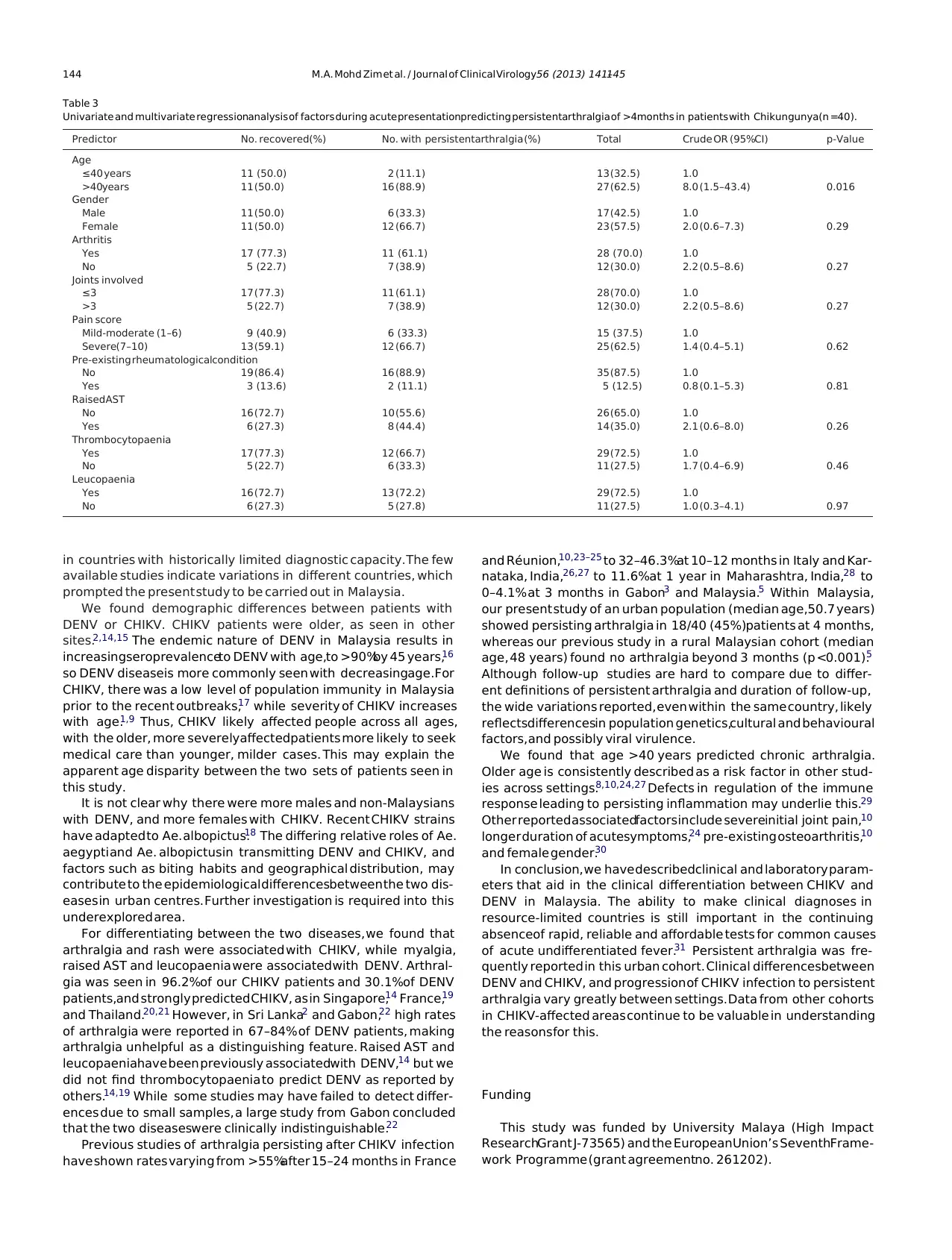
Analysis of selectedpredictors of persistent arthralgia is shown
in Table 3. Only age >40 years was shown to be an independent
Table 1
Demographiccharacteristicsof patients with Chikungunya(n =53) and dengue(n =113).
Factor Denguepatients (n, %) Chikungunyapatients (n, %) Total 2 p-Value
Age (years; mean± standard deviation) 31.0± 13.2 49.2± 14.0 – <0.001
Gender
Male 79 (69.9) 22 (41.5) 101(60.8) 12.2 0.001
Female 34 (30.1) 31 (58.5) 65 (39.2)
Ethnicity
Malay 47 (41.6) 30 (56.6) 77 (46.4) 13.4 0.004
Chinese 22 (19.5) 14 (26.4) 36 (21.7)
Indian 16 (14.2) 8 (15.1) 24 (14.5)
Others 28 (24.8) 1 (1.9) 29 (17.5)
3. Study design
This study was conductedat the University Malaya Medical Cen-
tre, in Kuala Lumpur, Malaysia. Patients aged >14years with acute
CHIKV and DENV infections confirmed by the diagnostic virology
laboratory from April 2008 to July 2009 were retrospectivelyiden-
tified. Two DENV caseswere randomly selectedfor eachCHIKV case
identified. Confirmed CHIKV infections had a positive culture, pos-
itive PCR detection of the E1 gene,11 or positive IgM by indirect
immunofluorescence.4 As serum samples were taken at different
time-points after onset of symptoms for each patient,not all CHIKV
patients were tested by all three methods.We used a positive viral
culture as specific confirmation of acute DENV infection, as a sin-
gle positive dengue IgM may also indicate infection up to several
months ago. Cultures were performed using Vero (African green
monkey kidney) and C6/36 (Ae. albopictus) cells, and identified
with polyclonal anti-CHIKV or monoclonal anti-DENV antibodies.
The medical records of the identified patients were reviewed for
demographic,clinical and laboratory data on initial presentationat
the hospital. Ethical approval for the study was obtained from the
hospital’s Medical Ethics Committee.
For follow-up, CHIKV patients were contacted by telephone in
2011.Informed consent was first obtained.The interview was con-
ducted using a predefinedstructured questionnaire.Data collected
included duration of symptoms, the intensity of self-reported pain
during the initial attack and chronic phases,and impact of symp-
toms on activitiesof daily living. Declarativenumerical rating scales
(NRS) were used to evaluate the pain intensity during the acute
and chronic phases.The pain score ranges between 0 and 10, and
were categorized into pain-free (0), mild (1–3), moderate (4–6)
and severe (7–10).12 In two previous studies, including one from
Malaysia, >95%of patients were pain-free by 3 months.3,5 For this
study, persistent arthralgia was defined as the presence of self-
reported pain more than 4 months after the acute illness.
Data were analyzed using SPSS15.0 (SPSSInc., Chicago,IL). For
univariate analysis, Mann–Whitney U tests were used for contin-
uous variables, and Fisher’s exact or chi-squared tests were used
for categorical variables. Logistic regression analysis was carried
out for two separate outcomes: first, to predict either DENV or
CHIKV infection; and second,to predict CHIKV patientswith persis-
tent arthralgia. Univariate logistic regression was initially carried
out for selectedvariables,basedon previous studies and biological
plausibility. Odds ratio (OR) and 95%confidenceintervals (CI) were
calculated.Those variables significant at p <0.2 were entered into
the multivariate regressionmodel, and retainedbasedon the likeli-
hood ratio test. Final values of p <0.05 were consideredsignificant.
The final model was then tested for collinearity, and assessedwith
the Hosmer and Lemeshow goodness-of-fit test and calculation of
the area under the receiver operating characteristiccurve.
4. Results
A total of 60 patients with confirmed CHIKV and 120 patients
with confirmed DENV were identified from laboratory records, for
which medical records could not be located for 7 CHIKV and 7
DENV patients.A total of 53 CHIKV patients and 113 DENV patients
were therefore included in the study. For CHIKV, 35 patients were
diagnosed by IgM, 12 by PCR, and 17 by culture, or a combina-
tion of these. The predominant DENV serotypes were DENV1 (46,
40.7%)and DENV2 (46, 40.7%),followed by DENV3 (20, 17.7%)and
DENV4 (1, 0.9%).The patients’ demographic details are shown in
Table 1. Compared to DENV patients, CHIKV patients were signifi-
cantly older and more likely to be female. There was a significant
difference in ethnicity, due to a greater number of non-Malaysian
nationals (n =28, 24.8%)diagnosed with DENV. These comprised
patients from Bangladesh(n =12), Nepal (n =11), Indonesia (n =4),
and Vietnam (n =1). There were 82 (72.6%)admissions in the DENV
group, and only 12 (22.6%)in the CHIKV group ( 2 =36.6,p <0.001).
Clinical and biochemical test comparisons between CHIKV and
DENV patients at presentation are shown in Table 2. The 5 most
frequently reported presenting symptoms in CHIKV patients were
fever (96.2%),arthralgia (96.2%),rash (58.5%),myalgia (32.1%),and
headache(22.6%).DENV patientscommonly reported fever (96.4%),
myalgia (74.3%),nausea/vomiting (66.4%),headache (57.5%),and
diarrhoea(39.8%).On univariate analysis,DENV patientswere more
likely to have headache,nausea/vomiting,diarrhoea, and myalgia;
while CHIKV patients were more likely to report rash and arthral-
gia. CHIKV patients had significantly lower aspartatetransaminase
levels (AST; 114.0 vs. 144.9U/L, p <0.001),higher white cell counts
(5.9 vs. 2.9 × 109/L, p <0.001),and higher platelet counts (200.9 vs.
78.5× 109/L, p =0.001).
On multivariate analysis, CHIKV was associatedwith arthralgia
(OR 159.0,95%CI 17.7–1430.1)and rash (OR 4.4, 95%CI 1.1–17.8);
and absenceof myalgia (OR 0.04,95%CI 0.01–0.2),absenceof raised
AST (OR 0.09,95%CI 0.02–0.4),and absenceof leucopaenia(OR 0.09,
95%CI 0.02–0.4).This model had satisfactory fit ( 2 =5.3, p =0.72)
and discrimination (area under the curve =0.97, 95%CI 0.95–0.99,
p <0.001).At a predicted probability cut-off value of 0.5,this model
had a sensitivity of 88.7%,specificity of 96.3%,positive predictive
value of 92.2%,negative predictive value of 94.5%,positive likeli-
hood ratio of 24.0, and negativelikelihood ratio of 0.12.
Patients with CHIKV were then telephoned for follow-up inter-
views, a mean duration of 20 ± 2 months (range, 15–24 months)
after the initial illness. Out of 53 CHIKV patients, 40 patients
were interviewed. Of the 13 patients not interviewed, 10 had the
incorrect contact numbers in their medical records, 1 patient had
migrated,and 2 patients had died – one death was associatedwith
CHIKV, as previously described,13 while the other death was due to
unrelated causes.At the time of interview, 31 (77.5%)were pain-
free, while 9 (22.5%)still had arthralgia, of which 6 had mild pain
and 3 had moderatepain. In 17 (42.5%)patients,arthralgia affected
at least one daily activity for <30 days, 20 (50%) patients were
affectedfor 30–90 days,and 3 (7.5%)were affectedfor >90days.The
median self-reported duration of arthralgia was 3 months (range,
0–24 months), with 18 (45.0%)of the patients reporting persistent
arthralgia beyond 4 months, and 9/40 (22.5%)beyond 1 year.
Analysis of selectedpredictors of persistent arthralgia is shown
in Table 3. Only age >40 years was shown to be an independent
Table 1
Demographiccharacteristicsof patients with Chikungunya(n =53) and dengue(n =113).
Factor Denguepatients (n, %) Chikungunyapatients (n, %) Total 2 p-Value
Age (years; mean± standard deviation) 31.0± 13.2 49.2± 14.0 – <0.001
Gender
Male 79 (69.9) 22 (41.5) 101(60.8) 12.2 0.001
Female 34 (30.1) 31 (58.5) 65 (39.2)
Ethnicity
Malay 47 (41.6) 30 (56.6) 77 (46.4) 13.4 0.004
Chinese 22 (19.5) 14 (26.4) 36 (21.7)
Indian 16 (14.2) 8 (15.1) 24 (14.5)
Others 28 (24.8) 1 (1.9) 29 (17.5)
M.A. Mohd Zim et al. / Journal of Clinical Virology56 (2013) 141–145 143
Table 2
Univariate and multivariate regressionanalysis of factors predicting a diagnosisof Chikungunya(n =53) rather than dengue(n =113).
Predictor n (%) No. diagnosed
as DENV
No. diagnosed
as CHIKV
Crude ORa (95%
CI)
p-Value Adjusted ORa
(95%CI)
p-Value
Pre-existing
rheumatological
condition
No 158(95.2) 112 (99.1) 46 (86.8) 1.0
Yes 8 (4.8) 1 (0.9) 7 (13.2) 17.04
(2.04–142.45)
0.01 NSb
Fever
No 6 (3.6) 4 (3.5) 2 (3.8) 1.0
Yes 160(96.4) 109 (96.5) 51 (96.2) 0.94
(0.17–5.28)
0.94
Chills
No 120(72.3) 77 (68.1) 43 (81.1) 1.0
Yes 46 (27.5) 36 (31.9) 10 (18.9) 0.50
(0.23–1.11)
0.09 NSb
Headache
No 89 (53.6) 48 (42.5) 41 (77.4) 1.0
Yes 77 (46.4) 65 (57.5) 12 (22.6) 0.22
(0.10–0.46)
<0.001 NSb
Pruritus
No 155(93.4) 108 (95.6) 47 (88.7) 1.0
Yes 11 (6.6) 5 (4.4) 6 (11.3) 2.76
(0.80–9.48)
0.11 NSb
Rash
No 103 (62.0) 81 (71.7) 22 (41.5) 1.0
Yes 63 (38.0) 32 (28.3) 31 (58.5) 3.57
(1.80–7.06)
<0.001 4.36
(1.07–17.76)
0.04
Nausea/vomiting
No 80 (48.2) 38 (33.6) 42 (79.2) 1.0
Yes 86 (51.8) 75 (66.4) 11 (20.8) 0.13
(0.06–0.29)
<0.001 NSb
Diarrhoea
No 113(68.1) 68 (60.2) 45 (84.9) 1.0
Yes 54 (31.9) 45 (39.8) 8 (15.1) 0.27
(0.12–0.62)
0.002 NSb
Myalgia
No 65 (39.2) 29 (25.7) 36 (67.9) 1.0
Yes 101(60.8) 84 (74.3) 17 (32.1) 0.16
(0.08–0.33)
<0.001 0.04
(0.01–0.21)
<0.001
Arthralgia
No 81 (48.8) 79 (69.9) 2 (3.8) 1.0
Yes 85 (51.2) 34 (30.1) 51 (96.2) 59.25
(13.64–257.41)
<0.001 158.95
(17.67–1430.05)
<0.001
Bleeding
No 149(89.8) 98 (86.7) 51 (96.2) 1.0
Yes 17 (10.2) 15 (13.3) 2 (3.8) 0.26
(0.06–1.16)
0.08 NSb
Hepatomegaly
No 155(93.4) 105 (92.9) 50 (94.3) 1.0
Yes 11 (6.6) 8 (7.1) 3 (5.7) 0.79
(0.20–3.10)
0.73
RaisedASTc
No 47 (29.2) 14 (13.0) 33 (62.3) 1.0
Yes 114(70.8) 95 (87.0) 20 (37.7) 0.09
(0.04–0.20)
<0.001 0.09
(0.02–0.38)
0.001
Thrombocytopaeniad
No 49 (29.5) 11 (9.7) 38 (71.7) 1.0
Yes 117(70.5) 102 (90.3) 15 (28.3) 0.04
(0.02–0.10)
<0.001 NSb
Leucopaeniae
No 58 (34.9) 20 (17.7) 38 (71.7) 1.0
Yes 108(65.1) 93 (82.3) 15 (28.3) 0.09
(0.04–0.18)
<0.001 0.09
(0.02–0.42)
0.002
AST, aspartatetransaminase;CHIKV, Chikungunyavirus.
a Odds ratios are stated as (odds of CHIKV diagnosis/oddsof denguediagnosis).
b Testedin the multivariate analysisand found to be not significant.
c Aspartatetransaminase,normal levels 15–37 U/L.
d Platelets,normal levels (150–400)× 109/L.
e White cell count, normal levels (4–10) × 109/L.
predictor (OR 8.0, 95%CI 1.5–43.4). Gender, pre-existing rheuma-
tological condition, and presence of arthritis, number of joints
involved, and severepain during acuteillness were not significantly
associatedwith persistent arthralgia.
5. Discussion
Studies comparing adult patients with DENV or CHIKV are few,
due to the previous relative rarity of CHIKV and its occurrence
Table 2
Univariate and multivariate regressionanalysis of factors predicting a diagnosisof Chikungunya(n =53) rather than dengue(n =113).
Predictor n (%) No. diagnosed
as DENV
No. diagnosed
as CHIKV
Crude ORa (95%
CI)
p-Value Adjusted ORa
(95%CI)
p-Value
Pre-existing
rheumatological
condition
No 158(95.2) 112 (99.1) 46 (86.8) 1.0
Yes 8 (4.8) 1 (0.9) 7 (13.2) 17.04
(2.04–142.45)
0.01 NSb
Fever
No 6 (3.6) 4 (3.5) 2 (3.8) 1.0
Yes 160(96.4) 109 (96.5) 51 (96.2) 0.94
(0.17–5.28)
0.94
Chills
No 120(72.3) 77 (68.1) 43 (81.1) 1.0
Yes 46 (27.5) 36 (31.9) 10 (18.9) 0.50
(0.23–1.11)
0.09 NSb
Headache
No 89 (53.6) 48 (42.5) 41 (77.4) 1.0
Yes 77 (46.4) 65 (57.5) 12 (22.6) 0.22
(0.10–0.46)
<0.001 NSb
Pruritus
No 155(93.4) 108 (95.6) 47 (88.7) 1.0
Yes 11 (6.6) 5 (4.4) 6 (11.3) 2.76
(0.80–9.48)
0.11 NSb
Rash
No 103 (62.0) 81 (71.7) 22 (41.5) 1.0
Yes 63 (38.0) 32 (28.3) 31 (58.5) 3.57
(1.80–7.06)
<0.001 4.36
(1.07–17.76)
0.04
Nausea/vomiting
No 80 (48.2) 38 (33.6) 42 (79.2) 1.0
Yes 86 (51.8) 75 (66.4) 11 (20.8) 0.13
(0.06–0.29)
<0.001 NSb
Diarrhoea
No 113(68.1) 68 (60.2) 45 (84.9) 1.0
Yes 54 (31.9) 45 (39.8) 8 (15.1) 0.27
(0.12–0.62)
0.002 NSb
Myalgia
No 65 (39.2) 29 (25.7) 36 (67.9) 1.0
Yes 101(60.8) 84 (74.3) 17 (32.1) 0.16
(0.08–0.33)
<0.001 0.04
(0.01–0.21)
<0.001
Arthralgia
No 81 (48.8) 79 (69.9) 2 (3.8) 1.0
Yes 85 (51.2) 34 (30.1) 51 (96.2) 59.25
(13.64–257.41)
<0.001 158.95
(17.67–1430.05)
<0.001
Bleeding
No 149(89.8) 98 (86.7) 51 (96.2) 1.0
Yes 17 (10.2) 15 (13.3) 2 (3.8) 0.26
(0.06–1.16)
0.08 NSb
Hepatomegaly
No 155(93.4) 105 (92.9) 50 (94.3) 1.0
Yes 11 (6.6) 8 (7.1) 3 (5.7) 0.79
(0.20–3.10)
0.73
RaisedASTc
No 47 (29.2) 14 (13.0) 33 (62.3) 1.0
Yes 114(70.8) 95 (87.0) 20 (37.7) 0.09
(0.04–0.20)
<0.001 0.09
(0.02–0.38)
0.001
Thrombocytopaeniad
No 49 (29.5) 11 (9.7) 38 (71.7) 1.0
Yes 117(70.5) 102 (90.3) 15 (28.3) 0.04
(0.02–0.10)
<0.001 NSb
Leucopaeniae
No 58 (34.9) 20 (17.7) 38 (71.7) 1.0
Yes 108(65.1) 93 (82.3) 15 (28.3) 0.09
(0.04–0.18)
<0.001 0.09
(0.02–0.42)
0.002
AST, aspartatetransaminase;CHIKV, Chikungunyavirus.
a Odds ratios are stated as (odds of CHIKV diagnosis/oddsof denguediagnosis).
b Testedin the multivariate analysisand found to be not significant.
c Aspartatetransaminase,normal levels 15–37 U/L.
d Platelets,normal levels (150–400)× 109/L.
e White cell count, normal levels (4–10) × 109/L.
predictor (OR 8.0, 95%CI 1.5–43.4). Gender, pre-existing rheuma-
tological condition, and presence of arthritis, number of joints
involved, and severepain during acuteillness were not significantly
associatedwith persistent arthralgia.
5. Discussion
Studies comparing adult patients with DENV or CHIKV are few,
due to the previous relative rarity of CHIKV and its occurrence
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
144 M.A. Mohd Zim et al. / Journal of Clinical Virology56 (2013) 141–145
Table 3
Univariate and multivariate regressionanalysis of factors during acute presentationpredicting persistentarthralgia of >4months in patients with Chikungunya(n =40).
Predictor No. recovered(%) No. with persistentarthralgia (%) Total Crude OR (95%CI) p-Value
Age
≤40 years 11 (50.0) 2 (11.1) 13 (32.5) 1.0
>40years 11 (50.0) 16 (88.9) 27 (62.5) 8.0 (1.5–43.4) 0.016
Gender
Male 11 (50.0) 6 (33.3) 17 (42.5) 1.0
Female 11 (50.0) 12 (66.7) 23 (57.5) 2.0 (0.6–7.3) 0.29
Arthritis
Yes 17 (77.3) 11 (61.1) 28 (70.0) 1.0
No 5 (22.7) 7 (38.9) 12 (30.0) 2.2 (0.5–8.6) 0.27
Joints involved
≤3 17 (77.3) 11 (61.1) 28 (70.0) 1.0
>3 5 (22.7) 7 (38.9) 12 (30.0) 2.2 (0.5–8.6) 0.27
Pain score
Mild-moderate (1–6) 9 (40.9) 6 (33.3) 15 (37.5) 1.0
Severe(7–10) 13 (59.1) 12 (66.7) 25 (62.5) 1.4 (0.4–5.1) 0.62
Pre-existing rheumatologicalcondition
No 19 (86.4) 16 (88.9) 35 (87.5) 1.0
Yes 3 (13.6) 2 (11.1) 5 (12.5) 0.8 (0.1–5.3) 0.81
RaisedAST
No 16 (72.7) 10 (55.6) 26 (65.0) 1.0
Yes 6 (27.3) 8 (44.4) 14 (35.0) 2.1 (0.6–8.0) 0.26
Thrombocytopaenia
Yes 17 (77.3) 12 (66.7) 29 (72.5) 1.0
No 5 (22.7) 6 (33.3) 11 (27.5) 1.7 (0.4–6.9) 0.46
Leucopaenia
Yes 16 (72.7) 13 (72.2) 29 (72.5) 1.0
No 6 (27.3) 5 (27.8) 11 (27.5) 1.0 (0.3–4.1) 0.97
in countries with historically limited diagnostic capacity. The few
available studies indicate variations in different countries, which
prompted the present study to be carried out in Malaysia.
We found demographic differences between patients with
DENV or CHIKV. CHIKV patients were older, as seen in other
sites.2,14,15 The endemic nature of DENV in Malaysia results in
increasingseroprevalenceto DENV with age,to >90%by 45 years,16
so DENV diseaseis more commonly seen with decreasingage.For
CHIKV, there was a low level of population immunity in Malaysia
prior to the recent outbreaks,17 while severity of CHIKV increases
with age.1,9 Thus, CHIKV likely affected people across all ages,
with the older, more severelyaffectedpatients more likely to seek
medical care than younger, milder cases. This may explain the
apparent age disparity between the two sets of patients seen in
this study.
It is not clear why there were more males and non-Malaysians
with DENV, and more females with CHIKV. Recent CHIKV strains
have adapted to Ae. albopictus.18 The differing relative roles of Ae.
aegypti and Ae. albopictusin transmitting DENV and CHIKV, and
factors such as biting habits and geographical distribution, may
contribute to the epidemiological differencesbetween the two dis-
eases in urban centres. Further investigation is required into this
underexplored area.
For differentiating between the two diseases, we found that
arthralgia and rash were associated with CHIKV, while myalgia,
raised AST and leucopaenia were associated with DENV. Arthral-
gia was seen in 96.2%of our CHIKV patients and 30.1%of DENV
patients,and strongly predicted CHIKV, as in Singapore,14 France,19
and Thailand.20,21 However, in Sri Lanka2 and Gabon,22 high rates
of arthralgia were reported in 67–84% of DENV patients, making
arthralgia unhelpful as a distinguishing feature. Raised AST and
leucopaeniahave been previously associatedwith DENV,14 but we
did not find thrombocytopaenia to predict DENV as reported by
others.14,19 While some studies may have failed to detect differ-
ences due to small samples, a large study from Gabon concluded
that the two diseaseswere clinically indistinguishable.22
Previous studies of arthralgia persisting after CHIKV infection
have shown rates varying from >55%after 15–24 months in France
and Réunion,10,23–25 to 32–46.3%at 10–12 months in Italy and Kar-
nataka, India,26,27 to 11.6%at 1 year in Maharashtra, India,28 to
0–4.1% at 3 months in Gabon3 and Malaysia.5 Within Malaysia,
our present study of an urban population (median age,50.7 years)
showed persisting arthralgia in 18/40 (45%)patients at 4 months,
whereas our previous study in a rural Malaysian cohort (median
age, 48 years) found no arthralgia beyond 3 months (p <0.001).5
Although follow-up studies are hard to compare due to differ-
ent definitions of persistent arthralgia and duration of follow-up,
the wide variations reported, even within the same country, likely
reflectsdifferencesin population genetics,cultural and behavioural
factors, and possibly viral virulence.
We found that age >40 years predicted chronic arthralgia.
Older age is consistently described as a risk factor in other stud-
ies across settings.8,10,24,27 Defects in regulation of the immune
response leading to persisting inflammation may underlie this.29
Other reported associatedfactors include severeinitial joint pain,10
longer duration of acutesymptoms,24 pre-existing osteoarthritis,10
and female gender.30
In conclusion, we have describedclinical and laboratory param-
eters that aid in the clinical differentiation between CHIKV and
DENV in Malaysia. The ability to make clinical diagnoses in
resource-limited countries is still important in the continuing
absenceof rapid, reliable and affordable tests for common causes
of acute undifferentiated fever.31 Persistent arthralgia was fre-
quently reported in this urban cohort. Clinical differencesbetween
DENV and CHIKV, and progression of CHIKV infection to persistent
arthralgia vary greatly between settings. Data from other cohorts
in CHIKV-affected areas continue to be valuable in understanding
the reasonsfor this.
Funding
This study was funded by University Malaya (High Impact
ResearchGrant J-73565) and the EuropeanUnion’s SeventhFrame-
work Programme (grant agreementno. 261202).
Table 3
Univariate and multivariate regressionanalysis of factors during acute presentationpredicting persistentarthralgia of >4months in patients with Chikungunya(n =40).
Predictor No. recovered(%) No. with persistentarthralgia (%) Total Crude OR (95%CI) p-Value
Age
≤40 years 11 (50.0) 2 (11.1) 13 (32.5) 1.0
>40years 11 (50.0) 16 (88.9) 27 (62.5) 8.0 (1.5–43.4) 0.016
Gender
Male 11 (50.0) 6 (33.3) 17 (42.5) 1.0
Female 11 (50.0) 12 (66.7) 23 (57.5) 2.0 (0.6–7.3) 0.29
Arthritis
Yes 17 (77.3) 11 (61.1) 28 (70.0) 1.0
No 5 (22.7) 7 (38.9) 12 (30.0) 2.2 (0.5–8.6) 0.27
Joints involved
≤3 17 (77.3) 11 (61.1) 28 (70.0) 1.0
>3 5 (22.7) 7 (38.9) 12 (30.0) 2.2 (0.5–8.6) 0.27
Pain score
Mild-moderate (1–6) 9 (40.9) 6 (33.3) 15 (37.5) 1.0
Severe(7–10) 13 (59.1) 12 (66.7) 25 (62.5) 1.4 (0.4–5.1) 0.62
Pre-existing rheumatologicalcondition
No 19 (86.4) 16 (88.9) 35 (87.5) 1.0
Yes 3 (13.6) 2 (11.1) 5 (12.5) 0.8 (0.1–5.3) 0.81
RaisedAST
No 16 (72.7) 10 (55.6) 26 (65.0) 1.0
Yes 6 (27.3) 8 (44.4) 14 (35.0) 2.1 (0.6–8.0) 0.26
Thrombocytopaenia
Yes 17 (77.3) 12 (66.7) 29 (72.5) 1.0
No 5 (22.7) 6 (33.3) 11 (27.5) 1.7 (0.4–6.9) 0.46
Leucopaenia
Yes 16 (72.7) 13 (72.2) 29 (72.5) 1.0
No 6 (27.3) 5 (27.8) 11 (27.5) 1.0 (0.3–4.1) 0.97
in countries with historically limited diagnostic capacity. The few
available studies indicate variations in different countries, which
prompted the present study to be carried out in Malaysia.
We found demographic differences between patients with
DENV or CHIKV. CHIKV patients were older, as seen in other
sites.2,14,15 The endemic nature of DENV in Malaysia results in
increasingseroprevalenceto DENV with age,to >90%by 45 years,16
so DENV diseaseis more commonly seen with decreasingage.For
CHIKV, there was a low level of population immunity in Malaysia
prior to the recent outbreaks,17 while severity of CHIKV increases
with age.1,9 Thus, CHIKV likely affected people across all ages,
with the older, more severelyaffectedpatients more likely to seek
medical care than younger, milder cases. This may explain the
apparent age disparity between the two sets of patients seen in
this study.
It is not clear why there were more males and non-Malaysians
with DENV, and more females with CHIKV. Recent CHIKV strains
have adapted to Ae. albopictus.18 The differing relative roles of Ae.
aegypti and Ae. albopictusin transmitting DENV and CHIKV, and
factors such as biting habits and geographical distribution, may
contribute to the epidemiological differencesbetween the two dis-
eases in urban centres. Further investigation is required into this
underexplored area.
For differentiating between the two diseases, we found that
arthralgia and rash were associated with CHIKV, while myalgia,
raised AST and leucopaenia were associated with DENV. Arthral-
gia was seen in 96.2%of our CHIKV patients and 30.1%of DENV
patients,and strongly predicted CHIKV, as in Singapore,14 France,19
and Thailand.20,21 However, in Sri Lanka2 and Gabon,22 high rates
of arthralgia were reported in 67–84% of DENV patients, making
arthralgia unhelpful as a distinguishing feature. Raised AST and
leucopaeniahave been previously associatedwith DENV,14 but we
did not find thrombocytopaenia to predict DENV as reported by
others.14,19 While some studies may have failed to detect differ-
ences due to small samples, a large study from Gabon concluded
that the two diseaseswere clinically indistinguishable.22
Previous studies of arthralgia persisting after CHIKV infection
have shown rates varying from >55%after 15–24 months in France
and Réunion,10,23–25 to 32–46.3%at 10–12 months in Italy and Kar-
nataka, India,26,27 to 11.6%at 1 year in Maharashtra, India,28 to
0–4.1% at 3 months in Gabon3 and Malaysia.5 Within Malaysia,
our present study of an urban population (median age,50.7 years)
showed persisting arthralgia in 18/40 (45%)patients at 4 months,
whereas our previous study in a rural Malaysian cohort (median
age, 48 years) found no arthralgia beyond 3 months (p <0.001).5
Although follow-up studies are hard to compare due to differ-
ent definitions of persistent arthralgia and duration of follow-up,
the wide variations reported, even within the same country, likely
reflectsdifferencesin population genetics,cultural and behavioural
factors, and possibly viral virulence.
We found that age >40 years predicted chronic arthralgia.
Older age is consistently described as a risk factor in other stud-
ies across settings.8,10,24,27 Defects in regulation of the immune
response leading to persisting inflammation may underlie this.29
Other reported associatedfactors include severeinitial joint pain,10
longer duration of acutesymptoms,24 pre-existing osteoarthritis,10
and female gender.30
In conclusion, we have describedclinical and laboratory param-
eters that aid in the clinical differentiation between CHIKV and
DENV in Malaysia. The ability to make clinical diagnoses in
resource-limited countries is still important in the continuing
absenceof rapid, reliable and affordable tests for common causes
of acute undifferentiated fever.31 Persistent arthralgia was fre-
quently reported in this urban cohort. Clinical differencesbetween
DENV and CHIKV, and progression of CHIKV infection to persistent
arthralgia vary greatly between settings. Data from other cohorts
in CHIKV-affected areas continue to be valuable in understanding
the reasonsfor this.
Funding
This study was funded by University Malaya (High Impact
ResearchGrant J-73565) and the EuropeanUnion’s SeventhFrame-
work Programme (grant agreementno. 261202).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
M.A. Mohd Zim et al. / Journal of Clinical Virology56 (2013) 141–145 145
Competing interests
None declared.
Ethical approval
Ethical approval was obtained from the Medical Ethics Com-
mittee of the University Malaya Medical Centre (referencenumber
800.70).
References
1. Staikowsky F, Talarmin F, Grivard P, Souab A, SchuffeneckerI, Le Roux K, et al.
Prospectivestudy of Chikungunyavirus acute infection in the island of La Réu-
nion during the 2005–2006 outbreak.PLoSONE 2009;4:e7603.
2. Kularatne SAM, Gihan MC, WeerasingheSC,GunasenaS. Concurrent outbreaks
of Chikungunyaand denguefever in Kandy, Sri Lanka,2006–07: a comparative
analysis of clinical and laboratory features.PostgradMed J 2009;85:342–6.
3. Nkoghe D, KassaRF, Caron M, Grard G, Mombo I, Bikié B, et al. Clinical forms of
Chikungunyain Gabon, 2010.PLoSNeglTrop Dis 2012;6:e1517.
4. Lam SK, Chua KB, Hooi PS, Rahimah MA, Kumari S, Tharmaratnam M, et al.
Chikungunyainfection – an emergingdiseasein Malaysia. SoutheastAsianJ Trop
Med Public Health2001;32:447–51.
5. Ayu SM, Lai LR, Chan YF, Hatim A, Hairi NN, Ayob A, et al. Seroprevalence
survey of Chikungunya virus in Bagan Panchor, Malaysia. Am J Trop Med Hyg
2010;83:1245–8.
6. SamIC, ChanYF, ChanSY, Loong SK,Chin HK, Hooi PS,et al. Chikungunyavirus of
Asian and Central/EastAfrican genotypesin Malaysia.J Clin Virol 2009;46:180–3.
7. Singh P, Mittal V, Rizvi MMA, Chhabra M, Sharma P, Rawat DS, et al.
The first dominant co-circulation of both dengue and chikungunya viruses
during the post-monsoon period of 2010 in Delhi, India. Epidemiol Infect
2012;140:1337–42.
8. Brighton SW, Prozesky OW, de la Harpe AL. Chikungunya virus infection – a
retrospectivestudy of 107 cases.S Afr Med J 1983;63:313–5.
9. Borgherini G, Poubeau P, Staikowsky F, Lory M, Le Moullec N, BecquartJP, et al.
Outbreak of Chikungunyaon Reunion Island: early clinical and laboratory fea-
tures in 157 adult patients.Clin InfectDis 2007;44:1401–7.
10. Sissoko D, Malvy D, Ezzedine K, Renault P, Moscetti F, Ledrans M, et al.
Post-epidemic Chikungunya disease on Reunion Island: course of rheumatic
manifestationsand associatedfactors over a 15-month period. PLoS Negl Trop
Dis 2009;3:e389.
11. Hasebe F, Parquet MC, Pandey BD, Mathenge EG, Morita K, Balasubramaniam
V, et al. Combined detection and genotypingof chikungunyavirus by a specific
reversetranscription-polymerasechain reaction.J Med Virol 2002;67:370–4.
12. Downie WW, LeathamPA, Rhind VM, Wright V, Branco JA, Anderson JA. Studies
with pain rating scales.Ann RheumDis 1978;37:382–4.
13. Sam IC, KamarulzamanA, Ong GS,Veriah RS,PonnampalavanarS, Chan YF, et al.
Chikungunyavirus-associateddeath in Malaysia. Trop Biomed2010;27:343–7.
14. Lee VJ, Chow A, ZhengX, CarrascoLR, Cook AR, Lye DC, et al. Simple clinical and
laboratory predictors of Chikungunya versus dengue infections in adults. PLoS
NeglTrop Dis 2012;6:e1786.
15. Frank C, Schöneberg I, Stark K. Trends in imported Chikungunya virus
infections in Germany, 2006–2009. Vector Borne Zoonotic Dis 2011;11:
631–6.
16. Muhammad Azami NA, Salleh SA, Neoh HM, Syed Zakaria SZ, Jamal R. Dengue
epidemic in Malaysia: not a predominantly urban disease anymore. BMC Res
Notes2011;4:216.
17. Marchette NJ, Rudnick A, Garcia R. Alphavirusesin Peninsular Malaysia. II. Sero-
logical evidence of human infection. SoutheastAsian J Trop Med Public Health
1980;11:14–23.
18. TsetsarkinKA, Chen R, Leal G, Forrester N, Higgs S, Huang J, et al. Chikungunya
virus emergenceis constrainedin Asia by lineage-specificadaptivelandscapes.
Proc Natl Acad Sci U S A 2011;108:7872–7.
19. Hochedez P, Canestri A, Guihot A, Brichler S, Bricaire F, Caumes E. Manage-
ment of travellerswith fever and exanthema,notably dengueand Chikungunya
infections.Am J Trop Med Hyg 2008;78:710–3.
20. Nimmannitya S, Halstead SB, Cohen SN, Margiotta MR. Dengue and chikun-
gunya virus infection in man in Thailand, 1962–1964. I. Observations on
hospitalized patients with hemorrhagic fever. Am J Trop Med Hyg 1969;18:
954–71.
21. LaoprasopwattanaK, Kaewjungwad L, Jarumanokul R, Geater Al. Differential
diagnosisof Chikungunya,dengueviral infection and other acutefebrileillnesses
in children. PediatrInfectDis J 2012;31:459–63.
22. Nkoghe D, Kassa RFK, Bisvigou U, Caron M, Grard G, Leroy EM. No clinical
or biological difference between Chikungunya and dengue fever dur-
ing the 2010 Gabonese outbreak. Infect Dis Rep 2012;4:e5. Available at:
http://www.pagepress.org/journals/index.php/idr/article/view/idr.2012.e5/pdf
23. Larrieu S, Pouderoux N, Pistone T, Filleul L, Receveur MC, Sissoko D,
et al. Factors associated with persistence of arthralgia among Chikungunya
virus-infected travellers: report of 42 French cases. J Clin Virol 2010;47:
85–8.
24. Couturier E, Guillemin F, Mura M, Léon L, Virion JM, Letort MJ, et al. Impaired
quality of life after Chikungunya virus infection: a 2-year follow-up study.
Rheumatology(Oxford)2012;51:1315–22.
25. Borgherini G, PoubeauP, JoassaumeA, Gouix A, Cotte L, Michault A, et al. Persis-
tent arthralgia associatedwith Chikungunyavirus: a study of 88 adult patients
on Reunion Island. Clin InfectDis 2008;47:469–75.
26. Kelvin AA, Banner D, Silvi G, Moro ML, Spataro N, Gaibani P. Inflammatory
cytokine expressionis associatedwith Chikungunyavirus resolution and symp-
tom severity.PLoSNeglTrop Dis 2011;5:e1279.
27. Manimunda SP, Vijayachari P, Uppoor R, Sugunan AP, Singh SS, Rai SK, et al.
Clinical progression of chikungunya fever during acute and chronic arthritic
stagesand the changesin joint morphology as revealedby imaging.TransR Soc
Trop Med Hyg 2010;104:392–9.
28. ChopraA, AnuradhaV, GhorpadeR, SalujaM. Acute Chikungunyaand persistent
musculoskeletalpain following the 2006 Indian epidemic: a 2-year prospective
rural community study. EpidemiolInfect2012;140:842–50.
29. Dupuis-Maguiraga L, Noret M, Brun S, Le Grand R, Gras G, Roques P.
Chikungunya disease: infection-associated markers from the acute to the
chronic phase of arbovirus-induced arthralgia. PLoS Negl Trop Dis 2012;6:
e1446.
30. Win MK, Chow A, DimatatacF, Go CJ, Leo YS. Chikungunyafever in Singapore:
acute clinical and laboratory features, and factors associatedwith persistent
arthralgia.J Clin Virol 2010;49:111–4.
31. SamIC, Chua CL,Chan YF. Chikungunyavirus diagnosisin the developingworld:
a pressingneed. ExpertRevAnti InfectTher2011;9:1089–91.
Competing interests
None declared.
Ethical approval
Ethical approval was obtained from the Medical Ethics Com-
mittee of the University Malaya Medical Centre (referencenumber
800.70).
References
1. Staikowsky F, Talarmin F, Grivard P, Souab A, SchuffeneckerI, Le Roux K, et al.
Prospectivestudy of Chikungunyavirus acute infection in the island of La Réu-
nion during the 2005–2006 outbreak.PLoSONE 2009;4:e7603.
2. Kularatne SAM, Gihan MC, WeerasingheSC,GunasenaS. Concurrent outbreaks
of Chikungunyaand denguefever in Kandy, Sri Lanka,2006–07: a comparative
analysis of clinical and laboratory features.PostgradMed J 2009;85:342–6.
3. Nkoghe D, KassaRF, Caron M, Grard G, Mombo I, Bikié B, et al. Clinical forms of
Chikungunyain Gabon, 2010.PLoSNeglTrop Dis 2012;6:e1517.
4. Lam SK, Chua KB, Hooi PS, Rahimah MA, Kumari S, Tharmaratnam M, et al.
Chikungunyainfection – an emergingdiseasein Malaysia. SoutheastAsianJ Trop
Med Public Health2001;32:447–51.
5. Ayu SM, Lai LR, Chan YF, Hatim A, Hairi NN, Ayob A, et al. Seroprevalence
survey of Chikungunya virus in Bagan Panchor, Malaysia. Am J Trop Med Hyg
2010;83:1245–8.
6. SamIC, ChanYF, ChanSY, Loong SK,Chin HK, Hooi PS,et al. Chikungunyavirus of
Asian and Central/EastAfrican genotypesin Malaysia.J Clin Virol 2009;46:180–3.
7. Singh P, Mittal V, Rizvi MMA, Chhabra M, Sharma P, Rawat DS, et al.
The first dominant co-circulation of both dengue and chikungunya viruses
during the post-monsoon period of 2010 in Delhi, India. Epidemiol Infect
2012;140:1337–42.
8. Brighton SW, Prozesky OW, de la Harpe AL. Chikungunya virus infection – a
retrospectivestudy of 107 cases.S Afr Med J 1983;63:313–5.
9. Borgherini G, Poubeau P, Staikowsky F, Lory M, Le Moullec N, BecquartJP, et al.
Outbreak of Chikungunyaon Reunion Island: early clinical and laboratory fea-
tures in 157 adult patients.Clin InfectDis 2007;44:1401–7.
10. Sissoko D, Malvy D, Ezzedine K, Renault P, Moscetti F, Ledrans M, et al.
Post-epidemic Chikungunya disease on Reunion Island: course of rheumatic
manifestationsand associatedfactors over a 15-month period. PLoS Negl Trop
Dis 2009;3:e389.
11. Hasebe F, Parquet MC, Pandey BD, Mathenge EG, Morita K, Balasubramaniam
V, et al. Combined detection and genotypingof chikungunyavirus by a specific
reversetranscription-polymerasechain reaction.J Med Virol 2002;67:370–4.
12. Downie WW, LeathamPA, Rhind VM, Wright V, Branco JA, Anderson JA. Studies
with pain rating scales.Ann RheumDis 1978;37:382–4.
13. Sam IC, KamarulzamanA, Ong GS,Veriah RS,PonnampalavanarS, Chan YF, et al.
Chikungunyavirus-associateddeath in Malaysia. Trop Biomed2010;27:343–7.
14. Lee VJ, Chow A, ZhengX, CarrascoLR, Cook AR, Lye DC, et al. Simple clinical and
laboratory predictors of Chikungunya versus dengue infections in adults. PLoS
NeglTrop Dis 2012;6:e1786.
15. Frank C, Schöneberg I, Stark K. Trends in imported Chikungunya virus
infections in Germany, 2006–2009. Vector Borne Zoonotic Dis 2011;11:
631–6.
16. Muhammad Azami NA, Salleh SA, Neoh HM, Syed Zakaria SZ, Jamal R. Dengue
epidemic in Malaysia: not a predominantly urban disease anymore. BMC Res
Notes2011;4:216.
17. Marchette NJ, Rudnick A, Garcia R. Alphavirusesin Peninsular Malaysia. II. Sero-
logical evidence of human infection. SoutheastAsian J Trop Med Public Health
1980;11:14–23.
18. TsetsarkinKA, Chen R, Leal G, Forrester N, Higgs S, Huang J, et al. Chikungunya
virus emergenceis constrainedin Asia by lineage-specificadaptivelandscapes.
Proc Natl Acad Sci U S A 2011;108:7872–7.
19. Hochedez P, Canestri A, Guihot A, Brichler S, Bricaire F, Caumes E. Manage-
ment of travellerswith fever and exanthema,notably dengueand Chikungunya
infections.Am J Trop Med Hyg 2008;78:710–3.
20. Nimmannitya S, Halstead SB, Cohen SN, Margiotta MR. Dengue and chikun-
gunya virus infection in man in Thailand, 1962–1964. I. Observations on
hospitalized patients with hemorrhagic fever. Am J Trop Med Hyg 1969;18:
954–71.
21. LaoprasopwattanaK, Kaewjungwad L, Jarumanokul R, Geater Al. Differential
diagnosisof Chikungunya,dengueviral infection and other acutefebrileillnesses
in children. PediatrInfectDis J 2012;31:459–63.
22. Nkoghe D, Kassa RFK, Bisvigou U, Caron M, Grard G, Leroy EM. No clinical
or biological difference between Chikungunya and dengue fever dur-
ing the 2010 Gabonese outbreak. Infect Dis Rep 2012;4:e5. Available at:
http://www.pagepress.org/journals/index.php/idr/article/view/idr.2012.e5/pdf
23. Larrieu S, Pouderoux N, Pistone T, Filleul L, Receveur MC, Sissoko D,
et al. Factors associated with persistence of arthralgia among Chikungunya
virus-infected travellers: report of 42 French cases. J Clin Virol 2010;47:
85–8.
24. Couturier E, Guillemin F, Mura M, Léon L, Virion JM, Letort MJ, et al. Impaired
quality of life after Chikungunya virus infection: a 2-year follow-up study.
Rheumatology(Oxford)2012;51:1315–22.
25. Borgherini G, PoubeauP, JoassaumeA, Gouix A, Cotte L, Michault A, et al. Persis-
tent arthralgia associatedwith Chikungunyavirus: a study of 88 adult patients
on Reunion Island. Clin InfectDis 2008;47:469–75.
26. Kelvin AA, Banner D, Silvi G, Moro ML, Spataro N, Gaibani P. Inflammatory
cytokine expressionis associatedwith Chikungunyavirus resolution and symp-
tom severity.PLoSNeglTrop Dis 2011;5:e1279.
27. Manimunda SP, Vijayachari P, Uppoor R, Sugunan AP, Singh SS, Rai SK, et al.
Clinical progression of chikungunya fever during acute and chronic arthritic
stagesand the changesin joint morphology as revealedby imaging.TransR Soc
Trop Med Hyg 2010;104:392–9.
28. ChopraA, AnuradhaV, GhorpadeR, SalujaM. Acute Chikungunyaand persistent
musculoskeletalpain following the 2006 Indian epidemic: a 2-year prospective
rural community study. EpidemiolInfect2012;140:842–50.
29. Dupuis-Maguiraga L, Noret M, Brun S, Le Grand R, Gras G, Roques P.
Chikungunya disease: infection-associated markers from the acute to the
chronic phase of arbovirus-induced arthralgia. PLoS Negl Trop Dis 2012;6:
e1446.
30. Win MK, Chow A, DimatatacF, Go CJ, Leo YS. Chikungunyafever in Singapore:
acute clinical and laboratory features, and factors associatedwith persistent
arthralgia.J Clin Virol 2010;49:111–4.
31. SamIC, Chua CL,Chan YF. Chikungunyavirus diagnosisin the developingworld:
a pressingneed. ExpertRevAnti InfectTher2011;9:1089–91.
1 out of 5

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.