Childcare Information Sheet: Assessment Workbook 4 Details
VerifiedAdded on 2022/08/15
|9
|2168
|21
Homework Assignment
AI Summary
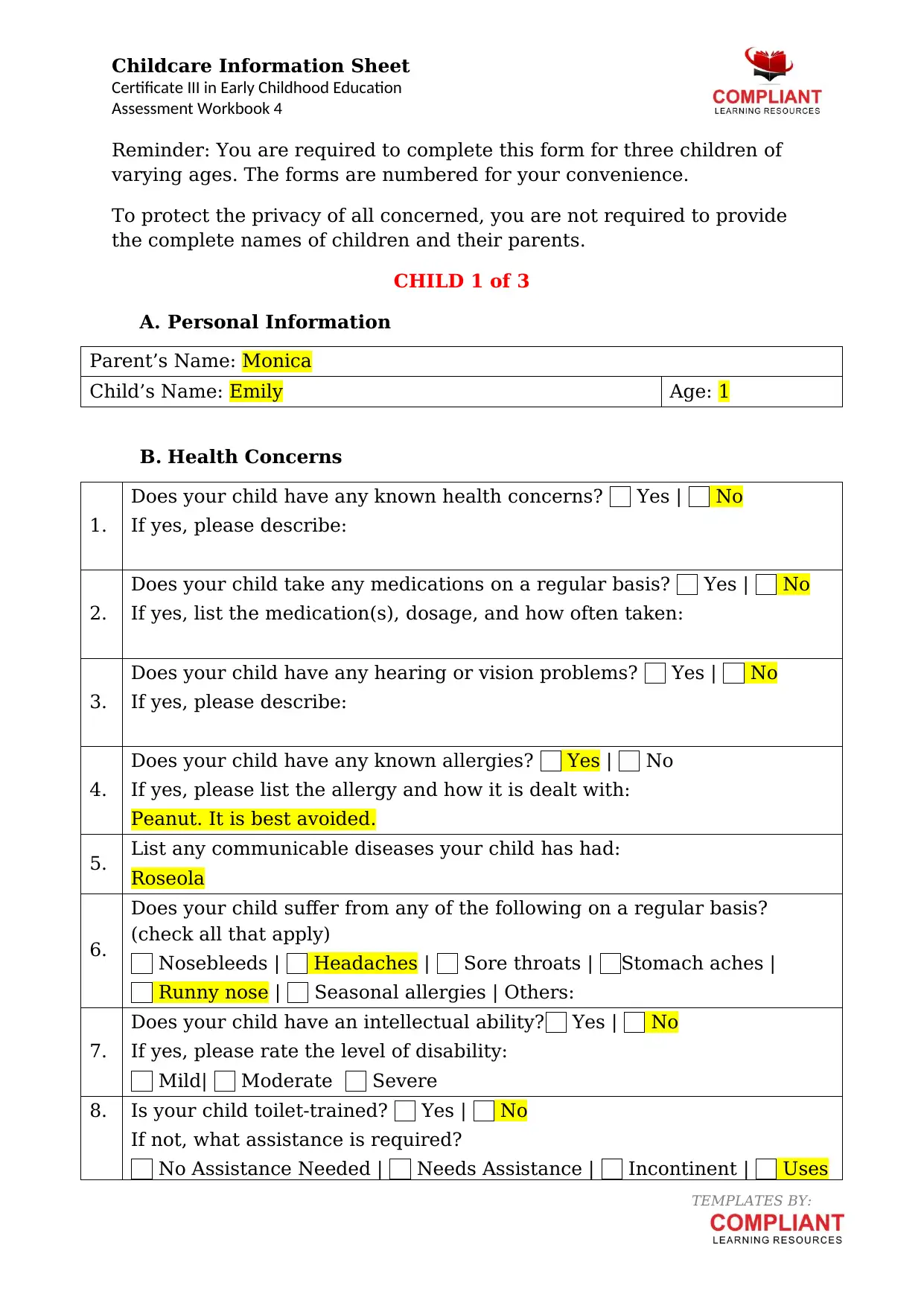
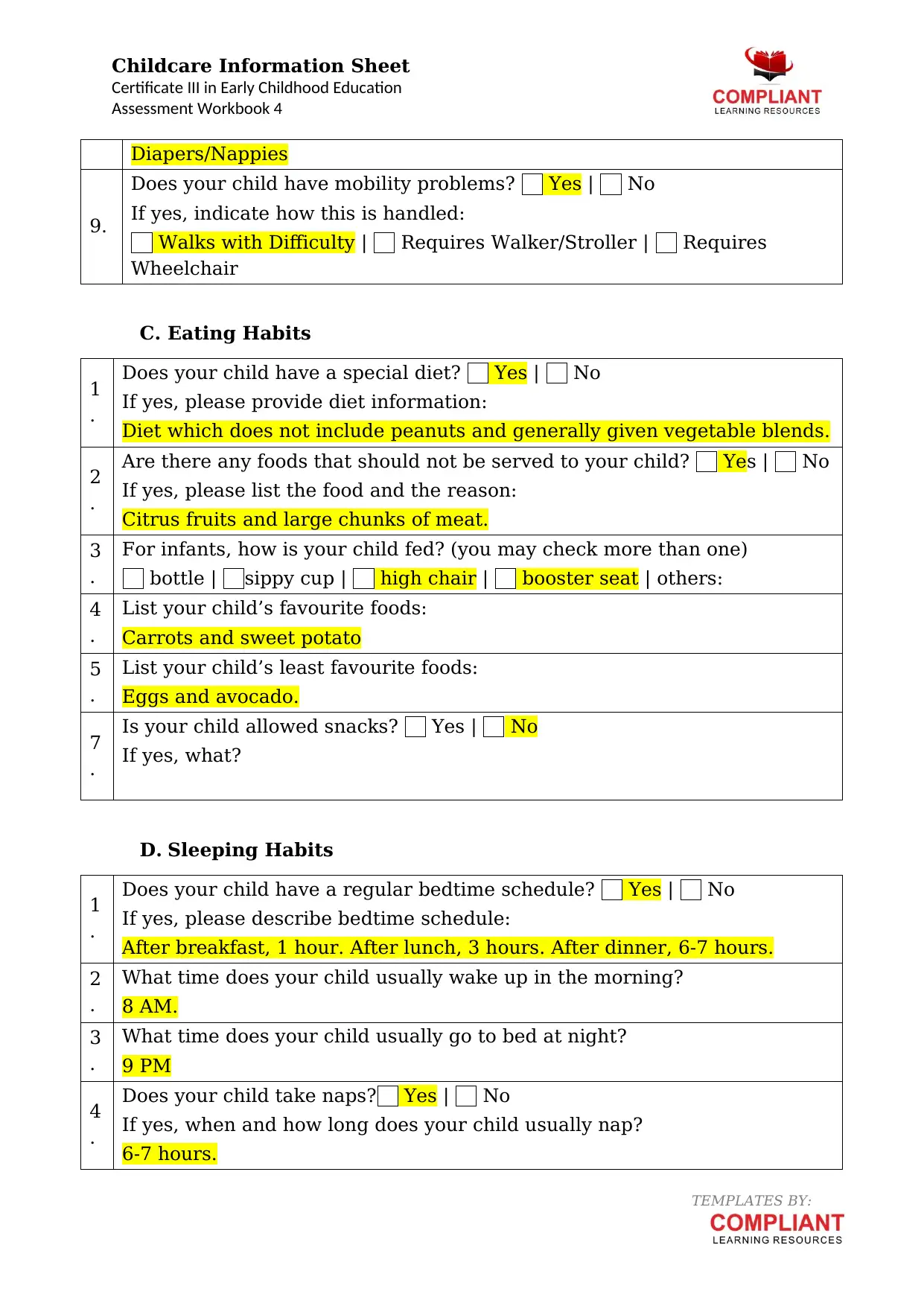
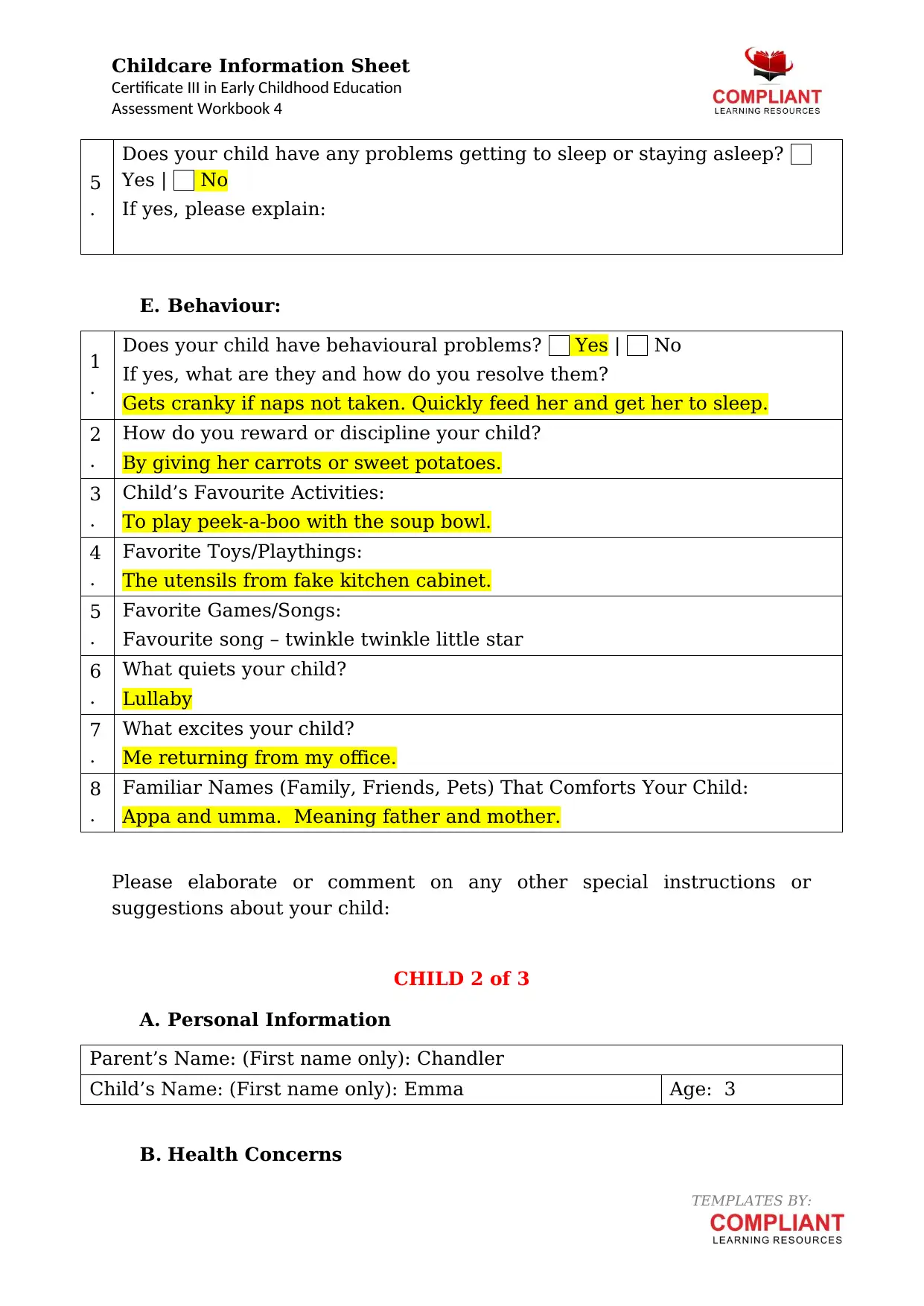
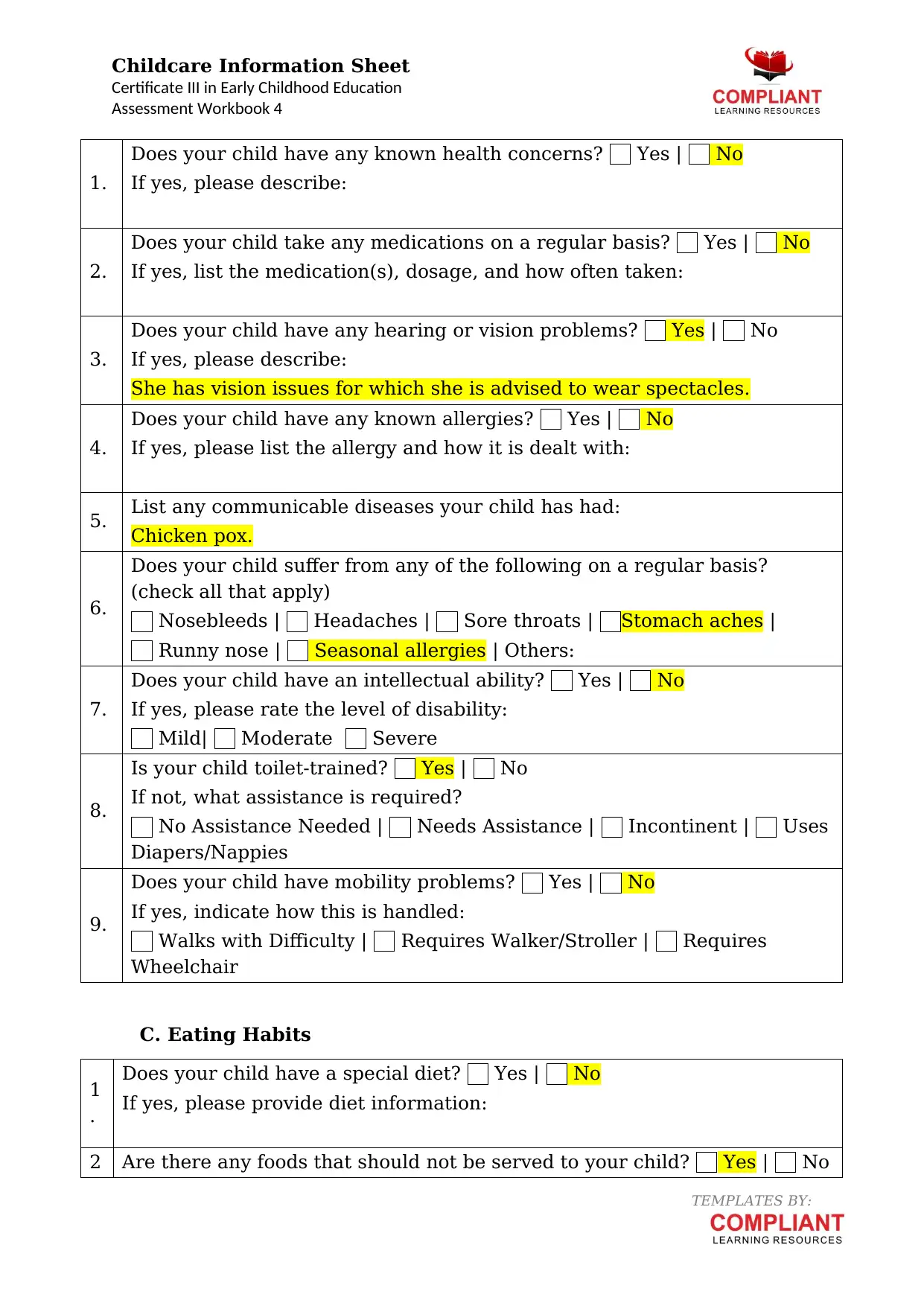
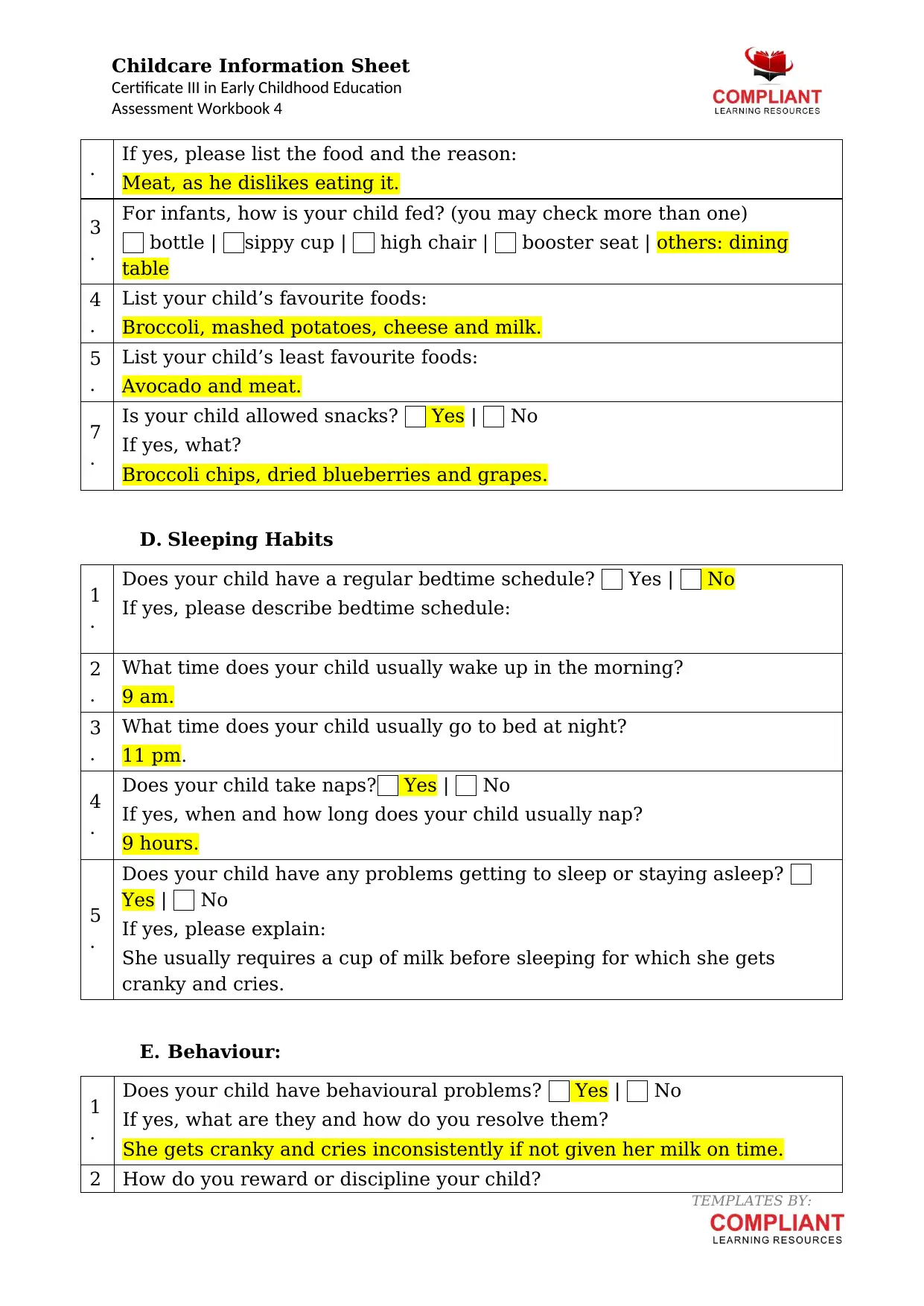
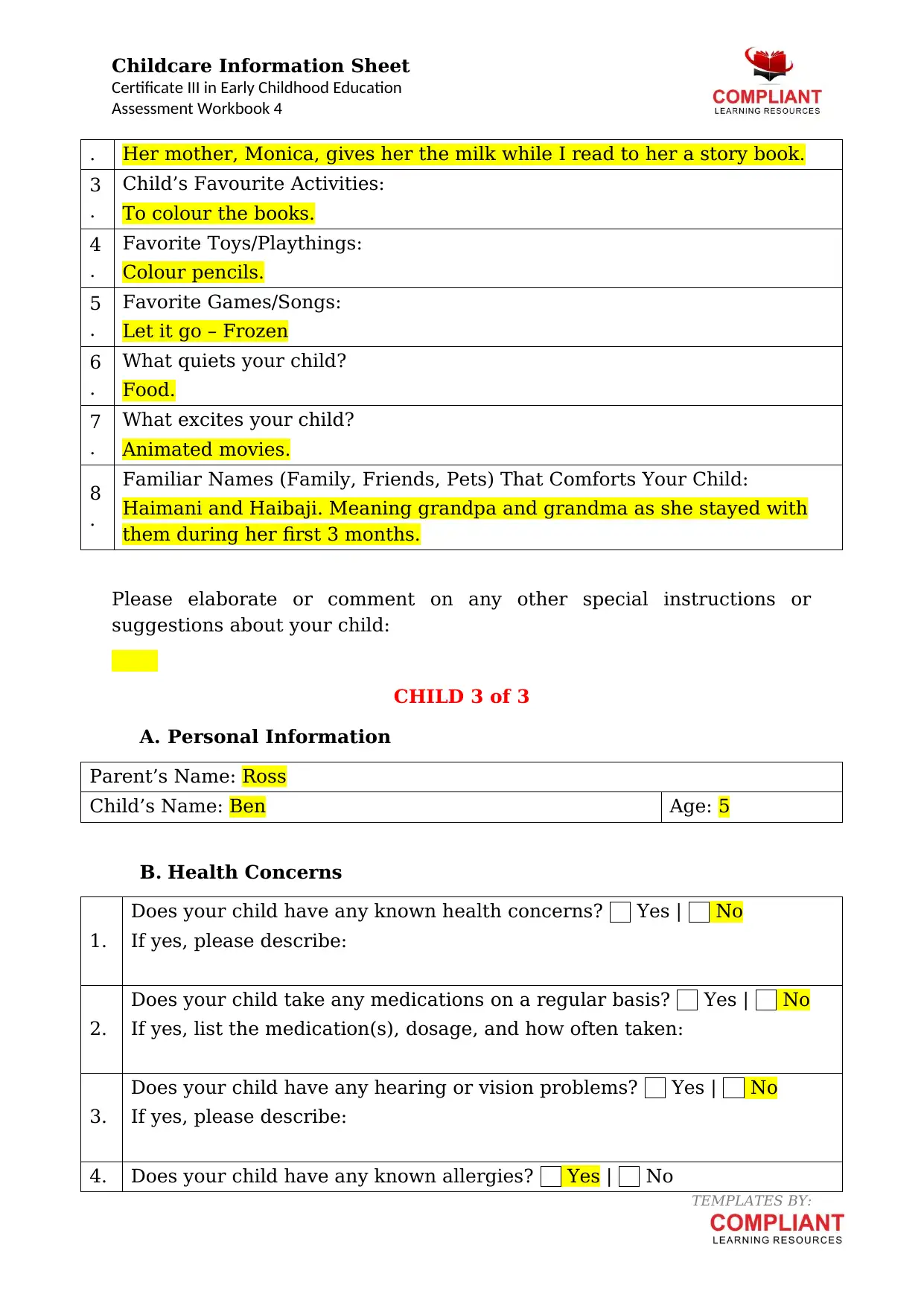
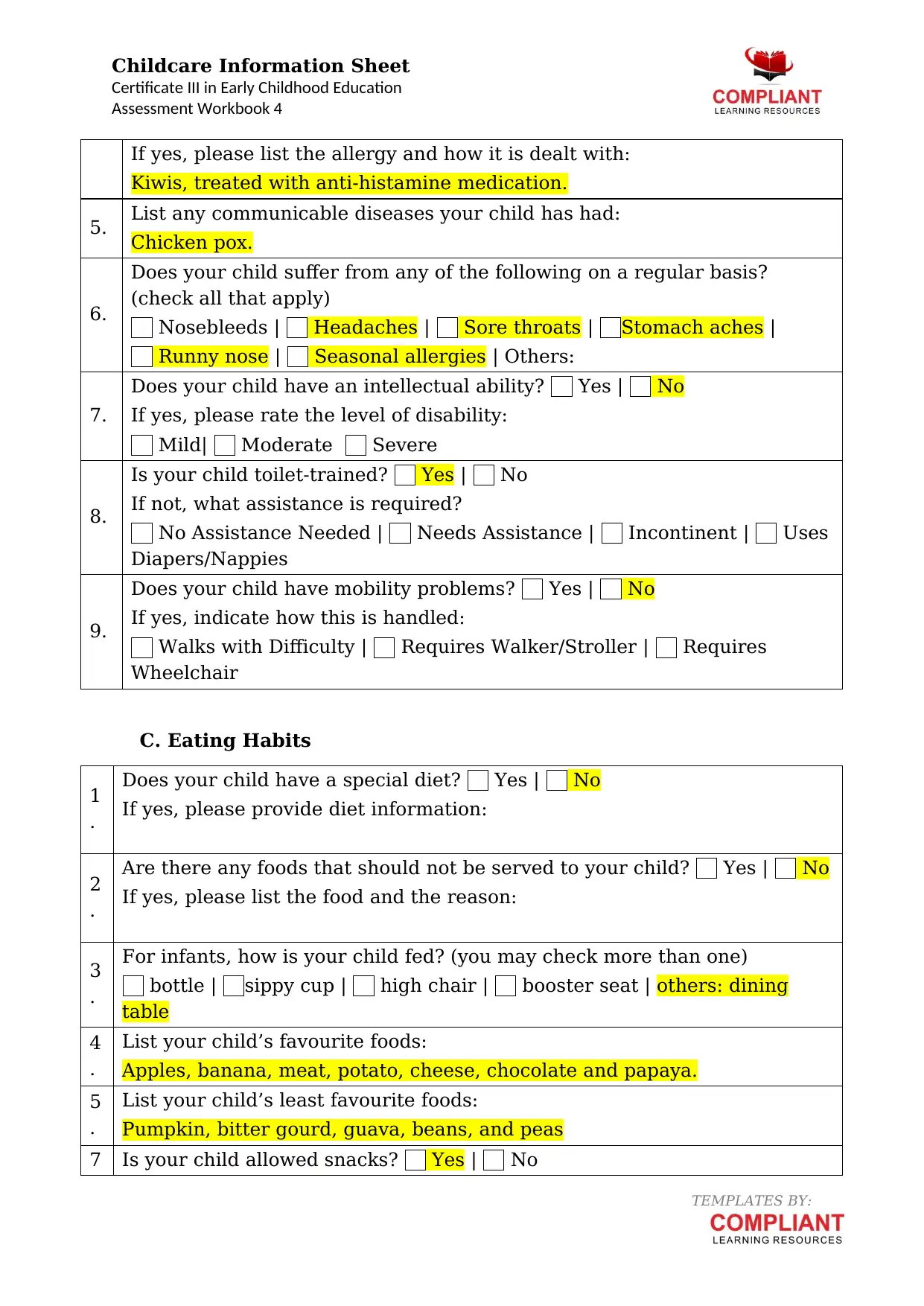
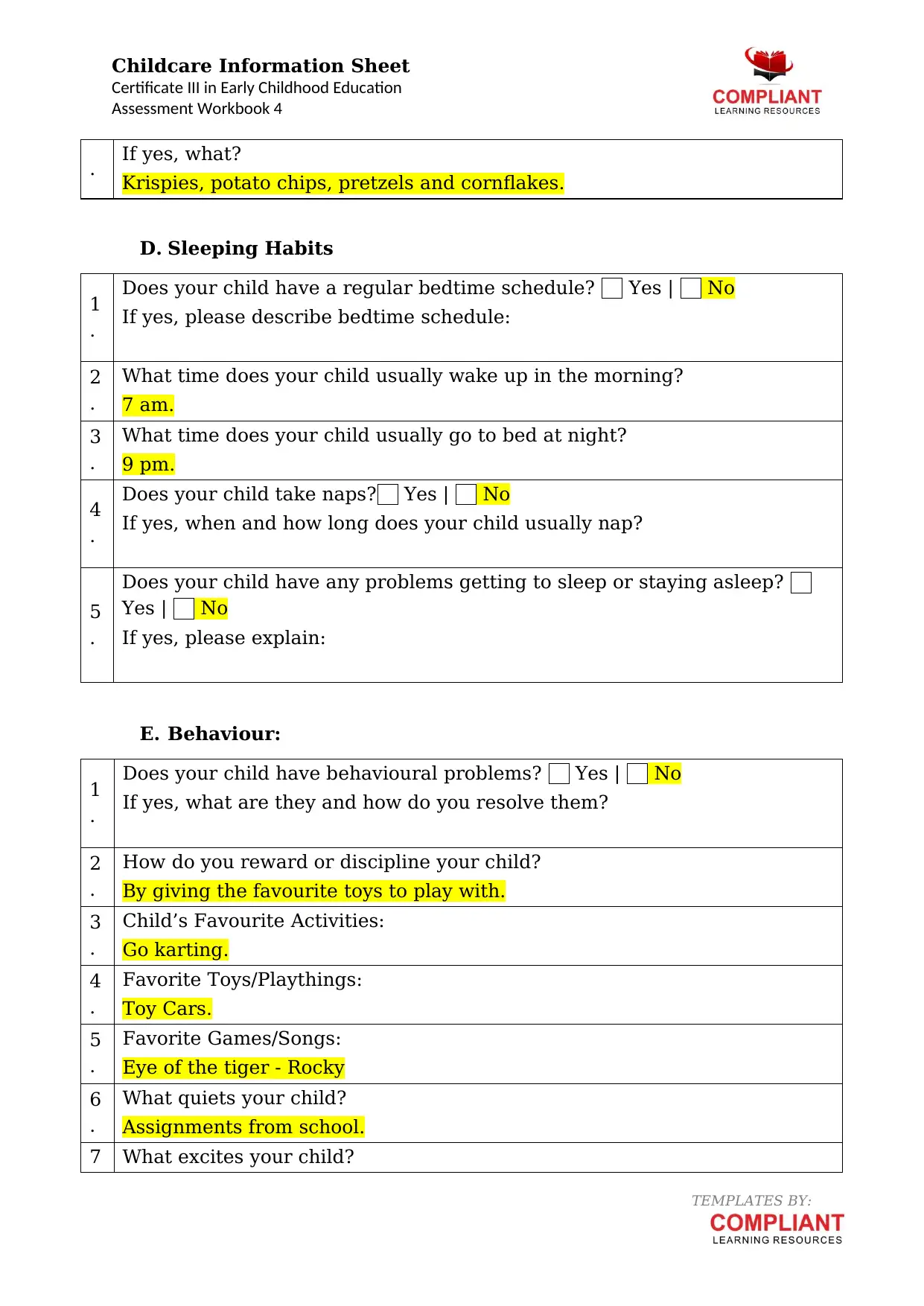
This assignment comprises three childcare information sheets, each detailing a different child's personal information, health concerns, eating habits, sleeping patterns, and behavioral characteristics. The sheets cover Emily, a child with peanut allergies and specific dietary needs; Emma, who has vision problems and a preference for specific foods and routines; and Ben, who has a kiwi allergy and enjoys go-karting. The information includes details about medications, allergies, favorite activities, and familiar names that comfort the children. This assignment is part of an assessment workbook for the Certificate III in Early Childhood Education and Care, providing a comprehensive overview of the children's individual needs and preferences, which is crucial for effective childcare practices.
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.