NURS2006: Enhancing Healthcare Through Effective Communication
VerifiedAdded on 2023/06/04
|8
|2029
|179
Report
AI Summary
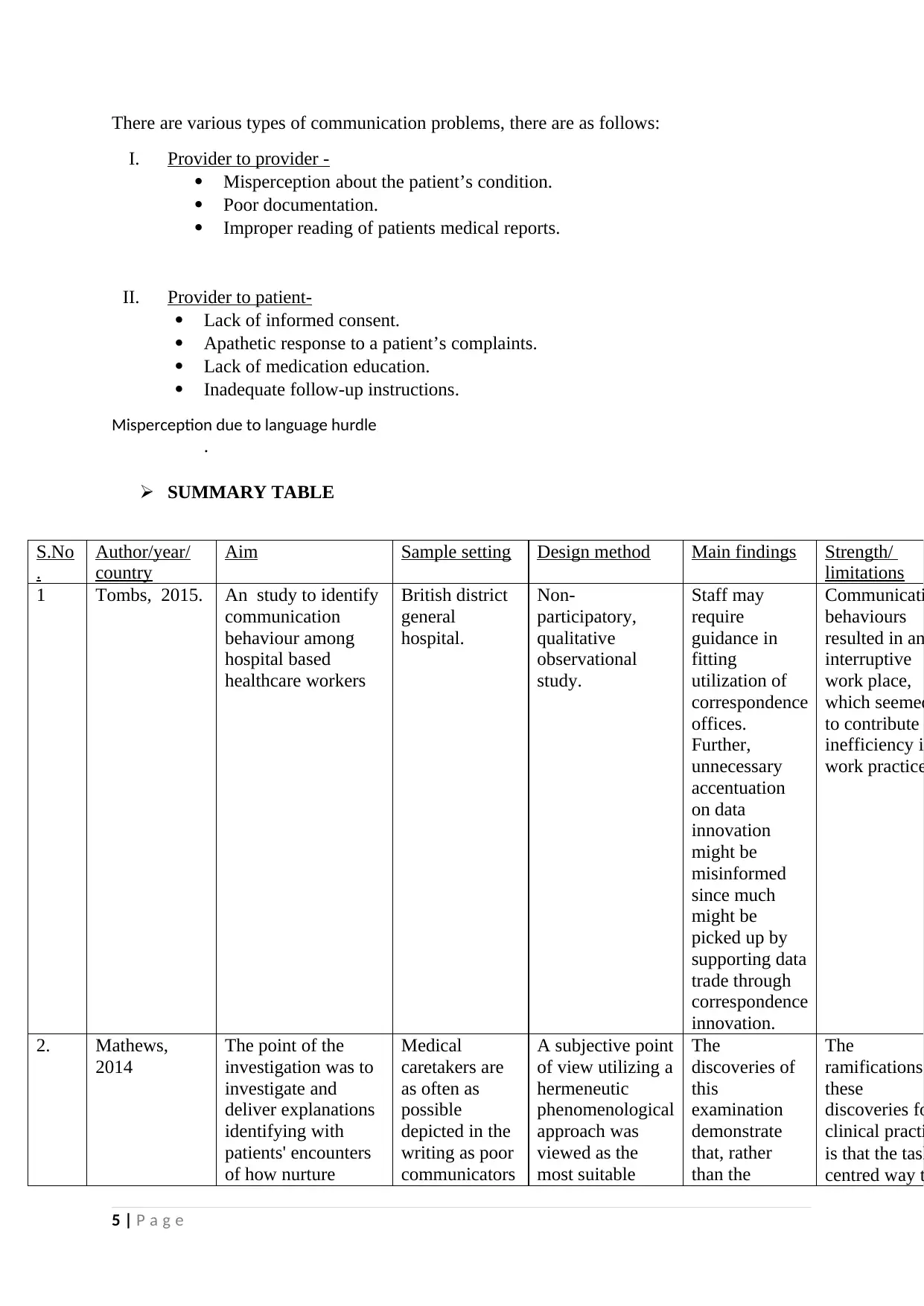
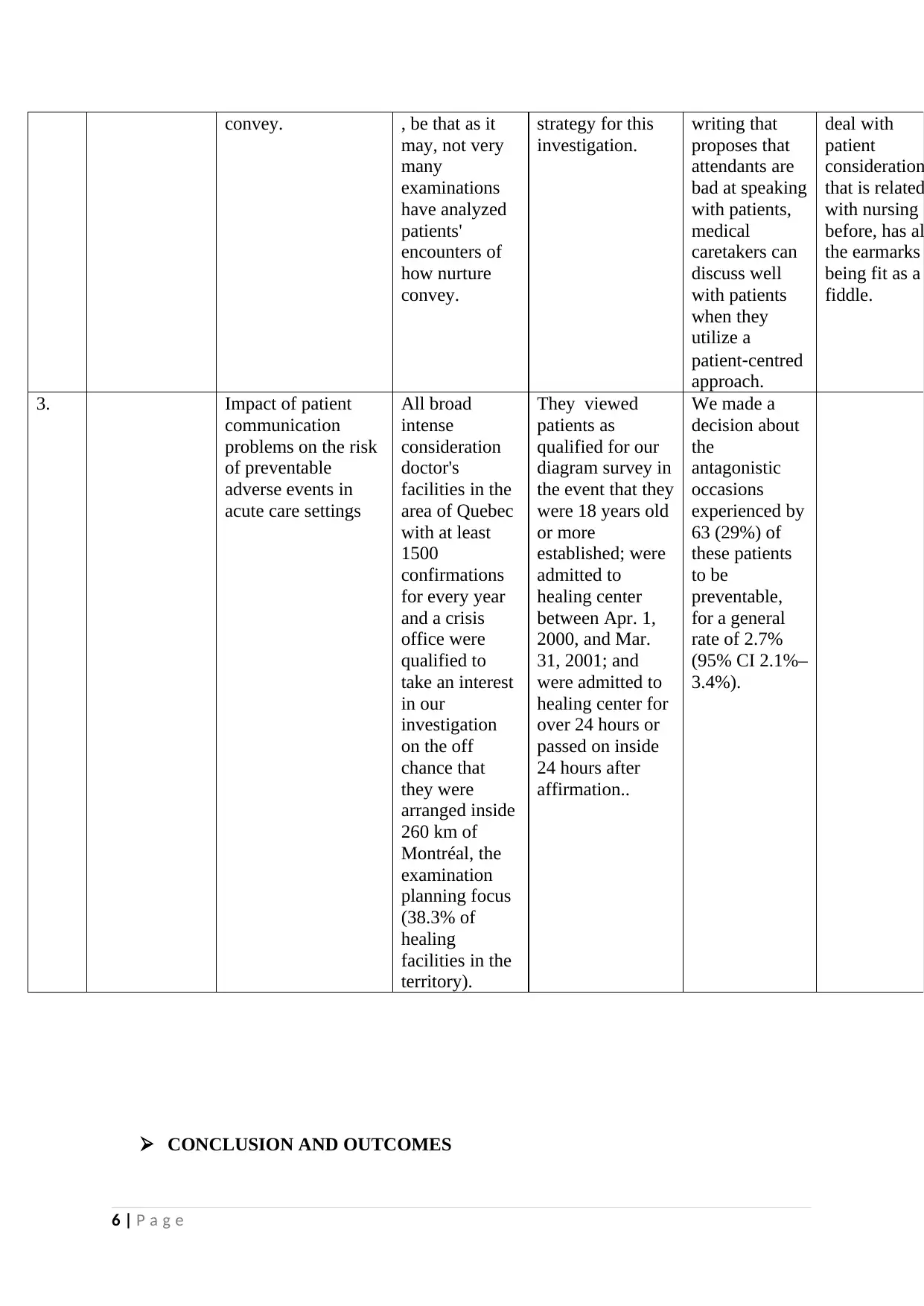
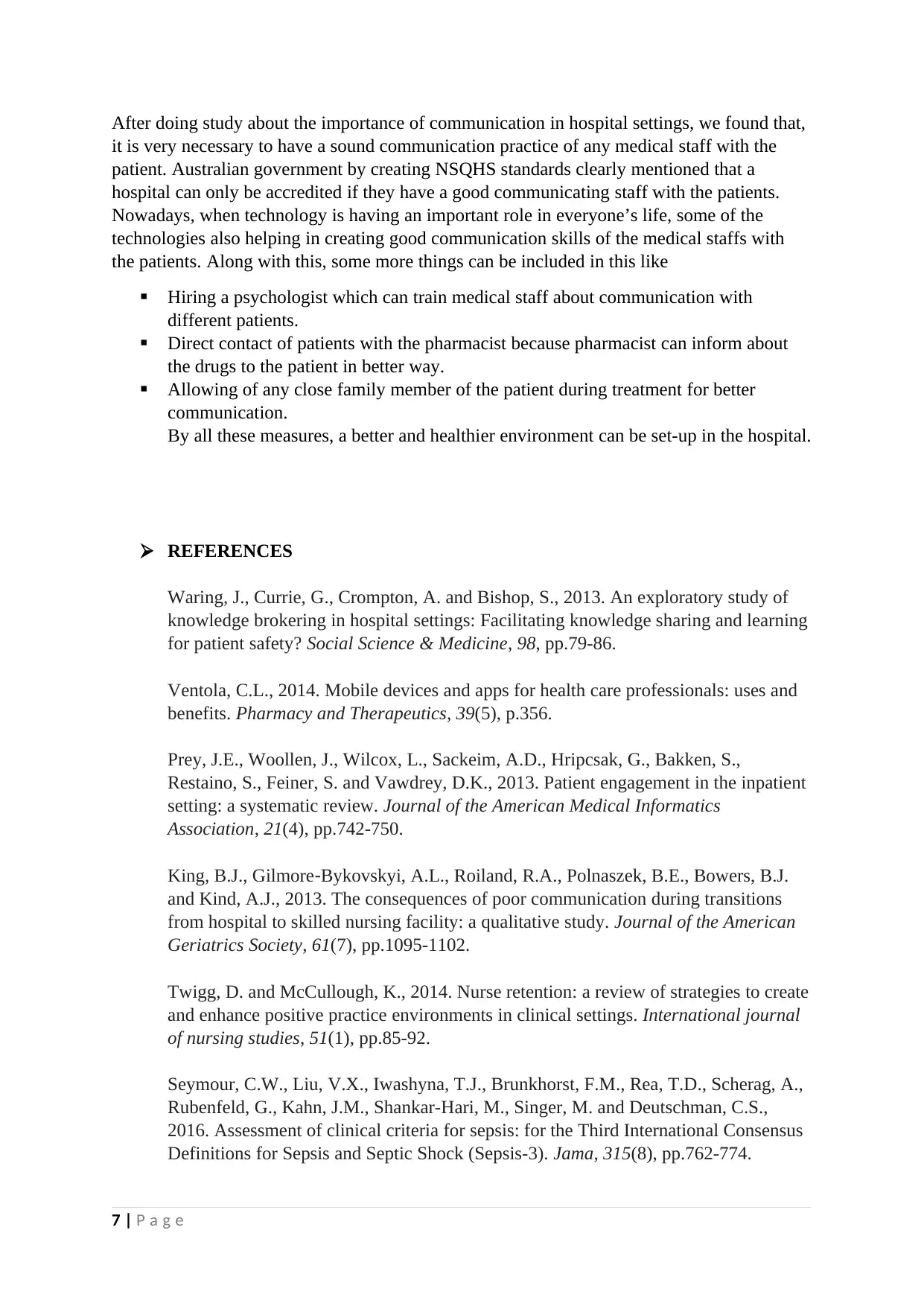
This report investigates the crucial role of clinical communication in healthcare settings, emphasizing its significance in fostering positive patient-doctor relationships, improving patient outcomes, and fulfilling the National Safety and Quality Health Service (NSQHS) Standards of Australia. It examines the importance of communication in various aspects of healthcare, including partnering with patients, ensuring medical safety, clinical handover, prevention of pressure injuries, and fall prevention. The report also addresses common communication problems, such as provider-to-provider and provider-to-patient issues, and explores reasons for improper communication, including misperceptions, poor documentation, lack of informed consent, and language barriers. Furthermore, it presents a summary table of relevant studies, highlighting their aims, methodologies, findings, strengths, and limitations. The report concludes by advocating for improved communication practices through measures like hiring psychologists for communication training, facilitating direct pharmacist-patient contact, and involving family members during treatment. Desklib offers a wealth of study resources, including past papers and solved assignments, to further support students in understanding and mastering this vital aspect of healthcare.
1 out of 8
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.