Clinical Pathway: Colon Cancer - Assessment, Treatment, and Discharge
VerifiedAdded on 2022/09/14
|10
|1314
|14
Report
AI Summary
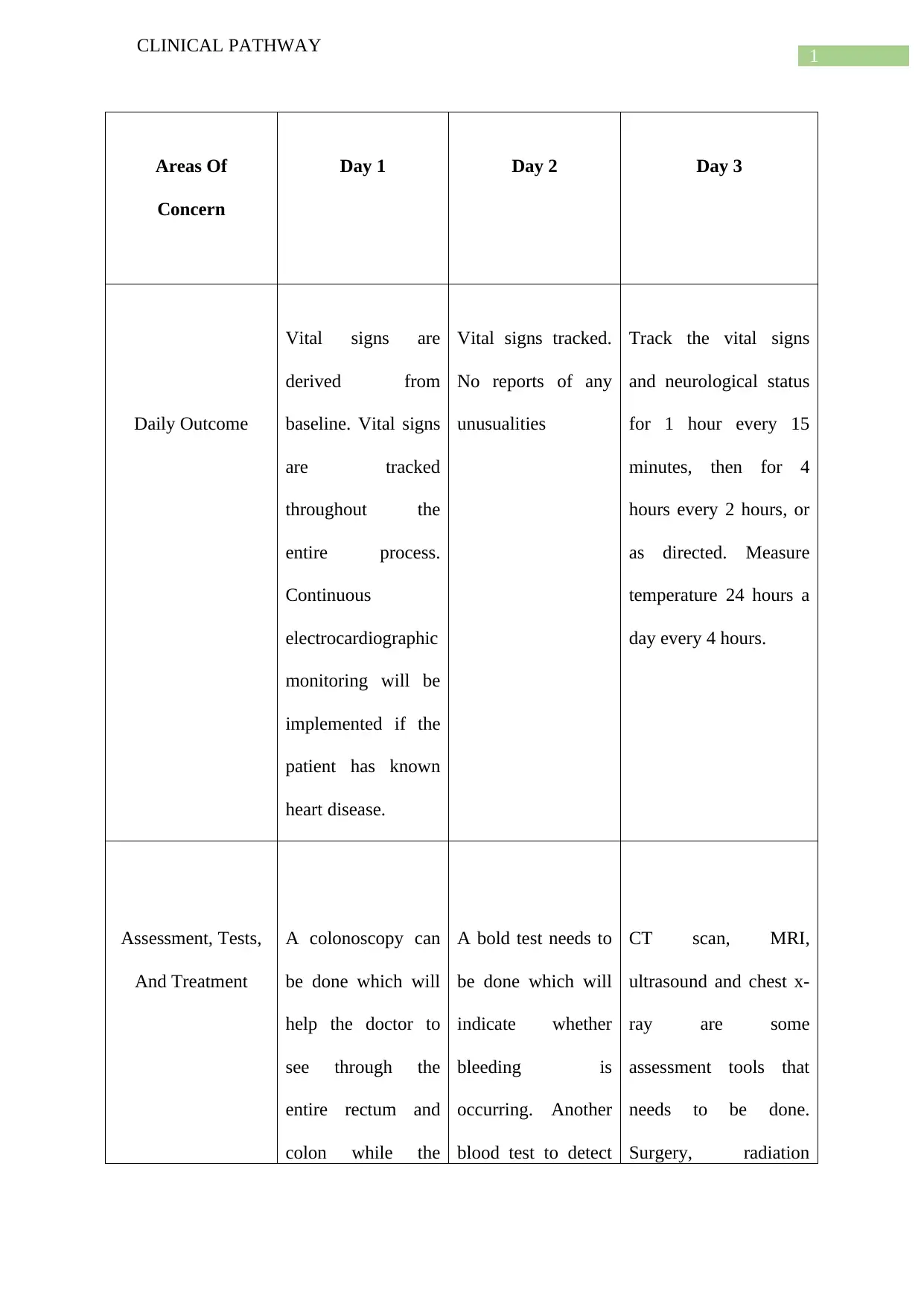
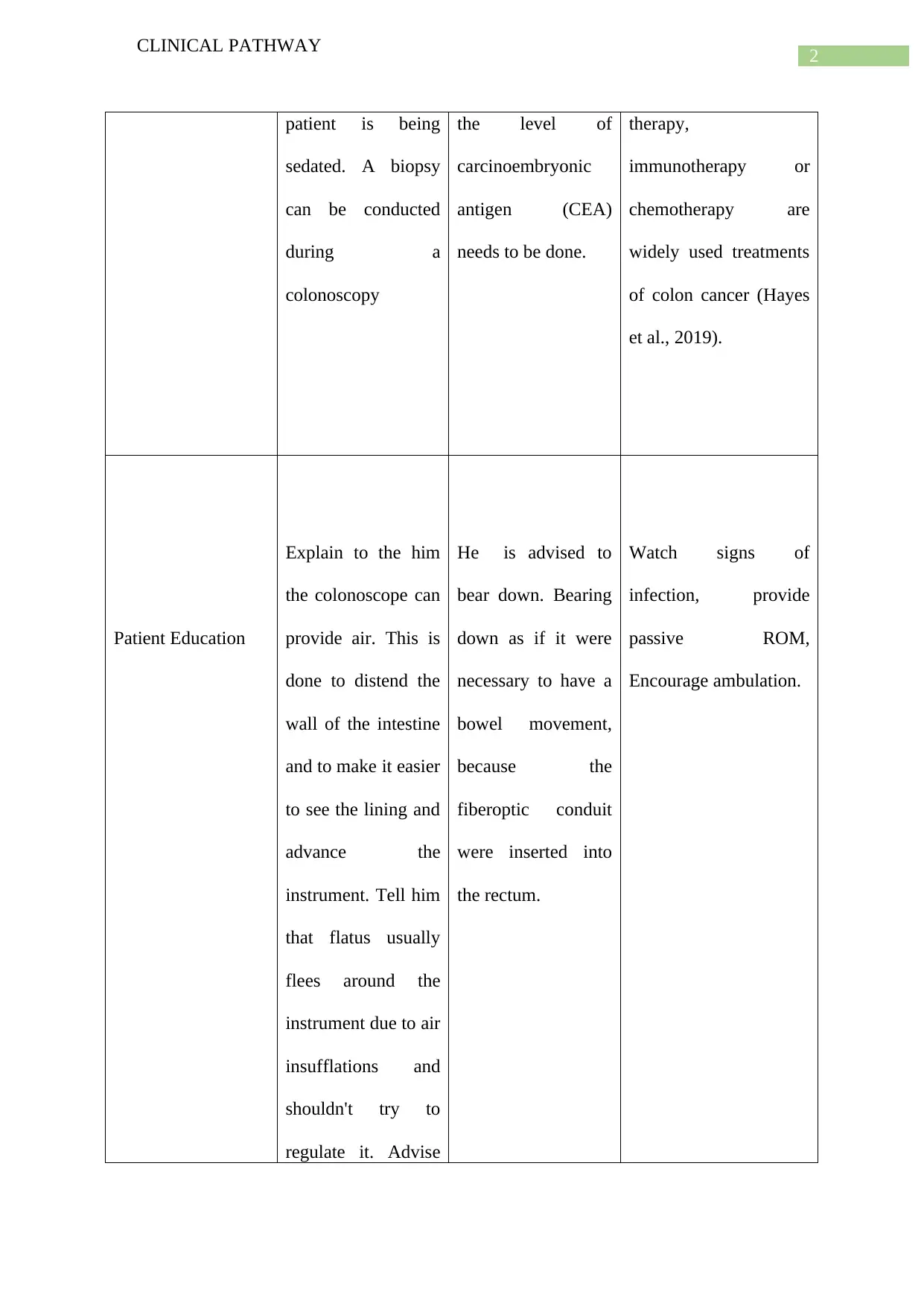
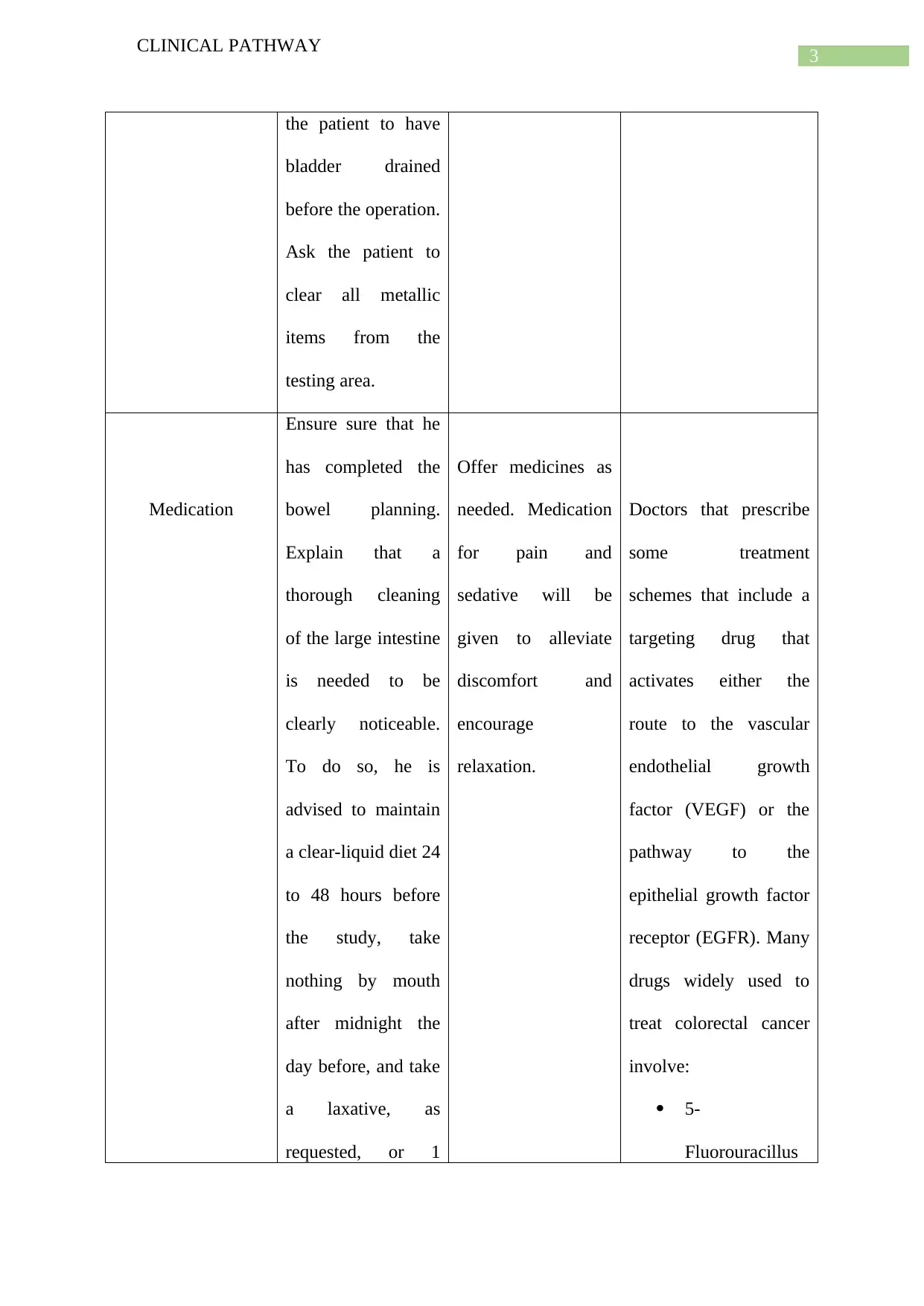
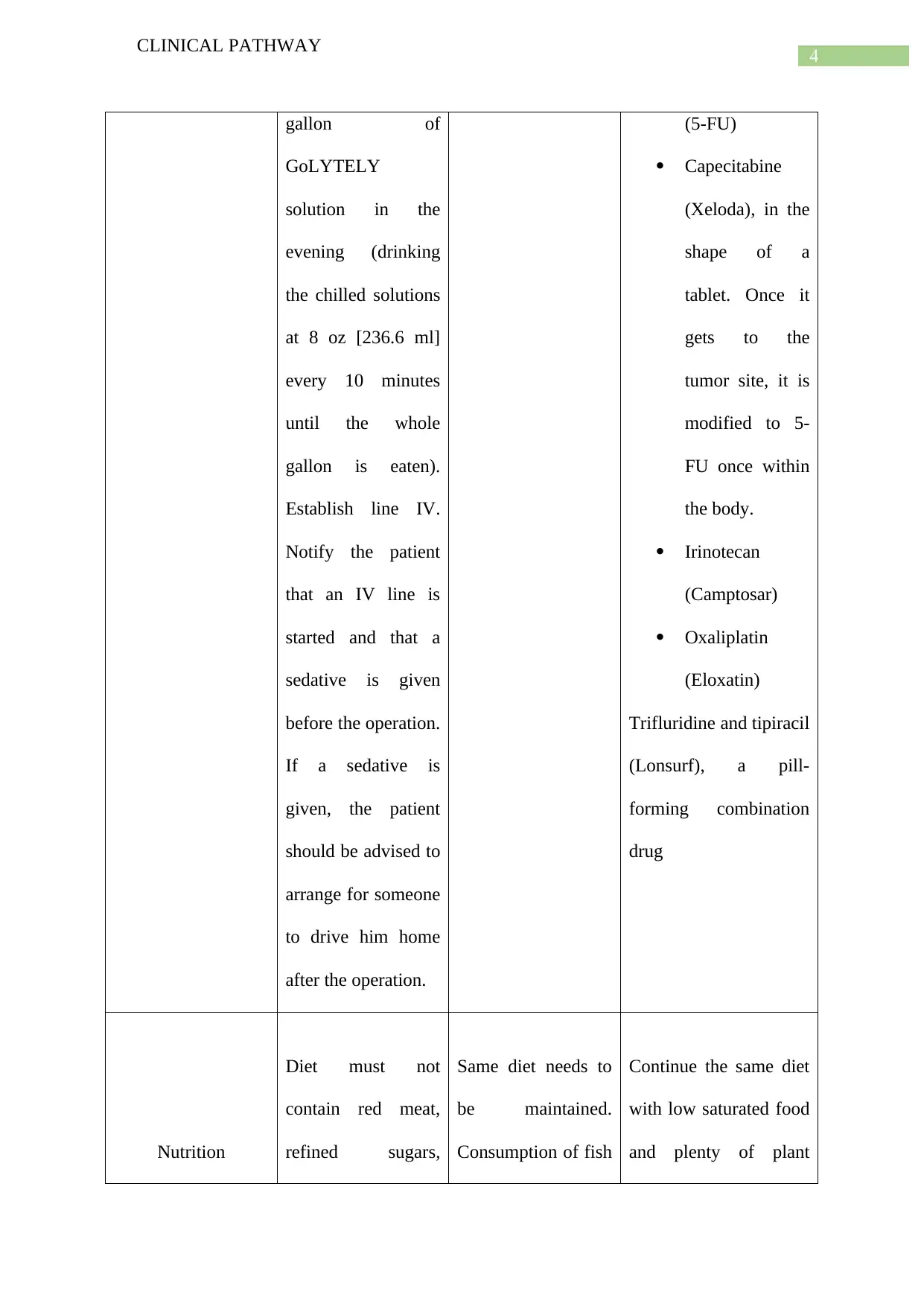
This clinical pathway report details the comprehensive management of colon cancer, encompassing various aspects of patient care from initial assessment to discharge planning. The report outlines the areas of concern, including vital signs monitoring, which is crucial throughout the entire process, along with assessment tools such as colonoscopy, blood tests, and imaging techniques like CT scans. It also discusses treatment options, including surgery, radiation therapy, immunotherapy, and chemotherapy. Patient education is emphasized, covering pre- and post-procedure instructions, medication administration, and dietary recommendations, such as avoiding red meat, refined sugars, and alcohol, and increasing plant-derived foods. Psychological support is addressed, acknowledging the psychosocial challenges faced by cancer survivors. Finally, the discharge plan is detailed, including follow-up care, medication instructions, and lifestyle modifications. The report references multiple studies supporting the described clinical pathway. This clinical pathway provides a structured approach to managing colon cancer, ensuring comprehensive and coordinated patient care.

1 out of 10


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.