Assessment 1 Essay: Community Health and Disease Prevention PUBH6006
VerifiedAdded on 2022/08/21
|16
|3395
|13
Essay
AI Summary
This essay, submitted by a student, analyzes community health and disease prevention strategies, particularly concerning Type 2 Diabetes Mellitus (T2DM). The essay begins by examining the prevalence of T2DM and its impact on various populations, especially Indigenous communities in Australia. It then explores the application of Laverack’s community-based health promotion ladder, focusing on community-based education, interactive community sessions, and special awareness campaigns for Aboriginal populations. The second part of the essay delves into capacity building and empowerment within communities, discussing key domains like learning opportunities, resource mobilization, leadership, and participatory decision-making. Finally, the essay applies the Health Belief Model (HBM) to motivate and educate individuals about T2DM prevention, analyzing its components and limitations in the context of social determinants of health. The assignment aims to demonstrate an understanding of community health principles and the application of various models to promote health awareness and disease prevention.

Running head: ASSESSMENT 1
Assessment 1
Name of the Student
Name of the University
Author Note
Assessment 1
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
ASSESSMENT 1
Introduction
According to the data reported in the National Health Survey conducted by the
Australian Government Department of Health (2016), nearly 85% of people who are
diagnosed with diabetes in Australia suffer from Type 2 Diabetes Mellitus (T2DM) and the
estimated population is over 1000000. Indigenous population in Australia like the aboriginals
and Torres Strait Islanders are more vulnerable towards developing this disease condition
(Australian Government Department of Health, 2016). The following essay aims to explore
the connection between the communities and the healthcare professionals towards promoting
disease empowerment with the help of community-based action. In doing so, the essay will
analyse three important steps of Laveracks community-based health promotion ladder for
promoting health awareness for T2DM. Second part of the assignment will analyse different
theories and models related to health promotion and practice. In the third and last of part of
the assignment, link between the capacity building and empowerment will be established
under the light of the Health Belief Model.
Part 1
The self-reported data published by the Australian Institute of Health Welfare
(AIHW) (2019) estimated 1.2 million (6%) Australian adults suffer from diabetes. Type 2
diabetes mellitus (T2DM), accounts for over half of the diabetes related deaths. Socio-
economic disadvantage is associated with higher level of diabetes prevalence along with
higher rates of hospitalization and death. Socio-economic disadvantage increase the
vulnerability of developing T2DM. T2DM is commonly known as metabolic disease that
leads to increase in the level of blood glucose resulting in the development of heart disease,
stroke, diabetic foot ulcers, retinoblastoma and renal failure (Kolb & Martin, 2017). The main
reason behind the development of diabetes and the associated co-morbidities include
ASSESSMENT 1
Introduction
According to the data reported in the National Health Survey conducted by the
Australian Government Department of Health (2016), nearly 85% of people who are
diagnosed with diabetes in Australia suffer from Type 2 Diabetes Mellitus (T2DM) and the
estimated population is over 1000000. Indigenous population in Australia like the aboriginals
and Torres Strait Islanders are more vulnerable towards developing this disease condition
(Australian Government Department of Health, 2016). The following essay aims to explore
the connection between the communities and the healthcare professionals towards promoting
disease empowerment with the help of community-based action. In doing so, the essay will
analyse three important steps of Laveracks community-based health promotion ladder for
promoting health awareness for T2DM. Second part of the assignment will analyse different
theories and models related to health promotion and practice. In the third and last of part of
the assignment, link between the capacity building and empowerment will be established
under the light of the Health Belief Model.
Part 1
The self-reported data published by the Australian Institute of Health Welfare
(AIHW) (2019) estimated 1.2 million (6%) Australian adults suffer from diabetes. Type 2
diabetes mellitus (T2DM), accounts for over half of the diabetes related deaths. Socio-
economic disadvantage is associated with higher level of diabetes prevalence along with
higher rates of hospitalization and death. Socio-economic disadvantage increase the
vulnerability of developing T2DM. T2DM is commonly known as metabolic disease that
leads to increase in the level of blood glucose resulting in the development of heart disease,
stroke, diabetic foot ulcers, retinoblastoma and renal failure (Kolb & Martin, 2017). The main
reason behind the development of diabetes and the associated co-morbidities include
2
ASSESSMENT 1
unhealthy lifestyle conditions like over-eating, inclination towards junk food, sedentary
lifestyle, substance abuse and high-level of stress. All these factors are regarded as
modifiable factors (Kolb & Martin, 2017). Reddy (2017) stated that proper education and
awareness about obesity and pre-diabetic condition and other modifiable risks factors are
helpful for the effective prevention of T2DM.
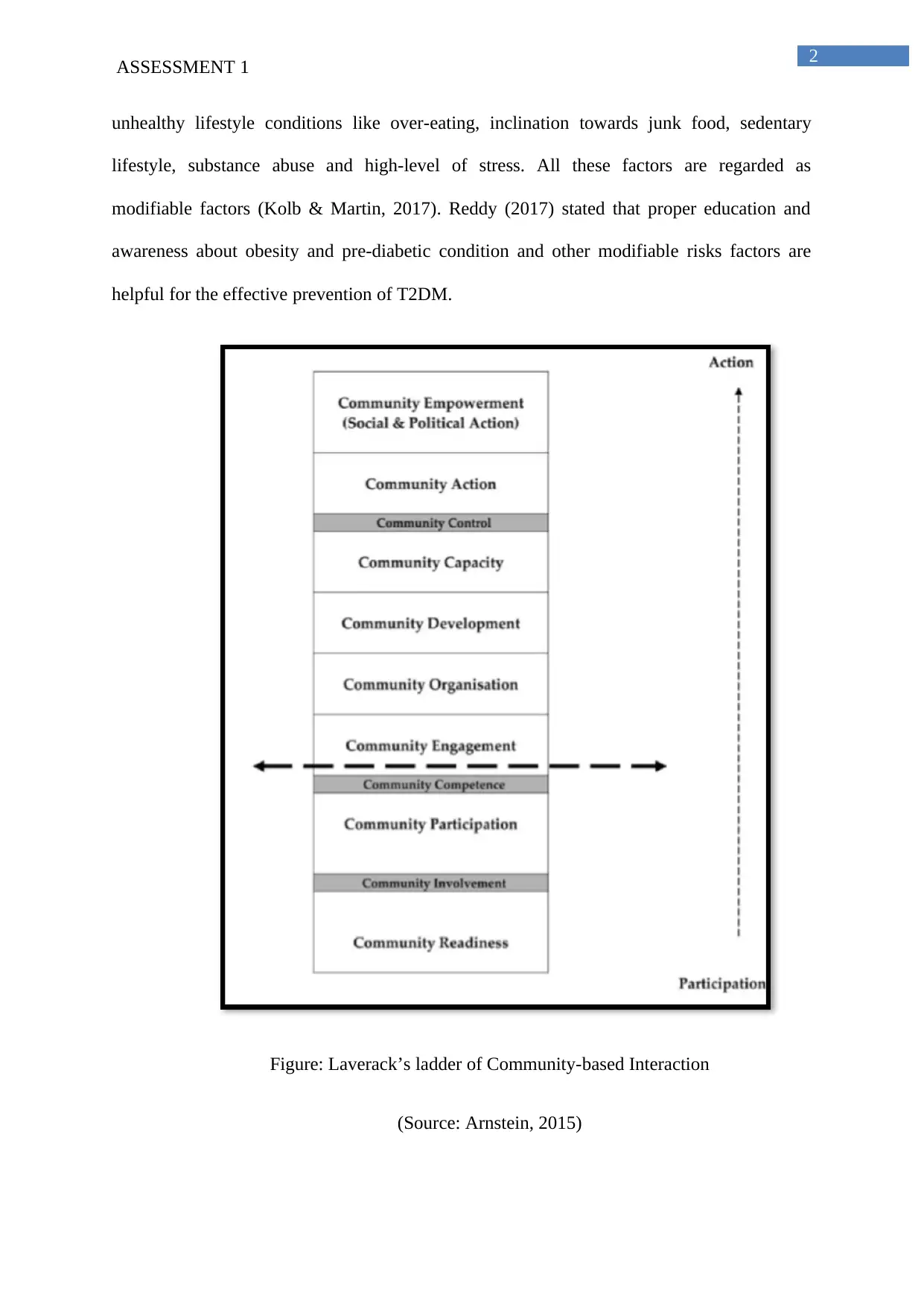
Figure: Laverack’s ladder of Community-based Interaction
(Source: Arnstein, 2015)
ASSESSMENT 1
unhealthy lifestyle conditions like over-eating, inclination towards junk food, sedentary
lifestyle, substance abuse and high-level of stress. All these factors are regarded as
modifiable factors (Kolb & Martin, 2017). Reddy (2017) stated that proper education and
awareness about obesity and pre-diabetic condition and other modifiable risks factors are
helpful for the effective prevention of T2DM.
Figure: Laverack’s ladder of Community-based Interaction
(Source: Arnstein, 2015)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
ASSESSMENT 1
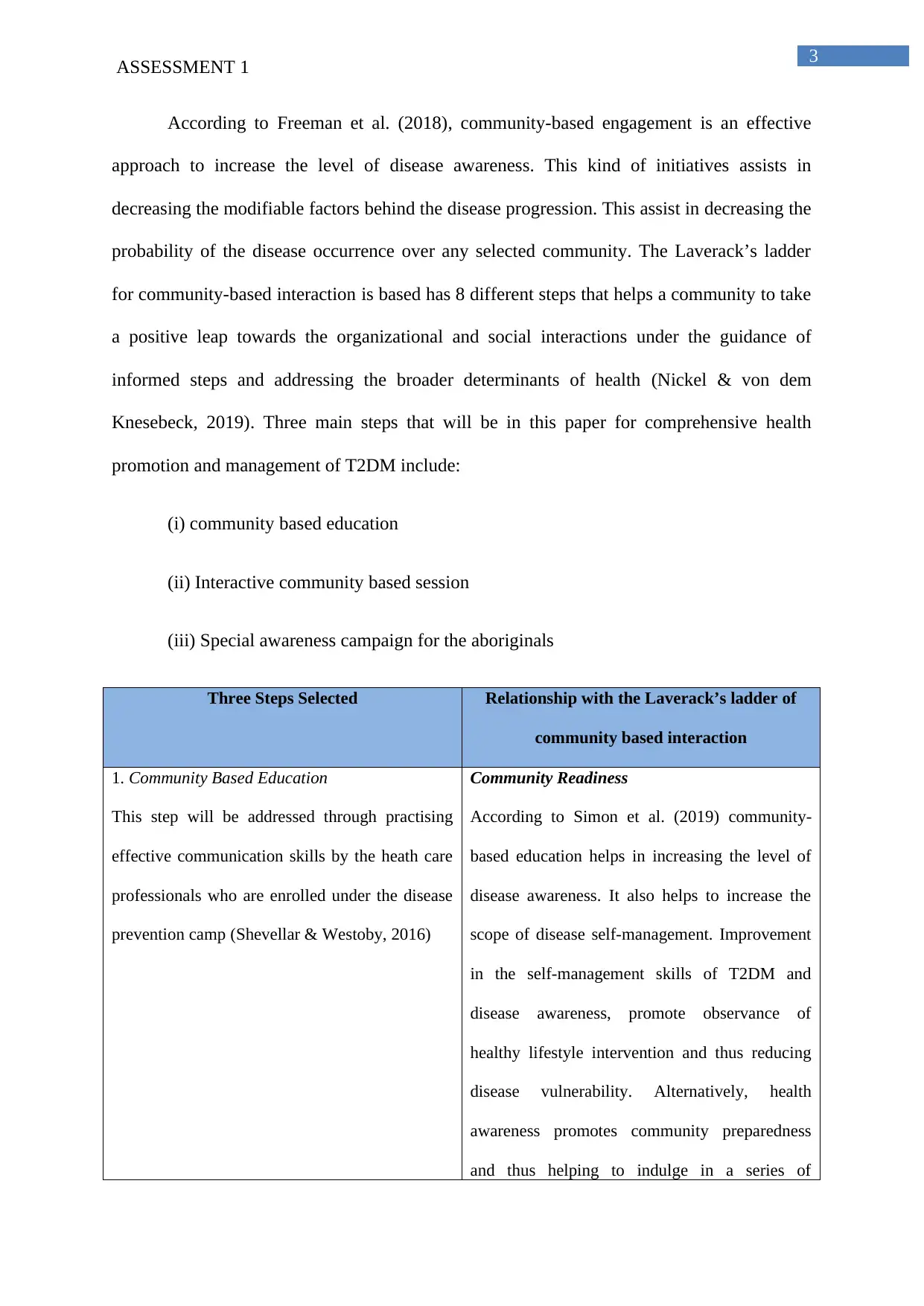
According to Freeman et al. (2018), community-based engagement is an effective
approach to increase the level of disease awareness. This kind of initiatives assists in
decreasing the modifiable factors behind the disease progression. This assist in decreasing the
probability of the disease occurrence over any selected community. The Laverack’s ladder
for community-based interaction is based has 8 different steps that helps a community to take
a positive leap towards the organizational and social interactions under the guidance of
informed steps and addressing the broader determinants of health (Nickel & von dem
Knesebeck, 2019). Three main steps that will be in this paper for comprehensive health
promotion and management of T2DM include:
(i) community based education
(ii) Interactive community based session
(iii) Special awareness campaign for the aboriginals
Three Steps Selected Relationship with the Laverack’s ladder of
community based interaction
1. Community Based Education
This step will be addressed through practising
effective communication skills by the heath care
professionals who are enrolled under the disease
prevention camp (Shevellar & Westoby, 2016)
Community Readiness
According to Simon et al. (2019) community-
based education helps in increasing the level of
disease awareness. It also helps to increase the
scope of disease self-management. Improvement
in the self-management skills of T2DM and
disease awareness, promote observance of
healthy lifestyle intervention and thus reducing
disease vulnerability. Alternatively, health
awareness promotes community preparedness
and thus helping to indulge in a series of
ASSESSMENT 1
According to Freeman et al. (2018), community-based engagement is an effective
approach to increase the level of disease awareness. This kind of initiatives assists in
decreasing the modifiable factors behind the disease progression. This assist in decreasing the
probability of the disease occurrence over any selected community. The Laverack’s ladder
for community-based interaction is based has 8 different steps that helps a community to take
a positive leap towards the organizational and social interactions under the guidance of
informed steps and addressing the broader determinants of health (Nickel & von dem
Knesebeck, 2019). Three main steps that will be in this paper for comprehensive health
promotion and management of T2DM include:
(i) community based education
(ii) Interactive community based session
(iii) Special awareness campaign for the aboriginals
Three Steps Selected Relationship with the Laverack’s ladder of
community based interaction
1. Community Based Education
This step will be addressed through practising
effective communication skills by the heath care
professionals who are enrolled under the disease
prevention camp (Shevellar & Westoby, 2016)
Community Readiness
According to Simon et al. (2019) community-
based education helps in increasing the level of
disease awareness. It also helps to increase the
scope of disease self-management. Improvement
in the self-management skills of T2DM and
disease awareness, promote observance of
healthy lifestyle intervention and thus reducing
disease vulnerability. Alternatively, health
awareness promotes community preparedness
and thus helping to indulge in a series of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
ASSESSMENT 1
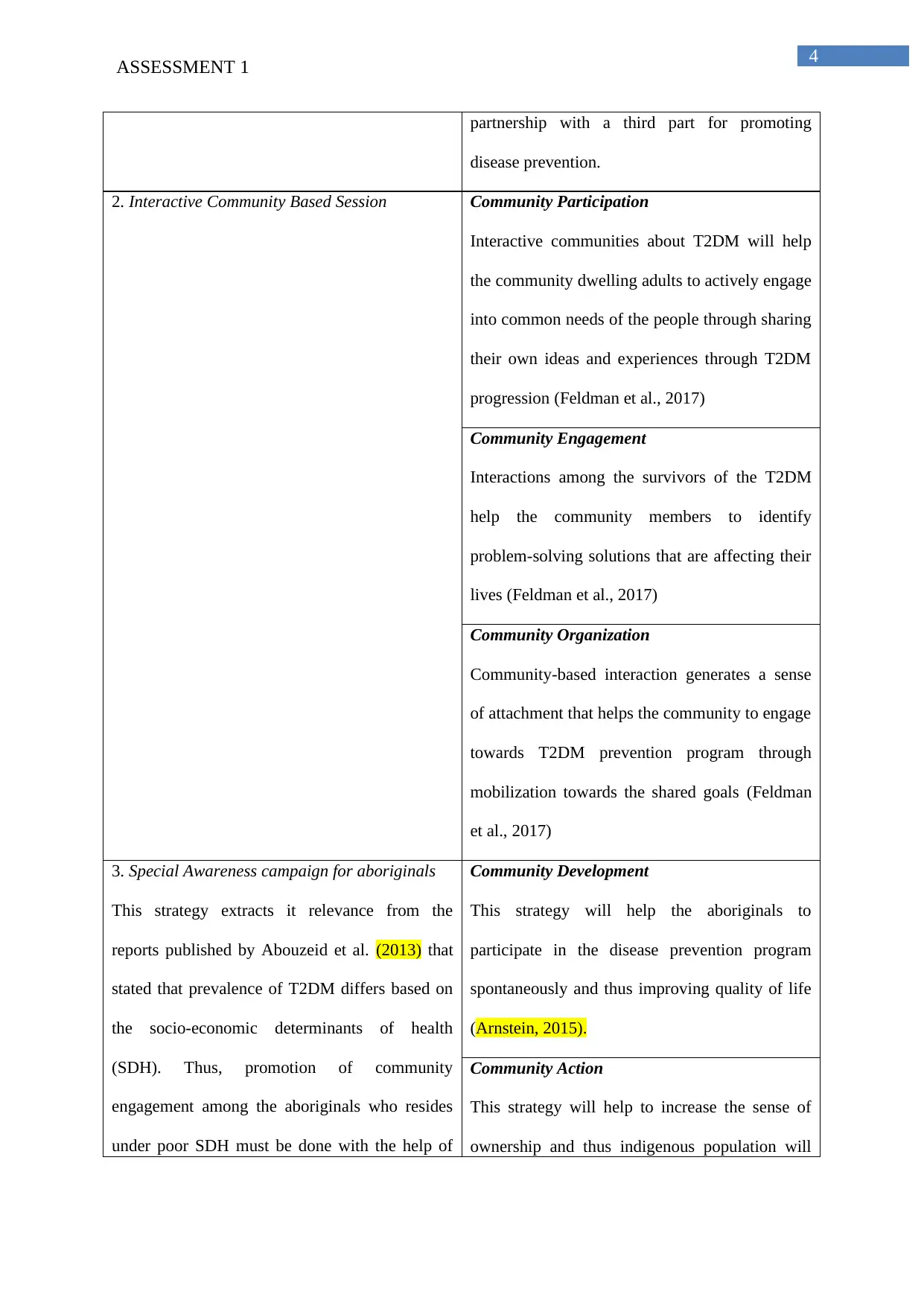
partnership with a third part for promoting
disease prevention.
2. Interactive Community Based Session Community Participation
Interactive communities about T2DM will help
the community dwelling adults to actively engage
into common needs of the people through sharing
their own ideas and experiences through T2DM
progression (Feldman et al., 2017)
Community Engagement
Interactions among the survivors of the T2DM
help the community members to identify
problem-solving solutions that are affecting their
lives (Feldman et al., 2017)
Community Organization
Community-based interaction generates a sense
of attachment that helps the community to engage
towards T2DM prevention program through
mobilization towards the shared goals (Feldman
et al., 2017)
3. Special Awareness campaign for aboriginals
This strategy extracts it relevance from the
reports published by Abouzeid et al. (2013) that
stated that prevalence of T2DM differs based on
the socio-economic determinants of health
(SDH). Thus, promotion of community
engagement among the aboriginals who resides
under poor SDH must be done with the help of
Community Development
This strategy will help the aboriginals to
participate in the disease prevention program
spontaneously and thus improving quality of life
(Arnstein, 2015).
Community Action
This strategy will help to increase the sense of
ownership and thus indigenous population will
ASSESSMENT 1
partnership with a third part for promoting
disease prevention.
2. Interactive Community Based Session Community Participation
Interactive communities about T2DM will help
the community dwelling adults to actively engage
into common needs of the people through sharing
their own ideas and experiences through T2DM
progression (Feldman et al., 2017)
Community Engagement
Interactions among the survivors of the T2DM
help the community members to identify
problem-solving solutions that are affecting their
lives (Feldman et al., 2017)
Community Organization
Community-based interaction generates a sense
of attachment that helps the community to engage
towards T2DM prevention program through
mobilization towards the shared goals (Feldman
et al., 2017)
3. Special Awareness campaign for aboriginals
This strategy extracts it relevance from the
reports published by Abouzeid et al. (2013) that
stated that prevalence of T2DM differs based on
the socio-economic determinants of health
(SDH). Thus, promotion of community
engagement among the aboriginals who resides
under poor SDH must be done with the help of
Community Development
This strategy will help the aboriginals to
participate in the disease prevention program
spontaneously and thus improving quality of life
(Arnstein, 2015).
Community Action
This strategy will help to increase the sense of
ownership and thus indigenous population will
5
ASSESSMENT 1
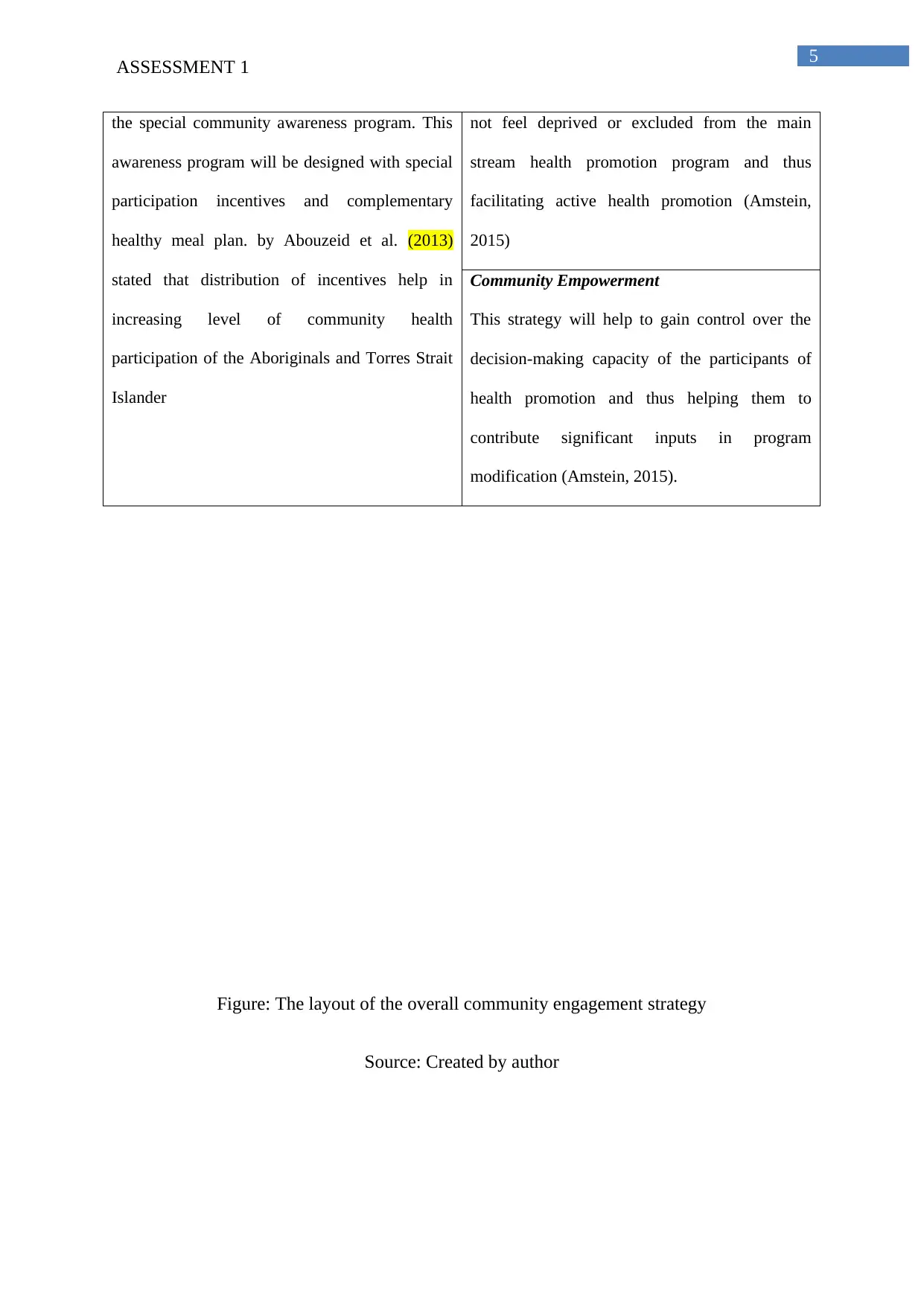
the special community awareness program. This
awareness program will be designed with special
participation incentives and complementary
healthy meal plan. by Abouzeid et al. (2013)
stated that distribution of incentives help in
increasing level of community health
participation of the Aboriginals and Torres Strait
Islander
not feel deprived or excluded from the main
stream health promotion program and thus
facilitating active health promotion (Amstein,
2015)
Community Empowerment
This strategy will help to gain control over the
decision-making capacity of the participants of
health promotion and thus helping them to
contribute significant inputs in program
modification (Amstein, 2015).
Figure: The layout of the overall community engagement strategy
Source: Created by author
ASSESSMENT 1
the special community awareness program. This
awareness program will be designed with special
participation incentives and complementary
healthy meal plan. by Abouzeid et al. (2013)
stated that distribution of incentives help in
increasing level of community health
participation of the Aboriginals and Torres Strait
Islander
not feel deprived or excluded from the main
stream health promotion program and thus
facilitating active health promotion (Amstein,
2015)
Community Empowerment
This strategy will help to gain control over the
decision-making capacity of the participants of
health promotion and thus helping them to
contribute significant inputs in program
modification (Amstein, 2015).
Figure: The layout of the overall community engagement strategy
Source: Created by author
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
ASSESSMENT 1
Part 2
According to Liberato et al. (2011), capacity building process under a community-
based intervention is the primary aim towards promoting disease awareness and prevention.
Liberato et al. (2011) are of the opinion that identification of different domains will help in
promoting comprehensive capacity building process and thus promoting community
development in health and social care. The 9 main domains identified by Liberato et al.
(2011) are learning opportunities and skills development”, “resource mobilization”,
“partnership/linkages/networking”, “leadership”, “participatory decision making”, “assets-
based approach”, “sense of community”, “communication”, and “development pathway”.
Community empowerment and ownership is defined as a process through which the
communities gain control over the resources that cast significant impact on their activities of
daily living and this also covers social determinants of health. The community empowerment
and other community-based practice have fine line of difference. The community
empowerment signifies the process of gaining power in order to improve participation in the
community dwelling adults in health-promotion (Lie, 2018). It is different from the concept
of capacity building that deals with the establishment of the assessment of community that
can be used for the disease prevention program (Lie, 2018).
Learning opportunities will deal with proper education about prognosis of T2M and
importance of healthy lifestyle interventions for reducing vulnerability of T2DM. Skill
development of T2DM management encompasses education towards importance of healthy
lifestyle habits like education about diet and physical activity. These health awareness
program will help to reduce the body mass index (BMI) thus helping to reduce the body
weight (American Diabetes Association, 2016). Resource mobilization signifies
comprehensive set of activities sue for securing additional resources for the development of
the community based healthcare program. Resource mobilization also helps in scanning for
ASSESSMENT 1
Part 2
According to Liberato et al. (2011), capacity building process under a community-
based intervention is the primary aim towards promoting disease awareness and prevention.
Liberato et al. (2011) are of the opinion that identification of different domains will help in
promoting comprehensive capacity building process and thus promoting community
development in health and social care. The 9 main domains identified by Liberato et al.
(2011) are learning opportunities and skills development”, “resource mobilization”,
“partnership/linkages/networking”, “leadership”, “participatory decision making”, “assets-
based approach”, “sense of community”, “communication”, and “development pathway”.
Community empowerment and ownership is defined as a process through which the
communities gain control over the resources that cast significant impact on their activities of
daily living and this also covers social determinants of health. The community empowerment
and other community-based practice have fine line of difference. The community
empowerment signifies the process of gaining power in order to improve participation in the
community dwelling adults in health-promotion (Lie, 2018). It is different from the concept
of capacity building that deals with the establishment of the assessment of community that
can be used for the disease prevention program (Lie, 2018).
Learning opportunities will deal with proper education about prognosis of T2M and
importance of healthy lifestyle interventions for reducing vulnerability of T2DM. Skill
development of T2DM management encompasses education towards importance of healthy
lifestyle habits like education about diet and physical activity. These health awareness
program will help to reduce the body mass index (BMI) thus helping to reduce the body
weight (American Diabetes Association, 2016). Resource mobilization signifies
comprehensive set of activities sue for securing additional resources for the development of
the community based healthcare program. Resource mobilization also helps in scanning for
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
ASSESSMENT 1
new opportunities for further exploration of the T2DM prevention program (Hills et al.,
2018). Lee (2020) stated that development of the social media competencies for
strengthening resource mobilization is helpful in improving the community based
intervention strategies towards effective disease prevention. Linkages/partnership and
networking will help in the establishment of synchronization with the stakeholders of the
community-base health and disease prevention camp for T2DM. Leadership is one o the
principal aspect behind the promotion of the community empowerment. Selection of efficient
leaders must be done among the community-participants and selected community leaders will
help in voicing the expectations and networking, two of the cope steps towards niche
building. Selection of the potential leaders within the community will help to increase the
sense of ownership. This kind of approach is helpful among the indigenous population as it
will help to promote the sense of empowerment under culturally competent healthcare
settings (Marmot, 2016). Participation of the end-users in disease prevention program and in
the decision-making process, helps in the promotion of empowerment. The participation in
the decision-making process will involve practice of physical exercise and execute of proper
anti-diabetic diet plan. This will help in the modification of the modifiable risk factors for
T2DM. The participation in the decision-making process will also involve regular check-up
of the blood glucose level under the community-based healthcare campaigns and under the
use of the glucometer. However, participation in the decision-making process must only be
done upon successful health awareness and health education (Kunz et al., 2017). The assets
based approach covers the assets of communities and its dwellers and mainly include lived
experiences. The incorporation of the lived experience will be done through exchange of the
thoughts and experiences under interactive sessions.. Communication among the community-
based participants will further help in the development of bond between them and thus
helping to promote empowerment and group-based health promotion activities. The initial
ASSESSMENT 1
new opportunities for further exploration of the T2DM prevention program (Hills et al.,
2018). Lee (2020) stated that development of the social media competencies for
strengthening resource mobilization is helpful in improving the community based
intervention strategies towards effective disease prevention. Linkages/partnership and
networking will help in the establishment of synchronization with the stakeholders of the
community-base health and disease prevention camp for T2DM. Leadership is one o the
principal aspect behind the promotion of the community empowerment. Selection of efficient
leaders must be done among the community-participants and selected community leaders will
help in voicing the expectations and networking, two of the cope steps towards niche
building. Selection of the potential leaders within the community will help to increase the
sense of ownership. This kind of approach is helpful among the indigenous population as it
will help to promote the sense of empowerment under culturally competent healthcare
settings (Marmot, 2016). Participation of the end-users in disease prevention program and in
the decision-making process, helps in the promotion of empowerment. The participation in
the decision-making process will involve practice of physical exercise and execute of proper
anti-diabetic diet plan. This will help in the modification of the modifiable risk factors for
T2DM. The participation in the decision-making process will also involve regular check-up
of the blood glucose level under the community-based healthcare campaigns and under the
use of the glucometer. However, participation in the decision-making process must only be
done upon successful health awareness and health education (Kunz et al., 2017). The assets
based approach covers the assets of communities and its dwellers and mainly include lived
experiences. The incorporation of the lived experience will be done through exchange of the
thoughts and experiences under interactive sessions.. Communication among the community-
based participants will further help in the development of bond between them and thus
helping to promote empowerment and group-based health promotion activities. The initial
8
ASSESSMENT 1
level of communication approach will include group-based discussion. This will be followed
by sharing of the information with the help of the newsletter, social media campaigns,
pamphlet ands road side advertisements and radio-advertisements. The content of
communication will cover topics like signs and symptoms of disease, disease prevention
strategies and how government of helping to reduce the vulnerability of T2DM. As the
community get exposure towards the detail of the disease prognosis along with the
government initiates, their level of empowerment and disease participation will increase
gradually (Thomas et al., 2019). Development of pathways will help to train people towards
successful disease prevention. This in turn will help the community to grow in a healthy
manner. Selected campaigns will cost-effective and will target the vulnerable population and
thus helping to increase the sense of belonging (Thomas et al., 2019).
Part 3
The Health Belief Model (HBM) will be employed for the motivation and education
of the community dwelling individuals for the effective prevention of T2DM. The HBM is
defined as a social cognition model that deals with understanding the perception of the
individuals about reality rather than how they respond to any particular situation (Luquis &
Kensinger, 2019). The HBM shares six beliefs that define the health-behaviour of the
individuals. The six different health beliefs include perceived susceptibility, perceived
seriousness, perceived benefits, perceived barriers, cues to action and health motivation.
ASSESSMENT 1
level of communication approach will include group-based discussion. This will be followed
by sharing of the information with the help of the newsletter, social media campaigns,
pamphlet ands road side advertisements and radio-advertisements. The content of
communication will cover topics like signs and symptoms of disease, disease prevention
strategies and how government of helping to reduce the vulnerability of T2DM. As the
community get exposure towards the detail of the disease prognosis along with the
government initiates, their level of empowerment and disease participation will increase
gradually (Thomas et al., 2019). Development of pathways will help to train people towards
successful disease prevention. This in turn will help the community to grow in a healthy
manner. Selected campaigns will cost-effective and will target the vulnerable population and
thus helping to increase the sense of belonging (Thomas et al., 2019).
Part 3
The Health Belief Model (HBM) will be employed for the motivation and education
of the community dwelling individuals for the effective prevention of T2DM. The HBM is
defined as a social cognition model that deals with understanding the perception of the
individuals about reality rather than how they respond to any particular situation (Luquis &
Kensinger, 2019). The HBM shares six beliefs that define the health-behaviour of the
individuals. The six different health beliefs include perceived susceptibility, perceived
seriousness, perceived benefits, perceived barriers, cues to action and health motivation.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
ASSESSMENT 1
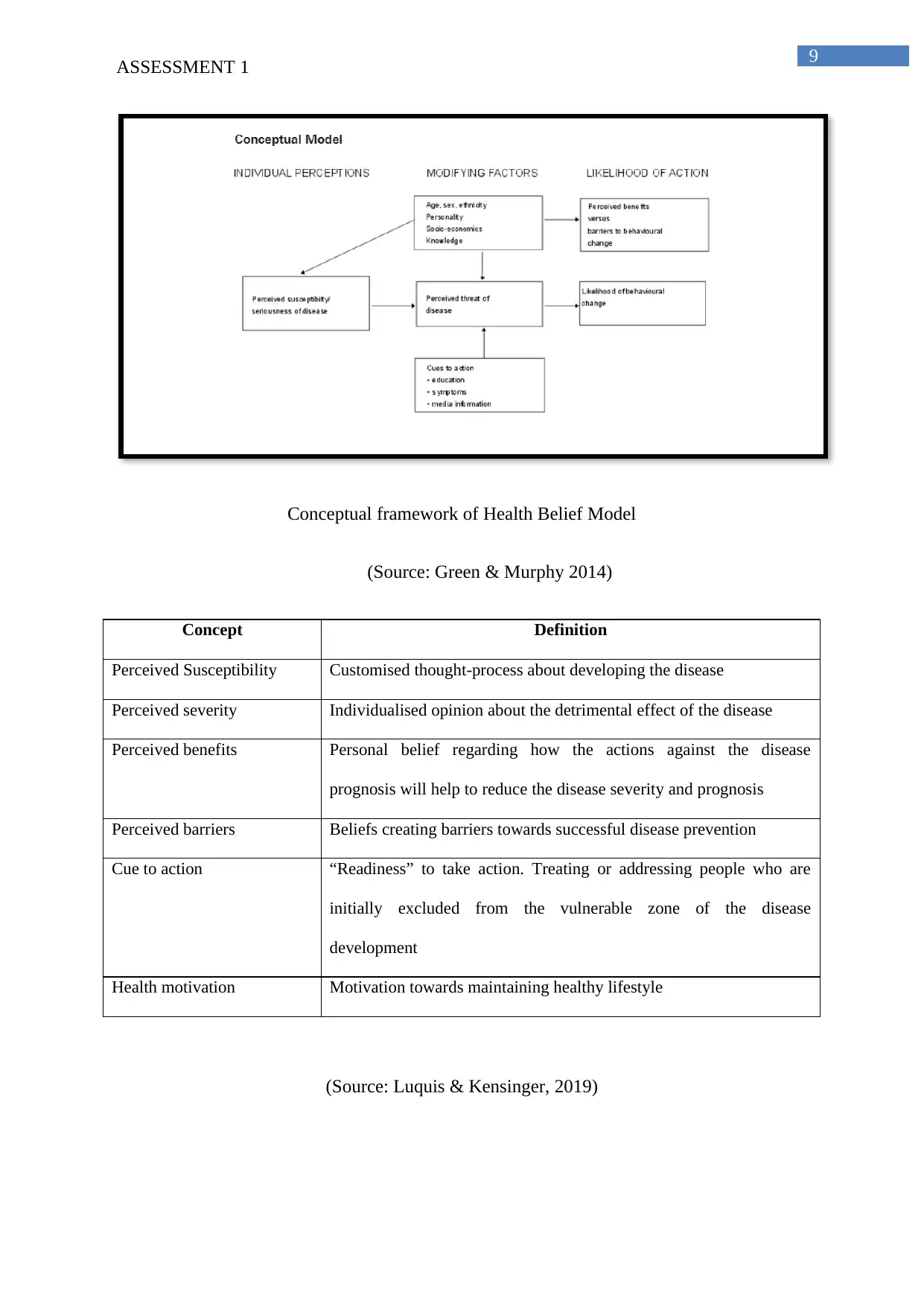
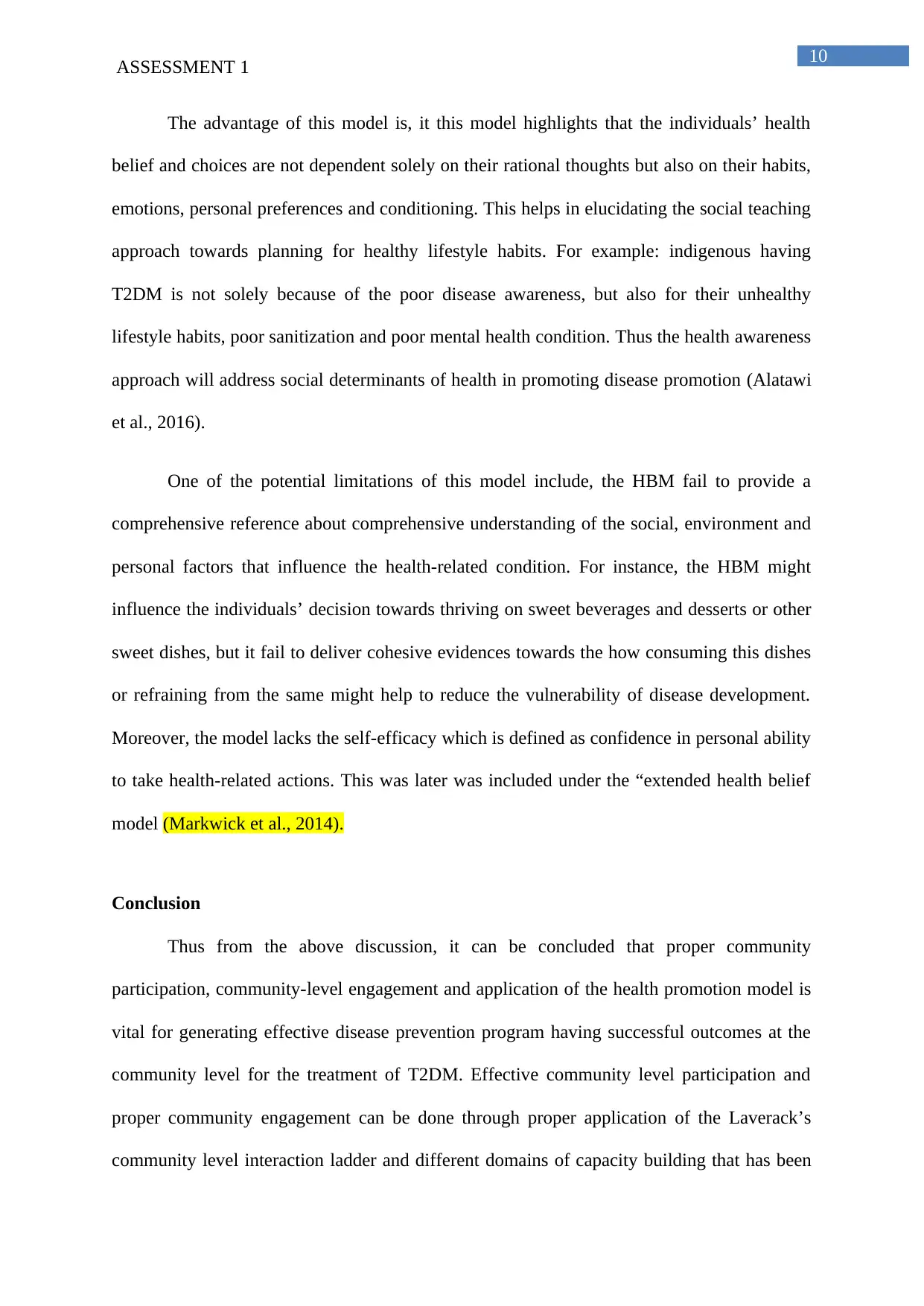
Conceptual framework of Health Belief Model
(Source: Green & Murphy 2014)
Concept Definition
Perceived Susceptibility Customised thought-process about developing the disease
Perceived severity Individualised opinion about the detrimental effect of the disease
Perceived benefits Personal belief regarding how the actions against the disease
prognosis will help to reduce the disease severity and prognosis
Perceived barriers Beliefs creating barriers towards successful disease prevention
Cue to action “Readiness” to take action. Treating or addressing people who are
initially excluded from the vulnerable zone of the disease
development
Health motivation Motivation towards maintaining healthy lifestyle
(Source: Luquis & Kensinger, 2019)
ASSESSMENT 1
Conceptual framework of Health Belief Model
(Source: Green & Murphy 2014)
Concept Definition
Perceived Susceptibility Customised thought-process about developing the disease
Perceived severity Individualised opinion about the detrimental effect of the disease
Perceived benefits Personal belief regarding how the actions against the disease
prognosis will help to reduce the disease severity and prognosis
Perceived barriers Beliefs creating barriers towards successful disease prevention
Cue to action “Readiness” to take action. Treating or addressing people who are
initially excluded from the vulnerable zone of the disease
development
Health motivation Motivation towards maintaining healthy lifestyle
(Source: Luquis & Kensinger, 2019)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
ASSESSMENT 1
The advantage of this model is, it this model highlights that the individuals’ health
belief and choices are not dependent solely on their rational thoughts but also on their habits,
emotions, personal preferences and conditioning. This helps in elucidating the social teaching
approach towards planning for healthy lifestyle habits. For example: indigenous having
T2DM is not solely because of the poor disease awareness, but also for their unhealthy
lifestyle habits, poor sanitization and poor mental health condition. Thus the health awareness
approach will address social determinants of health in promoting disease promotion (Alatawi
et al., 2016).
One of the potential limitations of this model include, the HBM fail to provide a
comprehensive reference about comprehensive understanding of the social, environment and
personal factors that influence the health-related condition. For instance, the HBM might
influence the individuals’ decision towards thriving on sweet beverages and desserts or other
sweet dishes, but it fail to deliver cohesive evidences towards the how consuming this dishes
or refraining from the same might help to reduce the vulnerability of disease development.
Moreover, the model lacks the self-efficacy which is defined as confidence in personal ability
to take health-related actions. This was later was included under the “extended health belief
model (Markwick et al., 2014).
Conclusion
Thus from the above discussion, it can be concluded that proper community
participation, community-level engagement and application of the health promotion model is
vital for generating effective disease prevention program having successful outcomes at the
community level for the treatment of T2DM. Effective community level participation and
proper community engagement can be done through proper application of the Laverack’s
community level interaction ladder and different domains of capacity building that has been
ASSESSMENT 1
The advantage of this model is, it this model highlights that the individuals’ health
belief and choices are not dependent solely on their rational thoughts but also on their habits,
emotions, personal preferences and conditioning. This helps in elucidating the social teaching
approach towards planning for healthy lifestyle habits. For example: indigenous having
T2DM is not solely because of the poor disease awareness, but also for their unhealthy
lifestyle habits, poor sanitization and poor mental health condition. Thus the health awareness
approach will address social determinants of health in promoting disease promotion (Alatawi
et al., 2016).
One of the potential limitations of this model include, the HBM fail to provide a
comprehensive reference about comprehensive understanding of the social, environment and
personal factors that influence the health-related condition. For instance, the HBM might
influence the individuals’ decision towards thriving on sweet beverages and desserts or other
sweet dishes, but it fail to deliver cohesive evidences towards the how consuming this dishes
or refraining from the same might help to reduce the vulnerability of disease development.
Moreover, the model lacks the self-efficacy which is defined as confidence in personal ability
to take health-related actions. This was later was included under the “extended health belief
model (Markwick et al., 2014).
Conclusion
Thus from the above discussion, it can be concluded that proper community
participation, community-level engagement and application of the health promotion model is
vital for generating effective disease prevention program having successful outcomes at the
community level for the treatment of T2DM. Effective community level participation and
proper community engagement can be done through proper application of the Laverack’s
community level interaction ladder and different domains of capacity building that has been

11
ASSESSMENT 1
identified by the Liberato et al. (2011). During the application of the HBM, proper back-up
plans must be maintained for addressing cues for action.
ASSESSMENT 1
identified by the Liberato et al. (2011). During the application of the HBM, proper back-up
plans must be maintained for addressing cues for action.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.