CNA253 Clinical Assessment: Evaluation of Miss Jane Green's Case
VerifiedAdded on 2023/06/13
|10
|1674
|310
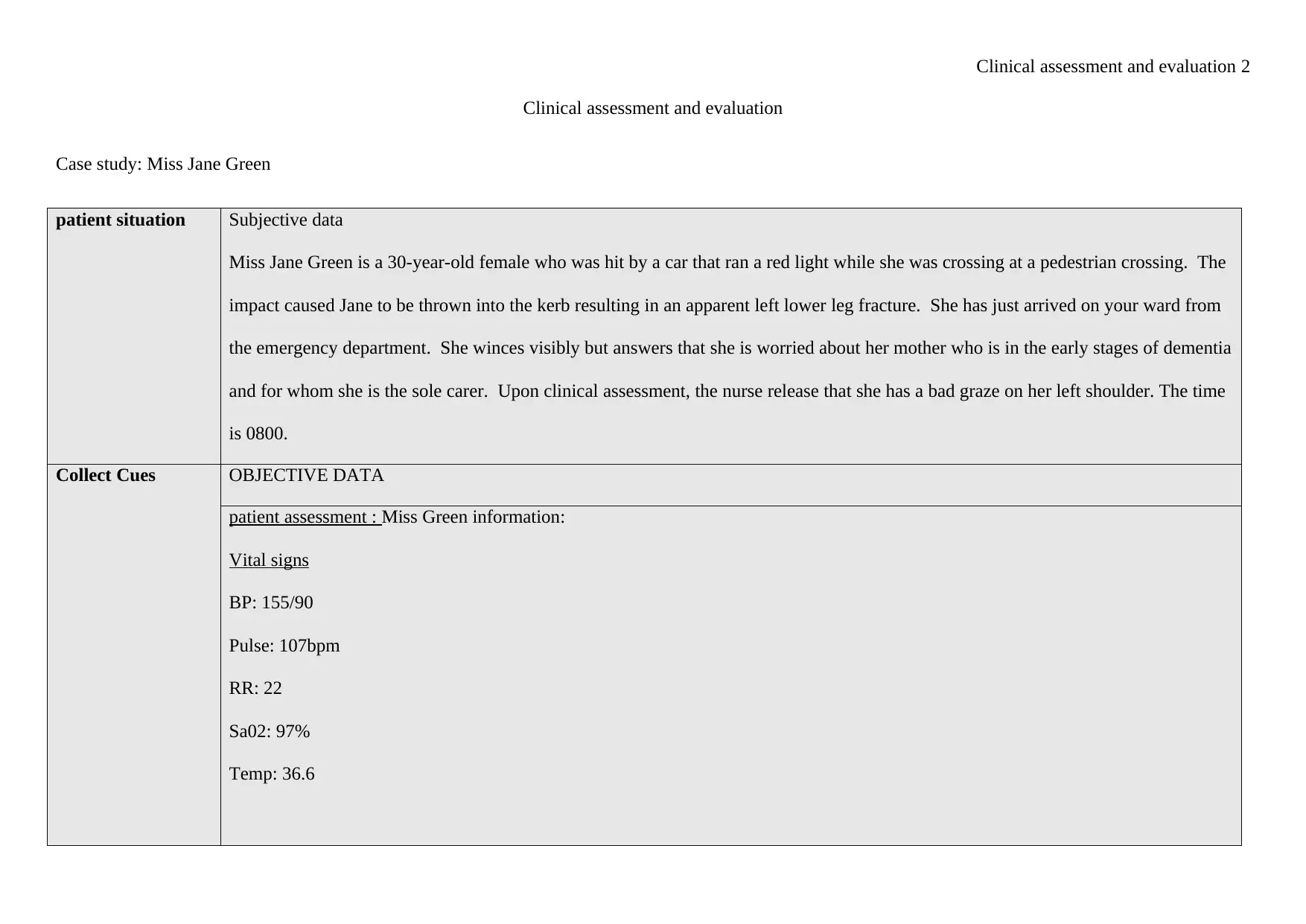
Case Study
AI Summary
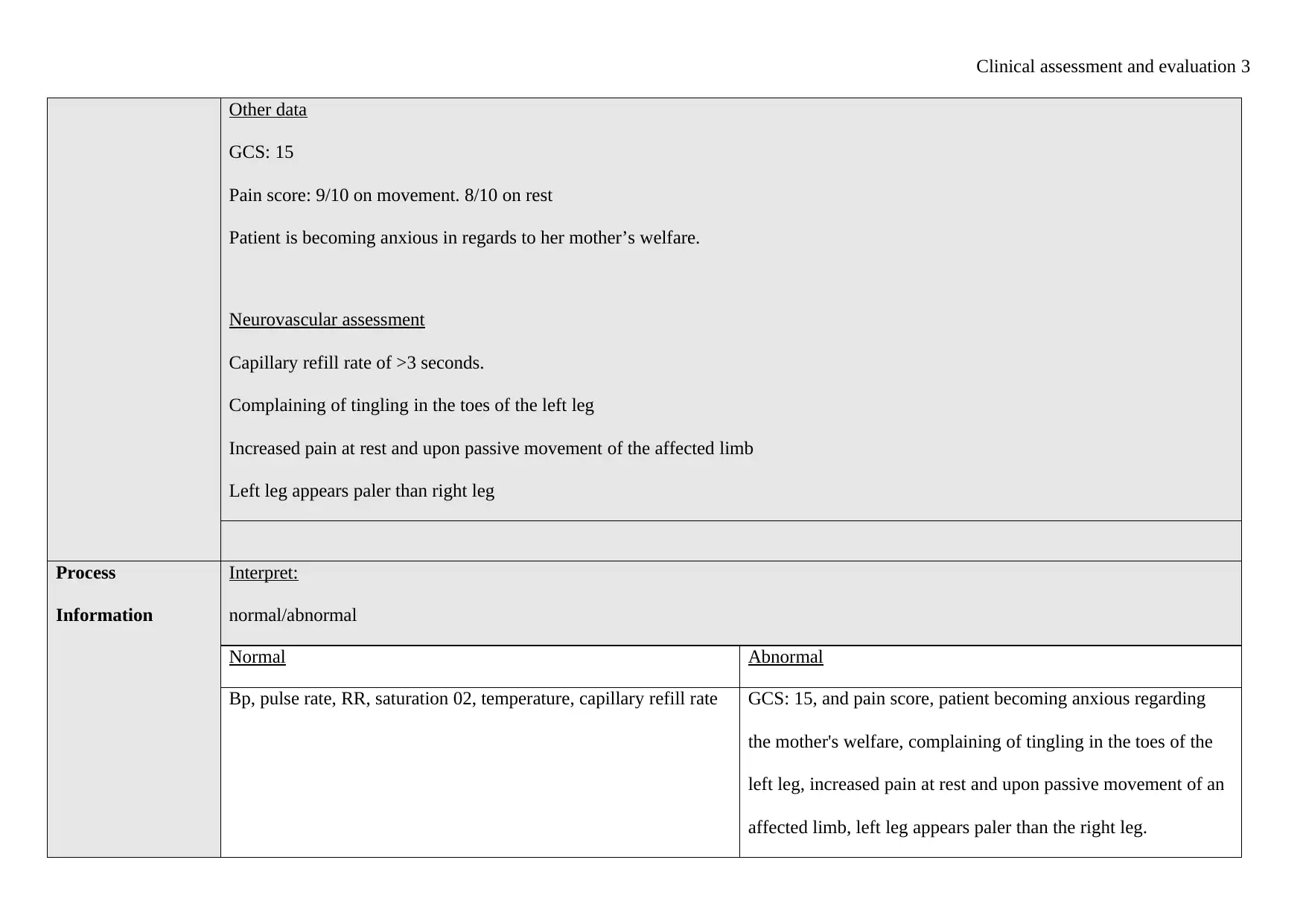
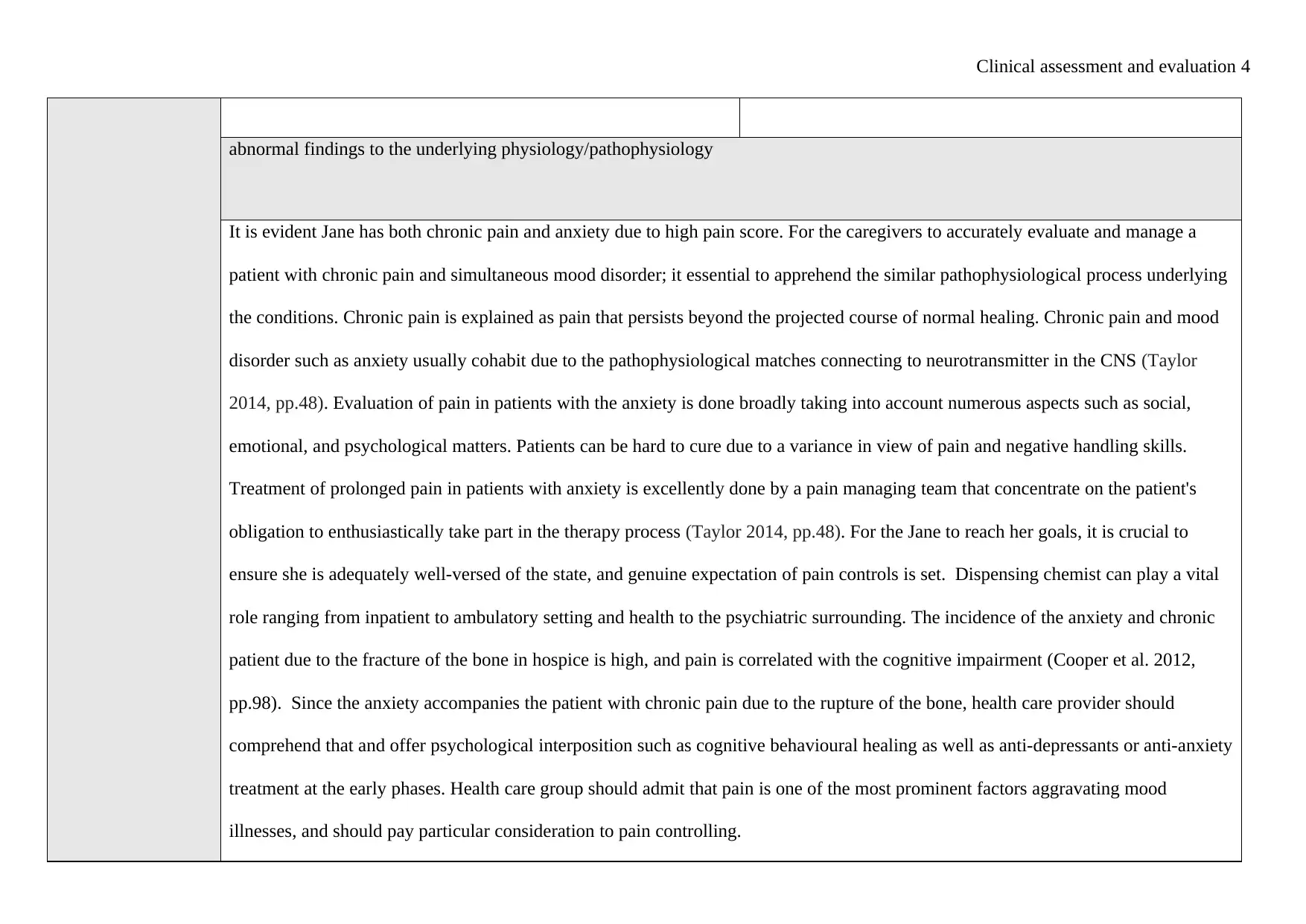
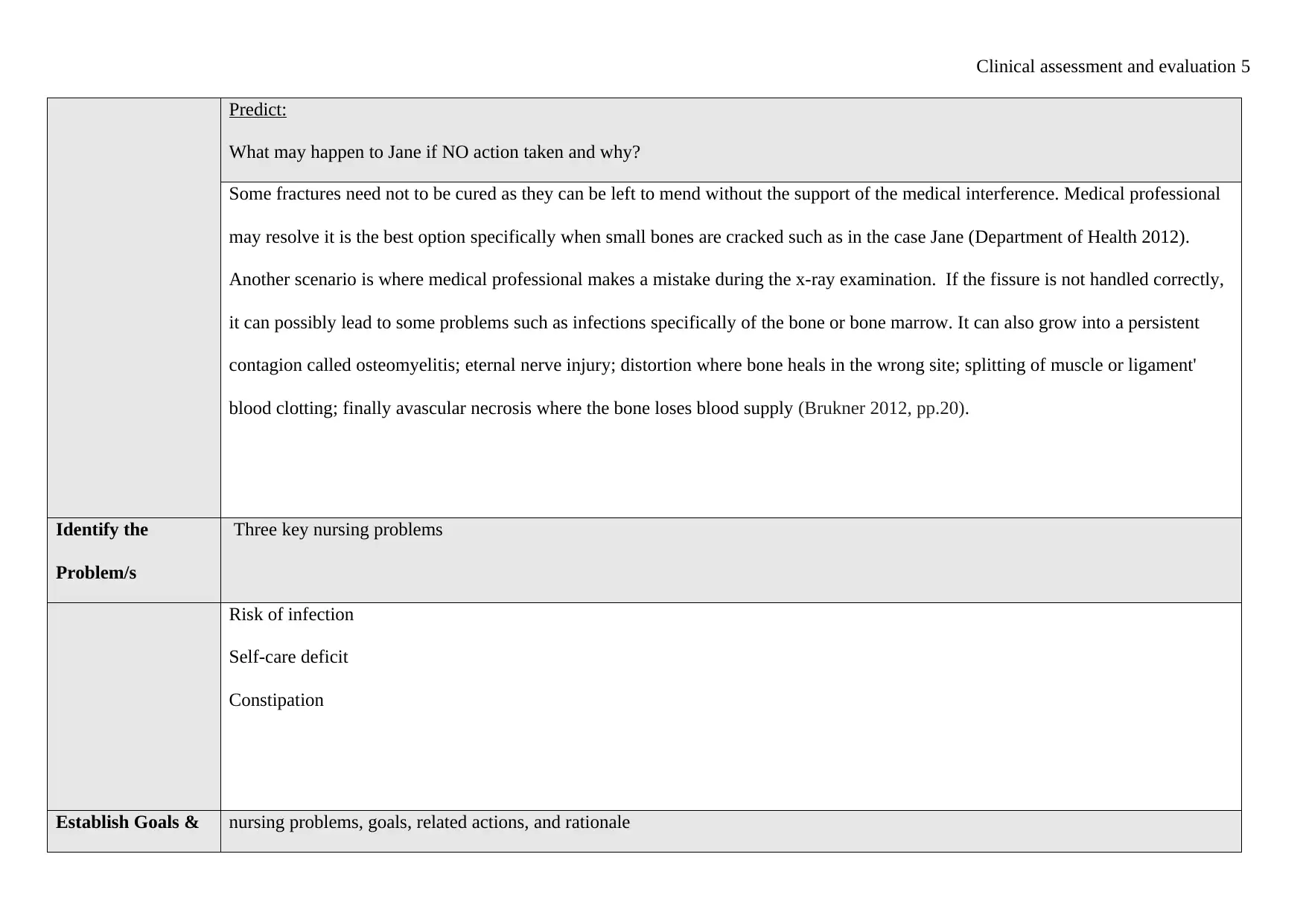
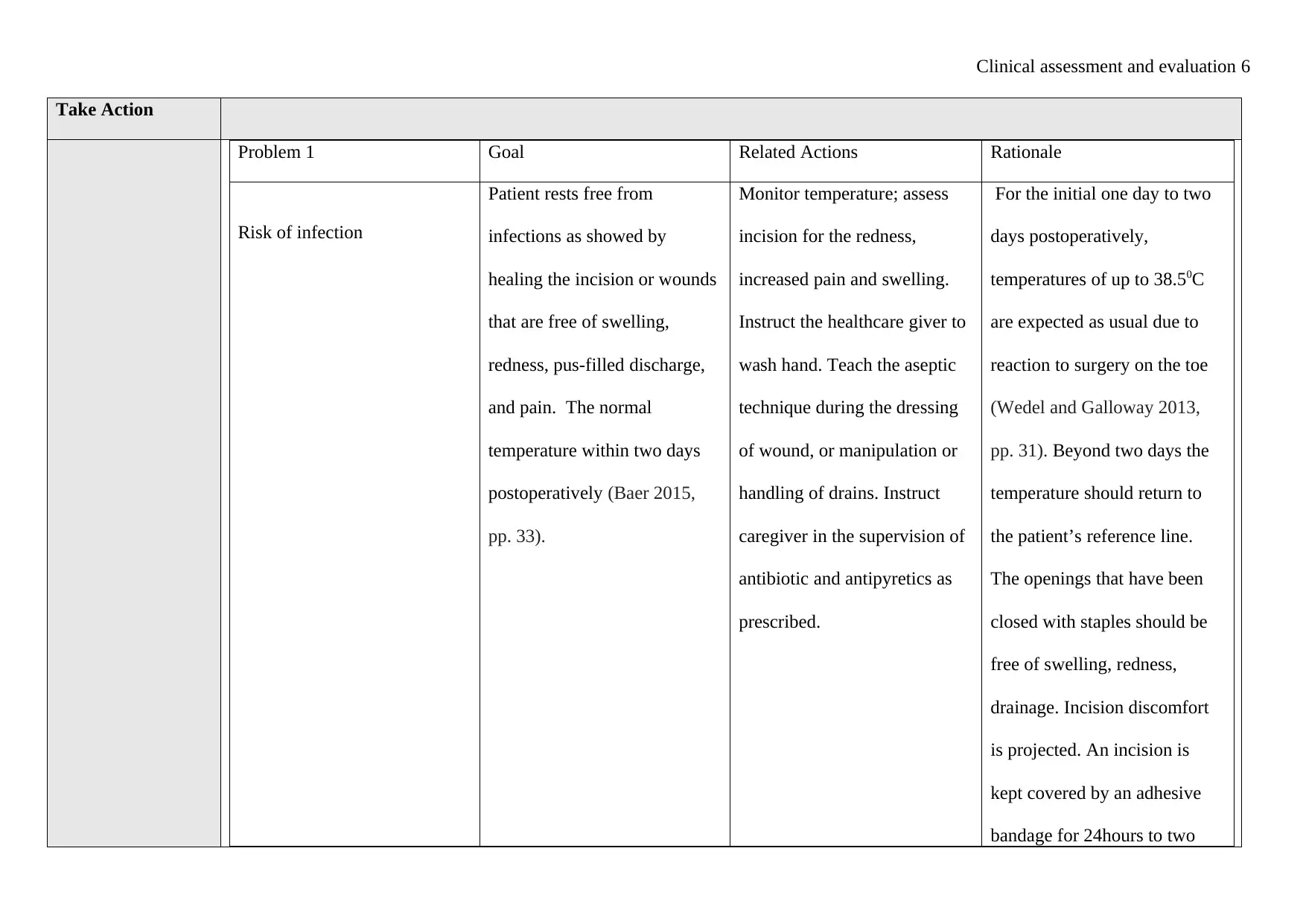
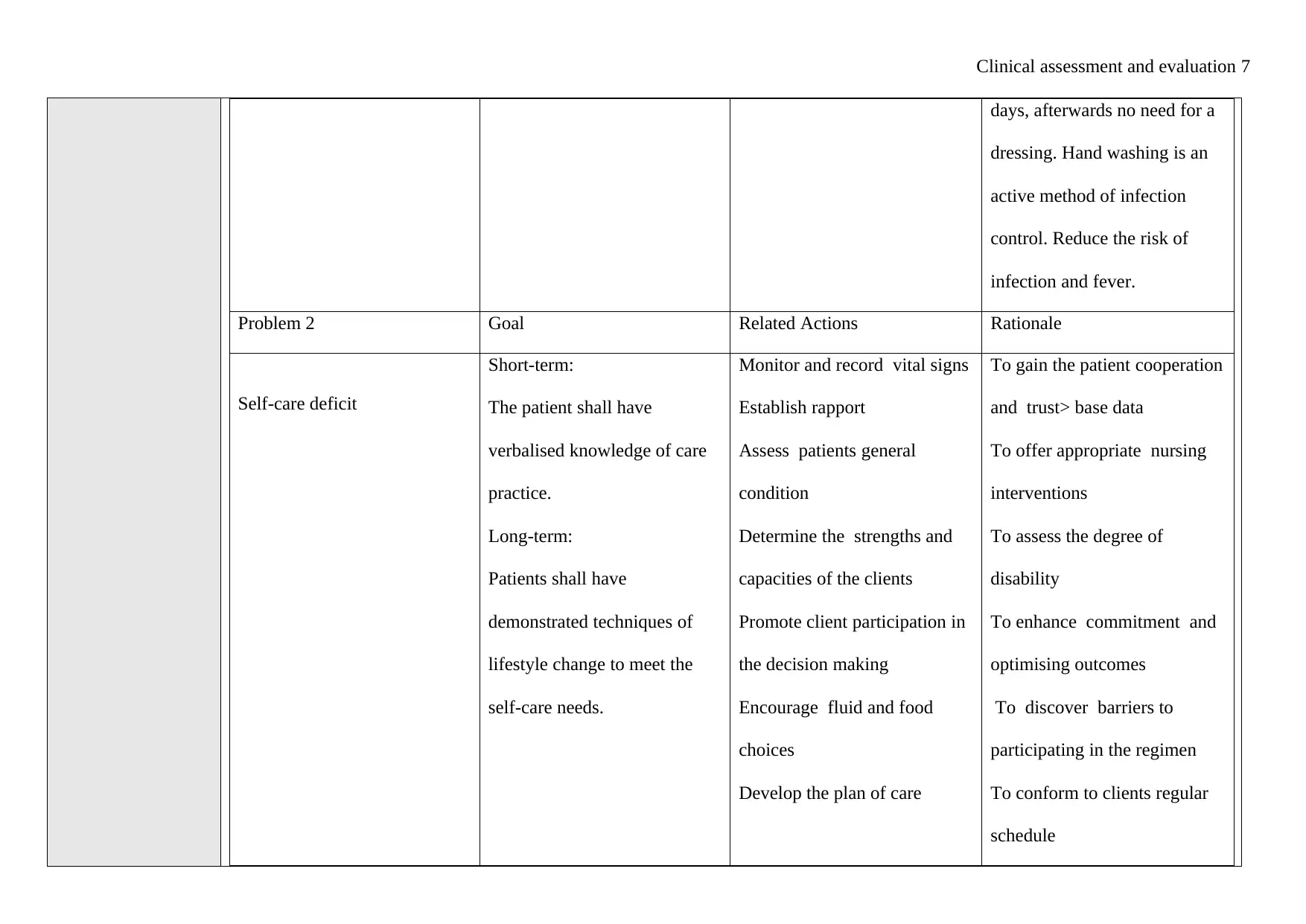
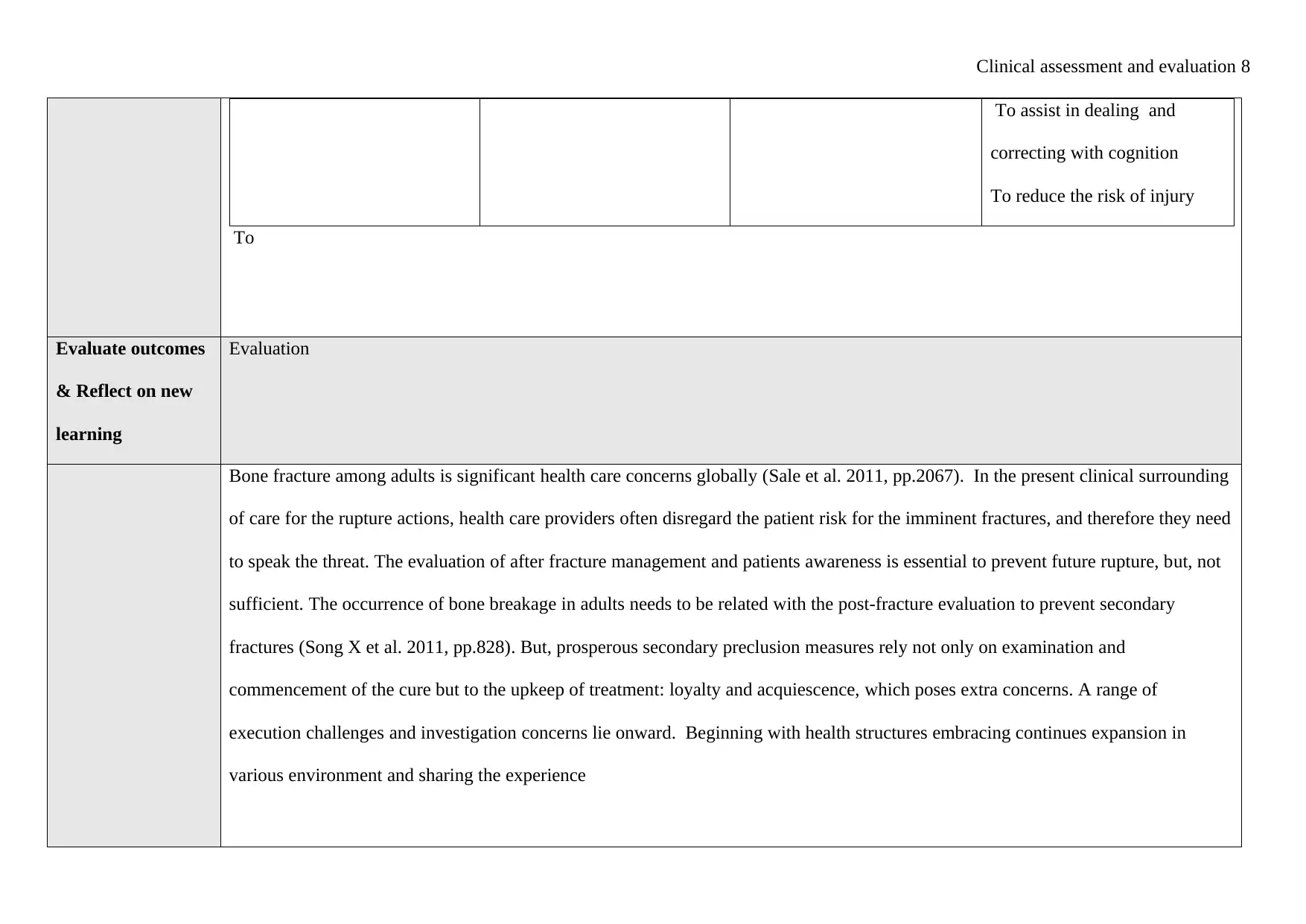
This case study presents a clinical assessment and evaluation of Miss Jane Green, a 30-year-old female admitted to the ward after being hit by a car, resulting in a left lower leg fracture. The assessment includes subjective data, such as the patient's concerns about her mother with dementia, and objective data, including vital signs, pain score, and neurovascular assessment. The analysis interprets normal and abnormal findings, relating them to underlying pathophysiology, particularly chronic pain and anxiety. It predicts potential negative outcomes if no action is taken and identifies key nursing problems like risk of infection, self-care deficit, and constipation. The study establishes goals and outlines related nursing actions with rationales, focusing on monitoring, infection control, and promoting self-care. The evaluation reflects on new learning and the importance of post-fracture management and patient awareness to prevent future fractures. The document concludes with a list of references.
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.