Clinical Trial Assessment Report: Cardiac Surgery and Drug X
VerifiedAdded on 2023/04/21
|13
|3146
|79
Report
AI Summary
This report presents a comprehensive assessment of a clinical trial, evaluating the effects of Drug X on patients undergoing mitral valve replacement (MVR) and coronary artery bypass grafting (CABG). The analysis covers various aspects, including the study design, ethical considerations, and statistical methods used. The report examines the strengths and weaknesses of the study design, such as randomization techniques and follow-up periods, and suggests improvements. It also delves into specific scenarios, like adverse events and patient exclusions, and their implications on the trial's outcomes. Furthermore, the report evaluates the statistical analysis, including the use of Mann-Whitney and Wilcoxon tests, and the interpretation of results, such as the significance of Troponin T levels. The report also includes the assessment of the off-pump versus on-pump CABG study. Overall, the report offers a detailed overview of the clinical trial, its findings, and its implications for future research and patient care.

Running head: CLINICAL TRIAL ASSESSMENT
CLINICAL TRIAL ASSESSMENT
Name of the Student
Name of the University
Author’s Note:
CLINICAL TRIAL ASSESSMENT
Name of the Student
Name of the University
Author’s Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CLINICAL TRIAL ASSESSMENT
Part 1
Answer to the question number 1:
Yes, this study will be under the area of clinical trial for investigational medicinal product
and will be subject to the ‘European Directive on Clinical Trials and The Medicines for
Human Use (Clinical Trials) Regulations (UK)’. The reason behind this is that this study
intend to investigate the effect of a new drug on human and therefore it had to be abide by the
directive and guideline provided by the afore mentioned agency (Mrc.ukri.org, 2019).
Answer to the Question number 2:
Before the start of this clinical trial, approvals have to be taken from several organization
bodies. The name and purpose of these organizational bodies are mentioned below:
Approval from Independent Scientific Review: First of all, it should be approved by a
group of scientist or researchers who will not be involved in this investigation to check the
protocol and study design (Mrc.ukri.org, 2019).
Approval from Ethics committee: Approval has to be taken from an individual ethics
committee and they check about the potential side effects of the treatment, patient recruitment
procedure, patient consent and whether this investigation is adhering to safety, rights, well-
being and dignity of the participants (Mrc.ukri.org, 2019).
Approval from Site- Specific assessment: Approval has to be taken from organization (like
hospitals) where this trial will take place to evaluate that the organization has required
equipment, staff and expertise (Mrc.ukri.org, 2019).
Approval from Clinical Trial Authorisation (CTA): every clinical trial comprises of
medical device or medicinal treatment has to be approved by Clinical Trial Authorisation
(CTA) (Mrc.ukri.org, 2019).
Part 1
Answer to the question number 1:
Yes, this study will be under the area of clinical trial for investigational medicinal product
and will be subject to the ‘European Directive on Clinical Trials and The Medicines for
Human Use (Clinical Trials) Regulations (UK)’. The reason behind this is that this study
intend to investigate the effect of a new drug on human and therefore it had to be abide by the
directive and guideline provided by the afore mentioned agency (Mrc.ukri.org, 2019).
Answer to the Question number 2:
Before the start of this clinical trial, approvals have to be taken from several organization
bodies. The name and purpose of these organizational bodies are mentioned below:
Approval from Independent Scientific Review: First of all, it should be approved by a
group of scientist or researchers who will not be involved in this investigation to check the
protocol and study design (Mrc.ukri.org, 2019).
Approval from Ethics committee: Approval has to be taken from an individual ethics
committee and they check about the potential side effects of the treatment, patient recruitment
procedure, patient consent and whether this investigation is adhering to safety, rights, well-
being and dignity of the participants (Mrc.ukri.org, 2019).
Approval from Site- Specific assessment: Approval has to be taken from organization (like
hospitals) where this trial will take place to evaluate that the organization has required
equipment, staff and expertise (Mrc.ukri.org, 2019).
Approval from Clinical Trial Authorisation (CTA): every clinical trial comprises of
medical device or medicinal treatment has to be approved by Clinical Trial Authorisation
(CTA) (Mrc.ukri.org, 2019).
2CLINICAL TRIAL ASSESSMENT
Answer to the question number 3:
Five other set- up task that’s need to be completed before the patient recruitment is
mentioned below:
1. Detailed scientific protocol for this investigation has to be in place before the patient
recruitment.
2. Assent documents and consent documents for the participants have to be ready.
3. A timeline for this investigation has to be drafted so that the participants can be aware of
the duration of the trial before giving consent.
4. IRB or Institutional Review Board has to be created so that it can be handle the matter
related to the confidentiality certificate and other necessary documents.
5. This investigation requires human use and therefore, a SMP or Safety Monitoring Plan has
to be created.
Answer to the question number 4:
Two weakness of this study design are mentioned below:
1. During the recruitment of the participants, no exclusion criteria were considered and
selected by the authors. Exclusion criteria like age, co-morbid disease might have made the
patients participating in this study more relevant.
2. The follow up period for this investigation is only 6 months and this is relatively low with
regard to clinical trial on human. Drug X will be used as a treatment for this investigation. A
drug can have side effects which might be expressed after six months. Therefore, 6 months
follow up period is too low for clinical trial with human and can be considered as a weakness
to this study design.
Answer to the question number 3:
Five other set- up task that’s need to be completed before the patient recruitment is
mentioned below:
1. Detailed scientific protocol for this investigation has to be in place before the patient
recruitment.
2. Assent documents and consent documents for the participants have to be ready.
3. A timeline for this investigation has to be drafted so that the participants can be aware of
the duration of the trial before giving consent.
4. IRB or Institutional Review Board has to be created so that it can be handle the matter
related to the confidentiality certificate and other necessary documents.
5. This investigation requires human use and therefore, a SMP or Safety Monitoring Plan has
to be created.
Answer to the question number 4:
Two weakness of this study design are mentioned below:
1. During the recruitment of the participants, no exclusion criteria were considered and
selected by the authors. Exclusion criteria like age, co-morbid disease might have made the
patients participating in this study more relevant.
2. The follow up period for this investigation is only 6 months and this is relatively low with
regard to clinical trial on human. Drug X will be used as a treatment for this investigation. A
drug can have side effects which might be expressed after six months. Therefore, 6 months
follow up period is too low for clinical trial with human and can be considered as a weakness
to this study design.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CLINICAL TRIAL ASSESSMENT
Answer to the question number 5:
Two strengths of this study design are mentioned below:
1. The randomization of this investigation will be computer generated. This is a significant
strength of this study as computer generated randomization will reduce the chances of
biasness during the group allocation.
2. One more strength of this study is that it will recruit patient with both MVR and MVR and
CABG. Therefore, from this investigation, it can also be interpreted that whether the drug X
has an effect on the CABG or not.
Answer to the question number 6:
The following improvements could be implemented in the study design to make it better:
1. Exclusion criteria like age, previous cardiac history, and co- morbid disease could be set up
in order to make the participants more relevant to this study design.
2. Follow up period for this investigation could be around 12 months from the completion of
surgery.
3. Number of sample size could be increased. The higher the sample size, the better it is.
Answer to the question number 7:
a) After the surgery, the patient will in the sole discretion of the PI or his/ her colleagues.
Therefore, any complication which might appear will be treated by the PI or his/ her
colleague’s sole discretion. In case of any scenario mentioned above, the PI or his/ her
colleague might treat the patient with might have reactionary effect with drug X or it might
interfere in the results. As a result, the final interpretation of the intervention method might
be erroneous.
Answer to the question number 5:
Two strengths of this study design are mentioned below:
1. The randomization of this investigation will be computer generated. This is a significant
strength of this study as computer generated randomization will reduce the chances of
biasness during the group allocation.
2. One more strength of this study is that it will recruit patient with both MVR and MVR and
CABG. Therefore, from this investigation, it can also be interpreted that whether the drug X
has an effect on the CABG or not.
Answer to the question number 6:
The following improvements could be implemented in the study design to make it better:
1. Exclusion criteria like age, previous cardiac history, and co- morbid disease could be set up
in order to make the participants more relevant to this study design.
2. Follow up period for this investigation could be around 12 months from the completion of
surgery.
3. Number of sample size could be increased. The higher the sample size, the better it is.
Answer to the question number 7:
a) After the surgery, the patient will in the sole discretion of the PI or his/ her colleagues.
Therefore, any complication which might appear will be treated by the PI or his/ her
colleague’s sole discretion. In case of any scenario mentioned above, the PI or his/ her
colleague might treat the patient with might have reactionary effect with drug X or it might
interfere in the results. As a result, the final interpretation of the intervention method might
be erroneous.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CLINICAL TRIAL ASSESSMENT
b) Following measures can be taken to minimize the implications:
1. The patient who has suffered these kinds of complications will be excluded from the final
data interpretation.
2. The PI or his/ her colleague should in contact with or part of the investigation team so that
necessary actions can be taken related to this kind of scenarios.
Answer to the question number 8:
a) This incident will be classified as MACE or Major cardiac adverse event. The patient will
not be discharged; necessary actions will be taken and will be in continuous vigilance unless
the risk of life can be averted. The investigation team should be notified as soon as possible
as this might in relation with their ongoing investigation.
b) This participant will be excluded from the study as the hip replacement surgery can have
significant effect on the cardiac surgery. Additionally, back to back surgery might not be
beneficial for the patient. Furthermore, the hip replacement surgery and its treatment can
have interfering effect on this investigation. Therefore, the investigation team will notify
concerned recruitment centre that the patient will not be participating in the investigation.
c) This incident must be notified to investigation team as they studying the effect of drug X.
Related and relevant approval body of this clinical trial, sponsor of this investigation should
also be notified.
Answer to the question number 9:
a) From the Figure 1 and 2, it can be seen that the Troponin T is not normally distributed and
Mann-Whitney test is used in case ordinal and continuous data. Therefore, the use Mann-
Whitney test in this scenario is justified.
b) Following measures can be taken to minimize the implications:
1. The patient who has suffered these kinds of complications will be excluded from the final
data interpretation.
2. The PI or his/ her colleague should in contact with or part of the investigation team so that
necessary actions can be taken related to this kind of scenarios.
Answer to the question number 8:
a) This incident will be classified as MACE or Major cardiac adverse event. The patient will
not be discharged; necessary actions will be taken and will be in continuous vigilance unless
the risk of life can be averted. The investigation team should be notified as soon as possible
as this might in relation with their ongoing investigation.
b) This participant will be excluded from the study as the hip replacement surgery can have
significant effect on the cardiac surgery. Additionally, back to back surgery might not be
beneficial for the patient. Furthermore, the hip replacement surgery and its treatment can
have interfering effect on this investigation. Therefore, the investigation team will notify
concerned recruitment centre that the patient will not be participating in the investigation.
c) This incident must be notified to investigation team as they studying the effect of drug X.
Related and relevant approval body of this clinical trial, sponsor of this investigation should
also be notified.
Answer to the question number 9:
a) From the Figure 1 and 2, it can be seen that the Troponin T is not normally distributed and
Mann-Whitney test is used in case ordinal and continuous data. Therefore, the use Mann-
Whitney test in this scenario is justified.
5CLINICAL TRIAL ASSESSMENT
b) Wilcoxon signed rank test can be used to analyse the treatment effect of Troponin T.
Mann-Whitney test just study the difference between the two independent groups and
therefore producing only p-value. On the other hand, Wilcoxon signed rank test also studies
same hypothesis with paired or matched samples (Benavoli, Corani & Mangili, 2016).
c) The higher confidence level interval for MVR and CABG patient might have happened
due to the low population size in comparison with the only MVR patients. Additionally, no
exclusion criteria before the beginning of the experiment might also be the contributing
factor.
Spearman correlation can be used to analyse the categorical data as this test does not depend
on the assumption on the normally distributed data and strength of this test is to analyse the
association between ordinal variables (Thirumalai, Chandhini & Vaishnavi, 2017).
Answer to the question number 10:
50 MVR patients and 50 MVR + CABG patients were selected for this study. Both groups of
the patients were divided in to two group of control and treatment and divide were made in
1:1 ratio. The pre- operative characteristics like age, gender, BMI were presented in the
detailed manner in Table 1 for both the groups. Figure 1 and 2 represents the trial outcomes
Troponin T both the groups. Figure 1 represents the data for MVR patients and Figure 2
represents the data for MVR with CABG patients. From the data presented in Table 2, it can
be seen that there is difference between the treatment group and control for both the MVR
patients and MVR with CABG patients. In both cases, Troponin T level is lower in case of
the treatment group in comparison with the control. However, the difference in the group of
patients with only MVR is not significant (p value – 0.82) whereas difference in the group of
patients with MVR and CABG is significant (p value – 0.0048). Figure 3 and 4 depicts the
difference between post operative hospital stay for the treatment and control group. Figure 3
b) Wilcoxon signed rank test can be used to analyse the treatment effect of Troponin T.
Mann-Whitney test just study the difference between the two independent groups and
therefore producing only p-value. On the other hand, Wilcoxon signed rank test also studies
same hypothesis with paired or matched samples (Benavoli, Corani & Mangili, 2016).
c) The higher confidence level interval for MVR and CABG patient might have happened
due to the low population size in comparison with the only MVR patients. Additionally, no
exclusion criteria before the beginning of the experiment might also be the contributing
factor.
Spearman correlation can be used to analyse the categorical data as this test does not depend
on the assumption on the normally distributed data and strength of this test is to analyse the
association between ordinal variables (Thirumalai, Chandhini & Vaishnavi, 2017).
Answer to the question number 10:
50 MVR patients and 50 MVR + CABG patients were selected for this study. Both groups of
the patients were divided in to two group of control and treatment and divide were made in
1:1 ratio. The pre- operative characteristics like age, gender, BMI were presented in the
detailed manner in Table 1 for both the groups. Figure 1 and 2 represents the trial outcomes
Troponin T both the groups. Figure 1 represents the data for MVR patients and Figure 2
represents the data for MVR with CABG patients. From the data presented in Table 2, it can
be seen that there is difference between the treatment group and control for both the MVR
patients and MVR with CABG patients. In both cases, Troponin T level is lower in case of
the treatment group in comparison with the control. However, the difference in the group of
patients with only MVR is not significant (p value – 0.82) whereas difference in the group of
patients with MVR and CABG is significant (p value – 0.0048). Figure 3 and 4 depicts the
difference between post operative hospital stay for the treatment and control group. Figure 3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CLINICAL TRIAL ASSESSMENT
represents the patients with only MVR and Figure 4 represents the patients with both MVR
and CABG. The trend lines for both the groups are similar.
Answer to the question number 11:
From the analysis, it can be concluded that the Drug X has an effect on the presence of
marker Troponin T. However, this difference is not significant in case of the patients with
only MVR but the difference is significant in case of patients with MVR and CABG. The
disparity in the statistical significance might have occurred due to the CABG. Therefore, it
was appropriate to put the patients in two different groups as the result suggested. The
combination of both the patients in a single group might have skewed the final outcome as
the patients were treated with different conditions. Selection bias would have been present in
the data if both groups of patients were put in a single group. Further investigation is required
to examine whether Drug X has an effect on CABG or vice versa.
Part 2
Answer to the question number 1:
The study type that has been designed for this investigation is Randomised Controlled Trial
(RCT).
Answer to the question number 2:
In this study, blinded randomisation has been used and a block size of 8 was used as
stratification.
Answer to the question number 3:
The sample population for this investigation was increased after the interim analysis to 2500
patients in order to uphold the power of 90 per cent whose odds ratio will be 0.63.
represents the patients with only MVR and Figure 4 represents the patients with both MVR
and CABG. The trend lines for both the groups are similar.
Answer to the question number 11:
From the analysis, it can be concluded that the Drug X has an effect on the presence of
marker Troponin T. However, this difference is not significant in case of the patients with
only MVR but the difference is significant in case of patients with MVR and CABG. The
disparity in the statistical significance might have occurred due to the CABG. Therefore, it
was appropriate to put the patients in two different groups as the result suggested. The
combination of both the patients in a single group might have skewed the final outcome as
the patients were treated with different conditions. Selection bias would have been present in
the data if both groups of patients were put in a single group. Further investigation is required
to examine whether Drug X has an effect on CABG or vice versa.
Part 2
Answer to the question number 1:
The study type that has been designed for this investigation is Randomised Controlled Trial
(RCT).
Answer to the question number 2:
In this study, blinded randomisation has been used and a block size of 8 was used as
stratification.
Answer to the question number 3:
The sample population for this investigation was increased after the interim analysis to 2500
patients in order to uphold the power of 90 per cent whose odds ratio will be 0.63.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CLINICAL TRIAL ASSESSMENT
Answer to the question number 4:
36 per cent participants had a history of myocardial infarction amongst the patients who
participated in the off- pump CABG.
Answer to the question number 5:
The ITT or Intention- to- Treat method is a conservative approach and it is generally under
estimate the effect of a clinical trial. On the other hand, Per- Protocol approach is more useful
in case of the sensitivity analyses. In case of clinical trial, general rule of thumb is that it is
better to stay conservative (Ranganathan, Pramesh & Aggarwal, 2016). Therefore, in regard
to clinical trial, Intention- to- Treat method is preferable in comparison with Per- Protocol
approach.
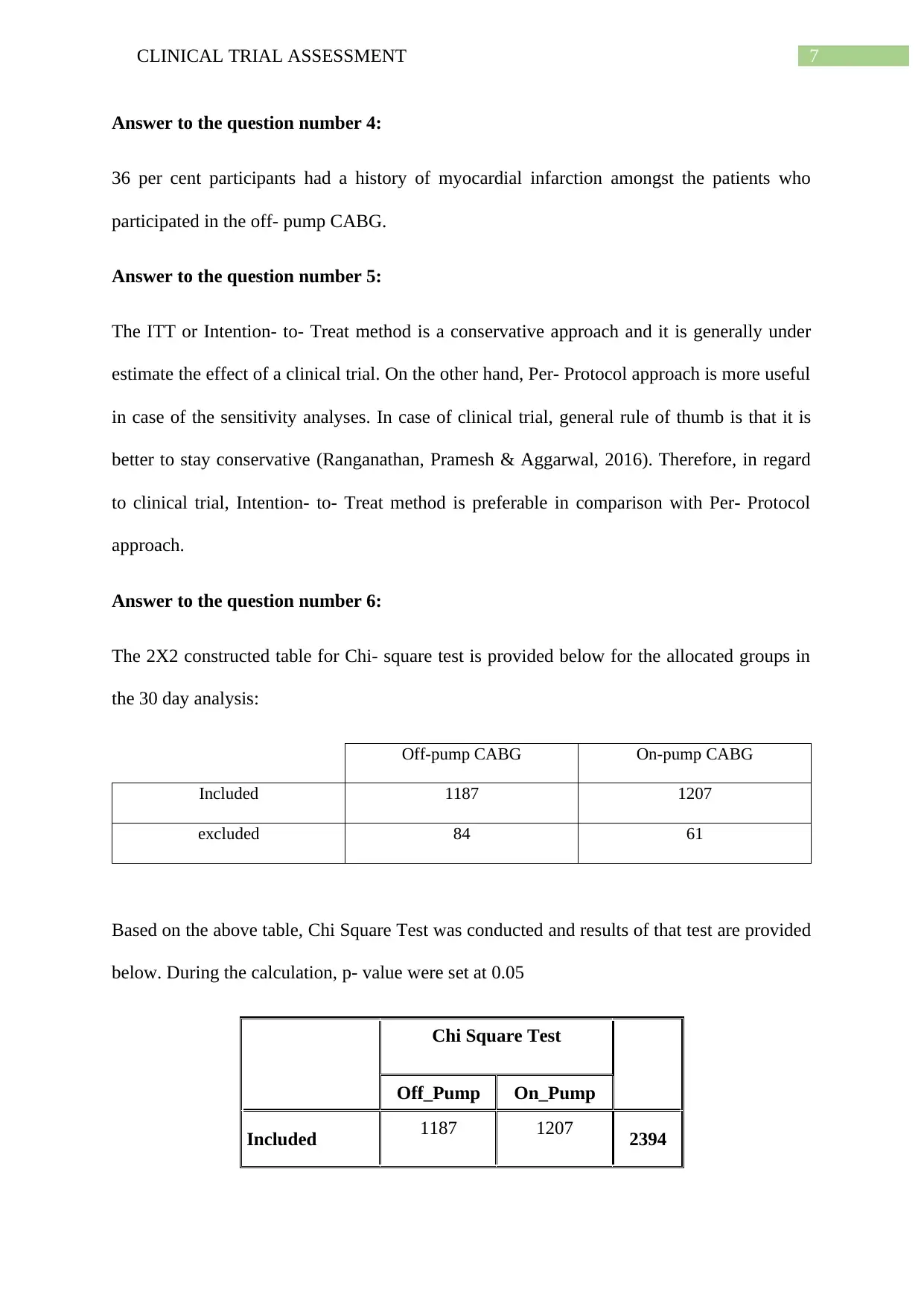
Answer to the question number 6:
The 2X2 constructed table for Chi- square test is provided below for the allocated groups in
the 30 day analysis:
Off-pump CABG On-pump CABG
Included 1187 1207
excluded 84 61
Based on the above table, Chi Square Test was conducted and results of that test are provided
below. During the calculation, p- value were set at 0.05
Chi Square Test
Off_Pump On_Pump
Included 1187 1207 2394
Answer to the question number 4:
36 per cent participants had a history of myocardial infarction amongst the patients who
participated in the off- pump CABG.
Answer to the question number 5:
The ITT or Intention- to- Treat method is a conservative approach and it is generally under
estimate the effect of a clinical trial. On the other hand, Per- Protocol approach is more useful
in case of the sensitivity analyses. In case of clinical trial, general rule of thumb is that it is
better to stay conservative (Ranganathan, Pramesh & Aggarwal, 2016). Therefore, in regard
to clinical trial, Intention- to- Treat method is preferable in comparison with Per- Protocol
approach.
Answer to the question number 6:
The 2X2 constructed table for Chi- square test is provided below for the allocated groups in
the 30 day analysis:
Off-pump CABG On-pump CABG
Included 1187 1207
excluded 84 61
Based on the above table, Chi Square Test was conducted and results of that test are provided
below. During the calculation, p- value were set at 0.05
Chi Square Test
Off_Pump On_Pump
Included 1187 1207 2394
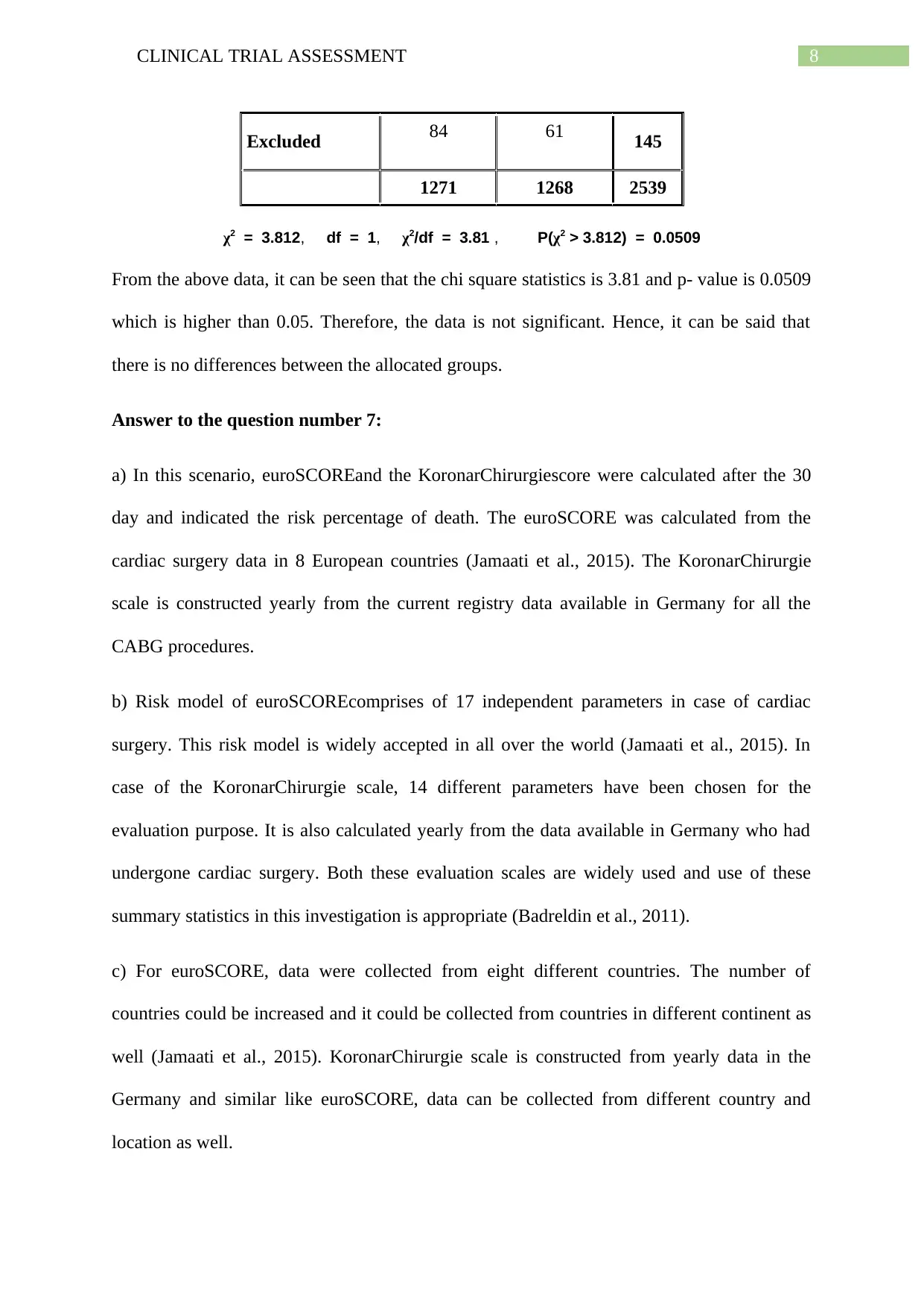
8CLINICAL TRIAL ASSESSMENT
Excluded 84 61 145
1271 1268 2539
χ2 = 3.812, df = 1, χ2/df = 3.81 , P(χ2 > 3.812) = 0.0509
From the above data, it can be seen that the chi square statistics is 3.81 and p- value is 0.0509
which is higher than 0.05. Therefore, the data is not significant. Hence, it can be said that
there is no differences between the allocated groups.
Answer to the question number 7:
a) In this scenario, euroSCOREand the KoronarChirurgiescore were calculated after the 30
day and indicated the risk percentage of death. The euroSCORE was calculated from the
cardiac surgery data in 8 European countries (Jamaati et al., 2015). The KoronarChirurgie
scale is constructed yearly from the current registry data available in Germany for all the
CABG procedures.
b) Risk model of euroSCOREcomprises of 17 independent parameters in case of cardiac
surgery. This risk model is widely accepted in all over the world (Jamaati et al., 2015). In
case of the KoronarChirurgie scale, 14 different parameters have been chosen for the
evaluation purpose. It is also calculated yearly from the data available in Germany who had
undergone cardiac surgery. Both these evaluation scales are widely used and use of these
summary statistics in this investigation is appropriate (Badreldin et al., 2011).
c) For euroSCORE, data were collected from eight different countries. The number of
countries could be increased and it could be collected from countries in different continent as
well (Jamaati et al., 2015). KoronarChirurgie scale is constructed from yearly data in the
Germany and similar like euroSCORE, data can be collected from different country and
location as well.
Excluded 84 61 145
1271 1268 2539
χ2 = 3.812, df = 1, χ2/df = 3.81 , P(χ2 > 3.812) = 0.0509
From the above data, it can be seen that the chi square statistics is 3.81 and p- value is 0.0509
which is higher than 0.05. Therefore, the data is not significant. Hence, it can be said that
there is no differences between the allocated groups.
Answer to the question number 7:
a) In this scenario, euroSCOREand the KoronarChirurgiescore were calculated after the 30
day and indicated the risk percentage of death. The euroSCORE was calculated from the
cardiac surgery data in 8 European countries (Jamaati et al., 2015). The KoronarChirurgie
scale is constructed yearly from the current registry data available in Germany for all the
CABG procedures.
b) Risk model of euroSCOREcomprises of 17 independent parameters in case of cardiac
surgery. This risk model is widely accepted in all over the world (Jamaati et al., 2015). In
case of the KoronarChirurgie scale, 14 different parameters have been chosen for the
evaluation purpose. It is also calculated yearly from the data available in Germany who had
undergone cardiac surgery. Both these evaluation scales are widely used and use of these
summary statistics in this investigation is appropriate (Badreldin et al., 2011).
c) For euroSCORE, data were collected from eight different countries. The number of
countries could be increased and it could be collected from countries in different continent as
well (Jamaati et al., 2015). KoronarChirurgie scale is constructed from yearly data in the
Germany and similar like euroSCORE, data can be collected from different country and
location as well.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CLINICAL TRIAL ASSESSMENT
Answer to the question number 8:
According to the authors of this study, the primary end point was any key adverse incident or
any composite of death with thirty days and within twelve months after surgery. The authors
of this investigation have used various statistical analysis tools like chi-square test, Mantel–
Haenszel chi-square tests, and Kaplan–Meier curves were used for the interpretation of their
data. The reasoning behind the choice of different tool is that each of the tools was used to
interpret different features of the study. To cite few examples, chi-square test was employed
to study the comparison at the end of 30 day end point whereas Kaplan–Meier curves were
constructed at the end of 12 month end point.
Answer to the question number 9:
a) The odds of the occurrence of the repeat revascularization for off- pump CABG patients in
comparison with the on- pump CABG patients at the end of 30 day end point is 2.42.
Therefore, it can be inferred that the off- Pump CABG has higher contribution towards the
occurrence of repeat revascularization. The p- value is also less that 0.05 which signifies that
the data are significant.
b) The risk of repeat revascularization after the completion of 12 month end point is no
different in comparison with the 30 day end point. In case of 12 month end point, the odds
ratio is 1.52. Hence, the odds ratio is higher than 1 in case of both the end points. Therefore,
it can be said that the risk of repeat revascularization after the completion of 12 month end
point is no statistically different while comparing with the 30 day end point (Diegeler et al.,
2013).
Answer to the question number 10:
Answer to the question number 8:
According to the authors of this study, the primary end point was any key adverse incident or
any composite of death with thirty days and within twelve months after surgery. The authors
of this investigation have used various statistical analysis tools like chi-square test, Mantel–
Haenszel chi-square tests, and Kaplan–Meier curves were used for the interpretation of their
data. The reasoning behind the choice of different tool is that each of the tools was used to
interpret different features of the study. To cite few examples, chi-square test was employed
to study the comparison at the end of 30 day end point whereas Kaplan–Meier curves were
constructed at the end of 12 month end point.
Answer to the question number 9:
a) The odds of the occurrence of the repeat revascularization for off- pump CABG patients in
comparison with the on- pump CABG patients at the end of 30 day end point is 2.42.
Therefore, it can be inferred that the off- Pump CABG has higher contribution towards the
occurrence of repeat revascularization. The p- value is also less that 0.05 which signifies that
the data are significant.
b) The risk of repeat revascularization after the completion of 12 month end point is no
different in comparison with the 30 day end point. In case of 12 month end point, the odds
ratio is 1.52. Hence, the odds ratio is higher than 1 in case of both the end points. Therefore,
it can be said that the risk of repeat revascularization after the completion of 12 month end
point is no statistically different while comparing with the 30 day end point (Diegeler et al.,
2013).
Answer to the question number 10:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

10CLINICAL TRIAL ASSESSMENT
In case of the patients who were in the On- pump CABG group, 89 per cent patients were
event free after 180 days and on the other hand, the patients who were in the Off- pump
CABG group, 91 per cent patients were event free after 180 days.
In case of the patients who were in the On- pump CABG group, 89 per cent patients were
event free after 180 days and on the other hand, the patients who were in the Off- pump
CABG group, 91 per cent patients were event free after 180 days.
11CLINICAL TRIAL ASSESSMENT
References:
Badreldin, A. M. A., Kania, A., Ismail, M. M. A., Lehmann, T., Gummert, J., Doenst, T.,
&Hekmat, K. (2011). KCH, the German preoperative score for isolated coronary
artery bypass surgery: is it superior to the logistic EuroSCORE?. The Thoracic and
cardiovascular surgeon, 59(07), 399-405.
Benavoli, A., Corani, G., & Mangili, F. (2016). Should we really use post-hoc tests based on
mean-ranks?. The Journal of Machine Learning Research, 17(1), 152-161.
Diegeler, A., Börgermann, J., Kappert, U., Breuer, M., Böning, A., Ursulescu,
A., ...&Veeckmann, P. (2013). Off-pump versus on-pump coronary-artery bypass
grafting in elderly patients. New England Journal of Medicine, 368(13), 1189-1198.
Jamaati, H., Najafi, A., Kahe, F., Karimi, Z., Ahmadi, Z., Bolursaz, M., ...&Hashemian, S. M.
(2015). Assessment of the EuroSCORE risk scoring system for patients undergoing
coronary artery bypass graft surgery in a group of Iranian patients. Indian journal of
critical care medicine: peer-reviewed, official publication of Indian Society of
Critical Care Medicine, 19(10), 576.
Mrc.ukri.org. (2019). MRC policy on UK clinical trials regulations - Research - Medical
Research Council. Retrieved from https://mrc.ukri.org/research/policies-and-
guidance-for-researchers/clinical-research-governance/clinical-trials-regulations/
Ranganathan, P., Pramesh, C. S., & Aggarwal, R. (2016). Common pitfalls in statistical
analysis: Intention-to-treat versus per-protocol analysis. Perspectives in clinical
research, 7(3), 144.
Thirumalai, C., Chandhini, S. A., & Vaishnavi, M. (2017, April). Analysing the concrete
compressive strength using Pearson and Spearman. In 2017 International conference
References:
Badreldin, A. M. A., Kania, A., Ismail, M. M. A., Lehmann, T., Gummert, J., Doenst, T.,
&Hekmat, K. (2011). KCH, the German preoperative score for isolated coronary
artery bypass surgery: is it superior to the logistic EuroSCORE?. The Thoracic and
cardiovascular surgeon, 59(07), 399-405.
Benavoli, A., Corani, G., & Mangili, F. (2016). Should we really use post-hoc tests based on
mean-ranks?. The Journal of Machine Learning Research, 17(1), 152-161.
Diegeler, A., Börgermann, J., Kappert, U., Breuer, M., Böning, A., Ursulescu,
A., ...&Veeckmann, P. (2013). Off-pump versus on-pump coronary-artery bypass
grafting in elderly patients. New England Journal of Medicine, 368(13), 1189-1198.
Jamaati, H., Najafi, A., Kahe, F., Karimi, Z., Ahmadi, Z., Bolursaz, M., ...&Hashemian, S. M.
(2015). Assessment of the EuroSCORE risk scoring system for patients undergoing
coronary artery bypass graft surgery in a group of Iranian patients. Indian journal of
critical care medicine: peer-reviewed, official publication of Indian Society of
Critical Care Medicine, 19(10), 576.
Mrc.ukri.org. (2019). MRC policy on UK clinical trials regulations - Research - Medical
Research Council. Retrieved from https://mrc.ukri.org/research/policies-and-
guidance-for-researchers/clinical-research-governance/clinical-trials-regulations/
Ranganathan, P., Pramesh, C. S., & Aggarwal, R. (2016). Common pitfalls in statistical
analysis: Intention-to-treat versus per-protocol analysis. Perspectives in clinical
research, 7(3), 144.
Thirumalai, C., Chandhini, S. A., & Vaishnavi, M. (2017, April). Analysing the concrete
compressive strength using Pearson and Spearman. In 2017 International conference
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.