Childcare Information Sheet: Certificate III in Early Childhood
VerifiedAdded on 2024/05/17
|10
|2290
|248
Practical Assignment
AI Summary
This assignment presents a completed Childcare Information Sheet, a component of the Certificate III in Early Childhood Education. It includes detailed personal information, health concerns, eating and sleeping habits, and behavioral patterns for three children of varying ages (2, 4 and 5 years old). The sheet covers aspects such as allergies, medications, special diets, bedtime schedules, favorite activities, and comforting factors for each child. The document provides a comprehensive overview of each child's needs and preferences, offering valuable insights for childcare providers. Desklib is a platform where students can access similar solved assignments and study resources.
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
Reminder: You are required to complete this form for three children of varying
ages. The forms are numbered for your convenience.
To protect the privacy of all concerned, you are not required to provide the
complete names of children and their parents.
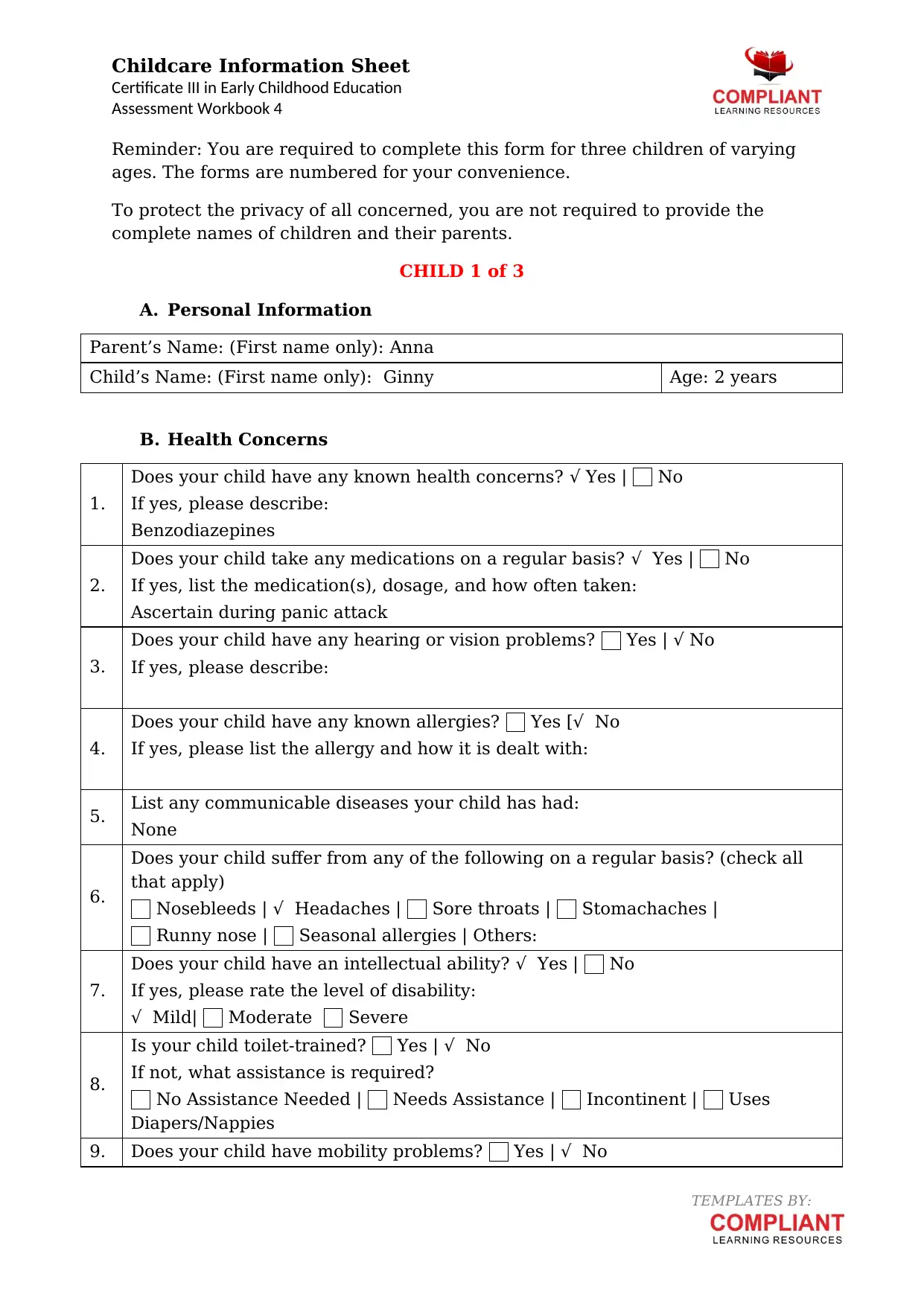
CHILD 1 of 3
A. Personal Information
Parent’s Name: (First name only): Anna
Child’s Name: (First name only): Ginny Age: 2 years
B. Health Concerns
1.
Does your child have any known health concerns? √ Yes | No
If yes, please describe:
Benzodiazepines
2.
Does your child take any medications on a regular basis? √ Yes | No
If yes, list the medication(s), dosage, and how often taken:
Ascertain during panic attack
3.
Does your child have any hearing or vision problems? Yes | √ No
If yes, please describe:
4.
Does your child have any known allergies? Yes [√ No
If yes, please list the allergy and how it is dealt with:
5. List any communicable diseases your child has had:
None
6.
Does your child suffer from any of the following on a regular basis? (check all
that apply)
Nosebleeds | √ Headaches | Sore throats | Stomachaches |
Runny nose | Seasonal allergies | Others:
7.
Does your child have an intellectual ability? √ Yes | No
If yes, please rate the level of disability:
√ Mild| Moderate Severe
8.
Is your child toilet-trained? Yes | √ No
If not, what assistance is required?
No Assistance Needed | Needs Assistance | Incontinent | Uses
Diapers/Nappies
9. Does your child have mobility problems? Yes | √ No
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
Reminder: You are required to complete this form for three children of varying
ages. The forms are numbered for your convenience.
To protect the privacy of all concerned, you are not required to provide the
complete names of children and their parents.
CHILD 1 of 3
A. Personal Information
Parent’s Name: (First name only): Anna
Child’s Name: (First name only): Ginny Age: 2 years
B. Health Concerns
1.
Does your child have any known health concerns? √ Yes | No
If yes, please describe:
Benzodiazepines
2.
Does your child take any medications on a regular basis? √ Yes | No
If yes, list the medication(s), dosage, and how often taken:
Ascertain during panic attack
3.
Does your child have any hearing or vision problems? Yes | √ No
If yes, please describe:
4.
Does your child have any known allergies? Yes [√ No
If yes, please list the allergy and how it is dealt with:
5. List any communicable diseases your child has had:
None
6.
Does your child suffer from any of the following on a regular basis? (check all
that apply)
Nosebleeds | √ Headaches | Sore throats | Stomachaches |
Runny nose | Seasonal allergies | Others:
7.
Does your child have an intellectual ability? √ Yes | No
If yes, please rate the level of disability:
√ Mild| Moderate Severe
8.
Is your child toilet-trained? Yes | √ No
If not, what assistance is required?
No Assistance Needed | Needs Assistance | Incontinent | Uses
Diapers/Nappies
9. Does your child have mobility problems? Yes | √ No
TEMPLATES BY:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
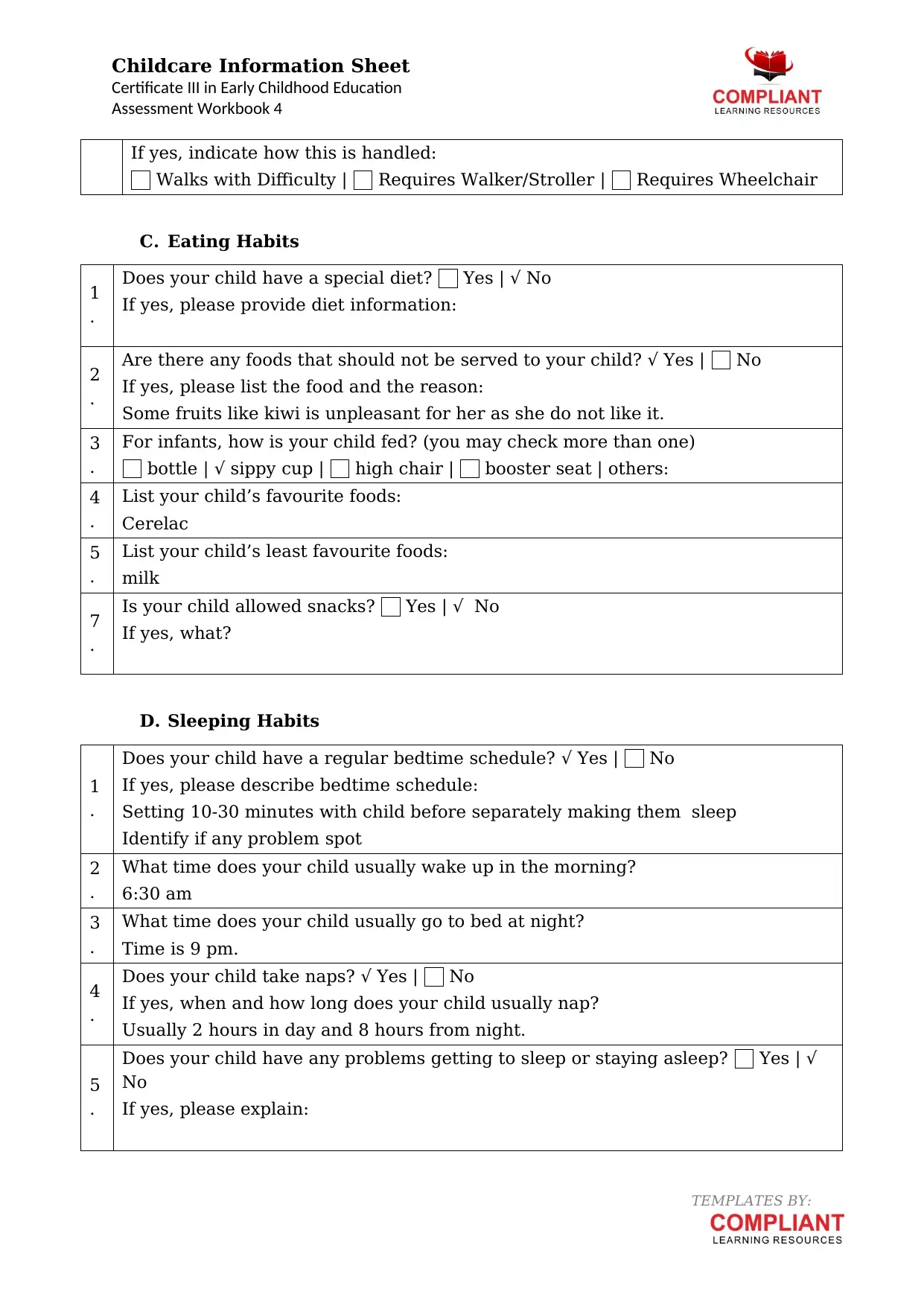
If yes, indicate how this is handled:
Walks with Difficulty | Requires Walker/Stroller | Requires Wheelchair
C. Eating Habits
1
.
Does your child have a special diet? Yes | √ No
If yes, please provide diet information:
2
.
Are there any foods that should not be served to your child? √ Yes | No
If yes, please list the food and the reason:
Some fruits like kiwi is unpleasant for her as she do not like it.
3
.
For infants, how is your child fed? (you may check more than one)
bottle | √ sippy cup | high chair | booster seat | others:
4
.
List your child’s favourite foods:
Cerelac
5
.
List your child’s least favourite foods:
milk
7
.
Is your child allowed snacks? Yes | √ No
If yes, what?
D. Sleeping Habits
1
.
Does your child have a regular bedtime schedule? √ Yes | No
If yes, please describe bedtime schedule:
Setting 10-30 minutes with child before separately making them sleep
Identify if any problem spot
2
.
What time does your child usually wake up in the morning?
6:30 am
3
.
What time does your child usually go to bed at night?
Time is 9 pm.
4
.
Does your child take naps? √ Yes | No
If yes, when and how long does your child usually nap?
Usually 2 hours in day and 8 hours from night.
5
.
Does your child have any problems getting to sleep or staying asleep? Yes | √
No
If yes, please explain:
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
If yes, indicate how this is handled:
Walks with Difficulty | Requires Walker/Stroller | Requires Wheelchair
C. Eating Habits
1
.
Does your child have a special diet? Yes | √ No
If yes, please provide diet information:
2
.
Are there any foods that should not be served to your child? √ Yes | No
If yes, please list the food and the reason:
Some fruits like kiwi is unpleasant for her as she do not like it.
3
.
For infants, how is your child fed? (you may check more than one)
bottle | √ sippy cup | high chair | booster seat | others:
4
.
List your child’s favourite foods:
Cerelac
5
.
List your child’s least favourite foods:
milk
7
.
Is your child allowed snacks? Yes | √ No
If yes, what?
D. Sleeping Habits
1
.
Does your child have a regular bedtime schedule? √ Yes | No
If yes, please describe bedtime schedule:
Setting 10-30 minutes with child before separately making them sleep
Identify if any problem spot
2
.
What time does your child usually wake up in the morning?
6:30 am
3
.
What time does your child usually go to bed at night?
Time is 9 pm.
4
.
Does your child take naps? √ Yes | No
If yes, when and how long does your child usually nap?
Usually 2 hours in day and 8 hours from night.
5
.
Does your child have any problems getting to sleep or staying asleep? Yes | √
No
If yes, please explain:
TEMPLATES BY:

Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
TEMPLATES BY:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
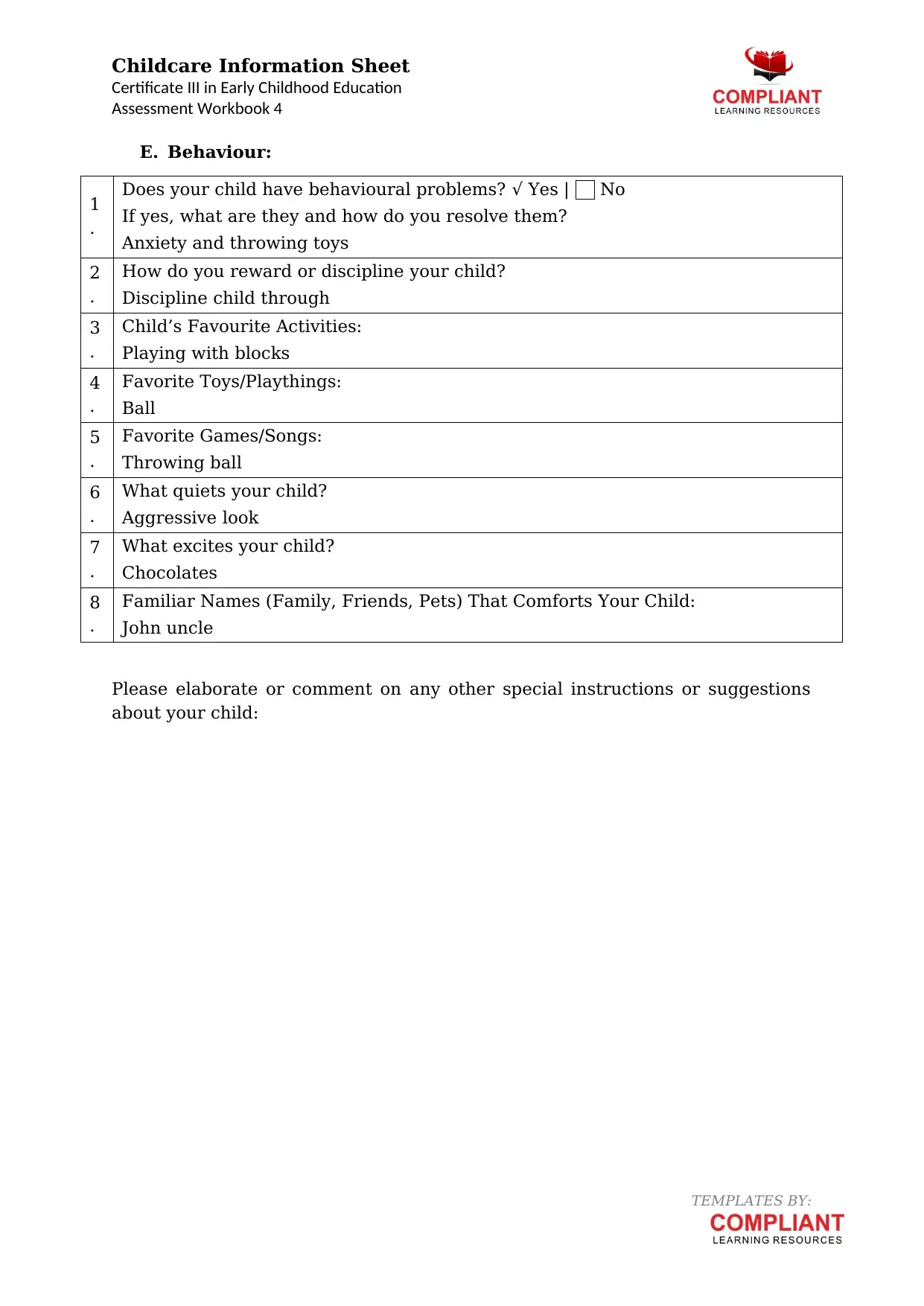
E. Behaviour:
1
.
Does your child have behavioural problems? √ Yes | No
If yes, what are they and how do you resolve them?
Anxiety and throwing toys
2
.
How do you reward or discipline your child?
Discipline child through
3
.
Child’s Favourite Activities:
Playing with blocks
4
.
Favorite Toys/Playthings:
Ball
5
.
Favorite Games/Songs:
Throwing ball
6
.
What quiets your child?
Aggressive look
7
.
What excites your child?
Chocolates
8
.
Familiar Names (Family, Friends, Pets) That Comforts Your Child:
John uncle
Please elaborate or comment on any other special instructions or suggestions
about your child:
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
E. Behaviour:
1
.
Does your child have behavioural problems? √ Yes | No
If yes, what are they and how do you resolve them?
Anxiety and throwing toys
2
.
How do you reward or discipline your child?
Discipline child through
3
.
Child’s Favourite Activities:
Playing with blocks
4
.
Favorite Toys/Playthings:
Ball
5
.
Favorite Games/Songs:
Throwing ball
6
.
What quiets your child?
Aggressive look
7
.
What excites your child?
Chocolates
8
.
Familiar Names (Family, Friends, Pets) That Comforts Your Child:
John uncle
Please elaborate or comment on any other special instructions or suggestions
about your child:
TEMPLATES BY:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
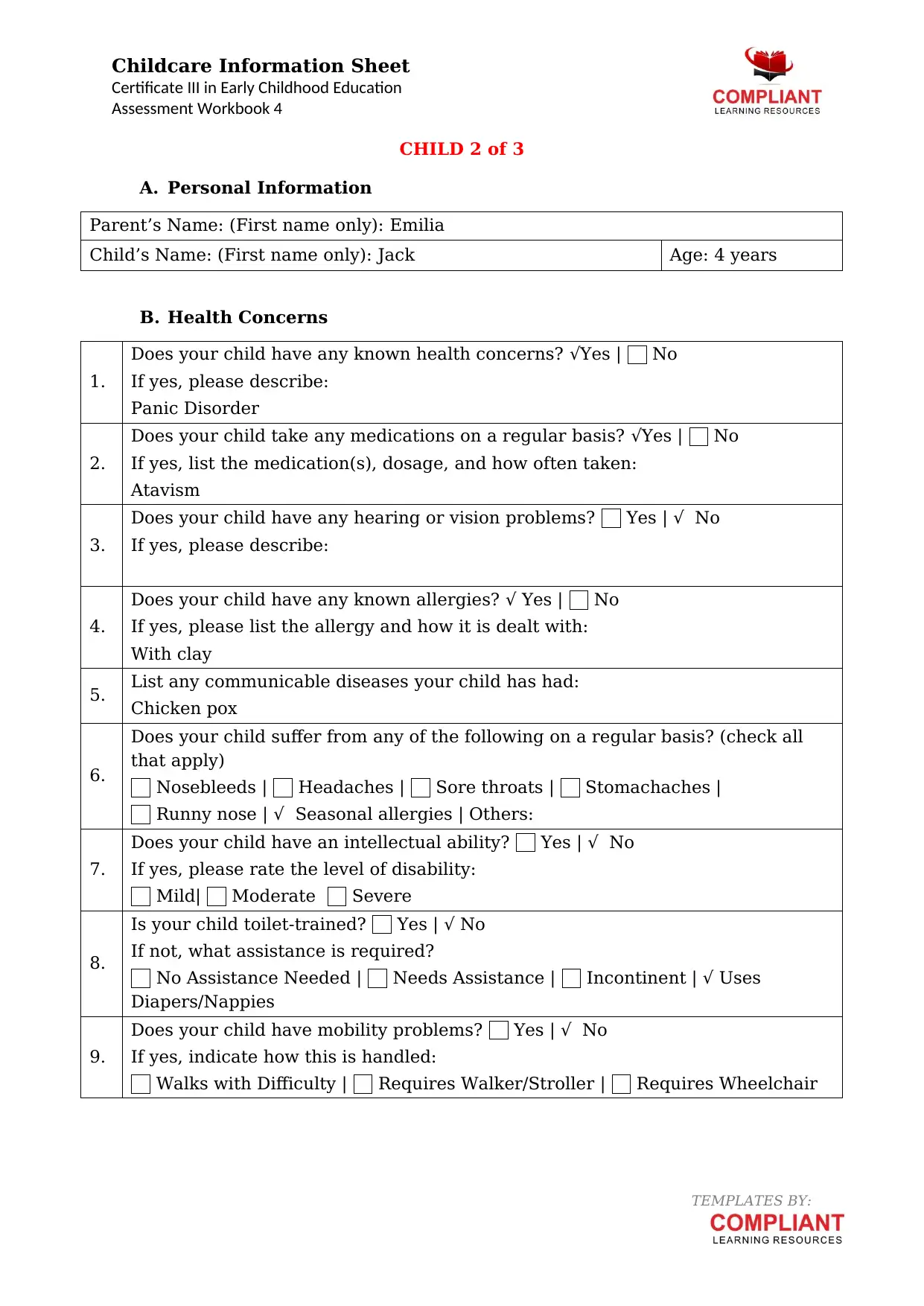
CHILD 2 of 3
A. Personal Information
Parent’s Name: (First name only): Emilia
Child’s Name: (First name only): Jack Age: 4 years
B. Health Concerns
1.
Does your child have any known health concerns? √Yes | No
If yes, please describe:
Panic Disorder
2.
Does your child take any medications on a regular basis? √Yes | No
If yes, list the medication(s), dosage, and how often taken:
Atavism
3.
Does your child have any hearing or vision problems? Yes | √ No
If yes, please describe:
4.
Does your child have any known allergies? √ Yes | No
If yes, please list the allergy and how it is dealt with:
With clay
5. List any communicable diseases your child has had:
Chicken pox
6.
Does your child suffer from any of the following on a regular basis? (check all
that apply)
Nosebleeds | Headaches | Sore throats | Stomachaches |
Runny nose | √ Seasonal allergies | Others:
7.
Does your child have an intellectual ability? Yes | √ No
If yes, please rate the level of disability:
Mild| Moderate Severe
8.
Is your child toilet-trained? Yes | √ No
If not, what assistance is required?
No Assistance Needed | Needs Assistance | Incontinent | √ Uses
Diapers/Nappies
9.
Does your child have mobility problems? Yes | √ No
If yes, indicate how this is handled:
Walks with Difficulty | Requires Walker/Stroller | Requires Wheelchair
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
CHILD 2 of 3
A. Personal Information
Parent’s Name: (First name only): Emilia
Child’s Name: (First name only): Jack Age: 4 years
B. Health Concerns
1.
Does your child have any known health concerns? √Yes | No
If yes, please describe:
Panic Disorder
2.
Does your child take any medications on a regular basis? √Yes | No
If yes, list the medication(s), dosage, and how often taken:
Atavism
3.
Does your child have any hearing or vision problems? Yes | √ No
If yes, please describe:
4.
Does your child have any known allergies? √ Yes | No
If yes, please list the allergy and how it is dealt with:
With clay
5. List any communicable diseases your child has had:
Chicken pox
6.
Does your child suffer from any of the following on a regular basis? (check all
that apply)
Nosebleeds | Headaches | Sore throats | Stomachaches |
Runny nose | √ Seasonal allergies | Others:
7.
Does your child have an intellectual ability? Yes | √ No
If yes, please rate the level of disability:
Mild| Moderate Severe
8.
Is your child toilet-trained? Yes | √ No
If not, what assistance is required?
No Assistance Needed | Needs Assistance | Incontinent | √ Uses
Diapers/Nappies
9.
Does your child have mobility problems? Yes | √ No
If yes, indicate how this is handled:
Walks with Difficulty | Requires Walker/Stroller | Requires Wheelchair
TEMPLATES BY:
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
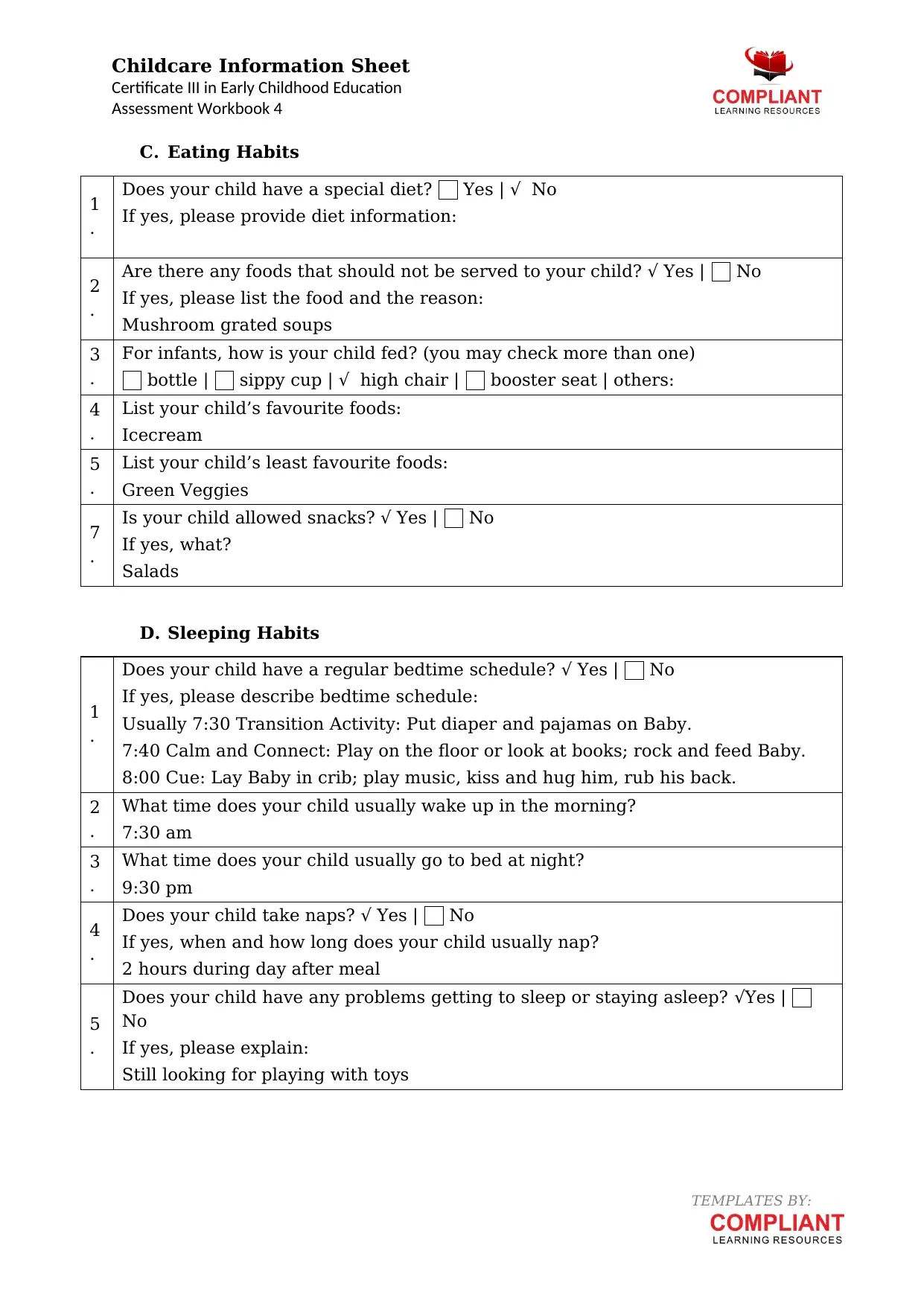
C. Eating Habits
1
.
Does your child have a special diet? Yes | √ No
If yes, please provide diet information:
2
.
Are there any foods that should not be served to your child? √ Yes | No
If yes, please list the food and the reason:
Mushroom grated soups
3
.
For infants, how is your child fed? (you may check more than one)
bottle | sippy cup | √ high chair | booster seat | others:
4
.
List your child’s favourite foods:
Icecream
5
.
List your child’s least favourite foods:
Green Veggies
7
.
Is your child allowed snacks? √ Yes | No
If yes, what?
Salads
D. Sleeping Habits
1
.
Does your child have a regular bedtime schedule? √ Yes | No
If yes, please describe bedtime schedule:
Usually 7:30 Transition Activity: Put diaper and pajamas on Baby.
7:40 Calm and Connect: Play on the floor or look at books; rock and feed Baby.
8:00 Cue: Lay Baby in crib; play music, kiss and hug him, rub his back.
2
.
What time does your child usually wake up in the morning?
7:30 am
3
.
What time does your child usually go to bed at night?
9:30 pm
4
.
Does your child take naps? √ Yes | No
If yes, when and how long does your child usually nap?
2 hours during day after meal
5
.
Does your child have any problems getting to sleep or staying asleep? √Yes |
No
If yes, please explain:
Still looking for playing with toys
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
C. Eating Habits
1
.
Does your child have a special diet? Yes | √ No
If yes, please provide diet information:
2
.
Are there any foods that should not be served to your child? √ Yes | No
If yes, please list the food and the reason:
Mushroom grated soups
3
.
For infants, how is your child fed? (you may check more than one)
bottle | sippy cup | √ high chair | booster seat | others:
4
.
List your child’s favourite foods:
Icecream
5
.
List your child’s least favourite foods:
Green Veggies
7
.
Is your child allowed snacks? √ Yes | No
If yes, what?
Salads
D. Sleeping Habits
1
.
Does your child have a regular bedtime schedule? √ Yes | No
If yes, please describe bedtime schedule:
Usually 7:30 Transition Activity: Put diaper and pajamas on Baby.
7:40 Calm and Connect: Play on the floor or look at books; rock and feed Baby.
8:00 Cue: Lay Baby in crib; play music, kiss and hug him, rub his back.
2
.
What time does your child usually wake up in the morning?
7:30 am
3
.
What time does your child usually go to bed at night?
9:30 pm
4
.
Does your child take naps? √ Yes | No
If yes, when and how long does your child usually nap?
2 hours during day after meal
5
.
Does your child have any problems getting to sleep or staying asleep? √Yes |
No
If yes, please explain:
Still looking for playing with toys
TEMPLATES BY:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
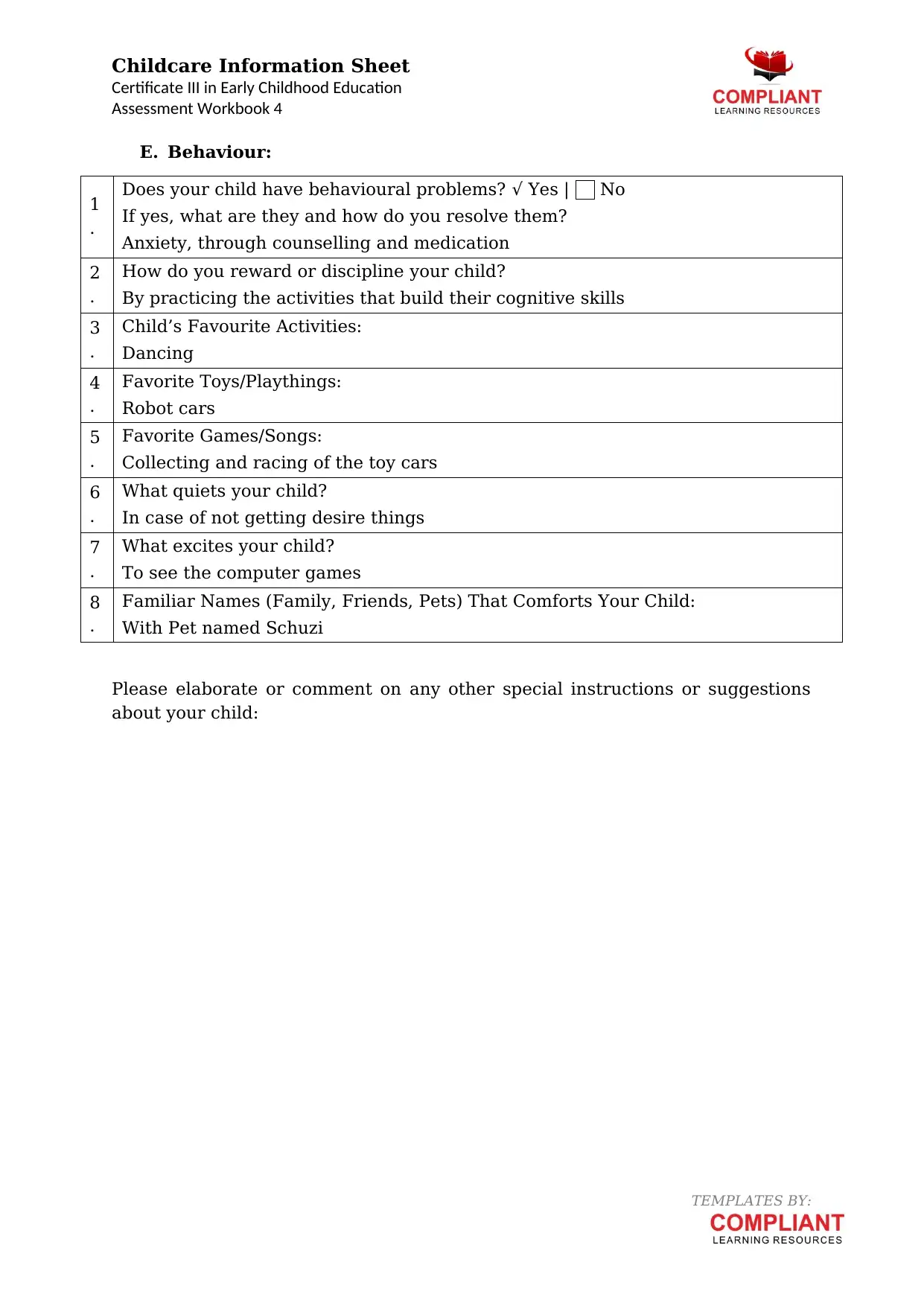
E. Behaviour:
1
.
Does your child have behavioural problems? √ Yes | No
If yes, what are they and how do you resolve them?
Anxiety, through counselling and medication
2
.
How do you reward or discipline your child?
By practicing the activities that build their cognitive skills
3
.
Child’s Favourite Activities:
Dancing
4
.
Favorite Toys/Playthings:
Robot cars
5
.
Favorite Games/Songs:
Collecting and racing of the toy cars
6
.
What quiets your child?
In case of not getting desire things
7
.
What excites your child?
To see the computer games
8
.
Familiar Names (Family, Friends, Pets) That Comforts Your Child:
With Pet named Schuzi
Please elaborate or comment on any other special instructions or suggestions
about your child:
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
E. Behaviour:
1
.
Does your child have behavioural problems? √ Yes | No
If yes, what are they and how do you resolve them?
Anxiety, through counselling and medication
2
.
How do you reward or discipline your child?
By practicing the activities that build their cognitive skills
3
.
Child’s Favourite Activities:
Dancing
4
.
Favorite Toys/Playthings:
Robot cars
5
.
Favorite Games/Songs:
Collecting and racing of the toy cars
6
.
What quiets your child?
In case of not getting desire things
7
.
What excites your child?
To see the computer games
8
.
Familiar Names (Family, Friends, Pets) That Comforts Your Child:
With Pet named Schuzi
Please elaborate or comment on any other special instructions or suggestions
about your child:
TEMPLATES BY:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
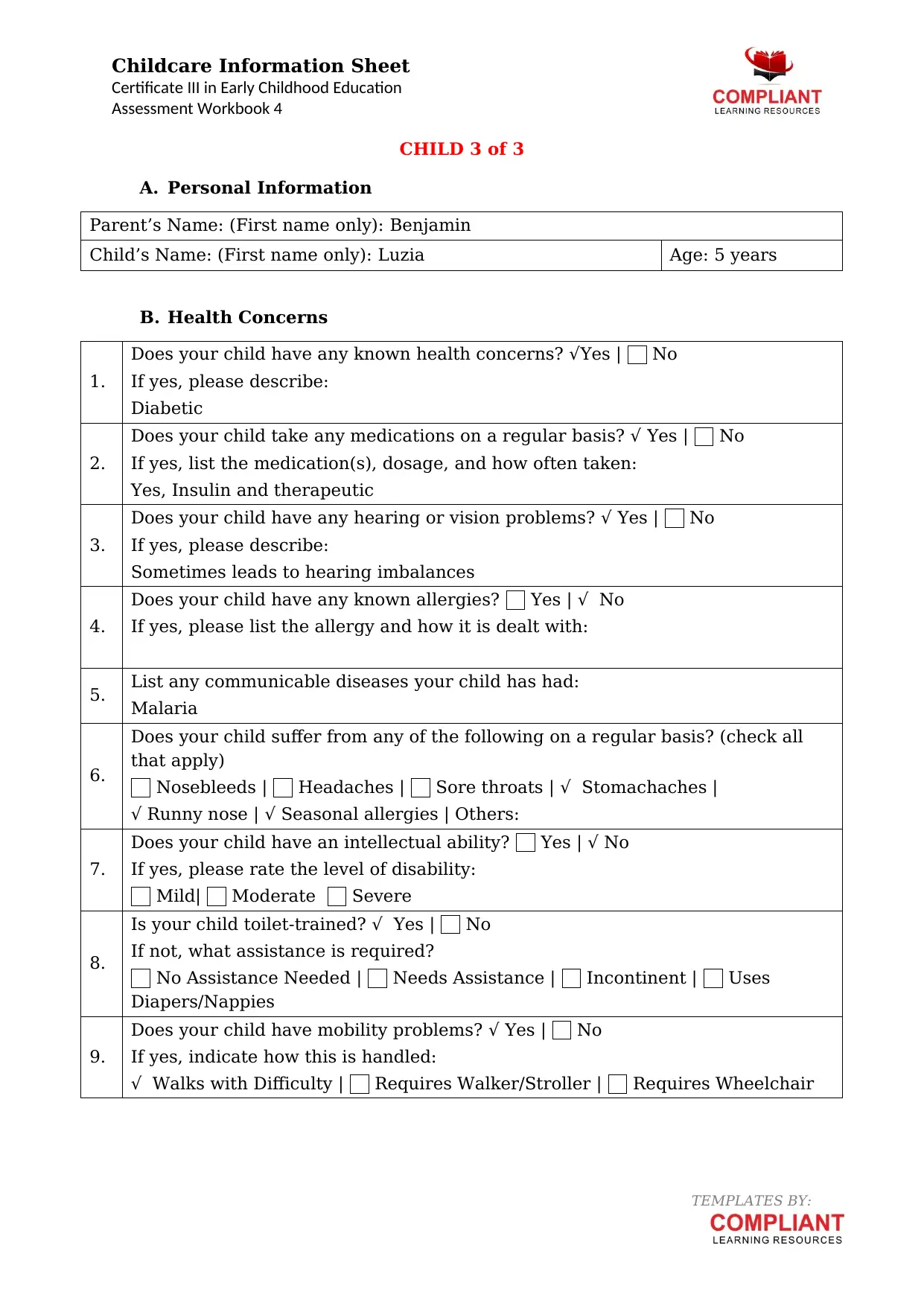
CHILD 3 of 3
A. Personal Information
Parent’s Name: (First name only): Benjamin
Child’s Name: (First name only): Luzia Age: 5 years
B. Health Concerns
1.
Does your child have any known health concerns? √Yes | No
If yes, please describe:
Diabetic
2.
Does your child take any medications on a regular basis? √ Yes | No
If yes, list the medication(s), dosage, and how often taken:
Yes, Insulin and therapeutic
3.
Does your child have any hearing or vision problems? √ Yes | No
If yes, please describe:
Sometimes leads to hearing imbalances
4.
Does your child have any known allergies? Yes | √ No
If yes, please list the allergy and how it is dealt with:
5. List any communicable diseases your child has had:
Malaria
6.
Does your child suffer from any of the following on a regular basis? (check all
that apply)
Nosebleeds | Headaches | Sore throats | √ Stomachaches |
√ Runny nose | √ Seasonal allergies | Others:
7.
Does your child have an intellectual ability? Yes | √ No
If yes, please rate the level of disability:
Mild| Moderate Severe
8.
Is your child toilet-trained? √ Yes | No
If not, what assistance is required?
No Assistance Needed | Needs Assistance | Incontinent | Uses
Diapers/Nappies
9.
Does your child have mobility problems? √ Yes | No
If yes, indicate how this is handled:
√ Walks with Difficulty | Requires Walker/Stroller | Requires Wheelchair
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
CHILD 3 of 3
A. Personal Information
Parent’s Name: (First name only): Benjamin
Child’s Name: (First name only): Luzia Age: 5 years
B. Health Concerns
1.
Does your child have any known health concerns? √Yes | No
If yes, please describe:
Diabetic
2.
Does your child take any medications on a regular basis? √ Yes | No
If yes, list the medication(s), dosage, and how often taken:
Yes, Insulin and therapeutic
3.
Does your child have any hearing or vision problems? √ Yes | No
If yes, please describe:
Sometimes leads to hearing imbalances
4.
Does your child have any known allergies? Yes | √ No
If yes, please list the allergy and how it is dealt with:
5. List any communicable diseases your child has had:
Malaria
6.
Does your child suffer from any of the following on a regular basis? (check all
that apply)
Nosebleeds | Headaches | Sore throats | √ Stomachaches |
√ Runny nose | √ Seasonal allergies | Others:
7.
Does your child have an intellectual ability? Yes | √ No
If yes, please rate the level of disability:
Mild| Moderate Severe
8.
Is your child toilet-trained? √ Yes | No
If not, what assistance is required?
No Assistance Needed | Needs Assistance | Incontinent | Uses
Diapers/Nappies
9.
Does your child have mobility problems? √ Yes | No
If yes, indicate how this is handled:
√ Walks with Difficulty | Requires Walker/Stroller | Requires Wheelchair
TEMPLATES BY:
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
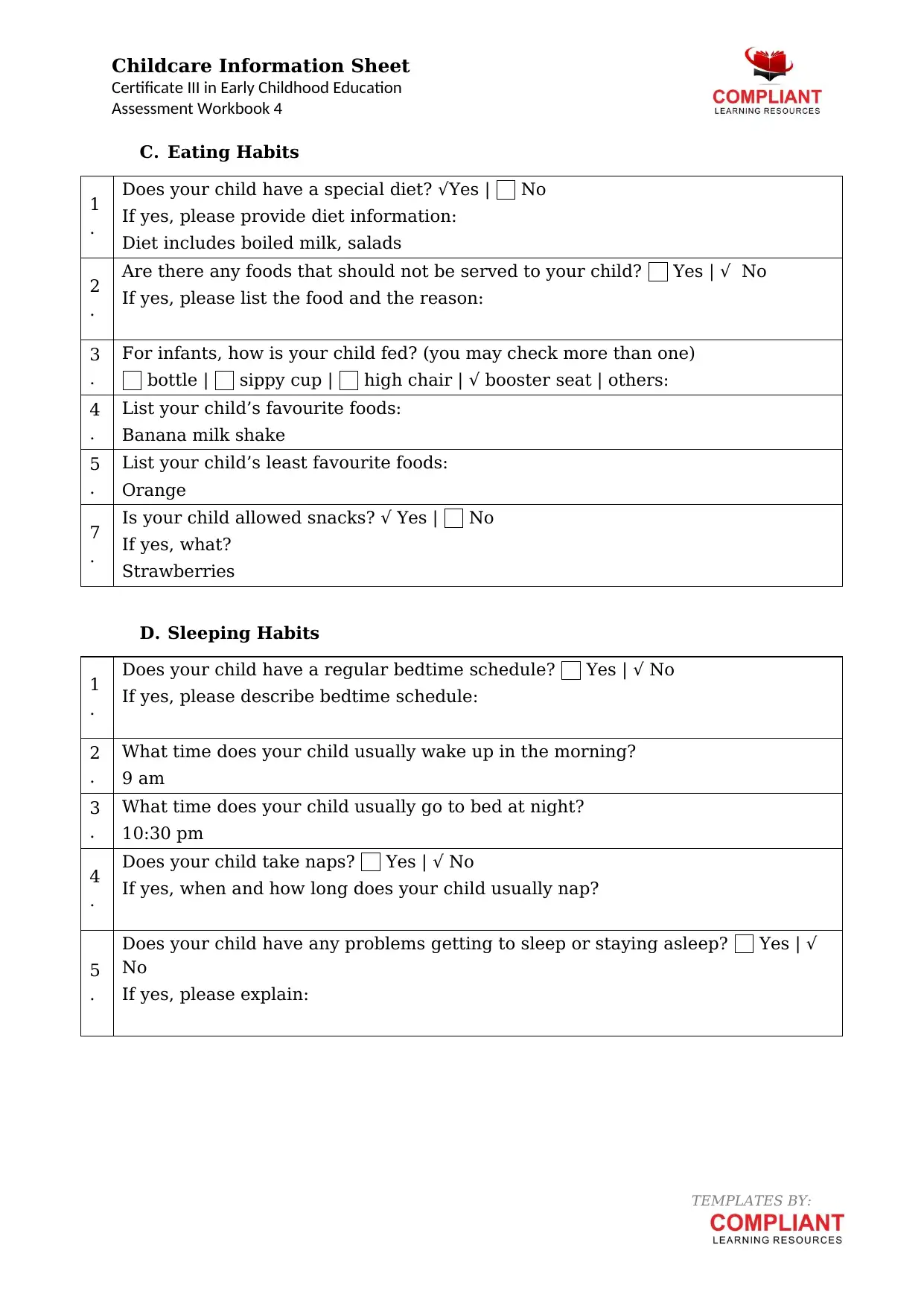
C. Eating Habits
1
.
Does your child have a special diet? √Yes | No
If yes, please provide diet information:
Diet includes boiled milk, salads
2
.
Are there any foods that should not be served to your child? Yes | √ No
If yes, please list the food and the reason:
3
.
For infants, how is your child fed? (you may check more than one)
bottle | sippy cup | high chair | √ booster seat | others:
4
.
List your child’s favourite foods:
Banana milk shake
5
.
List your child’s least favourite foods:
Orange
7
.
Is your child allowed snacks? √ Yes | No
If yes, what?
Strawberries
D. Sleeping Habits
1
.
Does your child have a regular bedtime schedule? Yes | √ No
If yes, please describe bedtime schedule:
2
.
What time does your child usually wake up in the morning?
9 am
3
.
What time does your child usually go to bed at night?
10:30 pm
4
.
Does your child take naps? Yes | √ No
If yes, when and how long does your child usually nap?
5
.
Does your child have any problems getting to sleep or staying asleep? Yes | √
No
If yes, please explain:
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
C. Eating Habits
1
.
Does your child have a special diet? √Yes | No
If yes, please provide diet information:
Diet includes boiled milk, salads
2
.
Are there any foods that should not be served to your child? Yes | √ No
If yes, please list the food and the reason:
3
.
For infants, how is your child fed? (you may check more than one)
bottle | sippy cup | high chair | √ booster seat | others:
4
.
List your child’s favourite foods:
Banana milk shake
5
.
List your child’s least favourite foods:
Orange
7
.
Is your child allowed snacks? √ Yes | No
If yes, what?
Strawberries
D. Sleeping Habits
1
.
Does your child have a regular bedtime schedule? Yes | √ No
If yes, please describe bedtime schedule:
2
.
What time does your child usually wake up in the morning?
9 am
3
.
What time does your child usually go to bed at night?
10:30 pm
4
.
Does your child take naps? Yes | √ No
If yes, when and how long does your child usually nap?
5
.
Does your child have any problems getting to sleep or staying asleep? Yes | √
No
If yes, please explain:
TEMPLATES BY:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Childcare Information Sheet
Certificate III in Early Childhood Education
Assessment Workbook 4
E. Behaviour:
1
.
Does your child have behavioural problems? Yes | √ No
If yes, what are they and how do you resolve them?
2
.
How do you reward or discipline your child?
Through positive discipline practices
3
.
Child’s Favourite Activities:
Watching TV
4
.
Favorite Toys/Playthings:
Doll
5
.
Favorite Games/Songs:
Playing House board
6
.
What quiets your child?
Loss of any toy
7
.
What excites your child?
Cartoons
8
.
Familiar Names (Family, Friends, Pets) That Comforts Your Child:
Cousin sister named Benjamin
Please elaborate or comment on any other special instructions or suggestions
about your child:
TEMPLATES BY:
Certificate III in Early Childhood Education
Assessment Workbook 4
E. Behaviour:
1
.
Does your child have behavioural problems? Yes | √ No
If yes, what are they and how do you resolve them?
2
.
How do you reward or discipline your child?
Through positive discipline practices
3
.
Child’s Favourite Activities:
Watching TV
4
.
Favorite Toys/Playthings:
Doll
5
.
Favorite Games/Songs:
Playing House board
6
.
What quiets your child?
Loss of any toy
7
.
What excites your child?
Cartoons
8
.
Familiar Names (Family, Friends, Pets) That Comforts Your Child:
Cousin sister named Benjamin
Please elaborate or comment on any other special instructions or suggestions
about your child:
TEMPLATES BY:
1 out of 10
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.