Comprehensive Analysis of COVID-19: Symptoms, Risks, and Prevention
VerifiedAdded on 2022/09/14
|9
|2473
|12
Report
AI Summary
This report provides a comprehensive overview of COVID-19, the novel coronavirus that emerged in late 2019, causing a global pandemic. It details the virus's characteristics, including its structure and mechanism of infection. The report outlines the various signs and symptoms of the disease, from mild to critical, and discusses the diagnostic criteria used to assess the severity of the infection. It also examines the clinical features, including the potential for pneumonia, ARDS, and other complications, alongside the risk factors associated with severe outcomes, such as age and pre-existing health conditions. Furthermore, the report emphasizes the importance of prevention strategies, including hygiene practices and social distancing, as recommended by the WHO and other health organizations. Statistical analyses and case studies from specific locations, such as Beijing, are included to provide insights into the geographical variations and clinical presentations of COVID-19. The report references relevant studies and research to support its findings.
Introduction:
During December 2019, the initial outbreak in Wuhan, the national and global reaction
to COVID-19 has been first identified. Generally, COVID-19 is an intensely controlled illness
but it may still be lethal, with a fatality incidence of 2 per cent. The advent of serious illness
may lead to death due to major alveolar damage and gradual respiratory failure. Since Feb 15,
there were nearly 66 580 confirmed reports and more than 1524 fatalities by this infection.
Following the advice of the WHO, the majority of countries carried out comprehensive
research, contact identification, separation and infection testing. The other strategies that
separate citizens from one another to reduce physical contact. The rising question about the
pandemic is what is the disease that caused massive deaths with a morbidity rate 2%.
This is a type of virus triggers that respiratory infection formerly known as corornavirus
diseases is renamed as COVID-19 or novel corona virus. This can induce inflammation and
develop mucus as well as fluids in the lungs 'airways that is medically known as pneumonia.
There are loads of different coronaviruses. Several of such viruses infect only livestock,
although some of them may also alter their mechanism of action and infect humans. The
viruses are tiny microscopic organism and depends on a host to get replicated. The primary
genetic material of all the viruses can be DNA or RNA including a protein coating for
protection. The viruses lacks in the protein machinery needed for the replication and hence
depend on the host machinery to reproduce. The viruses insert their unique genetic material in
the host cell nucleus and by hijacking the host protein making machinery get replicated
(Dimmock, Easton & Leppard, 2016).
Coronavirus ha a single stranded RNA including a protein “crown” that seems to be
spiky. The name corona came from the unique shape, as corona means “crown” in Latin. The
crown serves as the connection between the host and the virus that allows the virus protein
inside the host (Sheposh, 2020, Millet, & Whittaker, 2015).
During December 2019, the initial outbreak in Wuhan, the national and global reaction
to COVID-19 has been first identified. Generally, COVID-19 is an intensely controlled illness
but it may still be lethal, with a fatality incidence of 2 per cent. The advent of serious illness
may lead to death due to major alveolar damage and gradual respiratory failure. Since Feb 15,
there were nearly 66 580 confirmed reports and more than 1524 fatalities by this infection.
Following the advice of the WHO, the majority of countries carried out comprehensive
research, contact identification, separation and infection testing. The other strategies that
separate citizens from one another to reduce physical contact. The rising question about the
pandemic is what is the disease that caused massive deaths with a morbidity rate 2%.
This is a type of virus triggers that respiratory infection formerly known as corornavirus
diseases is renamed as COVID-19 or novel corona virus. This can induce inflammation and
develop mucus as well as fluids in the lungs 'airways that is medically known as pneumonia.
There are loads of different coronaviruses. Several of such viruses infect only livestock,
although some of them may also alter their mechanism of action and infect humans. The
viruses are tiny microscopic organism and depends on a host to get replicated. The primary
genetic material of all the viruses can be DNA or RNA including a protein coating for
protection. The viruses lacks in the protein machinery needed for the replication and hence
depend on the host machinery to reproduce. The viruses insert their unique genetic material in
the host cell nucleus and by hijacking the host protein making machinery get replicated
(Dimmock, Easton & Leppard, 2016).
Coronavirus ha a single stranded RNA including a protein “crown” that seems to be
spiky. The name corona came from the unique shape, as corona means “crown” in Latin. The
crown serves as the connection between the host and the virus that allows the virus protein
inside the host (Sheposh, 2020, Millet, & Whittaker, 2015).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Definition of Covid-19
COVID-19 (coronavirus disease 2019) is an infection of the respiratory tract with a
recently identified coronavirus, believed to have developed as a zoonotic virus, which then get
evolved or mutated in such a way that can affect the human. (n.d.).
Origin
In late 2019, an epidemic of the disease occurred in China. The infection is thought to have
developed in animals and to have transferred to humans, although scientists remain uncertain
of the precise cause of the pandemic. COVID-19 had expanded to almost 180 countries in
only a few months, alarming the World Health Organisation (WHO) to count a health
emergency (Sheposh, 2020).
Signs and symptoms:
For a total for 72 314 cases 44 672 were listed as COVID-19 verified cases For a total
for 72 314 cases 44 672 were listed as COVID-19 verified cases as per a recent study. 62%
detection of positive check findings with viral nucleic acid on throat swab tests. 16 186 as
reported cases that is 22% evaluation focused purely on signs and conditions, no study was
conducted because the potential of testing is inadequate to satisfy existing needs. e.), 10 567
as 15 percent scientifically treated cases; this classification is applied only in the province of
Hubei and the diagnosis is only symptom and exposure based as no standard test was applied
in this 15% case. However, involvement of lung imaging symptoms associated with
coronavirus pneumonia, including asymptomatic events in 889 cases that count as 1%. The
findinds are contrasting as diagnosis of viral nucleic acid give positive result but but there
is absence of signs such as nausea, dry cough and fatigue(Wu & McGoogan, 2020).
COVID-19 (coronavirus disease 2019) is an infection of the respiratory tract with a
recently identified coronavirus, believed to have developed as a zoonotic virus, which then get
evolved or mutated in such a way that can affect the human. (n.d.).
Origin
In late 2019, an epidemic of the disease occurred in China. The infection is thought to have
developed in animals and to have transferred to humans, although scientists remain uncertain
of the precise cause of the pandemic. COVID-19 had expanded to almost 180 countries in
only a few months, alarming the World Health Organisation (WHO) to count a health
emergency (Sheposh, 2020).
Signs and symptoms:
For a total for 72 314 cases 44 672 were listed as COVID-19 verified cases For a total
for 72 314 cases 44 672 were listed as COVID-19 verified cases as per a recent study. 62%
detection of positive check findings with viral nucleic acid on throat swab tests. 16 186 as
reported cases that is 22% evaluation focused purely on signs and conditions, no study was
conducted because the potential of testing is inadequate to satisfy existing needs. e.), 10 567
as 15 percent scientifically treated cases; this classification is applied only in the province of
Hubei and the diagnosis is only symptom and exposure based as no standard test was applied
in this 15% case. However, involvement of lung imaging symptoms associated with
coronavirus pneumonia, including asymptomatic events in 889 cases that count as 1%. The
findinds are contrasting as diagnosis of viral nucleic acid give positive result but but there
is absence of signs such as nausea, dry cough and fatigue(Wu & McGoogan, 2020).
Classified by severity of clinical symptoms of the disease:
Mild disease:
Non-pneumonia and moderate pneumonia which is manifested in 81 per cent of cases
that happened.
Severe disease:
Shortness of breath or dyspenea, the respiratory rate reduces down to lesser than
30/min, PaO2/FiO2 ratio or P/F that is the ratio between the blood pressure of the oxygen
(partial pressure of oxygen, PaO2), the percentage of oxygen supplied (fraction of inspired
oxygen, FiO2)] lesser than 300, and blood oxygen saturation (SpO2) lesser than or equal to
93%, and/or lung infiltrates higher than 50% within the next 24 to 48 hours. This symptoms
found to happen in 14% of the cases.
Critical disease: Myocardial infarction, septic shock, and/or multiple organ dysfunction
(MOD) or failure (MOF); this conditions are manifested in almost 5% of cases (Cascella etl.,
2020).
Statistical analysis of reports of Policy Agencies enable the medical symptoms of the disease
to be separated as per the extent of the medical images.
Location:
A study targeted people of Beijing to understand the effect of geographical location in
the COVID-19 patients. In order to evaluate the clinical and epidemiological features of
COVID-19 in Beijing, data from 262 reported cases were analyzed by the researchers. The
study is primarily based on the findings of quantitate analysis of COVID-19 infection as per
its seriousness. The study concluded that the features of patients diagnosed with COVID-19 in
Beijing clearly varied from those in Wuhan including lesser mortality rate and better
discharge levels, with new diagnosed patients slowly moving from imported to local. Also the
steps for preventing transmission at a preliminary stage were quite promising. By the case
Mild disease:
Non-pneumonia and moderate pneumonia which is manifested in 81 per cent of cases
that happened.
Severe disease:
Shortness of breath or dyspenea, the respiratory rate reduces down to lesser than
30/min, PaO2/FiO2 ratio or P/F that is the ratio between the blood pressure of the oxygen
(partial pressure of oxygen, PaO2), the percentage of oxygen supplied (fraction of inspired
oxygen, FiO2)] lesser than 300, and blood oxygen saturation (SpO2) lesser than or equal to
93%, and/or lung infiltrates higher than 50% within the next 24 to 48 hours. This symptoms
found to happen in 14% of the cases.
Critical disease: Myocardial infarction, septic shock, and/or multiple organ dysfunction
(MOD) or failure (MOF); this conditions are manifested in almost 5% of cases (Cascella etl.,
2020).
Statistical analysis of reports of Policy Agencies enable the medical symptoms of the disease
to be separated as per the extent of the medical images.
Location:
A study targeted people of Beijing to understand the effect of geographical location in
the COVID-19 patients. In order to evaluate the clinical and epidemiological features of
COVID-19 in Beijing, data from 262 reported cases were analyzed by the researchers. The
study is primarily based on the findings of quantitate analysis of COVID-19 infection as per
its seriousness. The study concluded that the features of patients diagnosed with COVID-19 in
Beijing clearly varied from those in Wuhan including lesser mortality rate and better
discharge levels, with new diagnosed patients slowly moving from imported to local. Also the
steps for preventing transmission at a preliminary stage were quite promising. By the case
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
study they recommend that the next measures on COVID-19 infection will concentrate on
advanced patient isolation and on quarantine for close associations in Beijing's families and
societies (Tian et al., 2020).
COVID-19 can cause mild, medium, or serious diseased condition. Extreme diarrhea, ARDS,
sepsis shock, and sepsis are among the serious health symptoms. The clinical development
to the disorder tends to be forecasting a positive development among most of the cases in the
patient. The clinical condition are found to be worsening with heart failure and MOD/MOF,
in some of the cases after a week. The criteria for both the extent of respiratory
insufficient , sepsis and septic shock diagnosis requirements should be seen as a guide.[13]
Uncomplicated (mild) Illness
This patients typically have signs of a viral infection in the upper respiratory tract,
including moderate fever, dry cough , nasal stiffness, malaise, sore throat, fatigue, body pain
or discomfort. There are no indicators or symptoms for a more severe disorder, like shortness
of breath. Non-respiratory signs including diarrhea are difficult to identify when contrasted to
prior HCoV infections.
A study of an array of family of 5 COVID-19 pneumonia patients in Anyang, China,
had interaction with an asymptomatic family member who had returned from the Wuhan
outbreak center prior to their initiation of symptoms. The chain of incidents shows that the
asymptomatic carrier has the potential to spread the coronavirus. The incubation time may
varies from patient to patient but can be visible within 19 days. However the reporting time is
0 to 24 days (Bai et al., 2020).
advanced patient isolation and on quarantine for close associations in Beijing's families and
societies (Tian et al., 2020).
COVID-19 can cause mild, medium, or serious diseased condition. Extreme diarrhea, ARDS,
sepsis shock, and sepsis are among the serious health symptoms. The clinical development
to the disorder tends to be forecasting a positive development among most of the cases in the
patient. The clinical condition are found to be worsening with heart failure and MOD/MOF,
in some of the cases after a week. The criteria for both the extent of respiratory
insufficient , sepsis and septic shock diagnosis requirements should be seen as a guide.[13]
Uncomplicated (mild) Illness
This patients typically have signs of a viral infection in the upper respiratory tract,
including moderate fever, dry cough , nasal stiffness, malaise, sore throat, fatigue, body pain
or discomfort. There are no indicators or symptoms for a more severe disorder, like shortness
of breath. Non-respiratory signs including diarrhea are difficult to identify when contrasted to
prior HCoV infections.
A study of an array of family of 5 COVID-19 pneumonia patients in Anyang, China,
had interaction with an asymptomatic family member who had returned from the Wuhan
outbreak center prior to their initiation of symptoms. The chain of incidents shows that the
asymptomatic carrier has the potential to spread the coronavirus. The incubation time may
varies from patient to patient but can be visible within 19 days. However the reporting time is
0 to 24 days (Bai et al., 2020).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Moderate Pneumonia
There are respiratory problems such as cough and dyspnea in adults and tachypnea in
infants but no evidence of serious pneumonia.
Severe Pneumonia
Fever with the additional symptom of severe respiratory distress, dyspnea, tachypnea with
breath rates greater than 30 breaths/min and hypoxia with SpO2 lesser than 90% on normal
room condition. The sign of fever should be closely evaluated as it can be mild or sometimes
missing even in extreme cases of the disease. Children can suffer from Cyanosis. The
assessment is clinical, and symptoms are removed by the help of radiological imaging (Xu et
al., 2010).
Acute Respiratory Distress Syndrome (ARDS)
Medical and ventilator requirements are needed for the diagnosis. The disorder indicates a
severe new-onset heart failure or aggravation of pre-established respiratory condition.
Specific types of ARDS are classified according to the extent of hypoxia. The classification is
according to the ratio PaO2/FiO2:
Mild ARDS: PaO2/FiO2 range in between 200 mmHg to 300 mmHg. For non-
ventilated or non-invasive ventilation (NIV) cases application of strong end-expiratory
pressure (PEEP) or a continuous positive airway pressure (CPAP) that is greater than
or equal to the pressure of cmH2O.
Moderate ARDS: PaO2/FiO2 in between the range of 100 mmHg to 200 mmHg.
Severe ARDS: PaO2/FiO2 that can be lesser than 100mmHg or equal to 100 mmHg.
A ratio of SpO2/FiO2 to some 315 is indicative of ARDS if PaO2 is unavailable.
The bilateral opacities with lung infiltrates greater than 50% found by chest imaging using
modern techniques like chest radiograph, CT scan, or lung ultrasound is not fully supported
by effusions, lung collapse, or lobar. Although clinical circumstance and ventilator evidence
There are respiratory problems such as cough and dyspnea in adults and tachypnea in
infants but no evidence of serious pneumonia.
Severe Pneumonia
Fever with the additional symptom of severe respiratory distress, dyspnea, tachypnea with
breath rates greater than 30 breaths/min and hypoxia with SpO2 lesser than 90% on normal
room condition. The sign of fever should be closely evaluated as it can be mild or sometimes
missing even in extreme cases of the disease. Children can suffer from Cyanosis. The
assessment is clinical, and symptoms are removed by the help of radiological imaging (Xu et
al., 2010).
Acute Respiratory Distress Syndrome (ARDS)
Medical and ventilator requirements are needed for the diagnosis. The disorder indicates a
severe new-onset heart failure or aggravation of pre-established respiratory condition.
Specific types of ARDS are classified according to the extent of hypoxia. The classification is
according to the ratio PaO2/FiO2:
Mild ARDS: PaO2/FiO2 range in between 200 mmHg to 300 mmHg. For non-
ventilated or non-invasive ventilation (NIV) cases application of strong end-expiratory
pressure (PEEP) or a continuous positive airway pressure (CPAP) that is greater than
or equal to the pressure of cmH2O.
Moderate ARDS: PaO2/FiO2 in between the range of 100 mmHg to 200 mmHg.
Severe ARDS: PaO2/FiO2 that can be lesser than 100mmHg or equal to 100 mmHg.
A ratio of SpO2/FiO2 to some 315 is indicative of ARDS if PaO2 is unavailable.
The bilateral opacities with lung infiltrates greater than 50% found by chest imaging using
modern techniques like chest radiograph, CT scan, or lung ultrasound is not fully supported
by effusions, lung collapse, or lobar. Although clinical circumstance and ventilator evidence
can be indicative of pulmonary edema in certain situations, the main respiratory source of the
edema is confirmed after heart failure or certain triggers like fluid overload are removed.
Echocardiography is a effective technique in this situations (Cascella etl., 2020).
Pulmonary CT Evaluation
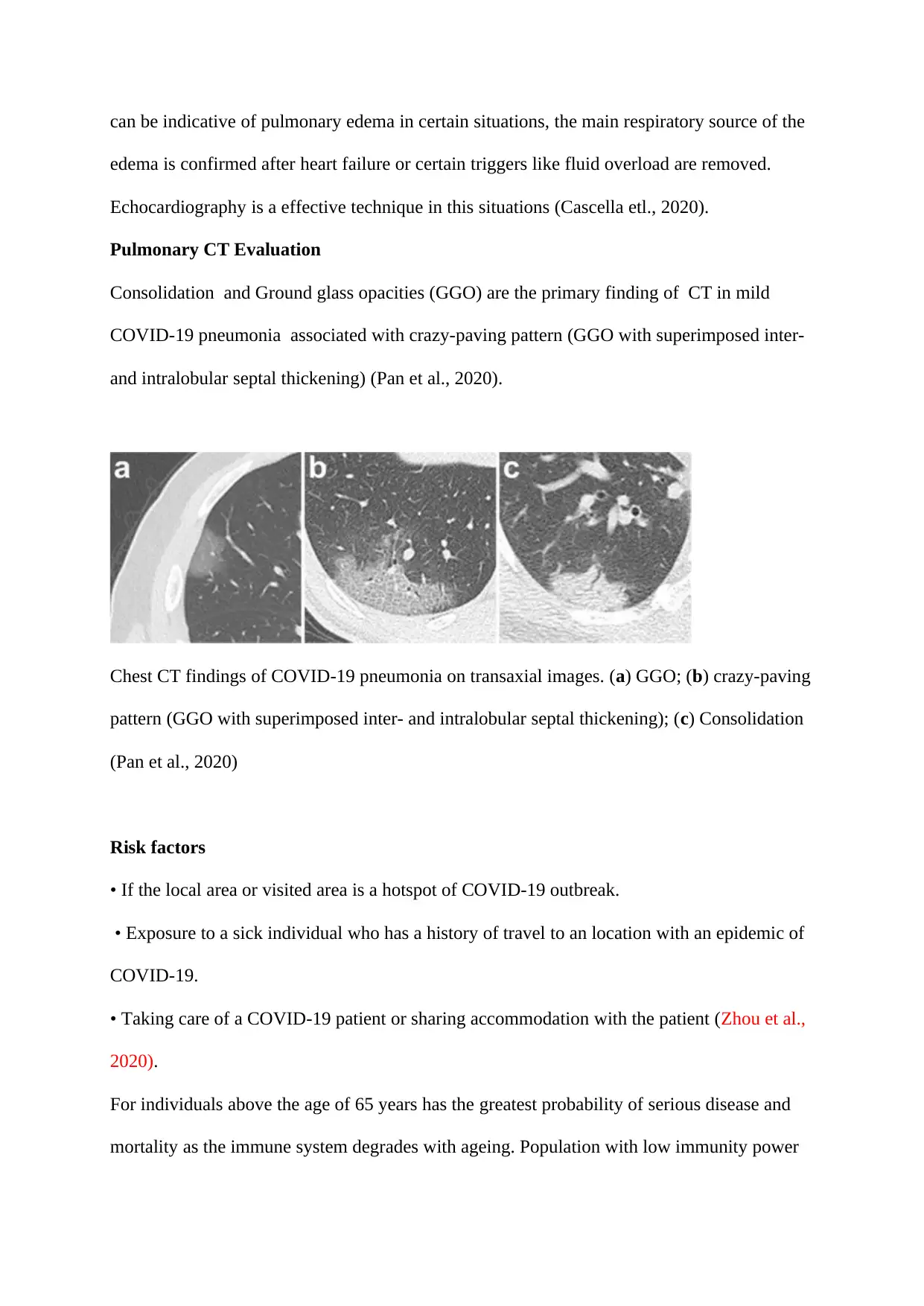
Consolidation and Ground glass opacities (GGO) are the primary finding of CT in mild
COVID-19 pneumonia associated with crazy-paving pattern (GGO with superimposed inter-
and intralobular septal thickening) (Pan et al., 2020).
Chest CT findings of COVID-19 pneumonia on transaxial images. (a) GGO; (b) crazy-paving
pattern (GGO with superimposed inter- and intralobular septal thickening); (c) Consolidation
(Pan et al., 2020)
Risk factors
• If the local area or visited area is a hotspot of COVID-19 outbreak.
• Exposure to a sick individual who has a history of travel to an location with an epidemic of
COVID-19.
• Taking care of a COVID-19 patient or sharing accommodation with the patient (Zhou et al.,
2020).
For individuals above the age of 65 years has the greatest probability of serious disease and
mortality as the immune system degrades with ageing. Population with low immunity power
edema is confirmed after heart failure or certain triggers like fluid overload are removed.
Echocardiography is a effective technique in this situations (Cascella etl., 2020).
Pulmonary CT Evaluation
Consolidation and Ground glass opacities (GGO) are the primary finding of CT in mild
COVID-19 pneumonia associated with crazy-paving pattern (GGO with superimposed inter-
and intralobular septal thickening) (Pan et al., 2020).
Chest CT findings of COVID-19 pneumonia on transaxial images. (a) GGO; (b) crazy-paving
pattern (GGO with superimposed inter- and intralobular septal thickening); (c) Consolidation
(Pan et al., 2020)
Risk factors
• If the local area or visited area is a hotspot of COVID-19 outbreak.
• Exposure to a sick individual who has a history of travel to an location with an epidemic of
COVID-19.
• Taking care of a COVID-19 patient or sharing accommodation with the patient (Zhou et al.,
2020).
For individuals above the age of 65 years has the greatest probability of serious disease and
mortality as the immune system degrades with ageing. Population with low immunity power
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
and Anyone with pre-existing condition of asthma, coronary disease, lung diabetes,
disorder, or kidney disease (Sheposh, 2020).
Prevention
The prevention recommendation by the WHO and other standard organizations are listed
below:
Eliminate the possibility of near communication with people with severe respiratory
infections.
Frequent hand washing with soap or disinfectants, especially if there is a doubt of
exposure to the virus.
Use protection when coming in contact with wild animals or farm visit.
Persons with severe airway infection signs must maintain their distance, use tissue
during sneezing and dispose the tissue immediately. They are also recommended to
wash their hand frequently (Who.int, 2020).
To reinforce, in specific, the implementation of rigorous sanitation procedures for the
safeguard and cure of infections in emergency medicine departments.
Immunocompromised person must not attain any kind of public gatherings(Cascella
etl., 2020).
disorder, or kidney disease (Sheposh, 2020).
Prevention
The prevention recommendation by the WHO and other standard organizations are listed
below:
Eliminate the possibility of near communication with people with severe respiratory
infections.
Frequent hand washing with soap or disinfectants, especially if there is a doubt of
exposure to the virus.
Use protection when coming in contact with wild animals or farm visit.
Persons with severe airway infection signs must maintain their distance, use tissue
during sneezing and dispose the tissue immediately. They are also recommended to
wash their hand frequently (Who.int, 2020).
To reinforce, in specific, the implementation of rigorous sanitation procedures for the
safeguard and cure of infections in emergency medicine departments.
Immunocompromised person must not attain any kind of public gatherings(Cascella
etl., 2020).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Refernces:
Bai, Y., Yao, L., Wei, T., Tian, F., Jin, D. Y., Chen, L., & Wang, M. (2020). Presumed
asymptomatic carrier transmission of COVID-19. Jama.
Cascella, M., Rajnik, M., Cuomo, A., Dulebohn, S. C., & Di Napoli, R. (2020). Features,
evaluation and treatment coronavirus (COVID-19). In StatPearls [Internet]. StatPearls
Publishing.
Dimmock, N. J., Easton, A. J., & Leppard, K. N. (2016). Introduction to modern virology.
John Wiley & Sons.
https://www.elsevier.com/__data/assets/pdf_file/0007/991366/COVID-19_120320.pdf
Millet, J. K., & Whittaker, G. R. (2015). Host cell proteases: Critical determinants of
coronavirus tropism and pathogenesis. Virus research, 202, 120-134.
Pan, F., Ye, T., Sun, P., Gui, S., Liang, B., Li, L., ... & Zheng, C. (2020). Time course of lung
changes on chest CT during recovery from 2019 novel coronavirus (COVID-19)
pneumonia. Radiology, 200370.
Sheposh, R. (2020). Coronavirus 2019 (COVID-19). Salem Press Encyclopedia of Health.
Tian, S., Hu, N., Lou, J., Chen, K., Kang, X., Xiang, Z., ... & Chen, G. (2020). Characteristics
of COVID-19 infection in Beijing. Journal of Infection.
Who.int. (2020). Advice for public. Retrieved 7 April 2020, from
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
Wu, Z., & McGoogan, J. M. (2020). Characteristics of and important lessons from the
coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72
314 cases from the Chinese Center for Disease Control and Prevention. Jama.
Www, www-clinicalkey-com.sdl.idm.oclc.org/#!/content/clinical_overview/67-s2.0-
0e7112a3-e94d-4136-94ba-cfdf9242ea43?scrollTo=#clinical-clarification-heading-6.
Bai, Y., Yao, L., Wei, T., Tian, F., Jin, D. Y., Chen, L., & Wang, M. (2020). Presumed
asymptomatic carrier transmission of COVID-19. Jama.
Cascella, M., Rajnik, M., Cuomo, A., Dulebohn, S. C., & Di Napoli, R. (2020). Features,
evaluation and treatment coronavirus (COVID-19). In StatPearls [Internet]. StatPearls
Publishing.
Dimmock, N. J., Easton, A. J., & Leppard, K. N. (2016). Introduction to modern virology.
John Wiley & Sons.
https://www.elsevier.com/__data/assets/pdf_file/0007/991366/COVID-19_120320.pdf
Millet, J. K., & Whittaker, G. R. (2015). Host cell proteases: Critical determinants of
coronavirus tropism and pathogenesis. Virus research, 202, 120-134.
Pan, F., Ye, T., Sun, P., Gui, S., Liang, B., Li, L., ... & Zheng, C. (2020). Time course of lung
changes on chest CT during recovery from 2019 novel coronavirus (COVID-19)
pneumonia. Radiology, 200370.
Sheposh, R. (2020). Coronavirus 2019 (COVID-19). Salem Press Encyclopedia of Health.
Tian, S., Hu, N., Lou, J., Chen, K., Kang, X., Xiang, Z., ... & Chen, G. (2020). Characteristics
of COVID-19 infection in Beijing. Journal of Infection.
Who.int. (2020). Advice for public. Retrieved 7 April 2020, from
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
Wu, Z., & McGoogan, J. M. (2020). Characteristics of and important lessons from the
coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72
314 cases from the Chinese Center for Disease Control and Prevention. Jama.
Www, www-clinicalkey-com.sdl.idm.oclc.org/#!/content/clinical_overview/67-s2.0-
0e7112a3-e94d-4136-94ba-cfdf9242ea43?scrollTo=#clinical-clarification-heading-6.

Xu, Z., Shi, L., Wang, Y., Zhang, J., Huang, L., Zhang, C., ... & Tai, Y. (2020). Pathological
findings of COVID-19 associated with acute respiratory distress syndrome. The
Lancet respiratory medicine, 8(4), 420-422.
Zhou, F., Yu, T., Du, R., Fan, G., Liu, Y., Liu, Z., ... & Guan, L. (2020). Clinical course and
risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a
retrospective cohort study. The Lancet.
findings of COVID-19 associated with acute respiratory distress syndrome. The
Lancet respiratory medicine, 8(4), 420-422.
Zhou, F., Yu, T., Du, R., Fan, G., Liu, Y., Liu, Z., ... & Guan, L. (2020). Clinical course and
risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a
retrospective cohort study. The Lancet.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.