CNA253 AT3: Scenario-Based Nursing Diagnosis and Care Plan
VerifiedAdded on 2023/04/23
|5
|1629
|53
Practical Assignment
AI Summary
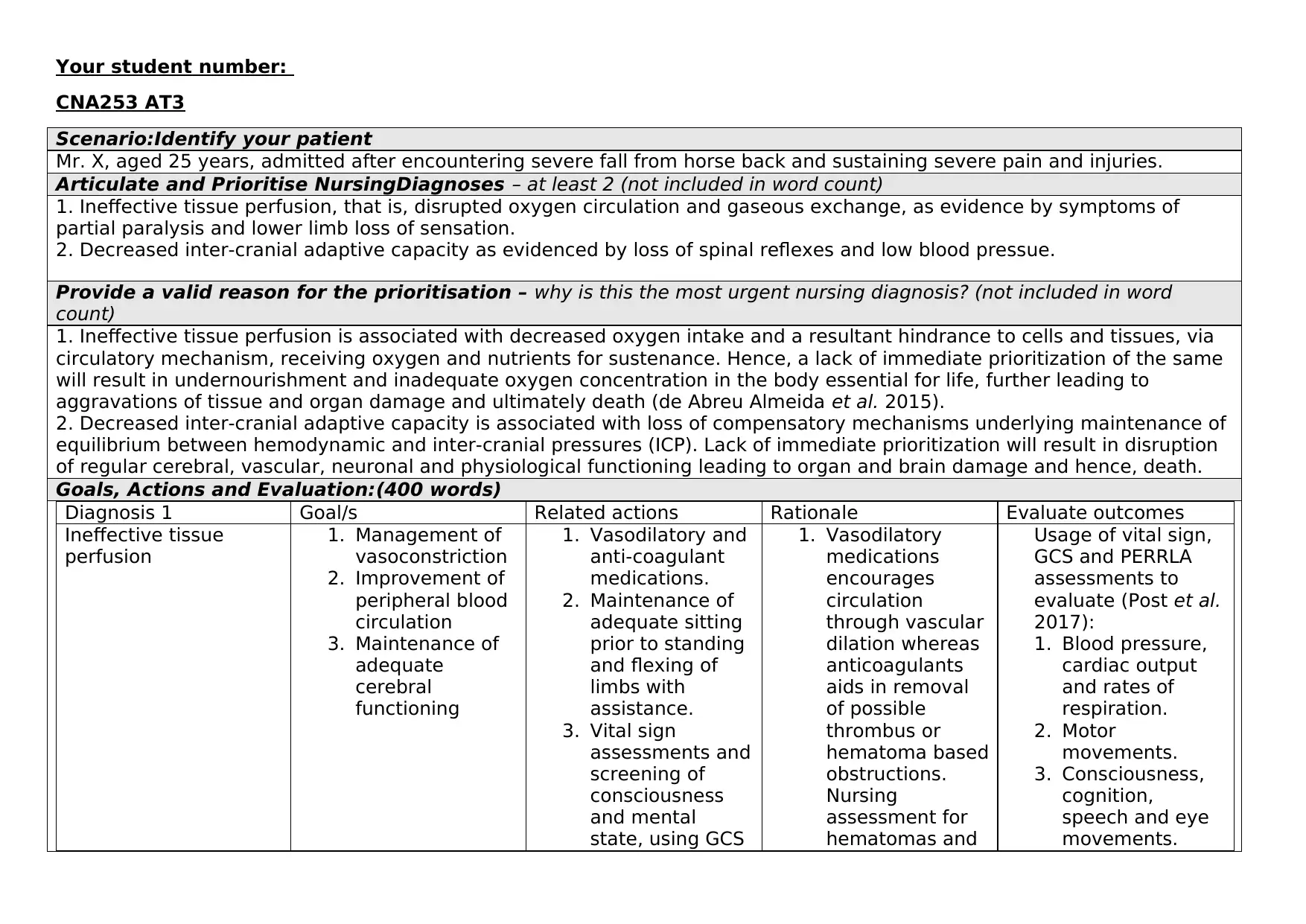
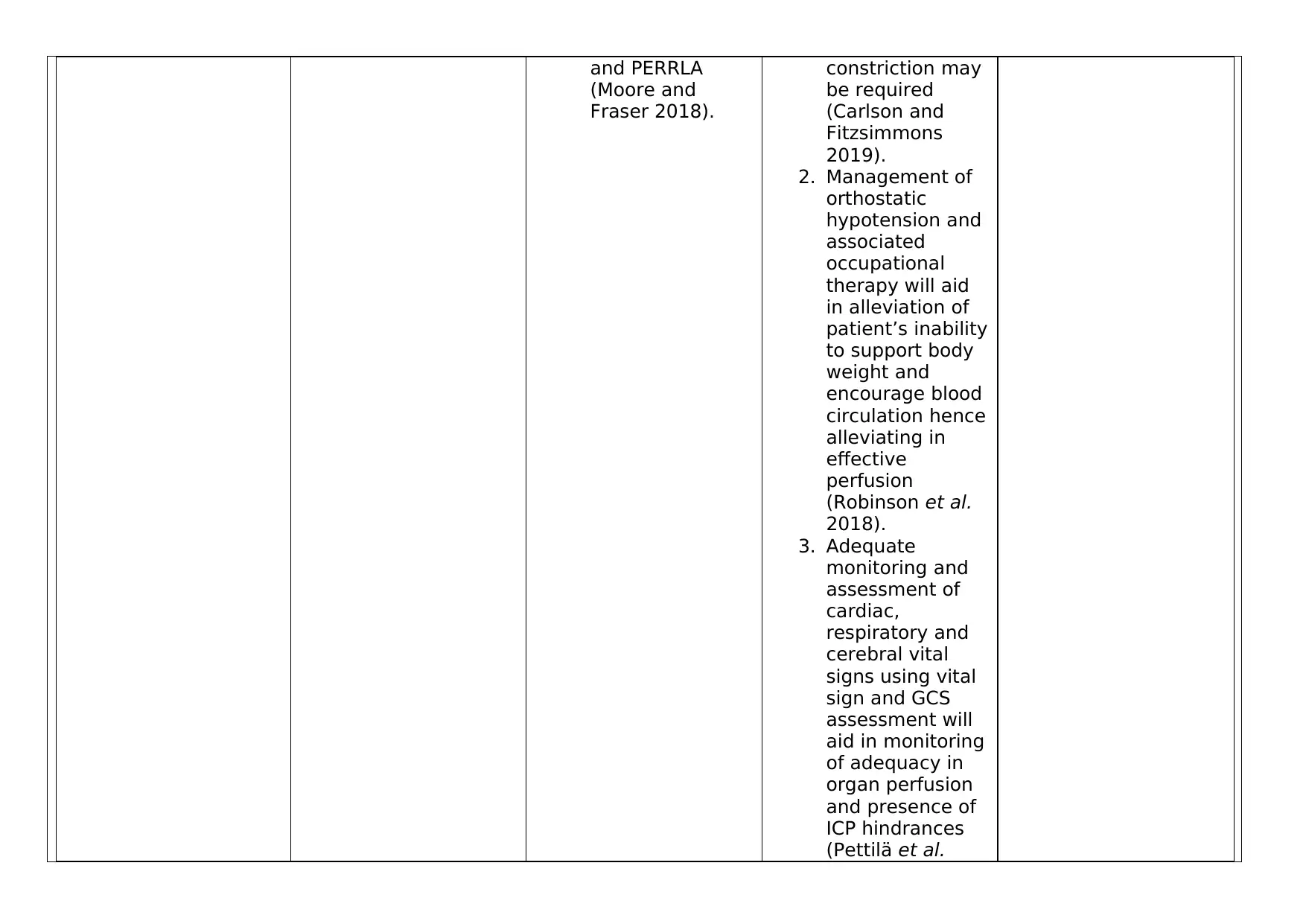
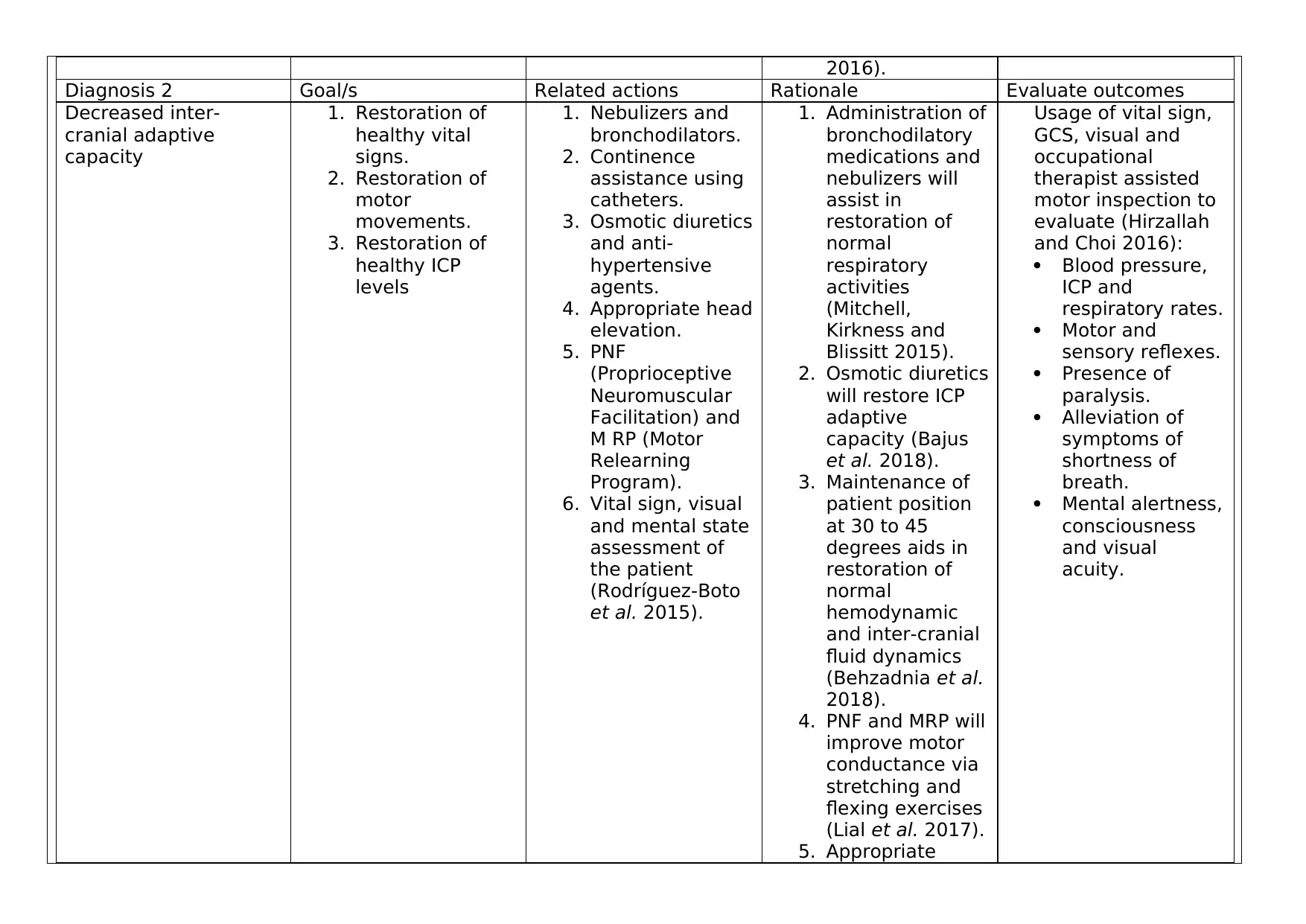
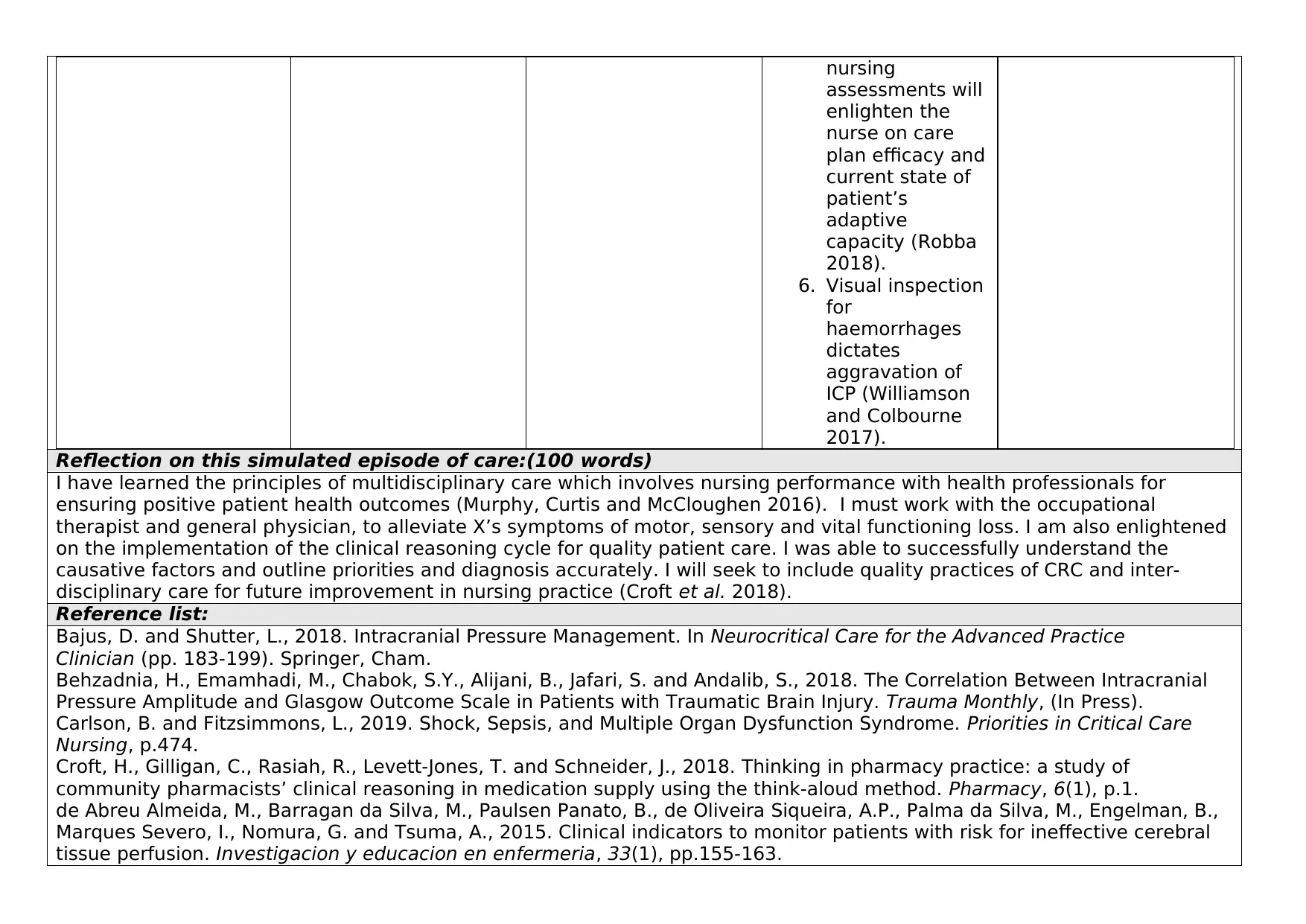
This assignment details a nursing care plan for a 25-year-old male, Mr. X, admitted after a severe fall from a horse. The student identifies and prioritizes two nursing diagnoses: Ineffective tissue perfusion and Decreased intracranial adaptive capacity. Justifications for prioritization are provided, emphasizing the life-threatening nature of these conditions. The assignment outlines specific goals, related nursing actions with rationales, and evaluation methods for each diagnosis, demonstrating the application of the clinical reasoning cycle. The care plan includes interventions such as medication management, monitoring vital signs, and occupational therapy. The student reflects on the simulated episode, highlighting the importance of multidisciplinary care and clinical reasoning in achieving positive patient outcomes. The assignment adheres to the rubric requirements, utilizing current scholarly literature and textbooks to support clinical decisions and substantiating statements. References are provided to support the evidence-based practice.
1 out of 5

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.