University Assignment: Community Management of Smoking and Lung Cancer
VerifiedAdded on 2022/08/22
|13
|3057
|14
Essay
AI Summary
This essay explores community management strategies for smoking and lung cancer, emphasizing the role of community-based interventions. It delves into the impact of smoking on lung cancer incidence and mortality, highlighting the need for effective prevention programs. The essay examines various community engagement strategies, including the use of Laverack's ladder of participation, and discusses capacity building for community empowerment and ownership of prevention programs. It also analyzes the health belief model and educational approaches for health promotion, providing insights into how these models can be applied to reduce smoking and lung cancer rates. The paper emphasizes the importance of leadership, communication, and participatory decision-making in fostering community involvement and achieving positive health outcomes. This assignment provides a comprehensive overview of strategies for community engagement, capacity building, and health promotion models in the context of smoking and lung cancer prevention.

Running head: COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
Community management of smoking and lung cancer
Name of the Student
Name of the University
Author Note
Community management of smoking and lung cancer
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
INTRODUCTION:
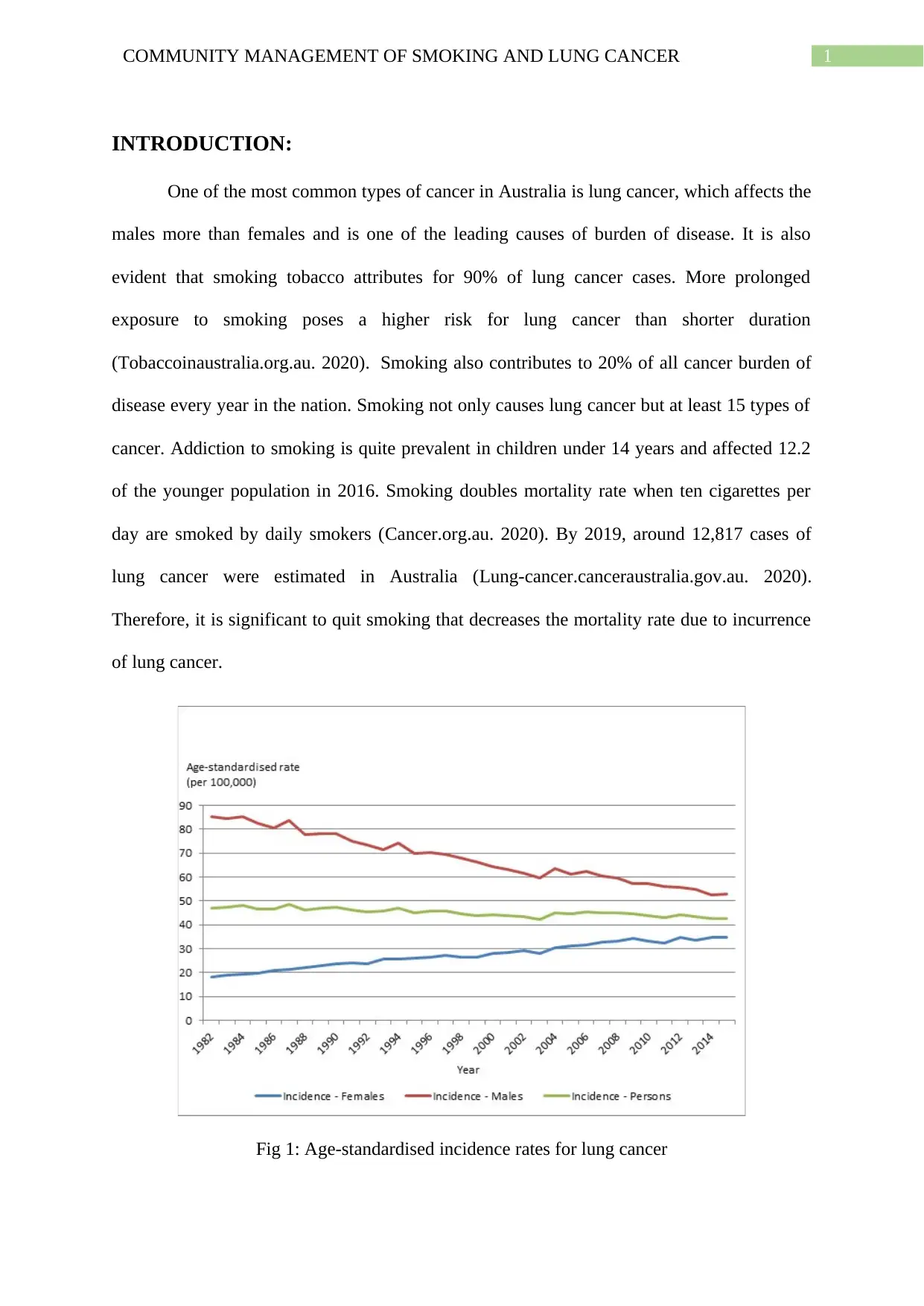
One of the most common types of cancer in Australia is lung cancer, which affects the
males more than females and is one of the leading causes of burden of disease. It is also
evident that smoking tobacco attributes for 90% of lung cancer cases. More prolonged
exposure to smoking poses a higher risk for lung cancer than shorter duration
(Tobaccoinaustralia.org.au. 2020). Smoking also contributes to 20% of all cancer burden of
disease every year in the nation. Smoking not only causes lung cancer but at least 15 types of
cancer. Addiction to smoking is quite prevalent in children under 14 years and affected 12.2
of the younger population in 2016. Smoking doubles mortality rate when ten cigarettes per
day are smoked by daily smokers (Cancer.org.au. 2020). By 2019, around 12,817 cases of
lung cancer were estimated in Australia (Lung-cancer.canceraustralia.gov.au. 2020).
Therefore, it is significant to quit smoking that decreases the mortality rate due to incurrence
of lung cancer.
Fig 1: Age-standardised incidence rates for lung cancer
INTRODUCTION:
One of the most common types of cancer in Australia is lung cancer, which affects the
males more than females and is one of the leading causes of burden of disease. It is also
evident that smoking tobacco attributes for 90% of lung cancer cases. More prolonged
exposure to smoking poses a higher risk for lung cancer than shorter duration
(Tobaccoinaustralia.org.au. 2020). Smoking also contributes to 20% of all cancer burden of
disease every year in the nation. Smoking not only causes lung cancer but at least 15 types of
cancer. Addiction to smoking is quite prevalent in children under 14 years and affected 12.2
of the younger population in 2016. Smoking doubles mortality rate when ten cigarettes per
day are smoked by daily smokers (Cancer.org.au. 2020). By 2019, around 12,817 cases of
lung cancer were estimated in Australia (Lung-cancer.canceraustralia.gov.au. 2020).
Therefore, it is significant to quit smoking that decreases the mortality rate due to incurrence
of lung cancer.
Fig 1: Age-standardised incidence rates for lung cancer
2COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
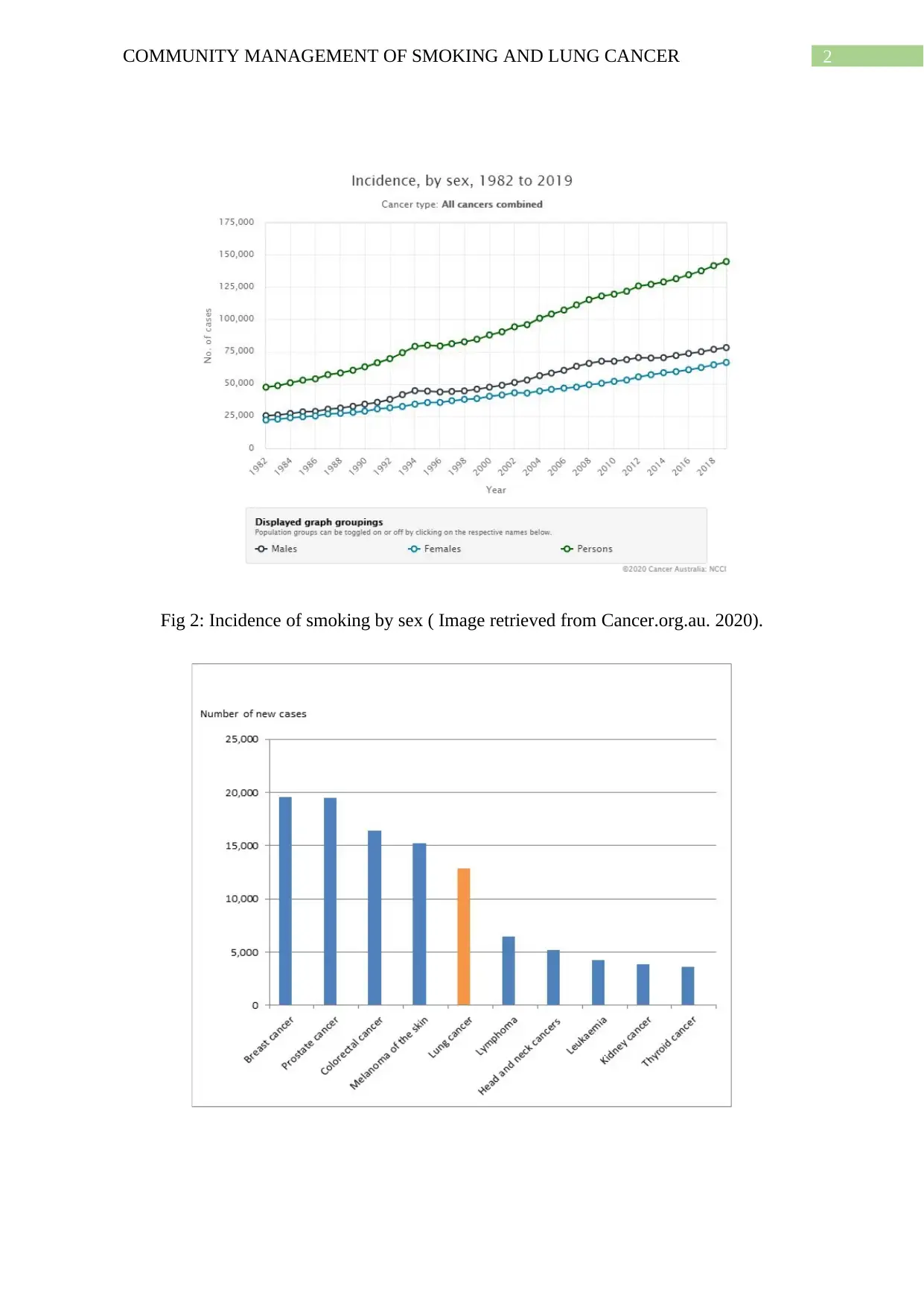
Fig 2: Incidence of smoking by sex ( Image retrieved from Cancer.org.au. 2020).
Fig 2: Incidence of smoking by sex ( Image retrieved from Cancer.org.au. 2020).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
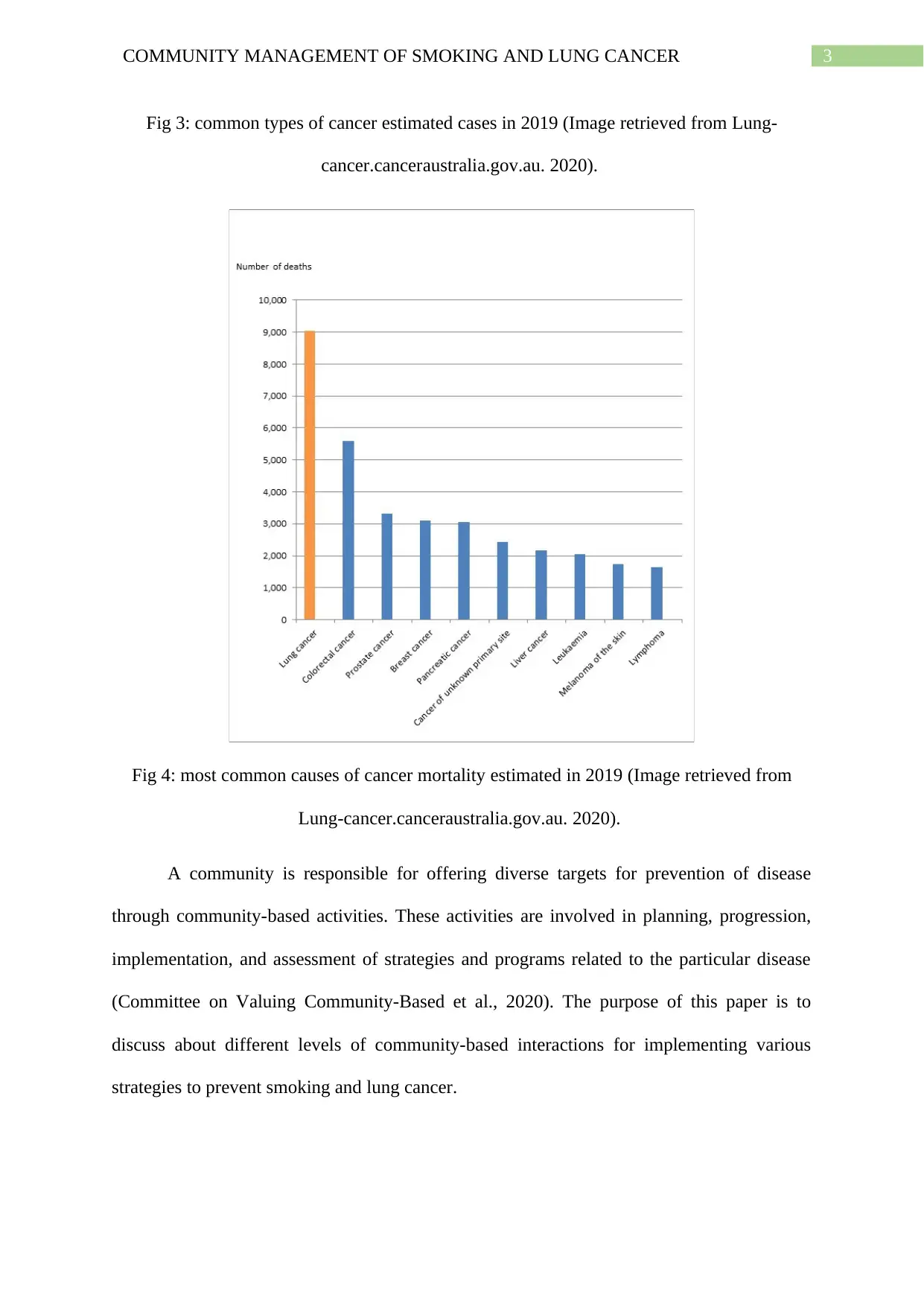
Fig 3: common types of cancer estimated cases in 2019 (Image retrieved from Lung-
cancer.canceraustralia.gov.au. 2020).
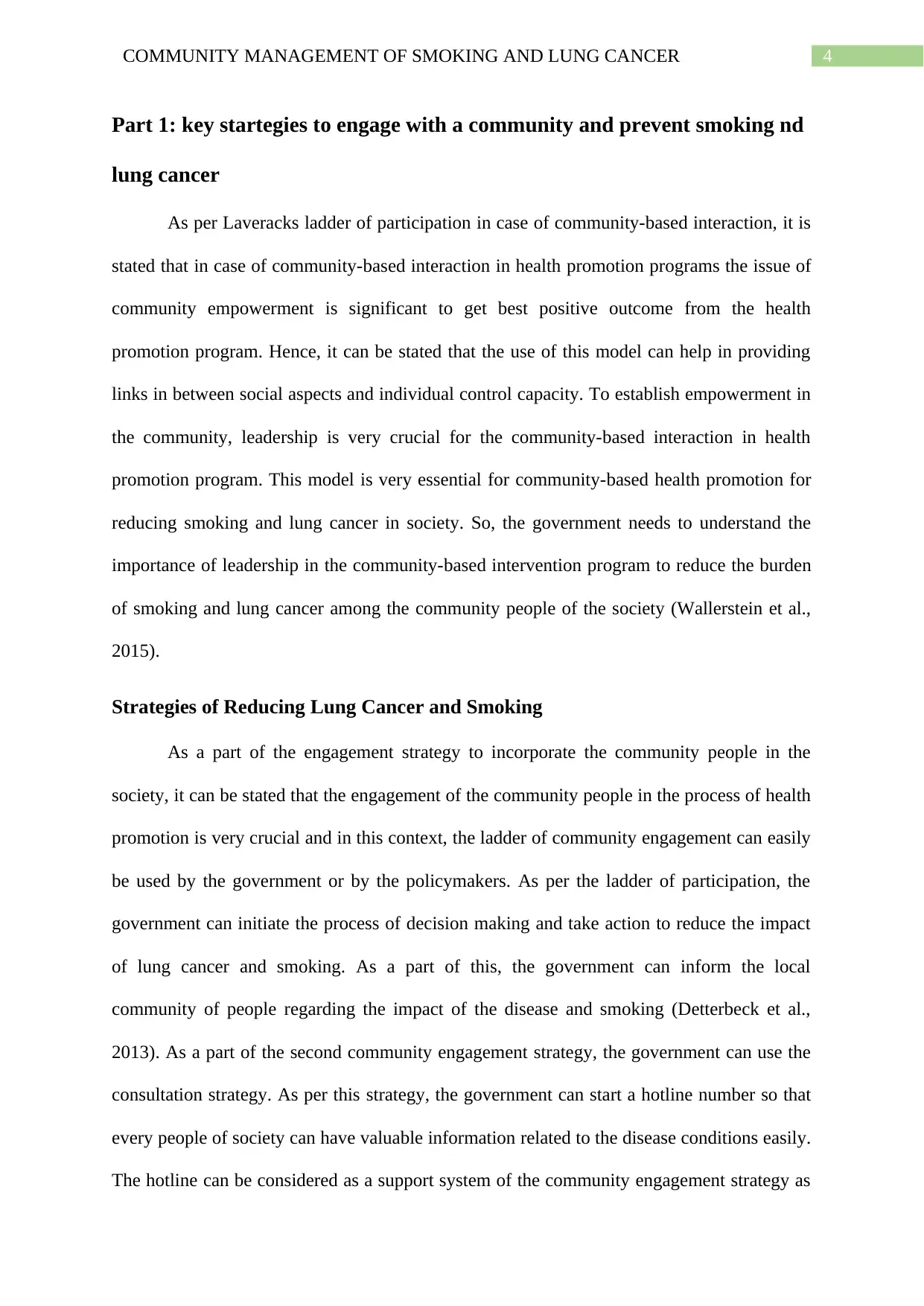
Fig 4: most common causes of cancer mortality estimated in 2019 (Image retrieved from
Lung-cancer.canceraustralia.gov.au. 2020).
A community is responsible for offering diverse targets for prevention of disease
through community-based activities. These activities are involved in planning, progression,
implementation, and assessment of strategies and programs related to the particular disease
(Committee on Valuing Community-Based et al., 2020). The purpose of this paper is to
discuss about different levels of community-based interactions for implementing various
strategies to prevent smoking and lung cancer.
Fig 3: common types of cancer estimated cases in 2019 (Image retrieved from Lung-
cancer.canceraustralia.gov.au. 2020).
Fig 4: most common causes of cancer mortality estimated in 2019 (Image retrieved from
Lung-cancer.canceraustralia.gov.au. 2020).
A community is responsible for offering diverse targets for prevention of disease
through community-based activities. These activities are involved in planning, progression,
implementation, and assessment of strategies and programs related to the particular disease
(Committee on Valuing Community-Based et al., 2020). The purpose of this paper is to
discuss about different levels of community-based interactions for implementing various
strategies to prevent smoking and lung cancer.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
Part 1: key startegies to engage with a community and prevent smoking nd
lung cancer
As per Laveracks ladder of participation in case of community-based interaction, it is
stated that in case of community-based interaction in health promotion programs the issue of
community empowerment is significant to get best positive outcome from the health
promotion program. Hence, it can be stated that the use of this model can help in providing
links in between social aspects and individual control capacity. To establish empowerment in
the community, leadership is very crucial for the community-based interaction in health
promotion program. This model is very essential for community-based health promotion for
reducing smoking and lung cancer in society. So, the government needs to understand the
importance of leadership in the community-based intervention program to reduce the burden
of smoking and lung cancer among the community people of the society (Wallerstein et al.,
2015).
Strategies of Reducing Lung Cancer and Smoking
As a part of the engagement strategy to incorporate the community people in the
society, it can be stated that the engagement of the community people in the process of health
promotion is very crucial and in this context, the ladder of community engagement can easily
be used by the government or by the policymakers. As per the ladder of participation, the
government can initiate the process of decision making and take action to reduce the impact
of lung cancer and smoking. As a part of this, the government can inform the local
community of people regarding the impact of the disease and smoking (Detterbeck et al.,
2013). As a part of the second community engagement strategy, the government can use the
consultation strategy. As per this strategy, the government can start a hotline number so that
every people of society can have valuable information related to the disease conditions easily.
The hotline can be considered as a support system of the community engagement strategy as
Part 1: key startegies to engage with a community and prevent smoking nd
lung cancer
As per Laveracks ladder of participation in case of community-based interaction, it is
stated that in case of community-based interaction in health promotion programs the issue of
community empowerment is significant to get best positive outcome from the health
promotion program. Hence, it can be stated that the use of this model can help in providing
links in between social aspects and individual control capacity. To establish empowerment in
the community, leadership is very crucial for the community-based interaction in health
promotion program. This model is very essential for community-based health promotion for
reducing smoking and lung cancer in society. So, the government needs to understand the
importance of leadership in the community-based intervention program to reduce the burden
of smoking and lung cancer among the community people of the society (Wallerstein et al.,
2015).
Strategies of Reducing Lung Cancer and Smoking
As a part of the engagement strategy to incorporate the community people in the
society, it can be stated that the engagement of the community people in the process of health
promotion is very crucial and in this context, the ladder of community engagement can easily
be used by the government or by the policymakers. As per the ladder of participation, the
government can initiate the process of decision making and take action to reduce the impact
of lung cancer and smoking. As a part of this, the government can inform the local
community of people regarding the impact of the disease and smoking (Detterbeck et al.,
2013). As a part of the second community engagement strategy, the government can use the
consultation strategy. As per this strategy, the government can start a hotline number so that
every people of society can have valuable information related to the disease conditions easily.
The hotline can be considered as a support system of the community engagement strategy as
5COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
this hotline system can answer the questions about the disease condition (Wilson et al., 2015).
As per the third strategy to engage the community in the prevention program of smoking and
lung cancer, the government can take involve the community people in the process of
prevention programs and should take opinions from the community members. As a part of
this, the government can conduct surveys, public meetings so that they can understand the
viewpoints of the public and can incorporate those views into the policy development for
reducing the cases of smoking and lung cancer (MacQueen et al., 2015).
Part 2: Capacity building for community empowerment and ownership of
prevention program:
Community health will not improve unless the capacity of the community is
strengthened adequately. Therefore it is essential to evaluate the capacity building process to
facilitate community activities in improving society and health. According to Liberato et al.,
(2011), building capacity has been developed through various domains that are assessed
through community-based interaction strategies, which are primary measures for preventing
smoking and occurrence of lung cancer. The domains identified by Liberato et al, (2011)
were through reviewing several models on building capacity. Learning opportunities and
development of skills identified in most of the models that attempt to build capabilities of the
community by teaching them on tobacco control and risk factors associated with smoking and
strengthening teams to be aware of the preventing smoking. Resource mobilization is another
domain where prevention programs should be attained by the community with the
involvement of influential community members. Partnership within a community
organization help to make the most vulnerable people from accessing health services related
to the disease and changing their attitudes and behavior towards smoking. Linkage and
this hotline system can answer the questions about the disease condition (Wilson et al., 2015).
As per the third strategy to engage the community in the prevention program of smoking and
lung cancer, the government can take involve the community people in the process of
prevention programs and should take opinions from the community members. As a part of
this, the government can conduct surveys, public meetings so that they can understand the
viewpoints of the public and can incorporate those views into the policy development for
reducing the cases of smoking and lung cancer (MacQueen et al., 2015).
Part 2: Capacity building for community empowerment and ownership of
prevention program:
Community health will not improve unless the capacity of the community is
strengthened adequately. Therefore it is essential to evaluate the capacity building process to
facilitate community activities in improving society and health. According to Liberato et al.,
(2011), building capacity has been developed through various domains that are assessed
through community-based interaction strategies, which are primary measures for preventing
smoking and occurrence of lung cancer. The domains identified by Liberato et al, (2011)
were through reviewing several models on building capacity. Learning opportunities and
development of skills identified in most of the models that attempt to build capabilities of the
community by teaching them on tobacco control and risk factors associated with smoking and
strengthening teams to be aware of the preventing smoking. Resource mobilization is another
domain where prevention programs should be attained by the community with the
involvement of influential community members. Partnership within a community
organization help to make the most vulnerable people from accessing health services related
to the disease and changing their attitudes and behavior towards smoking. Linkage and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
networking are also seen among different communities, thereby spreading awareness on
smoking cessation and improving overall health. Leadership is a domain where a initiative is
taken in motivating communities to participate in smoking prevention program and
overcoming barriers associated with the prevention program. Participatory decision-making
comes along with leadership, where different viewpoints from different members of the
community is considered regarding issues associated with smoking prevention and ways to
resolve the issues. These domains are required to be followed for community empowerment
and ownership of prevention of smoking and lung cancer.
There are some less frequent domains along withy some subdomains which were
identified and included in the community assessment. The first being the assets-based
approach where promotion of tobacco control occurs through identification of the protective
factors in the community. Sense of community that identifies the positive perceptions present
in community and its subdomain commitment to action where the community members feel
the responsibility for their activities. Communication is the basis of any approach where
campaigns and education on the health issue, and its prevention is disseminated to improve
individual health by improving literacy on health. The final domain is the development
pathway, which explains the process of building capacity.
Part 3: Model and Approaches to Health Promotion
There are various models and approaches for promoting health and prevention of
diseases. The model used for preventing smoking and lung cancer is the health belief model,
which will guide the community to improve health and initiate disease prevention programs.
This model is best for understanding the changes in health behavior; therefore it can
predetermine the changes in health behavior of every individual. This model is focused on
individual opinions regarding the health condition that is lung cancer, therefore, predict
networking are also seen among different communities, thereby spreading awareness on
smoking cessation and improving overall health. Leadership is a domain where a initiative is
taken in motivating communities to participate in smoking prevention program and
overcoming barriers associated with the prevention program. Participatory decision-making
comes along with leadership, where different viewpoints from different members of the
community is considered regarding issues associated with smoking prevention and ways to
resolve the issues. These domains are required to be followed for community empowerment
and ownership of prevention of smoking and lung cancer.
There are some less frequent domains along withy some subdomains which were
identified and included in the community assessment. The first being the assets-based
approach where promotion of tobacco control occurs through identification of the protective
factors in the community. Sense of community that identifies the positive perceptions present
in community and its subdomain commitment to action where the community members feel
the responsibility for their activities. Communication is the basis of any approach where
campaigns and education on the health issue, and its prevention is disseminated to improve
individual health by improving literacy on health. The final domain is the development
pathway, which explains the process of building capacity.
Part 3: Model and Approaches to Health Promotion
There are various models and approaches for promoting health and prevention of
diseases. The model used for preventing smoking and lung cancer is the health belief model,
which will guide the community to improve health and initiate disease prevention programs.
This model is best for understanding the changes in health behavior; therefore it can
predetermine the changes in health behavior of every individual. This model is focused on
individual opinions regarding the health condition that is lung cancer, therefore, predict
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
health-related behaviors of every individual. The key factors responsible for the influencing
the health related behaviours are perceived susceptibility that is perception of every
individual about the disease, perception severity that is belief about the consequence of the
disease, perceived benefits that is views on the positive effects of the action, perceived
barriers, signals to action that is contact with factors that give rise to the action and self-
efficacy that is the self-confidence of succeeding (Bowden & Manning, 2016).
This model is used to implement short term or long term interventions, and there are
some decision-making points that influence the change in health behaviors. The first being
the collection of information by conducting an assessment on the health needs of the
community to determine the risk population targeted for change. After which the
consequences of the health condition related to the risk behaviours is conveyed clearly so that
the degree of severeness is understood. Then the target population is made to understand
through communication about the steps of the prevention program and signifying the benefits
of the program. Then assistance is provided to the target population so that they identify and
decrease the obstructions to the implementation. Finally, actions are demonstrated by
building skills and giving support so that they grow self-efficacy to bring changes in their
behavior. The advantages of health belief model include- helping the community to
understand the barriers or reasons for failure to adapt to the disease prevention strategies, to
understand the responses of the person to the symptoms of the disease, and comply with the
medical treatment. The disadvantages of this model include- it does not consider the person
or other factors that influence the adoption of health behaviour, it does not consider the habits
of an individual therefore recommending to accept an action such as in smoking, and it does
not take into account the environmentak or economic factors that forbid or promote the
acceptance of the action (Skinner et al., 2015).
health-related behaviors of every individual. The key factors responsible for the influencing
the health related behaviours are perceived susceptibility that is perception of every
individual about the disease, perception severity that is belief about the consequence of the
disease, perceived benefits that is views on the positive effects of the action, perceived
barriers, signals to action that is contact with factors that give rise to the action and self-
efficacy that is the self-confidence of succeeding (Bowden & Manning, 2016).
This model is used to implement short term or long term interventions, and there are
some decision-making points that influence the change in health behaviors. The first being
the collection of information by conducting an assessment on the health needs of the
community to determine the risk population targeted for change. After which the
consequences of the health condition related to the risk behaviours is conveyed clearly so that
the degree of severeness is understood. Then the target population is made to understand
through communication about the steps of the prevention program and signifying the benefits
of the program. Then assistance is provided to the target population so that they identify and
decrease the obstructions to the implementation. Finally, actions are demonstrated by
building skills and giving support so that they grow self-efficacy to bring changes in their
behavior. The advantages of health belief model include- helping the community to
understand the barriers or reasons for failure to adapt to the disease prevention strategies, to
understand the responses of the person to the symptoms of the disease, and comply with the
medical treatment. The disadvantages of this model include- it does not consider the person
or other factors that influence the adoption of health behaviour, it does not consider the habits
of an individual therefore recommending to accept an action such as in smoking, and it does
not take into account the environmentak or economic factors that forbid or promote the
acceptance of the action (Skinner et al., 2015).
8COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
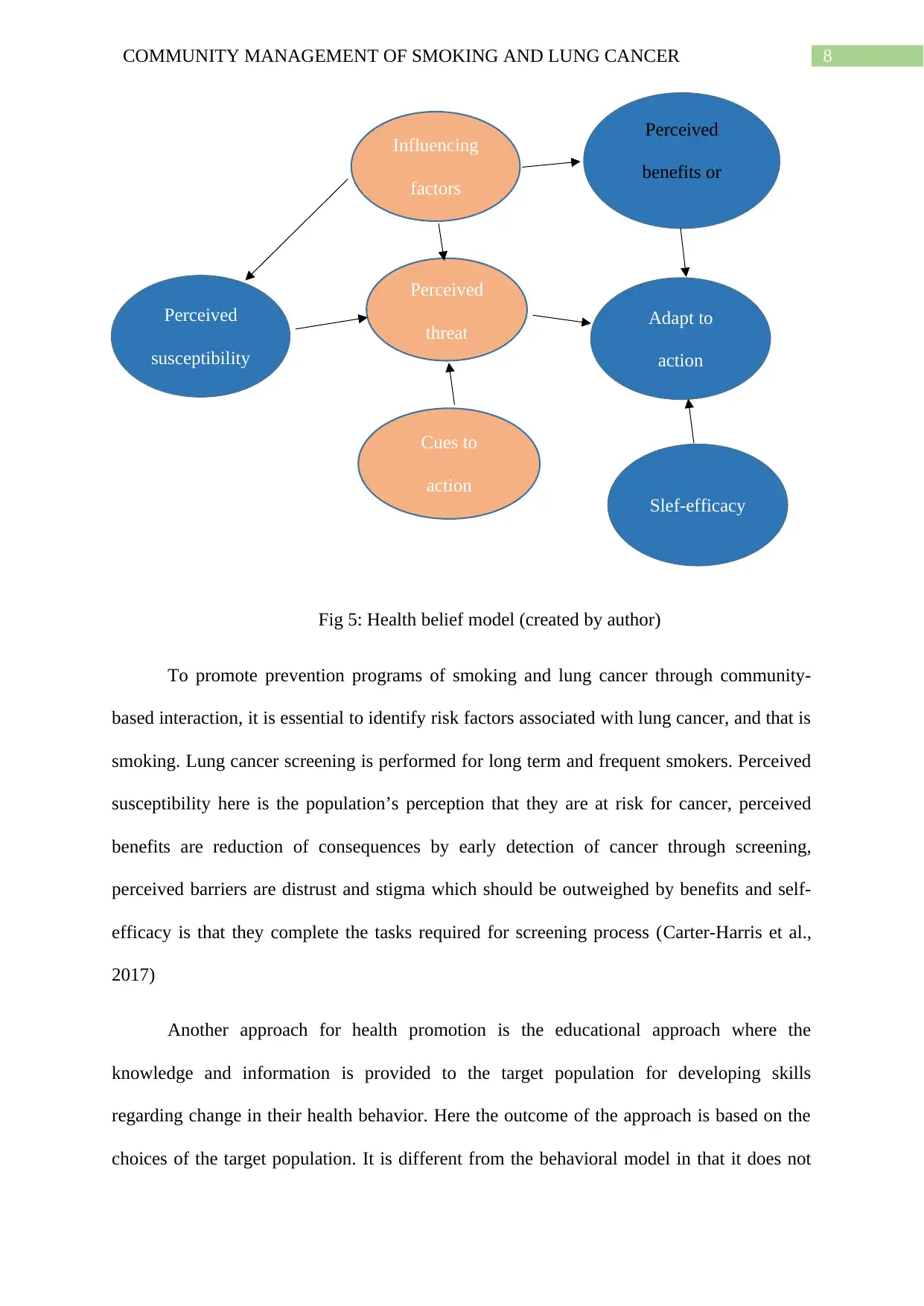
Fig 5: Health belief model (created by author)
To promote prevention programs of smoking and lung cancer through community-
based interaction, it is essential to identify risk factors associated with lung cancer, and that is
smoking. Lung cancer screening is performed for long term and frequent smokers. Perceived
susceptibility here is the population’s perception that they are at risk for cancer, perceived
benefits are reduction of consequences by early detection of cancer through screening,
perceived barriers are distrust and stigma which should be outweighed by benefits and self-
efficacy is that they complete the tasks required for screening process (Carter-Harris et al.,
2017)
Another approach for health promotion is the educational approach where the
knowledge and information is provided to the target population for developing skills
regarding change in their health behavior. Here the outcome of the approach is based on the
choices of the target population. It is different from the behavioral model in that it does not
Perceived
susceptibility
Influencing
factors
Cues to
action
Perceived
threat
Slef-efficacy
Adapt to
action
Perceived
benefits or
risks
Fig 5: Health belief model (created by author)
To promote prevention programs of smoking and lung cancer through community-
based interaction, it is essential to identify risk factors associated with lung cancer, and that is
smoking. Lung cancer screening is performed for long term and frequent smokers. Perceived
susceptibility here is the population’s perception that they are at risk for cancer, perceived
benefits are reduction of consequences by early detection of cancer through screening,
perceived barriers are distrust and stigma which should be outweighed by benefits and self-
efficacy is that they complete the tasks required for screening process (Carter-Harris et al.,
2017)
Another approach for health promotion is the educational approach where the
knowledge and information is provided to the target population for developing skills
regarding change in their health behavior. Here the outcome of the approach is based on the
choices of the target population. It is different from the behavioral model in that it does not
Perceived
susceptibility
Influencing
factors
Cues to
action
Perceived
threat
Slef-efficacy
Adapt to
action
Perceived
benefits or
risks
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
motivate or induce the change in a specific direction. The educational purpose will try to
bring the change; however, it is not mandatory for the person to follow the preferences of the
health promoter. The educational approach is a hypothesis based on the relationship between
knowledge and behavior, which believes that an increase in the knowledge will bring about
change in the behavior. The approach can be initiated by distributing leaflets and booklets
containing the information or audiovisual displays or face to face advice. This may provide
advantages to the participant to share their ideas and views on the health promotion program
and show their attitudes towards their health. The approach may be held through group
discussion or counseling. It may allow the participant to perform activities or be into real-life
situations to develop their skills in decision making (Sharma, 2016).
In case of health promotion for smoking cessation and lung cancer prevention, real-
life situations maybe when they are offered tobacco and watch their reaction when they are
trying to quit smoking. These educational programs are led by health promoters who
understand the factors promoting or hindering their learning on the intervention program.
Booklets and leaflets can have information regarding how risk factors are associated with
lung cancer and what are the ways one can prevent it. Counseling and one to one advice can
be helpful for people who are trying to quit smoking but are unable to do it. The advantages
of educational approach include- its aim at educating people about the disease condition,
associated factors and ways of prevention. It is also not persuasive in nature as the outcome is
entirely based on the choices of the participant. The disadvantages include- its basis of
assumption rather than conviction, the choices of the individuals may be negatively
influenced by social or economic factors, and decision-related to health can be complex
(Gilbert et al., 2014).
motivate or induce the change in a specific direction. The educational purpose will try to
bring the change; however, it is not mandatory for the person to follow the preferences of the
health promoter. The educational approach is a hypothesis based on the relationship between
knowledge and behavior, which believes that an increase in the knowledge will bring about
change in the behavior. The approach can be initiated by distributing leaflets and booklets
containing the information or audiovisual displays or face to face advice. This may provide
advantages to the participant to share their ideas and views on the health promotion program
and show their attitudes towards their health. The approach may be held through group
discussion or counseling. It may allow the participant to perform activities or be into real-life
situations to develop their skills in decision making (Sharma, 2016).
In case of health promotion for smoking cessation and lung cancer prevention, real-
life situations maybe when they are offered tobacco and watch their reaction when they are
trying to quit smoking. These educational programs are led by health promoters who
understand the factors promoting or hindering their learning on the intervention program.
Booklets and leaflets can have information regarding how risk factors are associated with
lung cancer and what are the ways one can prevent it. Counseling and one to one advice can
be helpful for people who are trying to quit smoking but are unable to do it. The advantages
of educational approach include- its aim at educating people about the disease condition,
associated factors and ways of prevention. It is also not persuasive in nature as the outcome is
entirely based on the choices of the participant. The disadvantages include- its basis of
assumption rather than conviction, the choices of the individuals may be negatively
influenced by social or economic factors, and decision-related to health can be complex
(Gilbert et al., 2014).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
Conclusion
In conclusion, it can be stated that lung cancer is one of the common type of cancer that
affects men more than women in Australia and smoking is the leading cause of lung cancer.
The incidence of lung cancer has increased over the years and therefore, community-based
approaches are required for cessation of smoking ad prevention of lung cancer. The
discussion includes how Laverack’s ladder of community-based participation is important in
promoting health of the community. Liberato’s concept of building capacity explains a
combination of 12 domains from different models and theories that intersect among each
other. The domains include the learning opportunities, resource mobilization, partnership,
leadership, and participatory decision making as the key domains along with other domains
and sub-domains for health promotion. There are models and approaches for health
promotion in lung cancer that include the health belief model and educational approach
whose aims are similar, but approaches and concepts are different. Finally, it is understood
community plays a significant role in preventing diseases and risk factors such as lung cancer
and smoking, thereby promoting health of the population.
Conclusion
In conclusion, it can be stated that lung cancer is one of the common type of cancer that
affects men more than women in Australia and smoking is the leading cause of lung cancer.
The incidence of lung cancer has increased over the years and therefore, community-based
approaches are required for cessation of smoking ad prevention of lung cancer. The
discussion includes how Laverack’s ladder of community-based participation is important in
promoting health of the community. Liberato’s concept of building capacity explains a
combination of 12 domains from different models and theories that intersect among each
other. The domains include the learning opportunities, resource mobilization, partnership,
leadership, and participatory decision making as the key domains along with other domains
and sub-domains for health promotion. There are models and approaches for health
promotion in lung cancer that include the health belief model and educational approach
whose aims are similar, but approaches and concepts are different. Finally, it is understood
community plays a significant role in preventing diseases and risk factors such as lung cancer
and smoking, thereby promoting health of the population.
11COMMUNITY MANAGEMENT OF SMOKING AND LUNG CANCER
References:
Bowden, J., & Manning, V. (Eds.). (2016). Health promotion in midwifery: principles and
practice. CRC Press.
Cancer.org.au. (2020). Cancer.org.au. Retrieved 18 March 2020, from
https://www.cancer.org.au/preventing-cancer/smoking-and-tobacco/smoking.html.
Carter-Harris, L., Ceppa, D. P., Hanna, N., & Rawl, S. M. (2017). Lung cancer screening:
what do long-term smokers know and believe?. Health expectations : an international
journal of public participation in health care and health policy, 20(1), 59–68.
https://doi.org/10.1111/hex.12433
Carter-Harris, L., Ceppa, D. P., Hanna, N., & Rawl, S. M. (2017). Lung cancer screening:
what do long-term smokers know and believe?. Health expectations : an international
journal of public participation in health care and health policy, 20(1), 59–68.
https://doi.org/10.1111/hex.12433
Committee on Valuing Community-Based, N., Practice, B., & Medicine, I.
(2020). Community-Based Prevention. Ncbi.nlm.nih.gov. Retrieved 18 March 2020,
from https://www.ncbi.nlm.nih.gov/books/NBK206935/.
Detterbeck, F. C., Mazzone, P. J., Naidich, D. P., & Bach, P. B. (2013). Screening for lung
cancer: diagnosis and management of lung cancer: American College of Chest
Physicians evidence-based clinical practice guidelines. Chest, 143(5), e78S-e92S.
Gilbert, G. G., Sawyer, R. G., & McNeill, E. B. (2014). Health education: Creating
strategies for school & community health. Jones & Bartlett Publishers.
References:
Bowden, J., & Manning, V. (Eds.). (2016). Health promotion in midwifery: principles and
practice. CRC Press.
Cancer.org.au. (2020). Cancer.org.au. Retrieved 18 March 2020, from
https://www.cancer.org.au/preventing-cancer/smoking-and-tobacco/smoking.html.
Carter-Harris, L., Ceppa, D. P., Hanna, N., & Rawl, S. M. (2017). Lung cancer screening:
what do long-term smokers know and believe?. Health expectations : an international
journal of public participation in health care and health policy, 20(1), 59–68.
https://doi.org/10.1111/hex.12433
Carter-Harris, L., Ceppa, D. P., Hanna, N., & Rawl, S. M. (2017). Lung cancer screening:
what do long-term smokers know and believe?. Health expectations : an international
journal of public participation in health care and health policy, 20(1), 59–68.
https://doi.org/10.1111/hex.12433
Committee on Valuing Community-Based, N., Practice, B., & Medicine, I.
(2020). Community-Based Prevention. Ncbi.nlm.nih.gov. Retrieved 18 March 2020,
from https://www.ncbi.nlm.nih.gov/books/NBK206935/.
Detterbeck, F. C., Mazzone, P. J., Naidich, D. P., & Bach, P. B. (2013). Screening for lung
cancer: diagnosis and management of lung cancer: American College of Chest
Physicians evidence-based clinical practice guidelines. Chest, 143(5), e78S-e92S.
Gilbert, G. G., Sawyer, R. G., & McNeill, E. B. (2014). Health education: Creating
strategies for school & community health. Jones & Bartlett Publishers.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.