University Case Study: Congestive Cardiac Failure Nursing Assessment
VerifiedAdded on 2023/04/07
|11
|2126
|144
Case Study
AI Summary
This case study analyzes congestive cardiac failure (CCF), outlining the disease, its causes, incidence, and risk factors. It explores the impact of CCF on patients and their families, using Mrs. Sharon McKenzie as a case example. The study details three common signs and symptoms of CCF—shortness of breath, fatigue, and fluid retention—explaining their underlying pathophysiology. It further discusses the pharmacodynamics and pharmacokinetics of digoxin, a common medication for CCF, and develops a nursing care plan for the patient's first eight hours post-admission. The plan includes goals, interventions, and rationales to stabilize the patient's condition and improve outcomes. The case study references relevant literature to support its findings and recommendations.

Running head: CONGESTIVE CARDIAC FAILURE
CONGESTIVE CARDIAC FAILURE
Name of the Student:
Name of the University:
Author Note:
CONGESTIVE CARDIAC FAILURE
Name of the Student:
Name of the University:
Author Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CONGESTIVE CARDIAC FAILURE
1. Outline the disease, causes, incidence and risk factors. Discuss the impact of the
selected disease on the patient and their family.
Answer: Congestive cardiac failure is a disorder where pumping efficiency of the heart is
reduced greatly. So the blood flow becomes slower in the body and the blood pressure
increases. The kidneys cause the body to retain more fluid which bloats up the arms, feet,
legs, ankles and lungs so the body is congested (Scott & Winters, 2015). So this disorder is
called as congested cardiac failure.
Causes of congestive cardiac failure:
History of myocardial infarction.
Heart valve related disorders.
Longstanding alcohol consumption.
High BP.
Coronary artery disorder.
Abnormalities in the heart rhythm.
Thyroid disorder.
Stiffening of heart muscles by viral infection.
Incidence:
Incidence of congestive cardiac failure increases significantly with aging. So older
people are more vulnerable to this disease. The incidence of congestive cardiac failure is
higher in men than women. 1 to 5 person per 1000 patients is affected by this disease among
people younger than 65 years while 10 person per 1000 patients is affected among people
older than 65 years (Dokainish et al., 2017). The number increases more among the people
older than 75 years. 1 to 2 % people are affected by congestive cardiac disease who are less
1. Outline the disease, causes, incidence and risk factors. Discuss the impact of the
selected disease on the patient and their family.
Answer: Congestive cardiac failure is a disorder where pumping efficiency of the heart is
reduced greatly. So the blood flow becomes slower in the body and the blood pressure
increases. The kidneys cause the body to retain more fluid which bloats up the arms, feet,
legs, ankles and lungs so the body is congested (Scott & Winters, 2015). So this disorder is
called as congested cardiac failure.
Causes of congestive cardiac failure:
History of myocardial infarction.
Heart valve related disorders.
Longstanding alcohol consumption.
High BP.
Coronary artery disorder.
Abnormalities in the heart rhythm.
Thyroid disorder.
Stiffening of heart muscles by viral infection.
Incidence:
Incidence of congestive cardiac failure increases significantly with aging. So older
people are more vulnerable to this disease. The incidence of congestive cardiac failure is
higher in men than women. 1 to 5 person per 1000 patients is affected by this disease among
people younger than 65 years while 10 person per 1000 patients is affected among people
older than 65 years (Dokainish et al., 2017). The number increases more among the people
older than 75 years. 1 to 2 % people are affected by congestive cardiac disease who are less
2CONGESTIVE CARDIAC FAILURE
than 65 years old. It is 2 to 3 % in people older than 65 years old while it reaches 5 to 10 % in
individuals older than 75 years.
Risk factors:
Previous incidence of myocardial infarction (Payne et al., 2015).
High BP.
Diabetes and prediabetes.
High level of Cholesterol.
Smoking and alcohol consumption.
Being physically dormant.
Having a history of heart related diseases in the family.
Being obese or overweight.
History of preeclampsia at the time of pregnancy.
Cardiomyopathy or heart enlargement.
Aberration in the heart valves.
Impact of congestive cardiac failure on the patient and their family
Mrs. Sharon McKenzie is 77 years old and suffering from acute congestive cardio
failure. She can not do simple things like going for a walk with her husband or gardening as
she feels out of breathe. Because of her physical condition her quality of life and social
interaction is affected. She is spending her life in hospital so she cannot spend quality time
with her family and friends. Because of this she is feeling isolated and her mental health is
deteriorating as well. The family is also going through anxiety and pain as the patient was in
emergency department. So the family is also mentally and financially burdened because of
the dismal health condition of the Mrs. McKenzie.
than 65 years old. It is 2 to 3 % in people older than 65 years old while it reaches 5 to 10 % in
individuals older than 75 years.
Risk factors:
Previous incidence of myocardial infarction (Payne et al., 2015).
High BP.
Diabetes and prediabetes.
High level of Cholesterol.
Smoking and alcohol consumption.
Being physically dormant.
Having a history of heart related diseases in the family.
Being obese or overweight.
History of preeclampsia at the time of pregnancy.
Cardiomyopathy or heart enlargement.
Aberration in the heart valves.
Impact of congestive cardiac failure on the patient and their family
Mrs. Sharon McKenzie is 77 years old and suffering from acute congestive cardio
failure. She can not do simple things like going for a walk with her husband or gardening as
she feels out of breathe. Because of her physical condition her quality of life and social
interaction is affected. She is spending her life in hospital so she cannot spend quality time
with her family and friends. Because of this she is feeling isolated and her mental health is
deteriorating as well. The family is also going through anxiety and pain as the patient was in
emergency department. So the family is also mentally and financially burdened because of
the dismal health condition of the Mrs. McKenzie.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CONGESTIVE CARDIAC FAILURE
2. Discuss three (3) common signs and symptoms of the selected disease and explain the
underlying pathophysiology of each.
Answer: Shortness of breath or dyspnea, fatigue and fluid retention in the body are the most
common symptoms of congestive cardiac failure.
Shortness of breath or Dyspnea: Poor cardiac output causes slower flow of blood. The
kidney causes fluid retention which affects the lung. The fluid filled lung causes
shortness of breath specially while performing a physical activity by the patient. Lung
congestion causes wheezing. As the cardiac output is slower the heart beats faster to
supply adequate blood to the body. This results in irregular and rapid heartbeat.
Lesser blood supply to kidney causes fluid and water retention by the kidney. It
causes swollen ankles, legs, abdomen which is called as edema (François, Ronco &
Bargman, 2015). Higher level of water retention causes the individual to urinate for
several times. The edema and bloating of the stomach may result in mild nausea and
loss of appetite.
Dizziness, weakness and fatigue is a common symptom as the blood supply is lesser
and slower due to poor cardiac output by the ventricles of the heart. So the oxygen
supply to the organ and the muscle is significantly lower which causes weakness,
fatigue. The oxygen supply to brain is also reduced which causes dizziness.
Extremities like fingers and feet get lesser supply of blood so it feels cold.
Ventricles pumps out blood from the heart to the whole body. In case of congested cardiac
failure the cardiac output is significantly reduced. So the blood supply to the different organs
and muscles of the body is slower and lesser. Blood carries oxygen to the different parts of
the body to lower blood supply causes reduced oxygen supply to the organs and the brain.
Sp02 at 92% on RA reflects the same. Dizziness and fatigue is caused by this. Lesser supply
2. Discuss three (3) common signs and symptoms of the selected disease and explain the
underlying pathophysiology of each.
Answer: Shortness of breath or dyspnea, fatigue and fluid retention in the body are the most
common symptoms of congestive cardiac failure.
Shortness of breath or Dyspnea: Poor cardiac output causes slower flow of blood. The
kidney causes fluid retention which affects the lung. The fluid filled lung causes
shortness of breath specially while performing a physical activity by the patient. Lung
congestion causes wheezing. As the cardiac output is slower the heart beats faster to
supply adequate blood to the body. This results in irregular and rapid heartbeat.
Lesser blood supply to kidney causes fluid and water retention by the kidney. It
causes swollen ankles, legs, abdomen which is called as edema (François, Ronco &
Bargman, 2015). Higher level of water retention causes the individual to urinate for
several times. The edema and bloating of the stomach may result in mild nausea and
loss of appetite.
Dizziness, weakness and fatigue is a common symptom as the blood supply is lesser
and slower due to poor cardiac output by the ventricles of the heart. So the oxygen
supply to the organ and the muscle is significantly lower which causes weakness,
fatigue. The oxygen supply to brain is also reduced which causes dizziness.
Extremities like fingers and feet get lesser supply of blood so it feels cold.
Ventricles pumps out blood from the heart to the whole body. In case of congested cardiac
failure the cardiac output is significantly reduced. So the blood supply to the different organs
and muscles of the body is slower and lesser. Blood carries oxygen to the different parts of
the body to lower blood supply causes reduced oxygen supply to the organs and the brain.
Sp02 at 92% on RA reflects the same. Dizziness and fatigue is caused by this. Lesser supply
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CONGESTIVE CARDIAC FAILURE
of blood causes the kidney to retain more fluid which causes edema. So the symptoms are
interlinked and one symptoms can escalate the other to further deteriorate the physical
condition of the patient. Mrs. McKenzie has all the symptoms related to congestive cardiac
failure that are discussed here.
3. Discuss the pharmacodynamics & pharmacokinetics of one (1) common class of drug
relevant to the chosen patient.
Answer: 250 mcg of Digoxin is prescribed for daily consumption to treat congestive cardiac
failure in Mrs. McKenzie. Pharmacodynamics and pharmacokinetics of digoxin is being
discussed here.
Pharmacodynamics
Digoxin increases efficiency of heart contractions which helps in the treatment of
congestive cardiac failure. It increases the contraction force of the heart muscles by inhibiting
the enzyme activity called ATPase. ATPase regulates calcium, potassium and sodium
movement into heart muscle. Force of contraction is controlled by Calcium. So entry of
calcium in the heart muscle increases by inhibiting ATPase activity. Digoxin is effective in
the treatment of rapid and abnormal atrial rhythms as it slows down the electrical
transmission between the ventricles and the atria of heart (Bavishi, Khan & Ather, 2015).
Rapid atrial rhythm and electric impulse can cause rapid contractions in the ventricles. This
causes inefficient cardiac output with inadequate oxygen and nutrients supply to the body.
Digoxin blocks the electric transmission between the atria and the ventricles by slowing
down the contraction of the ventricle (Lopes et al., 2018).
Pharmacokinetics
Most of the digoxin is absorbed (75 to 80%) in the proximal part of small intestine
when it is taken orally. 25 to 30 % binds to the serum albumin. High concentration of
of blood causes the kidney to retain more fluid which causes edema. So the symptoms are
interlinked and one symptoms can escalate the other to further deteriorate the physical
condition of the patient. Mrs. McKenzie has all the symptoms related to congestive cardiac
failure that are discussed here.
3. Discuss the pharmacodynamics & pharmacokinetics of one (1) common class of drug
relevant to the chosen patient.
Answer: 250 mcg of Digoxin is prescribed for daily consumption to treat congestive cardiac
failure in Mrs. McKenzie. Pharmacodynamics and pharmacokinetics of digoxin is being
discussed here.
Pharmacodynamics
Digoxin increases efficiency of heart contractions which helps in the treatment of
congestive cardiac failure. It increases the contraction force of the heart muscles by inhibiting
the enzyme activity called ATPase. ATPase regulates calcium, potassium and sodium
movement into heart muscle. Force of contraction is controlled by Calcium. So entry of
calcium in the heart muscle increases by inhibiting ATPase activity. Digoxin is effective in
the treatment of rapid and abnormal atrial rhythms as it slows down the electrical
transmission between the ventricles and the atria of heart (Bavishi, Khan & Ather, 2015).
Rapid atrial rhythm and electric impulse can cause rapid contractions in the ventricles. This
causes inefficient cardiac output with inadequate oxygen and nutrients supply to the body.
Digoxin blocks the electric transmission between the atria and the ventricles by slowing
down the contraction of the ventricle (Lopes et al., 2018).
Pharmacokinetics
Most of the digoxin is absorbed (75 to 80%) in the proximal part of small intestine
when it is taken orally. 25 to 30 % binds to the serum albumin. High concentration of
5CONGESTIVE CARDIAC FAILURE
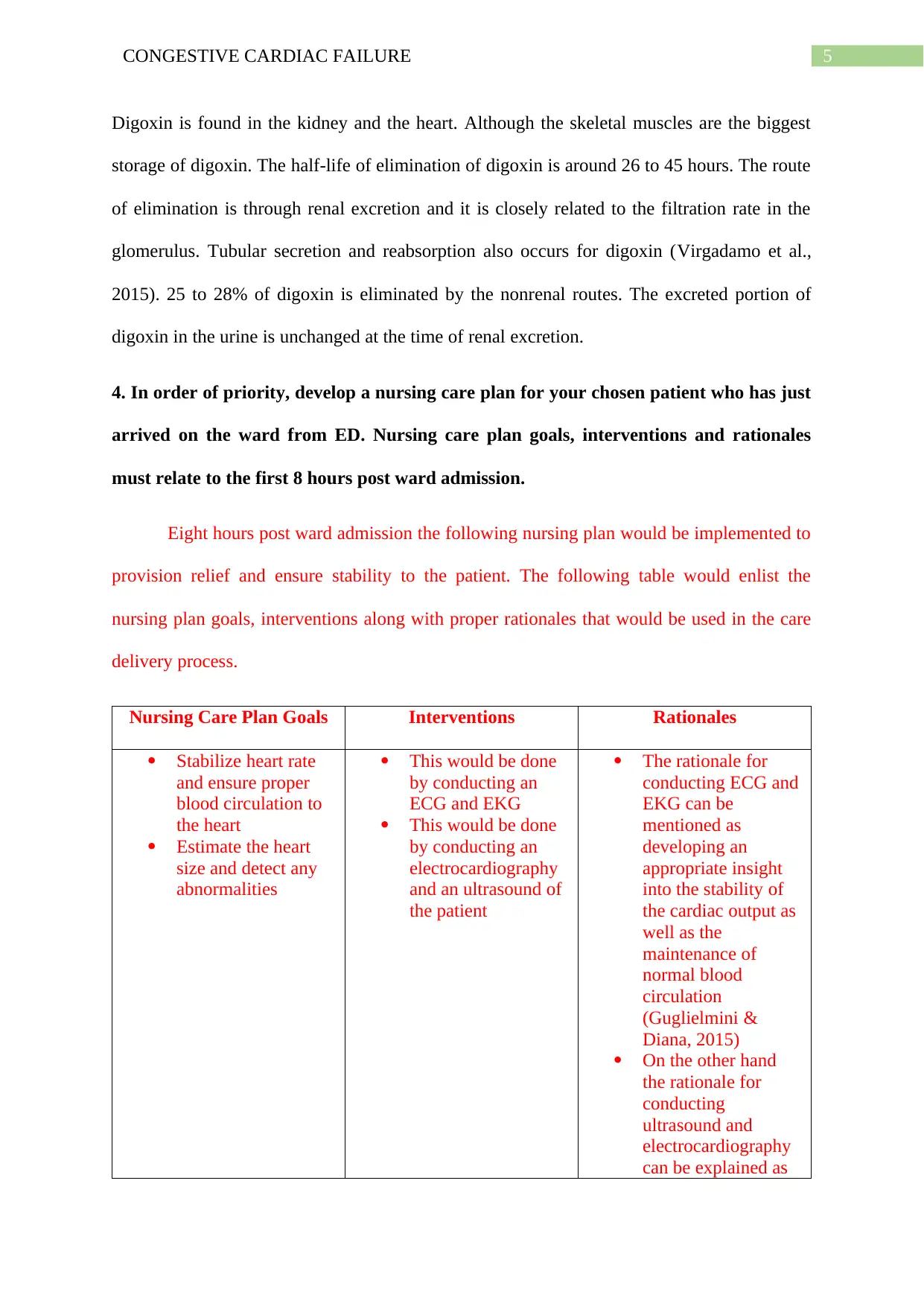
Digoxin is found in the kidney and the heart. Although the skeletal muscles are the biggest
storage of digoxin. The half-life of elimination of digoxin is around 26 to 45 hours. The route
of elimination is through renal excretion and it is closely related to the filtration rate in the
glomerulus. Tubular secretion and reabsorption also occurs for digoxin (Virgadamo et al.,
2015). 25 to 28% of digoxin is eliminated by the nonrenal routes. The excreted portion of
digoxin in the urine is unchanged at the time of renal excretion.
4. In order of priority, develop a nursing care plan for your chosen patient who has just
arrived on the ward from ED. Nursing care plan goals, interventions and rationales
must relate to the first 8 hours post ward admission.
Eight hours post ward admission the following nursing plan would be implemented to
provision relief and ensure stability to the patient. The following table would enlist the
nursing plan goals, interventions along with proper rationales that would be used in the care
delivery process.
Nursing Care Plan Goals Interventions Rationales
Stabilize heart rate
and ensure proper
blood circulation to
the heart
Estimate the heart
size and detect any
abnormalities
This would be done
by conducting an
ECG and EKG
This would be done
by conducting an
electrocardiography
and an ultrasound of
the patient
The rationale for
conducting ECG and
EKG can be
mentioned as
developing an
appropriate insight
into the stability of
the cardiac output as
well as the
maintenance of
normal blood
circulation
(Guglielmini &
Diana, 2015)
On the other hand
the rationale for
conducting
ultrasound and
electrocardiography
can be explained as
Digoxin is found in the kidney and the heart. Although the skeletal muscles are the biggest
storage of digoxin. The half-life of elimination of digoxin is around 26 to 45 hours. The route
of elimination is through renal excretion and it is closely related to the filtration rate in the
glomerulus. Tubular secretion and reabsorption also occurs for digoxin (Virgadamo et al.,
2015). 25 to 28% of digoxin is eliminated by the nonrenal routes. The excreted portion of
digoxin in the urine is unchanged at the time of renal excretion.
4. In order of priority, develop a nursing care plan for your chosen patient who has just
arrived on the ward from ED. Nursing care plan goals, interventions and rationales
must relate to the first 8 hours post ward admission.
Eight hours post ward admission the following nursing plan would be implemented to
provision relief and ensure stability to the patient. The following table would enlist the
nursing plan goals, interventions along with proper rationales that would be used in the care
delivery process.
Nursing Care Plan Goals Interventions Rationales
Stabilize heart rate
and ensure proper
blood circulation to
the heart
Estimate the heart
size and detect any
abnormalities
This would be done
by conducting an
ECG and EKG
This would be done
by conducting an
electrocardiography
and an ultrasound of
the patient
The rationale for
conducting ECG and
EKG can be
mentioned as
developing an
appropriate insight
into the stability of
the cardiac output as
well as the
maintenance of
normal blood
circulation
(Guglielmini &
Diana, 2015)
On the other hand
the rationale for
conducting
ultrasound and
electrocardiography
can be explained as
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CONGESTIVE CARDIAC FAILURE
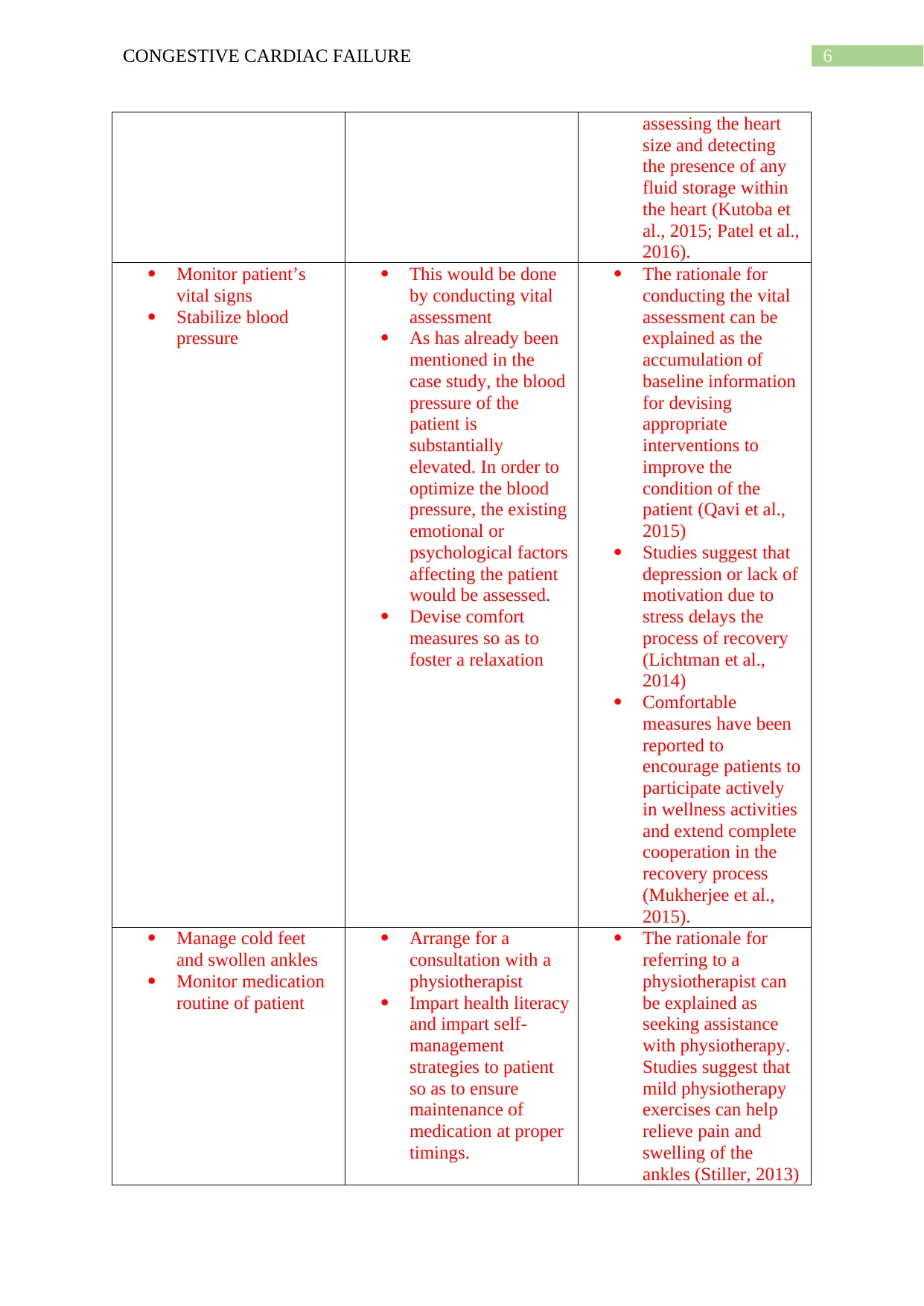
assessing the heart
size and detecting
the presence of any
fluid storage within
the heart (Kutoba et
al., 2015; Patel et al.,
2016).
Monitor patient’s
vital signs
Stabilize blood
pressure
This would be done
by conducting vital
assessment
As has already been
mentioned in the
case study, the blood
pressure of the
patient is
substantially
elevated. In order to
optimize the blood
pressure, the existing
emotional or
psychological factors
affecting the patient
would be assessed.
Devise comfort
measures so as to
foster a relaxation
The rationale for
conducting the vital
assessment can be
explained as the
accumulation of
baseline information
for devising
appropriate
interventions to
improve the
condition of the
patient (Qavi et al.,
2015)
Studies suggest that
depression or lack of
motivation due to
stress delays the
process of recovery
(Lichtman et al.,
2014)
Comfortable
measures have been
reported to
encourage patients to
participate actively
in wellness activities
and extend complete
cooperation in the
recovery process
(Mukherjee et al.,
2015).
Manage cold feet
and swollen ankles
Monitor medication
routine of patient
Arrange for a
consultation with a
physiotherapist
Impart health literacy
and impart self-
management
strategies to patient
so as to ensure
maintenance of
medication at proper
timings.
The rationale for
referring to a
physiotherapist can
be explained as
seeking assistance
with physiotherapy.
Studies suggest that
mild physiotherapy
exercises can help
relieve pain and
swelling of the
ankles (Stiller, 2013)
assessing the heart
size and detecting
the presence of any
fluid storage within
the heart (Kutoba et
al., 2015; Patel et al.,
2016).
Monitor patient’s
vital signs
Stabilize blood
pressure
This would be done
by conducting vital
assessment
As has already been
mentioned in the
case study, the blood
pressure of the
patient is
substantially
elevated. In order to
optimize the blood
pressure, the existing
emotional or
psychological factors
affecting the patient
would be assessed.
Devise comfort
measures so as to
foster a relaxation
The rationale for
conducting the vital
assessment can be
explained as the
accumulation of
baseline information
for devising
appropriate
interventions to
improve the
condition of the
patient (Qavi et al.,
2015)
Studies suggest that
depression or lack of
motivation due to
stress delays the
process of recovery
(Lichtman et al.,
2014)
Comfortable
measures have been
reported to
encourage patients to
participate actively
in wellness activities
and extend complete
cooperation in the
recovery process
(Mukherjee et al.,
2015).
Manage cold feet
and swollen ankles
Monitor medication
routine of patient
Arrange for a
consultation with a
physiotherapist
Impart health literacy
and impart self-
management
strategies to patient
so as to ensure
maintenance of
medication at proper
timings.
The rationale for
referring to a
physiotherapist can
be explained as
seeking assistance
with physiotherapy.
Studies suggest that
mild physiotherapy
exercises can help
relieve pain and
swelling of the
ankles (Stiller, 2013)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CONGESTIVE CARDIAC FAILURE
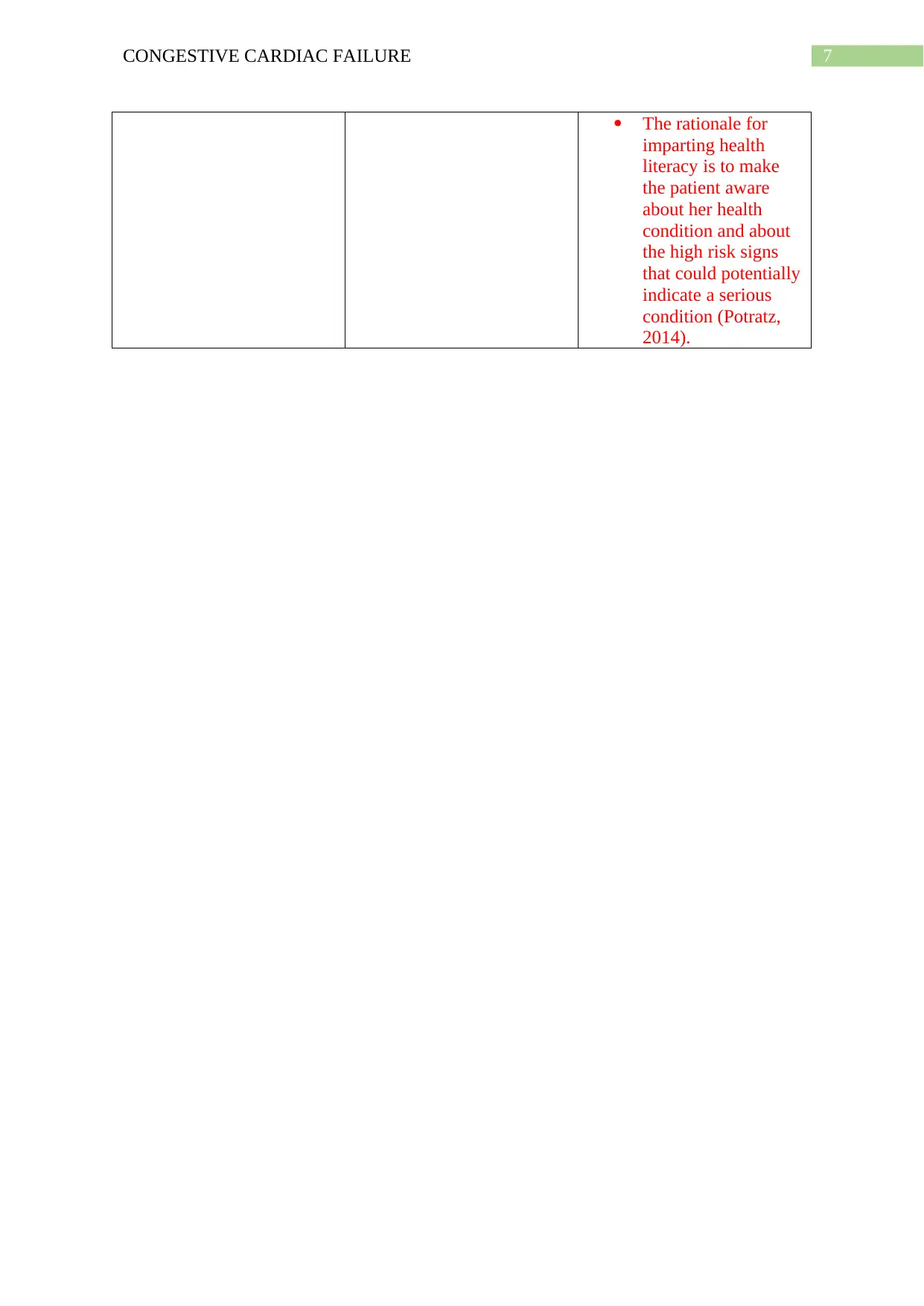
The rationale for
imparting health
literacy is to make
the patient aware
about her health
condition and about
the high risk signs
that could potentially
indicate a serious
condition (Potratz,
2014).
The rationale for
imparting health
literacy is to make
the patient aware
about her health
condition and about
the high risk signs
that could potentially
indicate a serious
condition (Potratz,
2014).
8CONGESTIVE CARDIAC FAILURE
References
Bavishi, C., Khan, A. R., & Ather, S. (2015). Digoxin in patients with atrial fibrillation and
heart failure: a meta-analysis. International journal of cardiology, 188, 99-101.
Dokainish, H., Teo, K., Zhu, J., Roy, A., AlHabib, K. F., ElSayed, A., ... & Orlandini, A.
(2017). Global mortality variations in patients with heart failure: results from the
International Congestive Heart Failure (INTER-CHF) prospective cohort study. The
Lancet Global Health, 5(7), e665-e672.
François, K., Ronco, C., & Bargman, J. M. (2015). Peritoneal dialysis for chronic congestive
heart failure. Blood purification, 40(1), 45-52.
Guglielmini, C., & Diana, A. (2015). Thoracic radiography in the cat: identification of
cardiomegaly and congestive heart failure. Journal of Veterinary Cardiology, 17,
S87-S101.
Kubota, Y., Asai, K., Furuse, E., Nakamura, S., Murai, K., Tsukada, Y. T., & Shimizu, W.
(2015). Impact of β-blocker selectivity on long-term outcomes in congestive heart
failure patients with chronic obstructive pulmonary disease. International journal of
chronic obstructive pulmonary disease, 10, 515.
Lichtman, J. H., Froelicher, E. S., Blumenthal, J. A., Carney, R. M., Doering, L. V., Frasure-
Smith, N., ... & Vaccarino, V. (2014). Depression as a risk factor for poor prognosis
among patients with acute coronary syndrome: systematic review and
recommendations: a scientific statement from the American Heart
Association. Circulation, 129(12), 1350-1369.
References
Bavishi, C., Khan, A. R., & Ather, S. (2015). Digoxin in patients with atrial fibrillation and
heart failure: a meta-analysis. International journal of cardiology, 188, 99-101.
Dokainish, H., Teo, K., Zhu, J., Roy, A., AlHabib, K. F., ElSayed, A., ... & Orlandini, A.
(2017). Global mortality variations in patients with heart failure: results from the
International Congestive Heart Failure (INTER-CHF) prospective cohort study. The
Lancet Global Health, 5(7), e665-e672.
François, K., Ronco, C., & Bargman, J. M. (2015). Peritoneal dialysis for chronic congestive
heart failure. Blood purification, 40(1), 45-52.
Guglielmini, C., & Diana, A. (2015). Thoracic radiography in the cat: identification of
cardiomegaly and congestive heart failure. Journal of Veterinary Cardiology, 17,
S87-S101.
Kubota, Y., Asai, K., Furuse, E., Nakamura, S., Murai, K., Tsukada, Y. T., & Shimizu, W.
(2015). Impact of β-blocker selectivity on long-term outcomes in congestive heart
failure patients with chronic obstructive pulmonary disease. International journal of
chronic obstructive pulmonary disease, 10, 515.
Lichtman, J. H., Froelicher, E. S., Blumenthal, J. A., Carney, R. M., Doering, L. V., Frasure-
Smith, N., ... & Vaccarino, V. (2014). Depression as a risk factor for poor prognosis
among patients with acute coronary syndrome: systematic review and
recommendations: a scientific statement from the American Heart
Association. Circulation, 129(12), 1350-1369.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CONGESTIVE CARDIAC FAILURE
Lopes, R. D., Rordorf, R., De Ferrari, G. M., Leonardi, S., Thomas, L., Wojdyla, D. M., ... &
Hanna, M. (2018). Digoxin and mortality in patients with atrial fibrillation. Journal of
the American College of Cardiology, 71(10), 1063-1074.
Mukherjee, S., Palit, S. K., Banerjee, S., Ariffin, M. R. K., Rondoni, L., & Bhattacharya, D.
K. (2015). Can complexity decrease in congestive heart failure?. Physica A:
Statistical Mechanics and its Applications, 439, 93-102.
Patel, N., Ju, C., Macon, C., Thadani, U., Schulte, P. J., Hernandez, A. F., ... & Fonarow, G.
C. (2016). Temporal trends of digoxin use in patients hospitalized with heart failure:
analysis from the American Heart Association Get With The Guidelines-Heart Failure
Registry. JACC: Heart Failure, 4(5), 348-356.
Payne, J. R., Borgeat, K., Brodbelt, D. C., Connolly, D. J., & Fuentes, V. L. (2015). Risk
factors associated with sudden death vs. congestive heart failure or arterial
thromboembolism in cats with hypertrophic cardiomyopathy. Journal of Veterinary
Cardiology, 17, S318-S328.
Potratz, W. J. (2014). Health Care Providers' Perceptions of Health Literacy (Doctoral
dissertation, Walden University).
Stiller, K. (2013). Physiotherapy in intensive care: an updated systematic
review. Chest, 144(3), 825-847.
Qavi, A. H., Kamal, R., & Schrier, R. W. (2015). Clinical use of diuretics in heart failure,
cirrhosis, and nephrotic syndrome. International journal of nephrology, 2015.
Scott, M. C., & Winters, M. E. (2015). Congestive heart failure. Emergency Medicine
Clinics, 33(3), 553-562
Lopes, R. D., Rordorf, R., De Ferrari, G. M., Leonardi, S., Thomas, L., Wojdyla, D. M., ... &
Hanna, M. (2018). Digoxin and mortality in patients with atrial fibrillation. Journal of
the American College of Cardiology, 71(10), 1063-1074.
Mukherjee, S., Palit, S. K., Banerjee, S., Ariffin, M. R. K., Rondoni, L., & Bhattacharya, D.
K. (2015). Can complexity decrease in congestive heart failure?. Physica A:
Statistical Mechanics and its Applications, 439, 93-102.
Patel, N., Ju, C., Macon, C., Thadani, U., Schulte, P. J., Hernandez, A. F., ... & Fonarow, G.
C. (2016). Temporal trends of digoxin use in patients hospitalized with heart failure:
analysis from the American Heart Association Get With The Guidelines-Heart Failure
Registry. JACC: Heart Failure, 4(5), 348-356.
Payne, J. R., Borgeat, K., Brodbelt, D. C., Connolly, D. J., & Fuentes, V. L. (2015). Risk
factors associated with sudden death vs. congestive heart failure or arterial
thromboembolism in cats with hypertrophic cardiomyopathy. Journal of Veterinary
Cardiology, 17, S318-S328.
Potratz, W. J. (2014). Health Care Providers' Perceptions of Health Literacy (Doctoral
dissertation, Walden University).
Stiller, K. (2013). Physiotherapy in intensive care: an updated systematic
review. Chest, 144(3), 825-847.
Qavi, A. H., Kamal, R., & Schrier, R. W. (2015). Clinical use of diuretics in heart failure,
cirrhosis, and nephrotic syndrome. International journal of nephrology, 2015.
Scott, M. C., & Winters, M. E. (2015). Congestive heart failure. Emergency Medicine
Clinics, 33(3), 553-562
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

10CONGESTIVE CARDIAC FAILURE
Virgadamo, S., Charnigo, R., Darrat, Y., Morales, G., & Elayi, C. S. (2015). Digoxin: A
systematic review in atrial fibrillation, congestive heart failure and post myocardial
infarction. World journal of cardiology, 7(11), 808.
Virgadamo, S., Charnigo, R., Darrat, Y., Morales, G., & Elayi, C. S. (2015). Digoxin: A
systematic review in atrial fibrillation, congestive heart failure and post myocardial
infarction. World journal of cardiology, 7(11), 808.
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.