SNPG962 Spring 2017: Clinical Reasoning and Asthma Management
VerifiedAdded on 2023/06/13
|17
|4460
|393
Report
AI Summary
This report provides a detailed analysis of the clinical reasoning cycle in the context of a 32-year-old asthma patient named Lucy. It begins by outlining the importance of clinical reasoning in nursing practice, emphasizing the collection of cues, processing of patient information, and formulation of effective care plans. The report then delves into a sequence of assessments, including gathering information about Lucy's background, vital signs, and medical history, with a focus on identifying potential risk factors and triggers for her asthma. Questions for patient assessment are proposed, highlighting the importance of patient-centered communication and understanding the patient's perspective. The analysis of findings correlates Lucy's symptoms with her family history, environmental factors, and vital sign abnormalities, leading to an evaluation of the results and conclusions regarding the patient's condition and potential management strategies. The report concludes by emphasizing the importance of genetic predisposition, environmental triggers, and documentation of subjective and objective data in formulating an appropriate diagnosis and providing optimal medical care.

Running head: CLINICAL JUDGEMENT AND REASONING
Assessment Task 2
Name of the Student
Name of the University
Author Note
Assessment Task 2
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CLINICAL JUDGEMENT AND REASONING
Clinical reasoning refers to the process by which healthcare professionals and nurses are
involved in collecting cues, processing patient information, and gaining a deeper understanding
of the situation or patient condition. This is generally followed by formulating an effective care
plan and implementing the decided interventions (Delany & Golding 2014, p.20). An evaluation
of the outcomes and reflection from the entire process helps in enhancing patient safety. This
assignment will discuss a clinical reasoning cycle, in relation to a case study of Lucy, a 32 year
old patient suffering from asthma.
Sequence of proposed assessment
The patient Lucy has been suffering from asthma since her childhood, and recently works
as a cleaner at a private aged care facility. Although daily inhalation of beclomethasone has
helped in reducing severity of her asthma conditions, she is currently facing several problems
that have led to the occurrence of respiratory distress and dyspnoea. With the aim of collecting
information about the patient and formulating an appropriate care plan, her context and situation
will be initially considered, followed by collecting information about all the vital cues, which in
turn will facilitate patient assessment. Gaining a deeper understanding about her social
background and the community in which she lives, is integral to the process of clinical
reasoning, as it will provide exhaustive information on the risk factors that might have increased
her susceptibility to the disease (Shaban 2015, p.5). Moreover, there is a need to record
appropriate information about the medical history of Lucy, and the crucial role that her social
and cultural life might have played on the onset of asthmatic symptoms (Chawla & Davis 2013,
p.661). Conducting an exhaustive review of her family history is essential, due to the fact that the
patient suffers from asthma since her childhood. Assessment of family history is also needed
because her father also suffered from asthma, and died at 40 years of age. Moreover, asthma has
Clinical reasoning refers to the process by which healthcare professionals and nurses are
involved in collecting cues, processing patient information, and gaining a deeper understanding
of the situation or patient condition. This is generally followed by formulating an effective care
plan and implementing the decided interventions (Delany & Golding 2014, p.20). An evaluation
of the outcomes and reflection from the entire process helps in enhancing patient safety. This
assignment will discuss a clinical reasoning cycle, in relation to a case study of Lucy, a 32 year
old patient suffering from asthma.
Sequence of proposed assessment
The patient Lucy has been suffering from asthma since her childhood, and recently works
as a cleaner at a private aged care facility. Although daily inhalation of beclomethasone has
helped in reducing severity of her asthma conditions, she is currently facing several problems
that have led to the occurrence of respiratory distress and dyspnoea. With the aim of collecting
information about the patient and formulating an appropriate care plan, her context and situation
will be initially considered, followed by collecting information about all the vital cues, which in
turn will facilitate patient assessment. Gaining a deeper understanding about her social
background and the community in which she lives, is integral to the process of clinical
reasoning, as it will provide exhaustive information on the risk factors that might have increased
her susceptibility to the disease (Shaban 2015, p.5). Moreover, there is a need to record
appropriate information about the medical history of Lucy, and the crucial role that her social
and cultural life might have played on the onset of asthmatic symptoms (Chawla & Davis 2013,
p.661). Conducting an exhaustive review of her family history is essential, due to the fact that the
patient suffers from asthma since her childhood. Assessment of family history is also needed
because her father also suffered from asthma, and died at 40 years of age. Moreover, asthma has
2CLINICAL JUDGEMENT AND REASONING
also been recognised as one of the diseases that are common in higher social classes (Stephens &
Townsend 2013, p.129). This can be correlated with a need to investigate her social background.
Initially, a vital signs assessment will be conducted to note abnormalities in the temperature,
respiration rate, pulse rate, and blood pressure.
Any deviation from the normal ranges would indicate the state of Lucy's essential body
functions (Storm‐Versloot et al. 2014, p.41). This can be directly be correlated with her
presenting symptoms of dyspnoea, tightness in the chest and wheezing cough. Hence, conduction
of an assessment of the major vital signs, will act as an evidence for presence of any respiratory
difficulties. This assessment will also help in gaining a deeper understanding of the underlined
pathophysiology that might have led to obstruction and inflammation of the airways, and
subsequent development of asthma. This will also be followed by conducting a respiratory
assessment that will involve counting the breathing rate of the patient, followed by auscultation,
where sounds from the lungs and heart will be heard by a stethoscope.
Questions that inform the proposed assessment
Most medical encounters often combine health promotion and problem oriented
approaches, in order to extract answers from the patients that display their hidden concerns,
about specific health abnormalities or symptoms. At times, it is necessary for noting down
exactly what the patient intends to mean by particular statements. Hence, formulating appropriate
questions, while maintaining the privacy and dignity of the patients, is imperative in clinical
assessment (Lin, Watson & Tsai 2013, p.169). All forms of data related to the patient history
form a crucial aspect of health assessment, since they facilitate the process of obtaining
information about previous allergy, illness or any surgeries that have been conducted on the
also been recognised as one of the diseases that are common in higher social classes (Stephens &
Townsend 2013, p.129). This can be correlated with a need to investigate her social background.
Initially, a vital signs assessment will be conducted to note abnormalities in the temperature,
respiration rate, pulse rate, and blood pressure.
Any deviation from the normal ranges would indicate the state of Lucy's essential body
functions (Storm‐Versloot et al. 2014, p.41). This can be directly be correlated with her
presenting symptoms of dyspnoea, tightness in the chest and wheezing cough. Hence, conduction
of an assessment of the major vital signs, will act as an evidence for presence of any respiratory
difficulties. This assessment will also help in gaining a deeper understanding of the underlined
pathophysiology that might have led to obstruction and inflammation of the airways, and
subsequent development of asthma. This will also be followed by conducting a respiratory
assessment that will involve counting the breathing rate of the patient, followed by auscultation,
where sounds from the lungs and heart will be heard by a stethoscope.
Questions that inform the proposed assessment
Most medical encounters often combine health promotion and problem oriented
approaches, in order to extract answers from the patients that display their hidden concerns,
about specific health abnormalities or symptoms. At times, it is necessary for noting down
exactly what the patient intends to mean by particular statements. Hence, formulating appropriate
questions, while maintaining the privacy and dignity of the patients, is imperative in clinical
assessment (Lin, Watson & Tsai 2013, p.169). All forms of data related to the patient history
form a crucial aspect of health assessment, since they facilitate the process of obtaining
information about previous allergy, illness or any surgeries that have been conducted on the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CLINICAL JUDGEMENT AND REASONING
patients. This is turn facilitates nurses and other healthcare professionals to understand about
probable risk factors that might have contributed to development of certain symptoms in the
patient. Hence, identification of the patient history is considered of utmost importance, and a
major priority while delivering optimal health care services (Frank, Basch & Selby 2014,
p.1513). With the aim of collecting relevant information that pertain to patient history,
developing appropriate communication skills is necessary. These skills initiate a patient centred
communication that provides assistance to understand and illicit the perspectives of the patient,
which includes their ideas, expectations, concerns, feelings, needs, and functioning (White &
Danis 2013, p.2325). Patient centred communication also helps to understand the unique cultural
and psychosocial aspects of the patients, and also facilitates the process of reaching a shared
understanding of the problems and treatment practices that will confirm with the values and
beliefs.
An initial establishment of rapport is followed by asking questions that relate to the
patient history, such as, “have you been diagnosed with any other illness since childhood, apart
from asthma?”, or, “did you undergo any major surgery ever?”, or “do you have allergies
towards any medication, food or external agents?”. Questions that relate to presence of pets or
close contact with pet dander and hair will also be formulated. This can be correlated to the fact
that exposure to pet dander have often been found to increase risks of asthma. Other questions
will focus on past medications such as, “do you remember the medicines that you used to take in
childhood for asthma?”, or “what medicines are you currently on?”. Questions related to social
background and family history will also be asked for obtaining a positive diagnosis of asthmatic
symptoms. Responses to these questions will facilitate the formation of a close association
patients. This is turn facilitates nurses and other healthcare professionals to understand about
probable risk factors that might have contributed to development of certain symptoms in the
patient. Hence, identification of the patient history is considered of utmost importance, and a
major priority while delivering optimal health care services (Frank, Basch & Selby 2014,
p.1513). With the aim of collecting relevant information that pertain to patient history,
developing appropriate communication skills is necessary. These skills initiate a patient centred
communication that provides assistance to understand and illicit the perspectives of the patient,
which includes their ideas, expectations, concerns, feelings, needs, and functioning (White &
Danis 2013, p.2325). Patient centred communication also helps to understand the unique cultural
and psychosocial aspects of the patients, and also facilitates the process of reaching a shared
understanding of the problems and treatment practices that will confirm with the values and
beliefs.
An initial establishment of rapport is followed by asking questions that relate to the
patient history, such as, “have you been diagnosed with any other illness since childhood, apart
from asthma?”, or, “did you undergo any major surgery ever?”, or “do you have allergies
towards any medication, food or external agents?”. Questions that relate to presence of pets or
close contact with pet dander and hair will also be formulated. This can be correlated to the fact
that exposure to pet dander have often been found to increase risks of asthma. Other questions
will focus on past medications such as, “do you remember the medicines that you used to take in
childhood for asthma?”, or “what medicines are you currently on?”. Questions related to social
background and family history will also be asked for obtaining a positive diagnosis of asthmatic
symptoms. Responses to these questions will facilitate the formation of a close association
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CLINICAL JUDGEMENT AND REASONING
between the presenting complaints and the past history, thereby facilitating the process of
nursing care.
Analysis of findings
Health assessment refers to the comprehensive plan of care that identifies the specific
preferences of the patients and how they will be addressed by the healthcare professionals or
skilled nursing staff. Therefore, health assessment can be defined as the evaluation of patient
health status by performing a thorough physical examination, after obtaining relevant
information regarding the patient history (Komenaka et al. 2014, p.378). Based on the responses
that will be obtained for the aforementioned questions, followed by conduction of the health
assessment, such as, vital signs measurement and respiratory trouble assessment, the findings
will be analysed and correlated with each other. An extensive study of the patient history
suggests that Lucy has been suffering from asthma since her childhood, which can be considered
hereditary due to presence of similar symptoms in her father that eventually resulted in his death.
This suggests that development of asthmatic symptoms, such as, tightness in the chest and
wheezing breath can be attributed to heredity, since the disease runs in her family (Lajunen,
Jaakkola & Jaakkola 2013, p.179). A range of environmental and genetic factors play an
important role in increasing susceptibility of an individual towards development of asthma.
Family history has often been considered as a risk factor, with 25 genes being identified that
have a close relationship with asthma in more than 6 populations. Some of these genes are IL10,
GSTM1, LTC4S, and IL4R (Meyers et al. 2014, p.410).
Furthermore, environmental factors such as, smoking during pregnancy, pollution and
exposure to indoor volatile organic compounds have also been recognised as triggers for asthma.
between the presenting complaints and the past history, thereby facilitating the process of
nursing care.
Analysis of findings
Health assessment refers to the comprehensive plan of care that identifies the specific
preferences of the patients and how they will be addressed by the healthcare professionals or
skilled nursing staff. Therefore, health assessment can be defined as the evaluation of patient
health status by performing a thorough physical examination, after obtaining relevant
information regarding the patient history (Komenaka et al. 2014, p.378). Based on the responses
that will be obtained for the aforementioned questions, followed by conduction of the health
assessment, such as, vital signs measurement and respiratory trouble assessment, the findings
will be analysed and correlated with each other. An extensive study of the patient history
suggests that Lucy has been suffering from asthma since her childhood, which can be considered
hereditary due to presence of similar symptoms in her father that eventually resulted in his death.
This suggests that development of asthmatic symptoms, such as, tightness in the chest and
wheezing breath can be attributed to heredity, since the disease runs in her family (Lajunen,
Jaakkola & Jaakkola 2013, p.179). A range of environmental and genetic factors play an
important role in increasing susceptibility of an individual towards development of asthma.
Family history has often been considered as a risk factor, with 25 genes being identified that
have a close relationship with asthma in more than 6 populations. Some of these genes are IL10,
GSTM1, LTC4S, and IL4R (Meyers et al. 2014, p.410).
Furthermore, environmental factors such as, smoking during pregnancy, pollution and
exposure to indoor volatile organic compounds have also been recognised as triggers for asthma.
5CLINICAL JUDGEMENT AND REASONING
The process of presenting questions to the patient will therefore help in gaining information
about probable environmental triggers as well that might have contributed to the disease.
Questions will be formulated that pertain to the nature of work that she is expected to perform at
the private aged care facility. Owing to the fact that she has the job of a cleaner at the
workplace, the likelihood of getting exposed to a range of pollutants and allergens are quite high,
which might lead to an exacerbation of asthma attack. Exposure to allergen, pollutants, and viral
infection has been found to worsen asthma.
The vital signs assessment was initially conducted to determine all forms of abnormality
in the normal physiology parameters. An analysis of this assessment states that her pulse rate was
115, temperature 38 °C, respiratory rate 32, blood pressure 160/90, and SaO2 91%. A study of
these vital signs help in establishing links between presence of severe respiratory distress in
Lucy, due to the fact that the pulse rate and respiratory rate are beyond the normal levels.
Furthermore, an elevated blood pressure also suggests presence of hypertensive symptoms in the
patient. However, the oxygen saturation falls within normal limits, which indicate lack of need
to deliver or implement oxygen therapy. Evidences have established strong association between
hypertension, increased breathing rate and high pulse rate, with asthma (Horeczko & Wintemute
2013, p. 179). Hence, conduction of the vital assessments and respiratory assessment helps in
drawing conclusions about the major physiological abnormalities presented by Lucy. Narrowing
of the airways, due to an inflammation of the bronchi and bronchioles, often led to the
development of symptoms such as, wheeziness, tightness in the chest and shortness of breath, all
of which were observed in the patient. An increase in respiratory rate can be attributed to the
action of neutrophils, eosinophils, and cytokines (Schleich et al. 2013, p.11).
The process of presenting questions to the patient will therefore help in gaining information
about probable environmental triggers as well that might have contributed to the disease.
Questions will be formulated that pertain to the nature of work that she is expected to perform at
the private aged care facility. Owing to the fact that she has the job of a cleaner at the
workplace, the likelihood of getting exposed to a range of pollutants and allergens are quite high,
which might lead to an exacerbation of asthma attack. Exposure to allergen, pollutants, and viral
infection has been found to worsen asthma.
The vital signs assessment was initially conducted to determine all forms of abnormality
in the normal physiology parameters. An analysis of this assessment states that her pulse rate was
115, temperature 38 °C, respiratory rate 32, blood pressure 160/90, and SaO2 91%. A study of
these vital signs help in establishing links between presence of severe respiratory distress in
Lucy, due to the fact that the pulse rate and respiratory rate are beyond the normal levels.
Furthermore, an elevated blood pressure also suggests presence of hypertensive symptoms in the
patient. However, the oxygen saturation falls within normal limits, which indicate lack of need
to deliver or implement oxygen therapy. Evidences have established strong association between
hypertension, increased breathing rate and high pulse rate, with asthma (Horeczko & Wintemute
2013, p. 179). Hence, conduction of the vital assessments and respiratory assessment helps in
drawing conclusions about the major physiological abnormalities presented by Lucy. Narrowing
of the airways, due to an inflammation of the bronchi and bronchioles, often led to the
development of symptoms such as, wheeziness, tightness in the chest and shortness of breath, all
of which were observed in the patient. An increase in respiratory rate can be attributed to the
action of neutrophils, eosinophils, and cytokines (Schleich et al. 2013, p.11).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CLINICAL JUDGEMENT AND REASONING
Failure to strike a balance between Th1 and Th2 cells often lead to inflammation of the
airways, thereby blocking the respiratory passage (Ji et al. 2014, p.78). This results in limitation
of airflow and subsequent respiratory distress in the patient. Owing to the fact that Lucy was
dyspnoic, and suffered from laboured and difficulty breathing, immediate medical attention
should be provided. Sudden drop in her oxygen saturation rate to 88% that is much lower than
the normal range of 95-100% also indicates the need of providing immediate healthcare services
for reducing respiratory trouble. This calls for the need of delivering supplemental oxygen for
preventing a worsening of symptoms (Martin & Grocott 2013, p.434). Conduction of a
respiratory assessment that also involved auscultation suggested the presence of wheezing or
continuous whistling and course sounds during breathing (Bohadana, Izbicki & Kraman 2014,
p.747). This can be attributed to the fact that the patient uses her accessory muscles during
respiration, which in turn contributed to laboured breathing. An inflammation of the bronchi and
bronchioles, due to exposure to allergens might have resulted in development of that sounds.
Hence, narrowing of the airways can be considered as the primary physiological abnormality that
led to the development of asthma symptoms, subsequently obstructing air flow and producing
courses sounds during breathing (Zhao, Lloyd & Noble 2013, p.335).
Evaluation of result
An evaluation of the results and drawing conclusions from the reports of the patient
facilitates the procedure of understanding the underlying pathophysiology that might have
contributed to a range of health abnormalities, manifested by the patient. Gaining information on
the patient history suggests that genetic predisposition can be considered as a major risk factor
that made the patient want susceptible to asthma. Extracting relevant information about the
medical and social history of the patient was gained by asking specific questions that pertained to
Failure to strike a balance between Th1 and Th2 cells often lead to inflammation of the
airways, thereby blocking the respiratory passage (Ji et al. 2014, p.78). This results in limitation
of airflow and subsequent respiratory distress in the patient. Owing to the fact that Lucy was
dyspnoic, and suffered from laboured and difficulty breathing, immediate medical attention
should be provided. Sudden drop in her oxygen saturation rate to 88% that is much lower than
the normal range of 95-100% also indicates the need of providing immediate healthcare services
for reducing respiratory trouble. This calls for the need of delivering supplemental oxygen for
preventing a worsening of symptoms (Martin & Grocott 2013, p.434). Conduction of a
respiratory assessment that also involved auscultation suggested the presence of wheezing or
continuous whistling and course sounds during breathing (Bohadana, Izbicki & Kraman 2014,
p.747). This can be attributed to the fact that the patient uses her accessory muscles during
respiration, which in turn contributed to laboured breathing. An inflammation of the bronchi and
bronchioles, due to exposure to allergens might have resulted in development of that sounds.
Hence, narrowing of the airways can be considered as the primary physiological abnormality that
led to the development of asthma symptoms, subsequently obstructing air flow and producing
courses sounds during breathing (Zhao, Lloyd & Noble 2013, p.335).
Evaluation of result
An evaluation of the results and drawing conclusions from the reports of the patient
facilitates the procedure of understanding the underlying pathophysiology that might have
contributed to a range of health abnormalities, manifested by the patient. Gaining information on
the patient history suggests that genetic predisposition can be considered as a major risk factor
that made the patient want susceptible to asthma. Extracting relevant information about the
medical and social history of the patient was gained by asking specific questions that pertained to
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CLINICAL JUDGEMENT AND REASONING
the patient. This in turn enhanced the objective of formulating an appropriate diagnosis, and
providing optimal medical care to the patients. Moreover, an analysis of the present situation and
context of the patient related to her job, also helped in getting sufficient information on the
triggers that might have led to the condition. Hence, the patient answers established strong
evidences for the asthmatic condition to be hereditary. Documentation of subjective and
objective data also suggested that the workplace might have exposed her to various
environmental triggers such as, allergens and pollutants that lead to an exacerbation of her
symptoms (Pult & Riede-Pult 2013, p.25). While, the subjective data helped in understanding the
patient’s point of view and perceptions about the presenting complaints, the objective data
involved all health parameters that were observed or measured.
Physical examination assisted in recognizing the presence of labored breathing
symptoms, accompanied by wheezing sounds (Noble et al. 2013, p.1465). On the other hand, the
vital signs assessment indicated presence of high blood pressure, high temperature and increased
respiratory rate, all of which have been linked with an increase in severity of asthma symptoms.
Drop in oxygen saturation levels at a later period also confirmed the presence of acute
inflammation in her bronchi and bronchioles, thereby suggesting the need of gaining an
understanding of the aetiology that might contribute to such diseases. Salbutamol is the most
commonly used drug for treating asthma, owing to its effects in opening up the airways present
in the lungs (Patel et al. 2013, p.33). However, the common side effects of salbutamol include
increased heart rate, dizziness, anxiety and headache. The nursing care plan will also take into
consideration the fact that the patient Lucy’s health condition showed deterioration upon
administration of the medicine salbutamol.
the patient. This in turn enhanced the objective of formulating an appropriate diagnosis, and
providing optimal medical care to the patients. Moreover, an analysis of the present situation and
context of the patient related to her job, also helped in getting sufficient information on the
triggers that might have led to the condition. Hence, the patient answers established strong
evidences for the asthmatic condition to be hereditary. Documentation of subjective and
objective data also suggested that the workplace might have exposed her to various
environmental triggers such as, allergens and pollutants that lead to an exacerbation of her
symptoms (Pult & Riede-Pult 2013, p.25). While, the subjective data helped in understanding the
patient’s point of view and perceptions about the presenting complaints, the objective data
involved all health parameters that were observed or measured.
Physical examination assisted in recognizing the presence of labored breathing
symptoms, accompanied by wheezing sounds (Noble et al. 2013, p.1465). On the other hand, the
vital signs assessment indicated presence of high blood pressure, high temperature and increased
respiratory rate, all of which have been linked with an increase in severity of asthma symptoms.
Drop in oxygen saturation levels at a later period also confirmed the presence of acute
inflammation in her bronchi and bronchioles, thereby suggesting the need of gaining an
understanding of the aetiology that might contribute to such diseases. Salbutamol is the most
commonly used drug for treating asthma, owing to its effects in opening up the airways present
in the lungs (Patel et al. 2013, p.33). However, the common side effects of salbutamol include
increased heart rate, dizziness, anxiety and headache. The nursing care plan will also take into
consideration the fact that the patient Lucy’s health condition showed deterioration upon
administration of the medicine salbutamol.
8CLINICAL JUDGEMENT AND REASONING
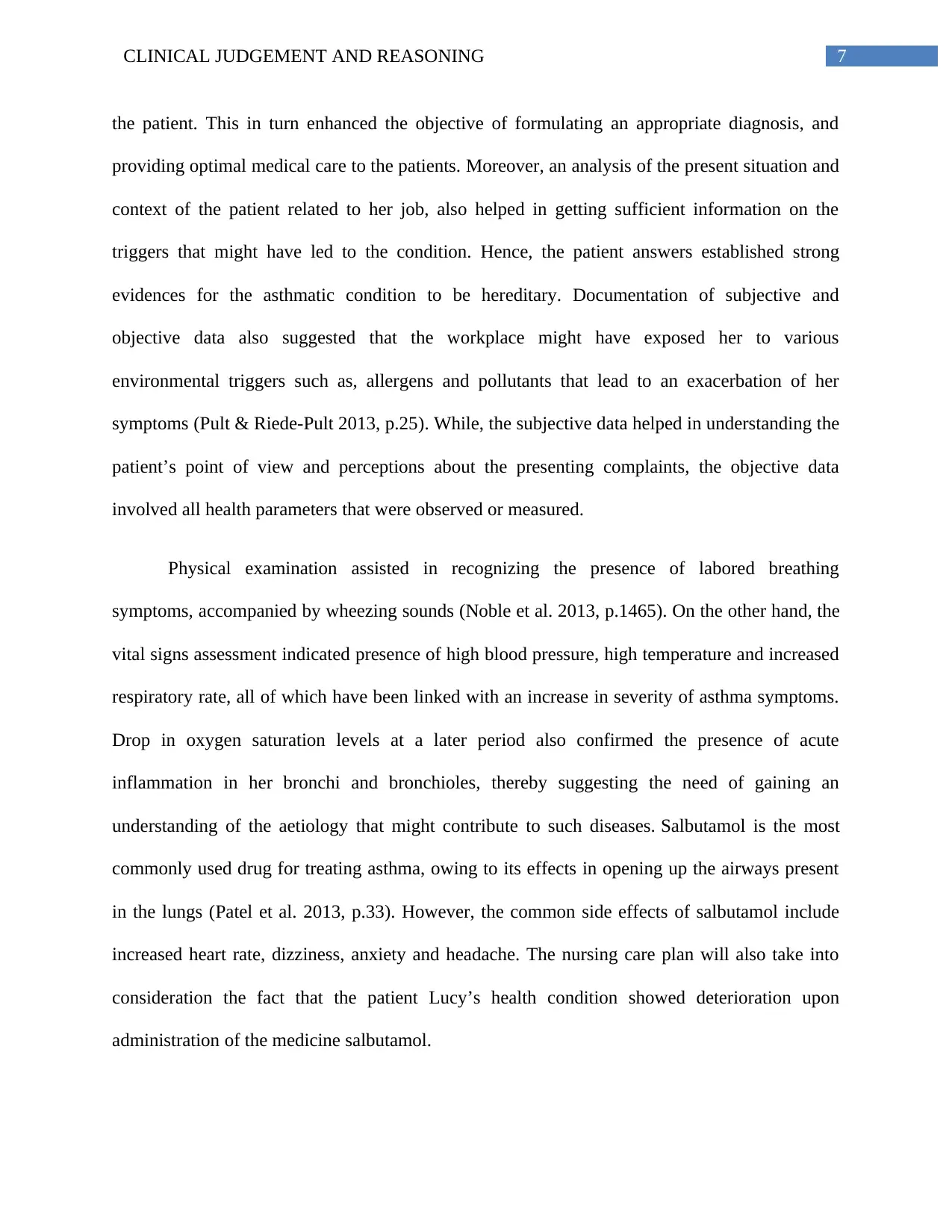
Nursing care plan
This refers to the documentation process that will encompass the set of actions that will
be implemented, for resolving or supporting accurate nursing diagnosis that have been identified
by nursing assessment. The nursing care plan will help in recording the interventions and will
also enable conducting an assessment of their effectiveness. This will facilitate a standardized,
holistic and evidence-based care.
Diagnosis Objective Intervention Rational
Respiratory
distress
To relieve the
patient Lucy from
wheezing and
laboured breathing
that she is suffering
from.
To facilitate her
easy recovery and
bring back the
respiratory rate
within normal
ranges
Conducting an
assessment of the vital
signs of the patient,
measuring the
respiratory death and
the heart rhythm.
Conducting an
auscultation to hear the
breathing sounds and
determining any
abnormality such as, a
whistling or coarse
sound.
Vital signs assessment will
help in noting abnormal
physiological patterns.
Auscultation will determine
presence of inflammation in
the bronchi or obstruction of
the airways
Nursing care plan
This refers to the documentation process that will encompass the set of actions that will
be implemented, for resolving or supporting accurate nursing diagnosis that have been identified
by nursing assessment. The nursing care plan will help in recording the interventions and will
also enable conducting an assessment of their effectiveness. This will facilitate a standardized,
holistic and evidence-based care.
Diagnosis Objective Intervention Rational
Respiratory
distress
To relieve the
patient Lucy from
wheezing and
laboured breathing
that she is suffering
from.
To facilitate her
easy recovery and
bring back the
respiratory rate
within normal
ranges
Conducting an
assessment of the vital
signs of the patient,
measuring the
respiratory death and
the heart rhythm.
Conducting an
auscultation to hear the
breathing sounds and
determining any
abnormality such as, a
whistling or coarse
sound.
Vital signs assessment will
help in noting abnormal
physiological patterns.
Auscultation will determine
presence of inflammation in
the bronchi or obstruction of
the airways
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CLINICAL JUDGEMENT AND REASONING
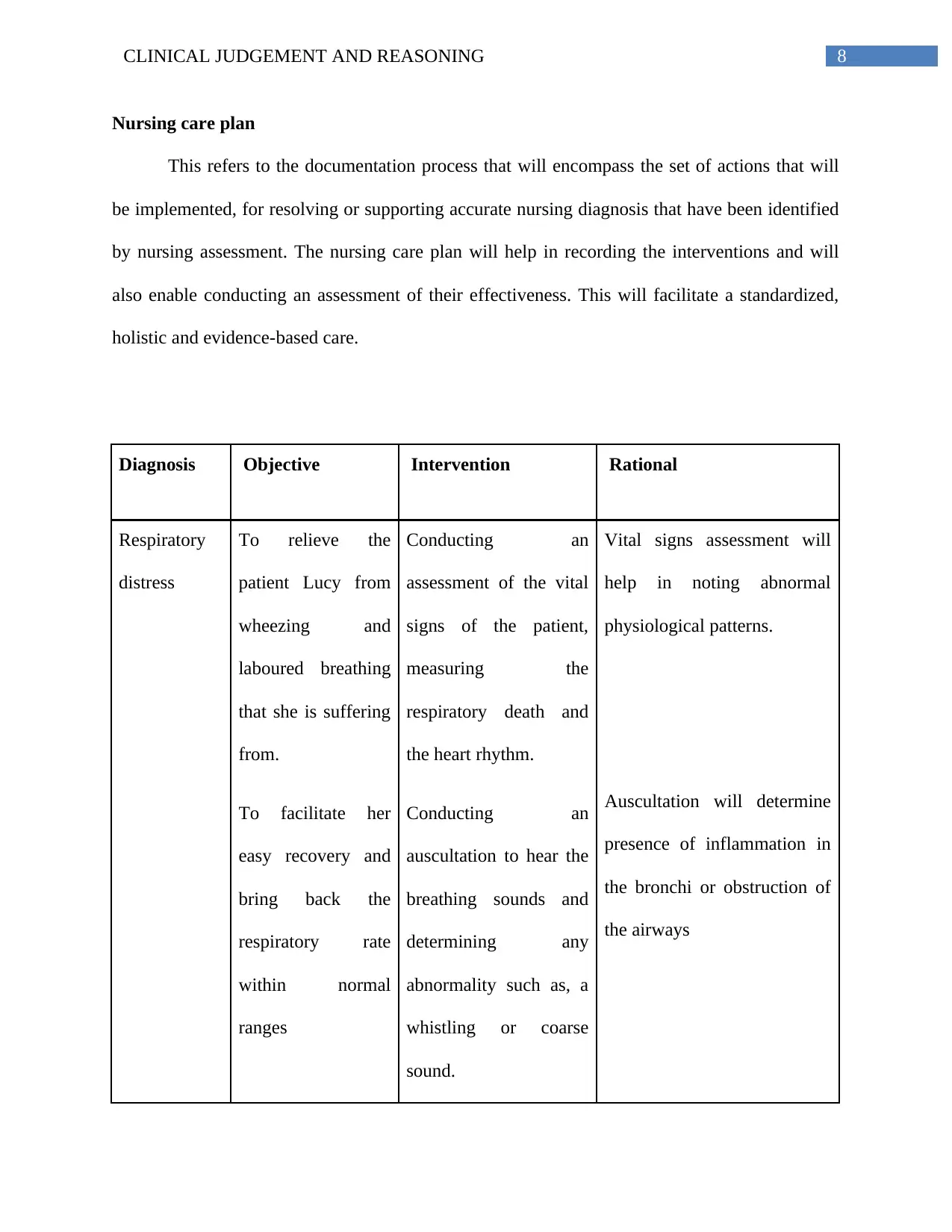
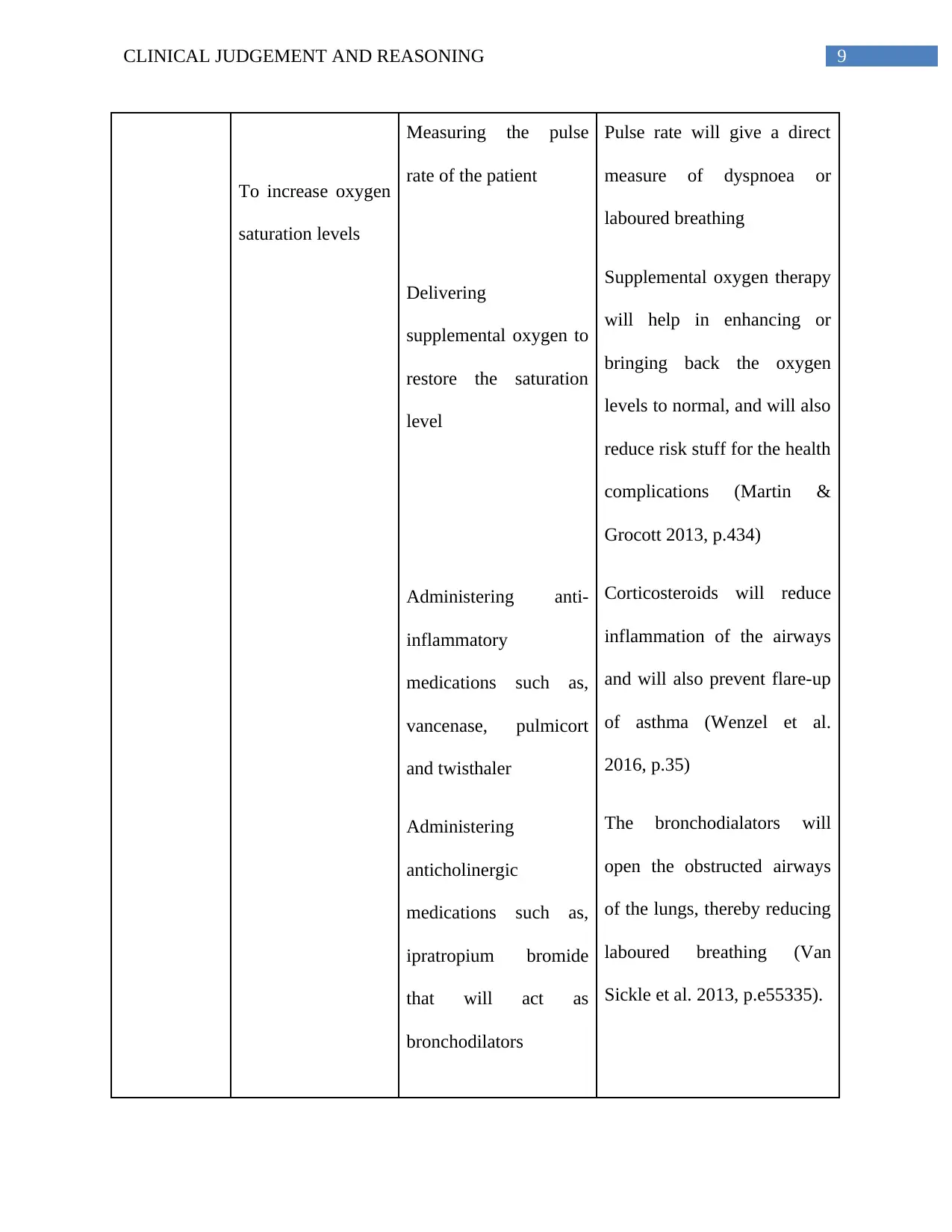
To increase oxygen
saturation levels
Measuring the pulse
rate of the patient
Delivering
supplemental oxygen to
restore the saturation
level
Administering anti-
inflammatory
medications such as,
vancenase, pulmicort
and twisthaler
Administering
anticholinergic
medications such as,
ipratropium bromide
that will act as
bronchodilators
Pulse rate will give a direct
measure of dyspnoea or
laboured breathing
Supplemental oxygen therapy
will help in enhancing or
bringing back the oxygen
levels to normal, and will also
reduce risk stuff for the health
complications (Martin &
Grocott 2013, p.434)
Corticosteroids will reduce
inflammation of the airways
and will also prevent flare-up
of asthma (Wenzel et al.
2016, p.35)
The bronchodialators will
open the obstructed airways
of the lungs, thereby reducing
laboured breathing (Van
Sickle et al. 2013, p.e55335).
To increase oxygen
saturation levels
Measuring the pulse
rate of the patient
Delivering
supplemental oxygen to
restore the saturation
level
Administering anti-
inflammatory
medications such as,
vancenase, pulmicort
and twisthaler
Administering
anticholinergic
medications such as,
ipratropium bromide
that will act as
bronchodilators
Pulse rate will give a direct
measure of dyspnoea or
laboured breathing
Supplemental oxygen therapy
will help in enhancing or
bringing back the oxygen
levels to normal, and will also
reduce risk stuff for the health
complications (Martin &
Grocott 2013, p.434)
Corticosteroids will reduce
inflammation of the airways
and will also prevent flare-up
of asthma (Wenzel et al.
2016, p.35)
The bronchodialators will
open the obstructed airways
of the lungs, thereby reducing
laboured breathing (Van
Sickle et al. 2013, p.e55335).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10CLINICAL JUDGEMENT AND REASONING
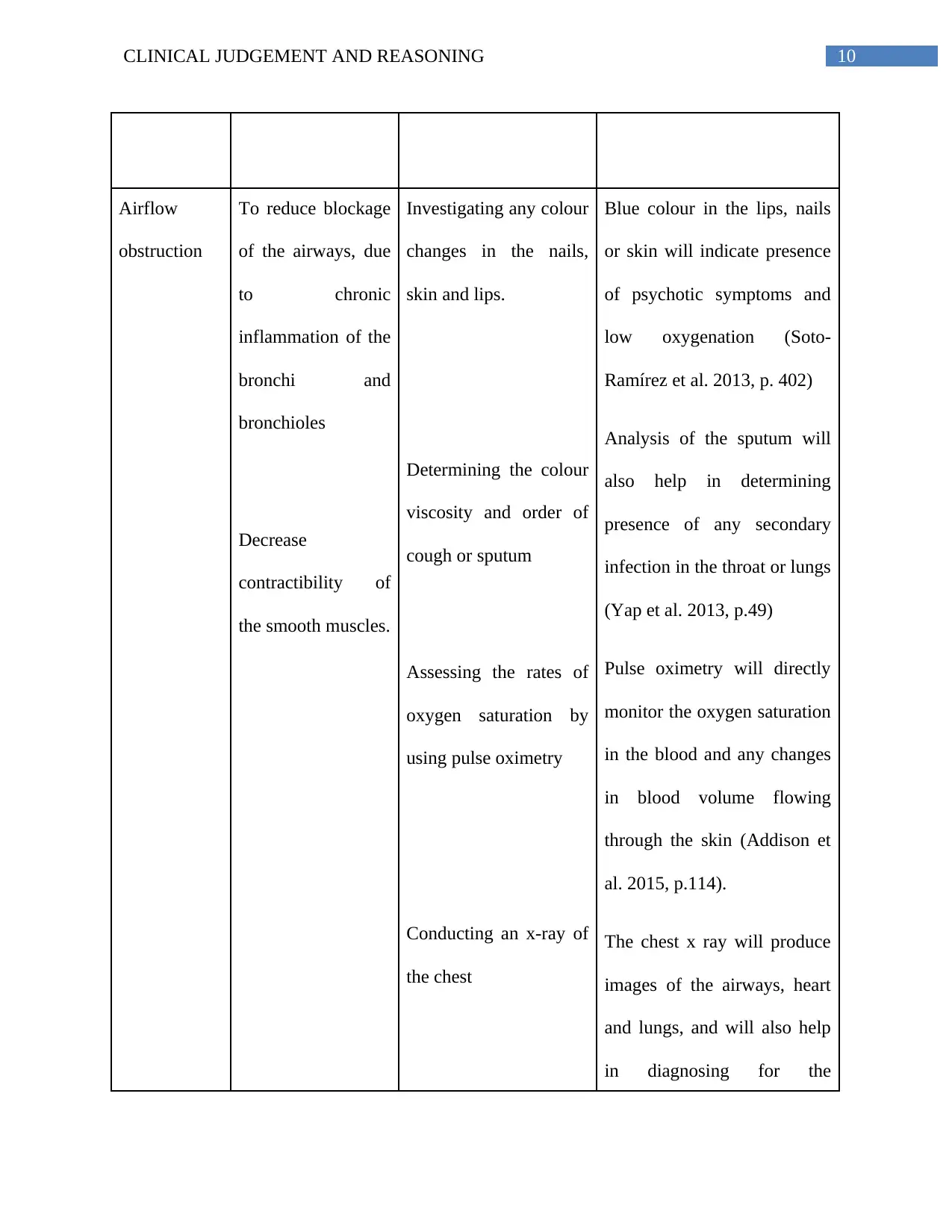
Airflow
obstruction
To reduce blockage
of the airways, due
to chronic
inflammation of the
bronchi and
bronchioles
Decrease
contractibility of
the smooth muscles.
Investigating any colour
changes in the nails,
skin and lips.
Determining the colour
viscosity and order of
cough or sputum
Assessing the rates of
oxygen saturation by
using pulse oximetry
Conducting an x-ray of
the chest
Blue colour in the lips, nails
or skin will indicate presence
of psychotic symptoms and
low oxygenation (Soto-
Ramírez et al. 2013, p. 402)
Analysis of the sputum will
also help in determining
presence of any secondary
infection in the throat or lungs
(Yap et al. 2013, p.49)
Pulse oximetry will directly
monitor the oxygen saturation
in the blood and any changes
in blood volume flowing
through the skin (Addison et
al. 2015, p.114).
The chest x ray will produce
images of the airways, heart
and lungs, and will also help
in diagnosing for the
Airflow
obstruction
To reduce blockage
of the airways, due
to chronic
inflammation of the
bronchi and
bronchioles
Decrease
contractibility of
the smooth muscles.
Investigating any colour
changes in the nails,
skin and lips.
Determining the colour
viscosity and order of
cough or sputum
Assessing the rates of
oxygen saturation by
using pulse oximetry
Conducting an x-ray of
the chest
Blue colour in the lips, nails
or skin will indicate presence
of psychotic symptoms and
low oxygenation (Soto-
Ramírez et al. 2013, p. 402)
Analysis of the sputum will
also help in determining
presence of any secondary
infection in the throat or lungs
(Yap et al. 2013, p.49)
Pulse oximetry will directly
monitor the oxygen saturation
in the blood and any changes
in blood volume flowing
through the skin (Addison et
al. 2015, p.114).
The chest x ray will produce
images of the airways, heart
and lungs, and will also help
in diagnosing for the
11CLINICAL JUDGEMENT AND REASONING
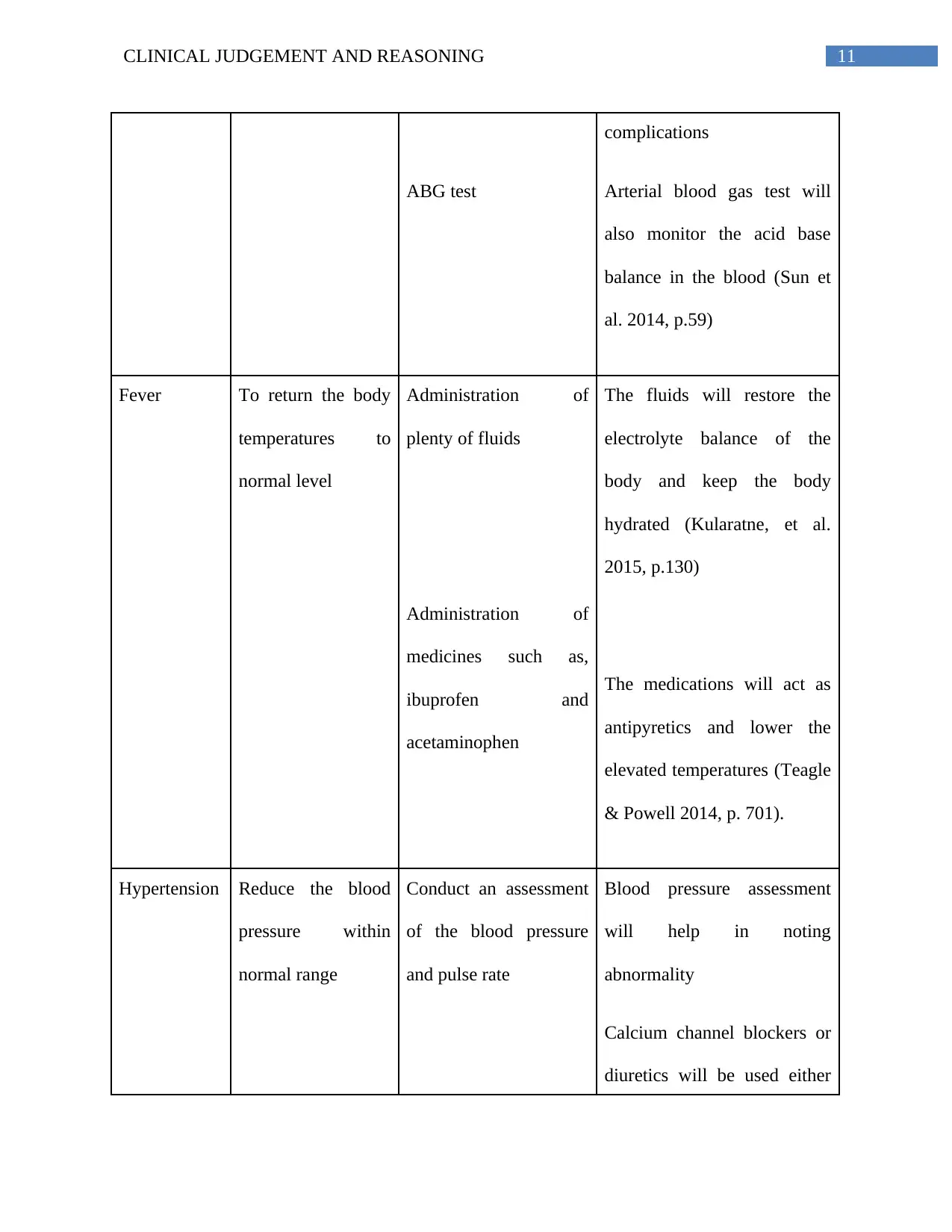
ABG test
complications
Arterial blood gas test will
also monitor the acid base
balance in the blood (Sun et
al. 2014, p.59)
Fever To return the body
temperatures to
normal level
Administration of
plenty of fluids
Administration of
medicines such as,
ibuprofen and
acetaminophen
The fluids will restore the
electrolyte balance of the
body and keep the body
hydrated (Kularatne, et al.
2015, p.130)
The medications will act as
antipyretics and lower the
elevated temperatures (Teagle
& Powell 2014, p. 701).
Hypertension Reduce the blood
pressure within
normal range
Conduct an assessment
of the blood pressure
and pulse rate
Blood pressure assessment
will help in noting
abnormality
Calcium channel blockers or
diuretics will be used either
ABG test
complications
Arterial blood gas test will
also monitor the acid base
balance in the blood (Sun et
al. 2014, p.59)
Fever To return the body
temperatures to
normal level
Administration of
plenty of fluids
Administration of
medicines such as,
ibuprofen and
acetaminophen
The fluids will restore the
electrolyte balance of the
body and keep the body
hydrated (Kularatne, et al.
2015, p.130)
The medications will act as
antipyretics and lower the
elevated temperatures (Teagle
& Powell 2014, p. 701).
Hypertension Reduce the blood
pressure within
normal range
Conduct an assessment
of the blood pressure
and pulse rate
Blood pressure assessment
will help in noting
abnormality
Calcium channel blockers or
diuretics will be used either
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 17
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.