Comprehensive Analysis: Nursing Assessment of Breathing Techniques
VerifiedAdded on 2023/06/13
|14
|3197
|292
Report
AI Summary
This report provides a comprehensive overview of nursing assessments related to breathing, focusing on techniques, interventions, and the application of the Roper-Logan-Tierney model. It covers various aspects of respiratory assessment, including inspection, palpation, percussion, and auscultation, along with the identification of normal and distressed respiratory signs. The report further delves into the management of Chronic Obstructive Pulmonary Disease (COPD), outlining nursing goals, interventions, and the importance of a multidisciplinary approach. Safety measures during respiratory assessments are also highlighted, emphasizing infection prevention and accurate monitoring. The document concludes by stressing the significance of patient education, self-management, and appropriate referrals for ensuring effective post-discharge care and minimizing exacerbation episodes. Desklib offers more solved assignments and study resources for nursing students.

Running head: NURSING ASSESSMENT OF BREATHING
NURSING ASSESSMENT OF BREATHING
Name of the Student
Name of the university
Author’s note
NURSING ASSESSMENT OF BREATHING
Name of the Student
Name of the university
Author’s note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1NURSING ASSESSMENT OF BREATHING
Part 1
The rate and the characteristics of respirations help to provide insight to the general health status
of the person. Breathlessness can be a very disturbing symptom for many people and assessment
of the breathing patterns help to identify the problem early and intervene with them.
People with lung diseases require their respiratory assessment to be more frequent than
the others. People suffering from chest infections, long term lung problems or people who smoke
tobacco daily will be benefitted if they have their respirations assessed regularly. There are
certain factors that impact the respiratory rate. They are the age, gender, weight, size, exercises
pain, anxiety, smoking habits and the effects of some medicines. The normal respiratory rate of a
man is about 14 to 18 breaths a minute and for a woman it is about 14 to 18 breaths per minute,
hence it is important to assess the respiration in order to measure any changes (Usmani & Barnes
2012, p.146-156). Some of the probable findings of a respiratory assessment can be deep and
swallowed breathing that may indicate anxiety. Shallow breathing that can be due to the effect of
some medicines (Thim et al. 2012,p. 117). Minimal chest movements are sometimes found in
asthma as a differential diagnosis. Person facing respiratory trouble may indicate towards the
onset of a lung or heart problems. Pain during breathing may indicate towards a chest infection
or cracked rib, chest infection or tumor in the lung (Usmani & Barnes 2012, p.146-156).
Breathing through mouth may indicate towards a blocked nose. Irregular breathing can be
common in older persons, but may also direct towards heart or brain problems.
Part 1
The rate and the characteristics of respirations help to provide insight to the general health status
of the person. Breathlessness can be a very disturbing symptom for many people and assessment
of the breathing patterns help to identify the problem early and intervene with them.
People with lung diseases require their respiratory assessment to be more frequent than
the others. People suffering from chest infections, long term lung problems or people who smoke
tobacco daily will be benefitted if they have their respirations assessed regularly. There are
certain factors that impact the respiratory rate. They are the age, gender, weight, size, exercises
pain, anxiety, smoking habits and the effects of some medicines. The normal respiratory rate of a
man is about 14 to 18 breaths a minute and for a woman it is about 14 to 18 breaths per minute,
hence it is important to assess the respiration in order to measure any changes (Usmani & Barnes
2012, p.146-156). Some of the probable findings of a respiratory assessment can be deep and
swallowed breathing that may indicate anxiety. Shallow breathing that can be due to the effect of
some medicines (Thim et al. 2012,p. 117). Minimal chest movements are sometimes found in
asthma as a differential diagnosis. Person facing respiratory trouble may indicate towards the
onset of a lung or heart problems. Pain during breathing may indicate towards a chest infection
or cracked rib, chest infection or tumor in the lung (Usmani & Barnes 2012, p.146-156).
Breathing through mouth may indicate towards a blocked nose. Irregular breathing can be
common in older persons, but may also direct towards heart or brain problems.
2NURSING ASSESSMENT OF BREATHING
While measuring the respirations, the depth, rate, pattern of respiration should be recorded. The
depth volume known as the tidal volume should be about 500ml. The breathing rate should've
equal with pause between each breath.
The pulmonary examination includes inspection, palpation, percussion and auscultation.
Inspection- Inspection is normally done with eyes and it begins with the initial greeting with the
patient. A nurse should notice the patient's facial expression in relation to inspiration and
expiration (Thim et al. 2012, p. 117).
Palpation- It is done by placing the palm of each hand on the superior portion of the
hemithoraces and the hand is then moved inferiorly below the twelfth ribs.
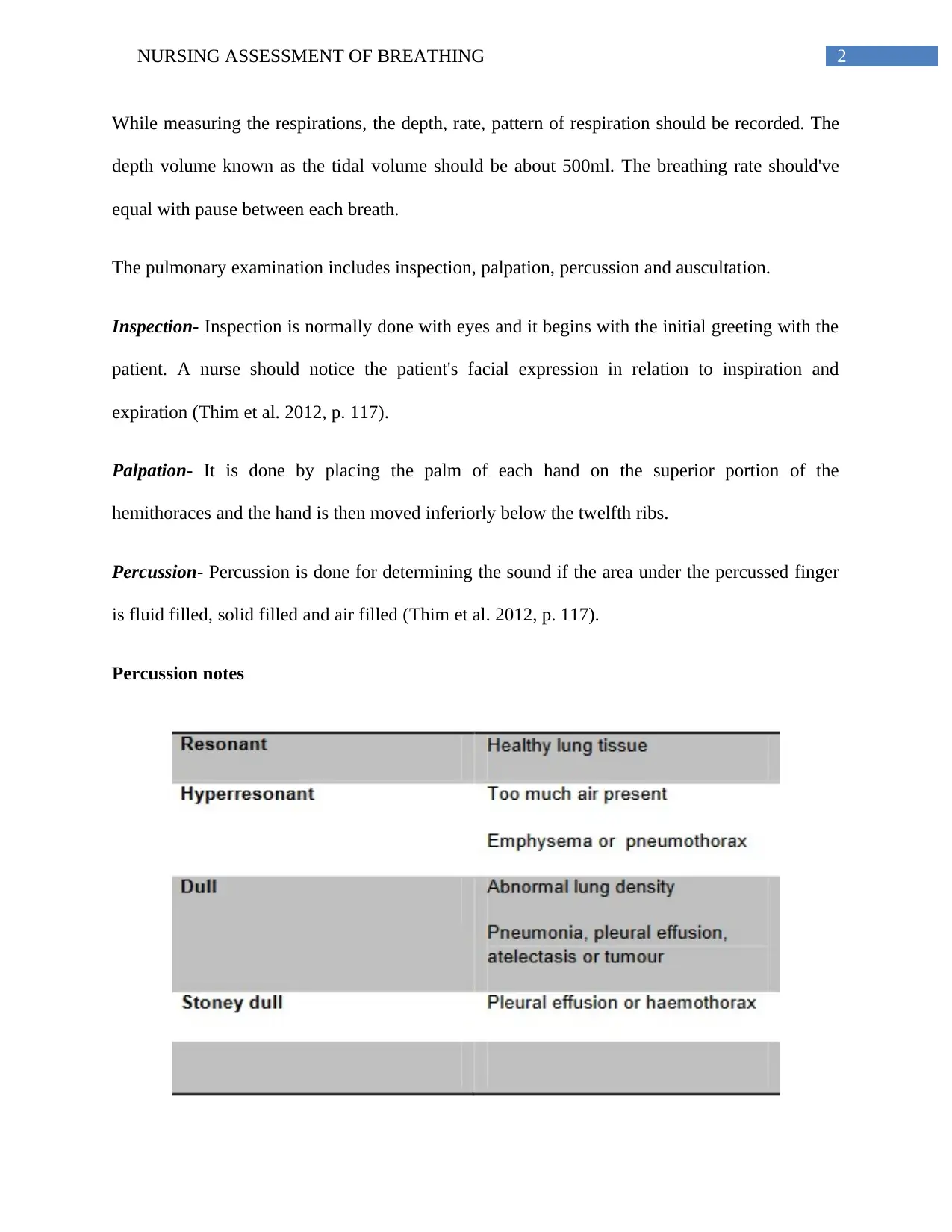
Percussion- Percussion is done for determining the sound if the area under the percussed finger
is fluid filled, solid filled and air filled (Thim et al. 2012, p. 117).
Percussion notes
While measuring the respirations, the depth, rate, pattern of respiration should be recorded. The
depth volume known as the tidal volume should be about 500ml. The breathing rate should've
equal with pause between each breath.
The pulmonary examination includes inspection, palpation, percussion and auscultation.
Inspection- Inspection is normally done with eyes and it begins with the initial greeting with the
patient. A nurse should notice the patient's facial expression in relation to inspiration and
expiration (Thim et al. 2012, p. 117).
Palpation- It is done by placing the palm of each hand on the superior portion of the
hemithoraces and the hand is then moved inferiorly below the twelfth ribs.
Percussion- Percussion is done for determining the sound if the area under the percussed finger
is fluid filled, solid filled and air filled (Thim et al. 2012, p. 117).
Percussion notes
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3NURSING ASSESSMENT OF BREATHING
Source: (Elsherif & Noble 2011,p.29-33)
A respiratory assessment includes the following:-
Speech:
Normal- No difficulties in speech
Respiratory distress- short sentences, short phrases or may be few words.
Cough:
Productive cough indicates COPD, bronchiectasis or COPD and CF if the patient is younger and
dry cough relates to asthma if younger and ILD if older (Csikesz & Gartman 2014).
Inspection of the hands
It is also necessary to inspect the hands. Tar staining on the fingers may indicate towards chain
smoking, which increases the chance of COPD and lung cancer. Tenderness and swelling of the
joints may indicate towards rheumatological diseases (Thim et al. 2012, p. 117).
Respiratory noises:
Normal- no noises or quite
Respiratory distress: Noises on breathing such as crackles or gasps may indicate some clinical
conditions. For example wheezing is the characteristic symptom of asthma (Kazaks et al. 2012,
p.83-92).
Chest auscultation:
Normal- no wheezes or crackles
Source: (Elsherif & Noble 2011,p.29-33)
A respiratory assessment includes the following:-
Speech:
Normal- No difficulties in speech
Respiratory distress- short sentences, short phrases or may be few words.
Cough:
Productive cough indicates COPD, bronchiectasis or COPD and CF if the patient is younger and
dry cough relates to asthma if younger and ILD if older (Csikesz & Gartman 2014).
Inspection of the hands
It is also necessary to inspect the hands. Tar staining on the fingers may indicate towards chain
smoking, which increases the chance of COPD and lung cancer. Tenderness and swelling of the
joints may indicate towards rheumatological diseases (Thim et al. 2012, p. 117).
Respiratory noises:
Normal- no noises or quite
Respiratory distress: Noises on breathing such as crackles or gasps may indicate some clinical
conditions. For example wheezing is the characteristic symptom of asthma (Kazaks et al. 2012,
p.83-92).
Chest auscultation:
Normal- no wheezes or crackles
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4NURSING ASSESSMENT OF BREATHING
Respiratory distress- Wheeze: expiratory; Presence of fine to coarse crackles, inspiratory stridor.
Auscultation of the lungs is an important part of the respiratory examination and is helpful for
diagnosing various respiratory disorders. Auscultation of the lungs includes breath sounds,
intensity, vocal resonance and adventitious sounds (Csikesz & Gartman 2014,p.277).
.
Respiratory rate:
Normal: Adults: 12-16/ minute, kids: 15-25/ minutes, Babies: 20-40/ minute
Respiratory distress: Tachypnoea- adults >24/min, kids>35/min, babies>50/min.
While measuring the respiratory rate it is essential to assess the color of the lips of the patient.
Patient having respiratory problems might have cyanosed lips. Cyanosis can also be seen in the
ear lobes, in the tip of the nose, nail beds.
Respiratory effort:
Normal- Minimum effort, small chest/abdo movement
Respiratory distress- Marked movement of the chest and the abdomen, use of the abdominal
muscles, sternal retraction, intercostals recession.
Observation of the breathing- to check whether the patient is mouth breathing or pursuing the
lips on expiration or using the abdominal muscled or flaring the nostrils. Flaring of nostrils in
babies indicates towards acute respiratory problem (Thim et al. 2012, p. 117).
Pulse rate:
Respiratory distress- Wheeze: expiratory; Presence of fine to coarse crackles, inspiratory stridor.
Auscultation of the lungs is an important part of the respiratory examination and is helpful for
diagnosing various respiratory disorders. Auscultation of the lungs includes breath sounds,
intensity, vocal resonance and adventitious sounds (Csikesz & Gartman 2014,p.277).
.
Respiratory rate:
Normal: Adults: 12-16/ minute, kids: 15-25/ minutes, Babies: 20-40/ minute
Respiratory distress: Tachypnoea- adults >24/min, kids>35/min, babies>50/min.
While measuring the respiratory rate it is essential to assess the color of the lips of the patient.
Patient having respiratory problems might have cyanosed lips. Cyanosis can also be seen in the
ear lobes, in the tip of the nose, nail beds.
Respiratory effort:
Normal- Minimum effort, small chest/abdo movement
Respiratory distress- Marked movement of the chest and the abdomen, use of the abdominal
muscles, sternal retraction, intercostals recession.
Observation of the breathing- to check whether the patient is mouth breathing or pursuing the
lips on expiration or using the abdominal muscled or flaring the nostrils. Flaring of nostrils in
babies indicates towards acute respiratory problem (Thim et al. 2012, p. 117).
Pulse rate:
5NURSING ASSESSMENT OF BREATHING
Normal- Adults: 60-80 / min
Kids: 80 –120
Babies: 100 –140
Respiratory distress: In case of tachycardia, the signs can be - adults>24/min
Kids>35/ min, babies>50/min.
Skin:
Normal- Pink and normal
Respiratory distress: Sweaty, pale and cyanosis can also occur.
Oximetry:
Normal: 96% _ on room air.
Respiratory distress: 90-95% on room air, <90%= serious hypoxia.
A pulse oximeter is used for measuring the oxygen saturation level of the patient. This will
provide a reading of the oxygenation of the red blood cells. If a pulse oximeter is used then the
patient may require less arterial blood gases performed (Jubran 2015, p. 272).
Pulsus paradoxus- The pulse wave volume decreases with inspiration then it may indicate with
COPD (Thim et al. 2012, p. 117).
Flapping tremor- Indicates retention of the CO2 and thus type 2 respiratory failure (Csikesz &
Gartman 2014,p.277). .
Normal- Adults: 60-80 / min
Kids: 80 –120
Babies: 100 –140
Respiratory distress: In case of tachycardia, the signs can be - adults>24/min
Kids>35/ min, babies>50/min.
Skin:
Normal- Pink and normal
Respiratory distress: Sweaty, pale and cyanosis can also occur.
Oximetry:
Normal: 96% _ on room air.
Respiratory distress: 90-95% on room air, <90%= serious hypoxia.
A pulse oximeter is used for measuring the oxygen saturation level of the patient. This will
provide a reading of the oxygenation of the red blood cells. If a pulse oximeter is used then the
patient may require less arterial blood gases performed (Jubran 2015, p. 272).
Pulsus paradoxus- The pulse wave volume decreases with inspiration then it may indicate with
COPD (Thim et al. 2012, p. 117).
Flapping tremor- Indicates retention of the CO2 and thus type 2 respiratory failure (Csikesz &
Gartman 2014,p.277). .
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6NURSING ASSESSMENT OF BREATHING
Safety measures while respiratory assessment
It is necessary to wash the hands thoroughly between patients to prevent infection.
Respirations should be recorded full minutes for monitoring the respiration pattern and
ensuring the accuracy of the observation (Kazaks et al. 2012 p.83-92).
If the patient is using the oxygen mask or nasal cannula it should be noted that they were
properly placed before the recording. It is also necessary to check that the oxygen flow is
as prescribed and is recorded in the chart.
Part 2
The Roper-Logan-Tierney Model of nursing consists of five components the can be used
for describing the individual in relation to prevent the clinical condition, maintaining of the
health, self efficacy and coping up with the exacerbations (Alligood 2017). The patient centered
nursing according to the R-L-T model, consists of four phases: Assessing, planning,
implementing and evaluating (McCrae 2012,p.222-229).
Assessment
The Roper-Logan-Tierney Model for Nursing is a nursing framework that is based on the
activities of daily living such as breathing (McCrae 2012, 222-229). As per the model it is first
important to find out the main clinical priorities (Aldridge et al. 2011,p.52). If a person with
COPD is considered then the person should mostly have difficulties with breathing, drinking and
swallowing (Jung 2009, p.422-428). At first it is necessary to assess the vital signs of the patient.
COPD is chronic illness that is featured by a permanent obstruction in the airways (Elsherif &
Safety measures while respiratory assessment
It is necessary to wash the hands thoroughly between patients to prevent infection.
Respirations should be recorded full minutes for monitoring the respiration pattern and
ensuring the accuracy of the observation (Kazaks et al. 2012 p.83-92).
If the patient is using the oxygen mask or nasal cannula it should be noted that they were
properly placed before the recording. It is also necessary to check that the oxygen flow is
as prescribed and is recorded in the chart.
Part 2
The Roper-Logan-Tierney Model of nursing consists of five components the can be used
for describing the individual in relation to prevent the clinical condition, maintaining of the
health, self efficacy and coping up with the exacerbations (Alligood 2017). The patient centered
nursing according to the R-L-T model, consists of four phases: Assessing, planning,
implementing and evaluating (McCrae 2012,p.222-229).
Assessment
The Roper-Logan-Tierney Model for Nursing is a nursing framework that is based on the
activities of daily living such as breathing (McCrae 2012, 222-229). As per the model it is first
important to find out the main clinical priorities (Aldridge et al. 2011,p.52). If a person with
COPD is considered then the person should mostly have difficulties with breathing, drinking and
swallowing (Jung 2009, p.422-428). At first it is necessary to assess the vital signs of the patient.
COPD is chronic illness that is featured by a permanent obstruction in the airways (Elsherif &
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING ASSESSMENT OF BREATHING
Noble 2011, p.29-33). This obstruction interferes with the normal breathing. The exacerbation
indicates the worsening of the disease.
It is to be mentioned that a person having COPD can have the vital signs McKinney
2012,p.41) – PaO2: 70 mmHg (↓)
HCO3: 19 mmHg (↓)
SpO2: 88% (↓).
The peak respiratory flow rate is used for assessing the lung function and for determining
the progress of the patient to the medications. The modified early warning score helps to measure
any changes in the patient and recognizing any improvement or deterioration of the patient
(McKinney 2012, p.41).
As mentioned in the previous part of the assignment, assessment of cough is necessary
for checking the capability of the patient to expectorate. The color and the consistency of the
cough would help the nurse in assessing the clinical condition of the patient (Haruna et al. 2010,
p.10)..
One of the clinical characteristics of COPD is pain while breathing. Post sternal pain can
be caused by the infection in the inflammation in the trachea. A visual analog scale was used to
assess the pain (Elsherif & Noble 2011, p.29-33).
Some of the problems that can be identified in patients having COPD are changes in the
respiratory rate, wheezing, coughing, respiratory pain, and production of abnormal sputum
(Haruna et al. 2010, p.10).
Nursing planning
Noble 2011, p.29-33). This obstruction interferes with the normal breathing. The exacerbation
indicates the worsening of the disease.
It is to be mentioned that a person having COPD can have the vital signs McKinney
2012,p.41) – PaO2: 70 mmHg (↓)
HCO3: 19 mmHg (↓)
SpO2: 88% (↓).
The peak respiratory flow rate is used for assessing the lung function and for determining
the progress of the patient to the medications. The modified early warning score helps to measure
any changes in the patient and recognizing any improvement or deterioration of the patient
(McKinney 2012, p.41).
As mentioned in the previous part of the assignment, assessment of cough is necessary
for checking the capability of the patient to expectorate. The color and the consistency of the
cough would help the nurse in assessing the clinical condition of the patient (Haruna et al. 2010,
p.10)..
One of the clinical characteristics of COPD is pain while breathing. Post sternal pain can
be caused by the infection in the inflammation in the trachea. A visual analog scale was used to
assess the pain (Elsherif & Noble 2011, p.29-33).
Some of the problems that can be identified in patients having COPD are changes in the
respiratory rate, wheezing, coughing, respiratory pain, and production of abnormal sputum
(Haruna et al. 2010, p.10).
Nursing planning
8NURSING ASSESSMENT OF BREATHING
The main nursing goal to deal with a patient having COPD is to prevent the potential
exacerbation of the problems. Other aims includes, enabling the patient to breathe comfortably
(Elsherif & Noble 2011, p.29-33). Maintaining the oxygen saturation rate above 90%, ensure
effective coughing; reduce the anxiety in the patient and an infection free respiratory tract.
Another goal is to enable the patient to use oxygen and inhale correctly (McCrae 2012,p. 222-
229).
Interventions
In order to improve the breathing, psychological and the physiological, socio-cultural and
the environmental factors should be taken in to account. The patient should be kept in an upright
position in order to assist the expansion of the lungs. The vital signs of the patient have to be
checked after every 15 minutes (Elsherif & Noble 2011, p.29-33).
After the provision of oxygen, the arterial blood gases should be rechecked for allowing
the detection of any augmented concentration of the carbon-dioxide or the falling pH (Jung 2009,
p.422-428). As per the NICE guidelines, it is recommended that the patient can be given oxygen
by a venturi mask that would help to deliver the accurate oxygen concentration. In order to
improve the breathing pattern in the patient, humidification device can be given after discussing
with the doctor (Holland 2008, p.265-288). Short-acting beta 2-agonist bronchodilator can be
given for relaxing the smooth muscles and improve the breathing. Patients who have frequent
episodes of COPD exacerbations, bronchodilators can also be provided by the help of nebulizers.
Nurses should encourage the patient for fluid intake as intake fluid helps in thinning of the
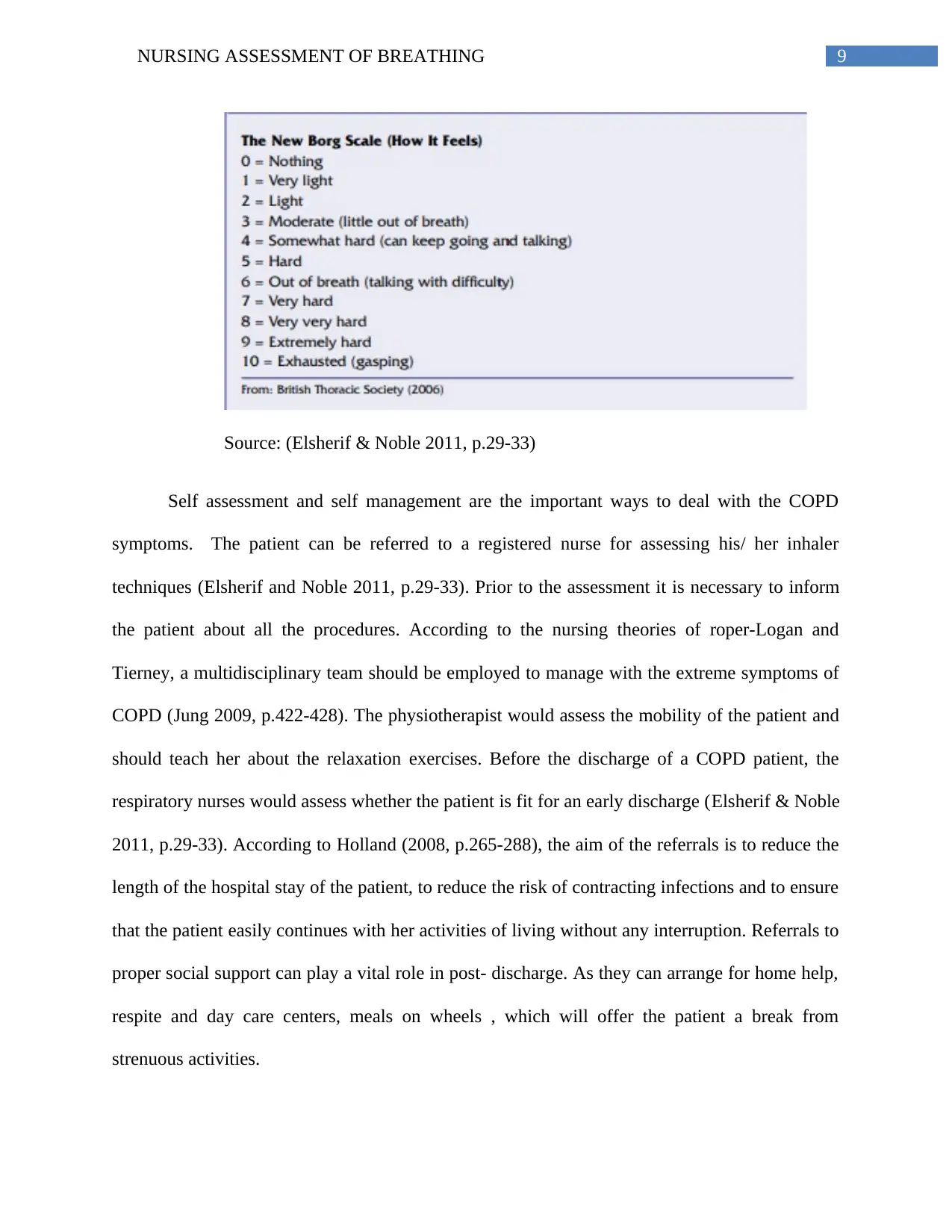
secretions. The New Borg Scale can be used to assess how the patient feels (Elsherif & Noble
2011, p.29-33).
The main nursing goal to deal with a patient having COPD is to prevent the potential
exacerbation of the problems. Other aims includes, enabling the patient to breathe comfortably
(Elsherif & Noble 2011, p.29-33). Maintaining the oxygen saturation rate above 90%, ensure
effective coughing; reduce the anxiety in the patient and an infection free respiratory tract.
Another goal is to enable the patient to use oxygen and inhale correctly (McCrae 2012,p. 222-
229).
Interventions
In order to improve the breathing, psychological and the physiological, socio-cultural and
the environmental factors should be taken in to account. The patient should be kept in an upright
position in order to assist the expansion of the lungs. The vital signs of the patient have to be
checked after every 15 minutes (Elsherif & Noble 2011, p.29-33).
After the provision of oxygen, the arterial blood gases should be rechecked for allowing
the detection of any augmented concentration of the carbon-dioxide or the falling pH (Jung 2009,
p.422-428). As per the NICE guidelines, it is recommended that the patient can be given oxygen
by a venturi mask that would help to deliver the accurate oxygen concentration. In order to
improve the breathing pattern in the patient, humidification device can be given after discussing
with the doctor (Holland 2008, p.265-288). Short-acting beta 2-agonist bronchodilator can be
given for relaxing the smooth muscles and improve the breathing. Patients who have frequent
episodes of COPD exacerbations, bronchodilators can also be provided by the help of nebulizers.
Nurses should encourage the patient for fluid intake as intake fluid helps in thinning of the
secretions. The New Borg Scale can be used to assess how the patient feels (Elsherif & Noble
2011, p.29-33).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9NURSING ASSESSMENT OF BREATHING
Source: (Elsherif & Noble 2011, p.29-33)
Self assessment and self management are the important ways to deal with the COPD
symptoms. The patient can be referred to a registered nurse for assessing his/ her inhaler
techniques (Elsherif and Noble 2011, p.29-33). Prior to the assessment it is necessary to inform
the patient about all the procedures. According to the nursing theories of roper-Logan and
Tierney, a multidisciplinary team should be employed to manage with the extreme symptoms of
COPD (Jung 2009, p.422-428). The physiotherapist would assess the mobility of the patient and
should teach her about the relaxation exercises. Before the discharge of a COPD patient, the
respiratory nurses would assess whether the patient is fit for an early discharge (Elsherif & Noble
2011, p.29-33). According to Holland (2008, p.265-288), the aim of the referrals is to reduce the
length of the hospital stay of the patient, to reduce the risk of contracting infections and to ensure
that the patient easily continues with her activities of living without any interruption. Referrals to
proper social support can play a vital role in post- discharge. As they can arrange for home help,
respite and day care centers, meals on wheels , which will offer the patient a break from
strenuous activities.
Source: (Elsherif & Noble 2011, p.29-33)
Self assessment and self management are the important ways to deal with the COPD
symptoms. The patient can be referred to a registered nurse for assessing his/ her inhaler
techniques (Elsherif and Noble 2011, p.29-33). Prior to the assessment it is necessary to inform
the patient about all the procedures. According to the nursing theories of roper-Logan and
Tierney, a multidisciplinary team should be employed to manage with the extreme symptoms of
COPD (Jung 2009, p.422-428). The physiotherapist would assess the mobility of the patient and
should teach her about the relaxation exercises. Before the discharge of a COPD patient, the
respiratory nurses would assess whether the patient is fit for an early discharge (Elsherif & Noble
2011, p.29-33). According to Holland (2008, p.265-288), the aim of the referrals is to reduce the
length of the hospital stay of the patient, to reduce the risk of contracting infections and to ensure
that the patient easily continues with her activities of living without any interruption. Referrals to
proper social support can play a vital role in post- discharge. As they can arrange for home help,
respite and day care centers, meals on wheels , which will offer the patient a break from
strenuous activities.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10NURSING ASSESSMENT OF BREATHING
It is to be noted that in most of the cases the COPD is mainly caused by the bacterial or
viral infections, hence vaccinations can be given to lessen the number of the exacerbation
episodes. Pneumococcal and flu vaccinations can be given. According to Hemming (2010, p.
171), patients with acute respiratory distress can be referred to pulmonary rehabilitation, where a
multi-disciplinary approach can be provided, where the patient will be educated about the
routined exercises, nutritional advice and other tips (Hemming 2010, p.171). The patient’s
weight should be checked for once in every week. Such a program will be able to improve the
patient's breathing, reduced level of anxiety and self management of the clinical condition. It has
to be remembered that respiratory distress affects the patient both physically and psychologically
as regular episodes of breathlessness can bring about distress in the personal as well as the
professional life; this can impact further on her breathing and dyspnoea (Holland 2008, p.265-
288). Assistance with dressing, washing and toileting may increase the confidence in the patient
(Hemming 2010, p.171). Patients having distressing episodes of respiratory distress may have
lost appetite that can affect their body mass index and the nutritional status. The patient should
be encouraged to take a balanced diet and enough exercises.
Evaluation
Evaluation of the patient’s condition can be done by asking the patient about any
respiratory distress. The visual analog pain assessment scale can be used to determine if the chest
pain have subsided. The patient would become more competent to use the bronchodilators or the
nebulizers. He/ she will be able to do the exercises properly. The patient would be able to
expectorate the cough easily. Correct nursing assessment would help to get beck the vital signs to
normal. The SpO2 would be above 90 percent, which would indicate a low risk of the clinical
It is to be noted that in most of the cases the COPD is mainly caused by the bacterial or
viral infections, hence vaccinations can be given to lessen the number of the exacerbation
episodes. Pneumococcal and flu vaccinations can be given. According to Hemming (2010, p.
171), patients with acute respiratory distress can be referred to pulmonary rehabilitation, where a
multi-disciplinary approach can be provided, where the patient will be educated about the
routined exercises, nutritional advice and other tips (Hemming 2010, p.171). The patient’s
weight should be checked for once in every week. Such a program will be able to improve the
patient's breathing, reduced level of anxiety and self management of the clinical condition. It has
to be remembered that respiratory distress affects the patient both physically and psychologically
as regular episodes of breathlessness can bring about distress in the personal as well as the
professional life; this can impact further on her breathing and dyspnoea (Holland 2008, p.265-
288). Assistance with dressing, washing and toileting may increase the confidence in the patient
(Hemming 2010, p.171). Patients having distressing episodes of respiratory distress may have
lost appetite that can affect their body mass index and the nutritional status. The patient should
be encouraged to take a balanced diet and enough exercises.
Evaluation
Evaluation of the patient’s condition can be done by asking the patient about any
respiratory distress. The visual analog pain assessment scale can be used to determine if the chest
pain have subsided. The patient would become more competent to use the bronchodilators or the
nebulizers. He/ she will be able to do the exercises properly. The patient would be able to
expectorate the cough easily. Correct nursing assessment would help to get beck the vital signs to
normal. The SpO2 would be above 90 percent, which would indicate a low risk of the clinical
11NURSING ASSESSMENT OF BREATHING
condition. The patient will show less anxiety. The nutritional assessment of the patient would
show a good nutritional status. The patient would say that he was feeling better.
condition. The patient will show less anxiety. The nutritional assessment of the patient would
show a good nutritional status. The patient would say that he was feeling better.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.