Case Study: Clinical Reasoning Cycle and Patient MR Amari's Condition
VerifiedAdded on 2020/03/01
|10
|2400
|456
Case Study
AI Summary
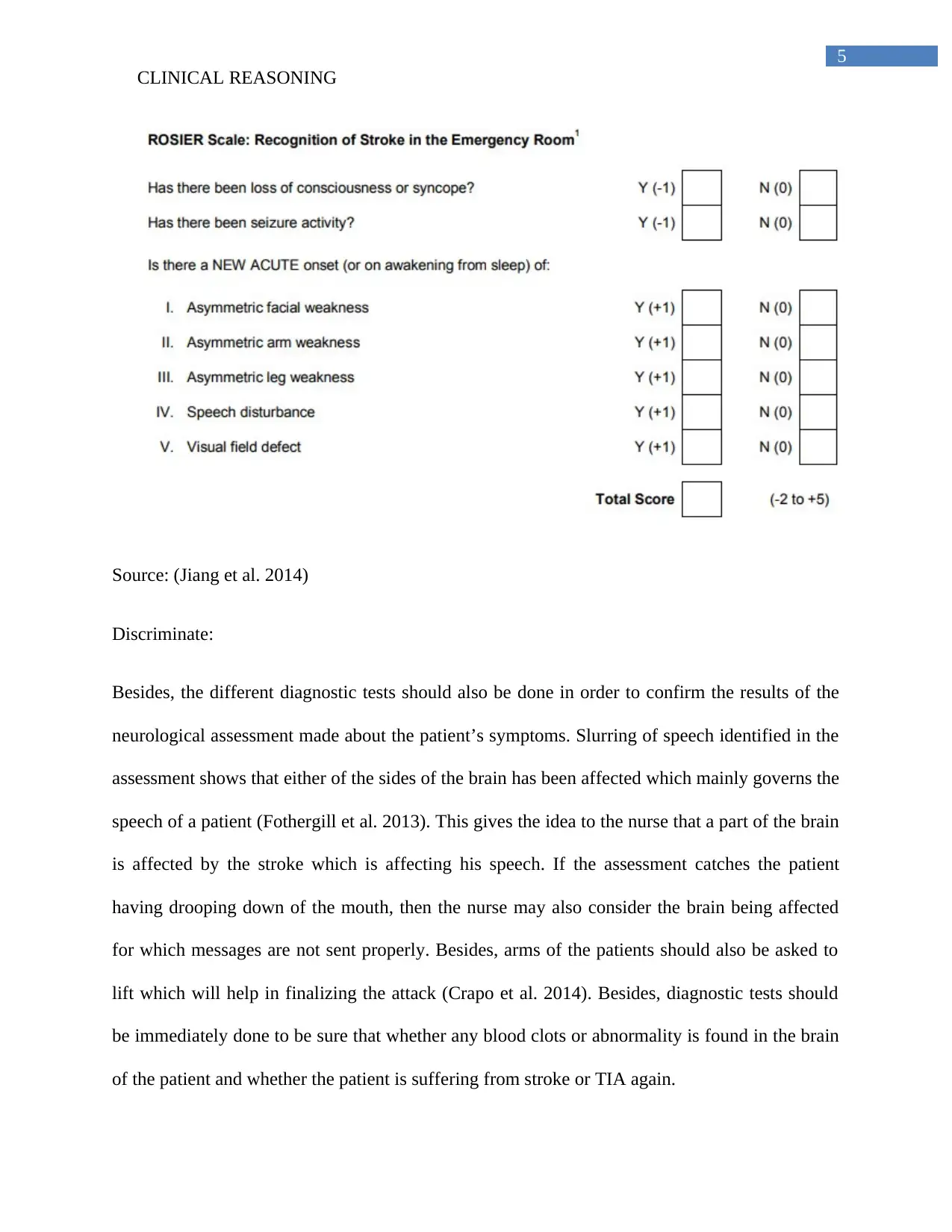
This case study explores the clinical reasoning process of a nurse caring for a patient, Mrs. Amari, admitted with transient ischemic attack (TIA) symptoms. The nurse follows the clinical reasoning cycle, starting with assessing the patient's situation, including her medical history of hypertension, hypercholesterolemia, and tribal customs of smoking. The case details the collection of cues, including physical assessments such as facial droop, slurred speech, and vital signs. The nurse gathers information, recalls relevant medical knowledge about TIA and stroke, interprets the gathered data, discriminates between potential diagnoses, and infers relationships between the patient's condition and her medical history and vital signs. Diagnostic tests, including the FAST and ROSIER assessments, are employed to evaluate the patient's condition, leading to the conclusion that Mrs. Amari is likely experiencing another TIA or potentially a stroke, prompting the nurse to recommend immediate interventions and diagnostic testing. The case study emphasizes the importance of a methodical approach to patient care and the application of clinical reasoning skills in identifying, diagnosing, and managing neurological conditions like TIA and stroke.

1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.