Clinical Reasoning Cycle: Case Study on Coronary Artery Disease
VerifiedAdded on 2022/12/15
|11
|1743
|165
Presentation
AI Summary
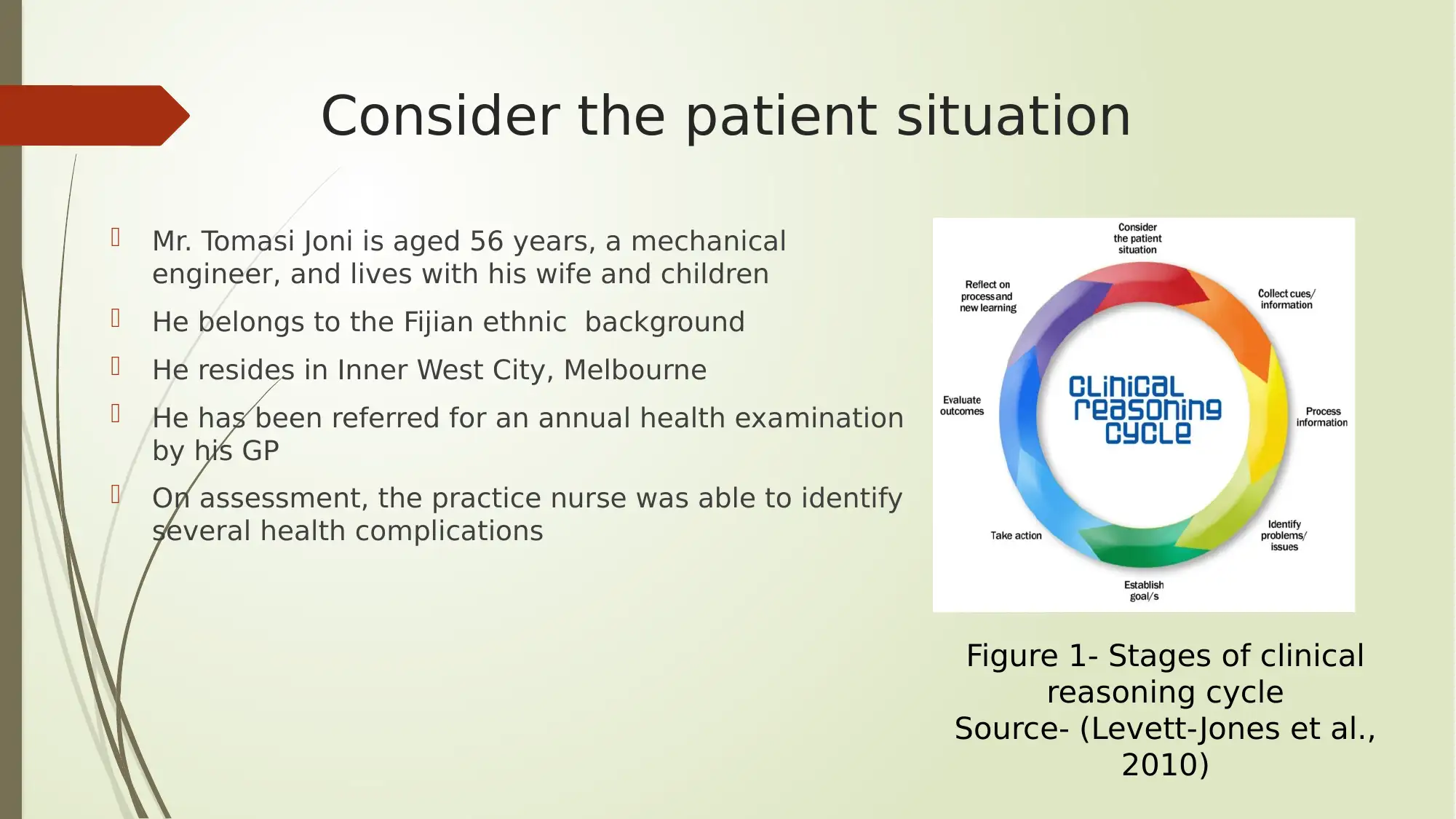
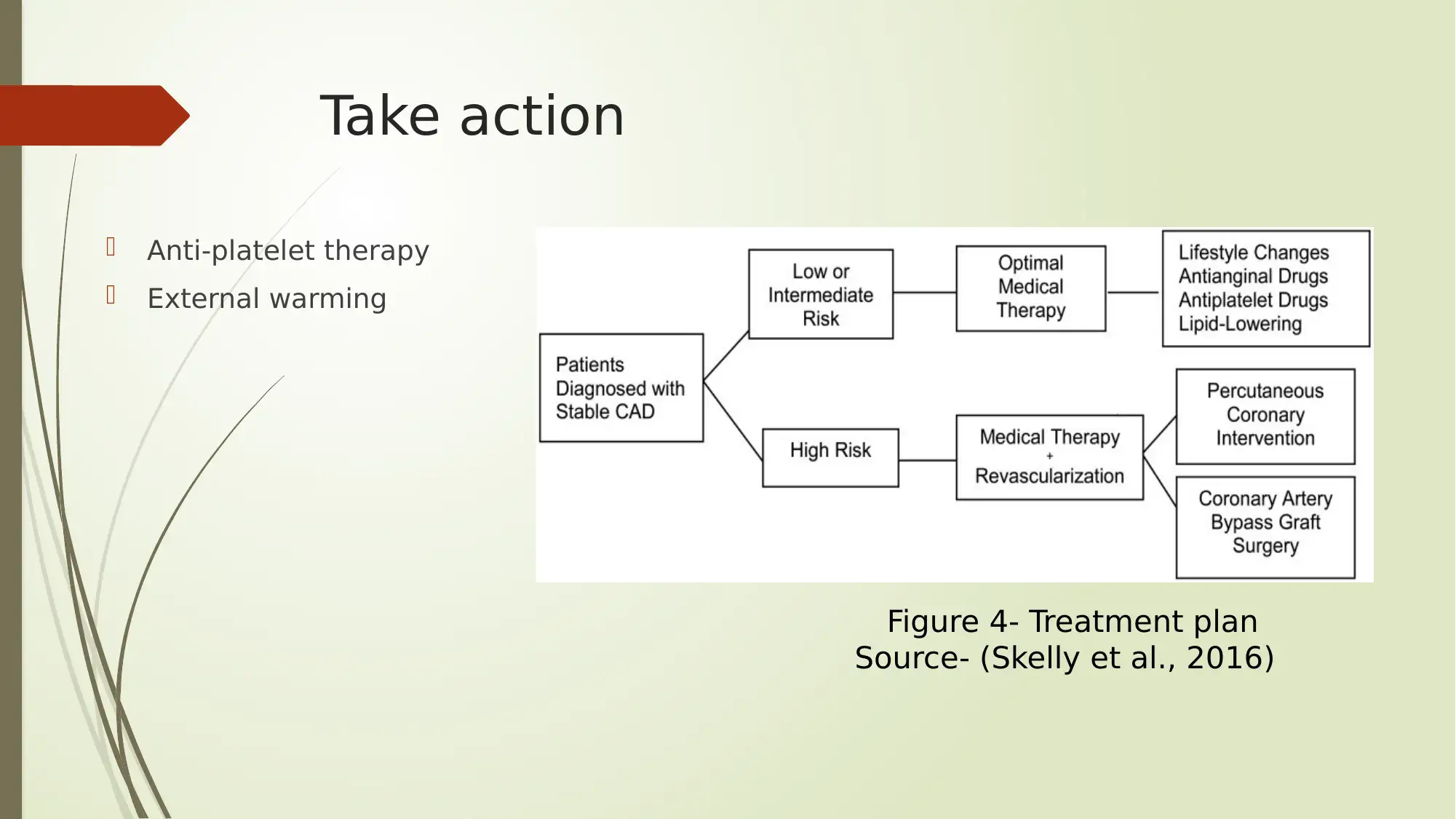
This presentation analyzes a case study of Mr. Tomasi Joni, a 56-year-old mechanical engineer with a history of hypertension, AMI, and other health complications. The presentation follows the clinical reasoning cycle to assess Mr. Joni's risk of developing coronary artery disease (CAD). It begins by considering the patient's situation, including his medical history, lifestyle, and current health indicators. The presentation then collects and processes information, identifying key cues such as elevated blood pressure, abnormal cholesterol levels, and other risk factors. The core of the presentation focuses on the pathophysiology of CAD, explaining the mechanisms of the disease and its clinical manifestations. Goals are established to restore balance between oxygen demand and supply and take action by administering medications and initiating lifestyle changes. The presentation concludes by discussing the outcomes of the nursing care plan and the importance of clinical reasoning in understanding and managing CAD. The presentation also includes references to support the discussed concepts.
1 out of 11
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.