Critical Reflection: First People Healthcare and Australian Policies
VerifiedAdded on 2021/06/17
|9
|2673
|104
Essay
AI Summary
This essay presents a critical reflection on First People healthcare within the context of professional practice, focusing on the impact of historical policies, particularly the protection and segregation era (1890-1950), on Indigenous Australians. The essay explores themes such as perceived inferiority, social Darwinism, custom alienation, and poor living conditions, analyzing their adverse effects on the health and well-being of Indigenous communities. The author reflects on their own cultural background, life experiences, and worldview, acknowledging how these factors influence their perceptions and interactions with Indigenous people in healthcare settings. The essay discusses the importance of cultural awareness, respect, and competence in delivering person-centered care, emphasizing the need to address historical trauma, promote equity, and adopt a holistic approach to healthcare. The reflection highlights the author's increased understanding of the historical context and its ongoing impact, emphasizing the importance of recognizing human rights, self-determination, and family/kinship structures within Indigenous communities. The essay concludes by outlining the author's commitment to integrating cultural awareness, respect, and competence into their professional practice to improve healthcare outcomes for Indigenous Australians.

UNIT:
NAME:
DATE:
NAME:
DATE:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Critical Reflection
Introduction
Understanding first people health care is an important part in delivering a person centered health
care in professional practice. The Australian history from colonization and policy has had
adverse health effect to the indigenous Australians. Indigenous people/ first people in Australia
refer to Aboriginals and Torres Islander Slate who occupied Australia before colonization
(Kirmayer, 2012). The indigenous people had their culture, way of knowing and doing things
and a history for their community. Colonization and subsequent government policies undermined
indigenous people way of life whose effects are also felt in today’s indigenous communities. The
unit on first people health and practice has exposed me so several policies that affected the
indigenous communities that give me understand in and appreciation of diversity and need for
respect in professional practice in or to deliver quality and person centered health care. The
following essay is a critical reflection on how own culture, life experiences, worldview and
dominant cultural paradigm that do influence perceptions of and interactions with indigenous
people in health care. This will involve defining and discussing protection and segregation
policies of 1850 to 1950 and a critically reflection how the policy relates to health care and my
professional practice.
Introduction
Understanding first people health care is an important part in delivering a person centered health
care in professional practice. The Australian history from colonization and policy has had
adverse health effect to the indigenous Australians. Indigenous people/ first people in Australia
refer to Aboriginals and Torres Islander Slate who occupied Australia before colonization
(Kirmayer, 2012). The indigenous people had their culture, way of knowing and doing things
and a history for their community. Colonization and subsequent government policies undermined
indigenous people way of life whose effects are also felt in today’s indigenous communities. The
unit on first people health and practice has exposed me so several policies that affected the
indigenous communities that give me understand in and appreciation of diversity and need for
respect in professional practice in or to deliver quality and person centered health care. The
following essay is a critical reflection on how own culture, life experiences, worldview and
dominant cultural paradigm that do influence perceptions of and interactions with indigenous
people in health care. This will involve defining and discussing protection and segregation
policies of 1850 to 1950 and a critically reflection how the policy relates to health care and my
professional practice.
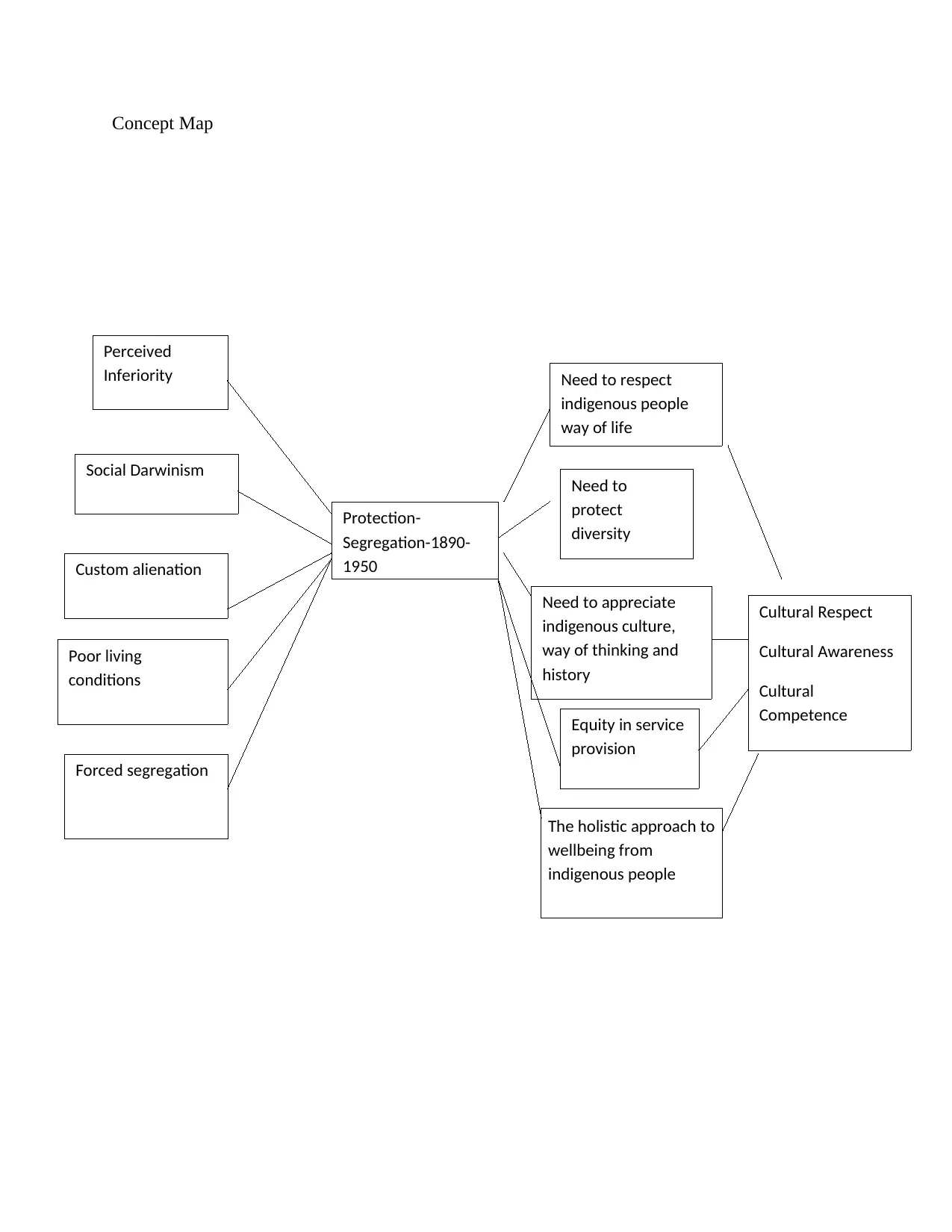
Concept Map
Perceived
Inferiority
Social Darwinism
Custom alienation
Poor living
conditions
Protection-
Segregation-1890-
1950
Need to respect
indigenous people
way of life
Need to
protect
diversity
Need to appreciate
indigenous culture,
way of thinking and
history
Equity in service
provision
Cultural Respect
Cultural Awareness
Cultural
Competence
Forced segregation
The holistic approach to
wellbeing from
indigenous people
Perceived
Inferiority
Social Darwinism
Custom alienation
Poor living
conditions
Protection-
Segregation-1890-
1950
Need to respect
indigenous people
way of life
Need to
protect
diversity
Need to appreciate
indigenous culture,
way of thinking and
history
Equity in service
provision
Cultural Respect
Cultural Awareness
Cultural
Competence
Forced segregation
The holistic approach to
wellbeing from
indigenous people
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Protection through segregation was a policy era in 1890s to 1950s. The protection and
segregation policy era aimed to move indigenous people onto reserves and control their relation
with other Australians. This policy era was after colonization and White Australia policy eras
that did not consider indigenous people needs as part of the Australian citizens. The protection
through segregation policy era was characterized by several themes that had profound effect to
first people of Australia. One of the issues is that they were perceived inferiority of the first
people of Australia. The indigenous people were viewed as inferior to other Australian. For
example, the New South Wales had established Protection Boards that controlled the Aboriginal
populations. This theme entails that the indigenous Australians has no freedom of self
determination and their practices where viewed as threat to the Australian society. The second
theme in the protection through segregation was social Darwism where the indigenous people
were expected to die out (Scott et al., 2012). It was estimated that the indigenous population had
fallen to 60000 in 1920s from more than 300000 in 1788 (Long, 2012). For example, in 1909 the
Boards had power that allowed them to remove Aboriginal people from urban areas and put them
in control reserves. This theme show the perception that the policy makers had that the
aboriginals would die out and were not envisioned to be part of the Australian society. The third
theme in the protection by segregation policy era is custom alienation. Different cultural groups
of indigenous people were forced to stay together. Indigenous people had different cultures and
being forced to live together caused disharmony. The indigenous communities were also
relocated from their ancestral land. This alienated their culture that enhanced their well being.
For example, the Aboriginals had spiritual connection to land while Torres Islander has spiritual
connectivity to the sea. Alienating the indigenous customs had a profound wellbeing of
indigenous people. The fourth theme evident in the protection through segregation era is
separation of children from their parent. Separation of children had social and health negative
effects to both parents and children. Parents of indigenous children were separated from their
children that were a painful and stressful event that changed indigenous people perception to
other Australia. The indigenous people became less trusting of white Australians. For instance,
boys were forcefully removed and taken to Kinchela Boys home while girls were taken to
Coontamundra girl. The other theme in this policy era was poor living conditions. The
indigenous people were provided with poor conditions that included meager rations of products
such as sugar, flour, tea and other substance (Muller, 2014). This affected the indigenous people
segregation policy era aimed to move indigenous people onto reserves and control their relation
with other Australians. This policy era was after colonization and White Australia policy eras
that did not consider indigenous people needs as part of the Australian citizens. The protection
through segregation policy era was characterized by several themes that had profound effect to
first people of Australia. One of the issues is that they were perceived inferiority of the first
people of Australia. The indigenous people were viewed as inferior to other Australian. For
example, the New South Wales had established Protection Boards that controlled the Aboriginal
populations. This theme entails that the indigenous Australians has no freedom of self
determination and their practices where viewed as threat to the Australian society. The second
theme in the protection through segregation was social Darwism where the indigenous people
were expected to die out (Scott et al., 2012). It was estimated that the indigenous population had
fallen to 60000 in 1920s from more than 300000 in 1788 (Long, 2012). For example, in 1909 the
Boards had power that allowed them to remove Aboriginal people from urban areas and put them
in control reserves. This theme show the perception that the policy makers had that the
aboriginals would die out and were not envisioned to be part of the Australian society. The third
theme in the protection by segregation policy era is custom alienation. Different cultural groups
of indigenous people were forced to stay together. Indigenous people had different cultures and
being forced to live together caused disharmony. The indigenous communities were also
relocated from their ancestral land. This alienated their culture that enhanced their well being.
For example, the Aboriginals had spiritual connection to land while Torres Islander has spiritual
connectivity to the sea. Alienating the indigenous customs had a profound wellbeing of
indigenous people. The fourth theme evident in the protection through segregation era is
separation of children from their parent. Separation of children had social and health negative
effects to both parents and children. Parents of indigenous children were separated from their
children that were a painful and stressful event that changed indigenous people perception to
other Australia. The indigenous people became less trusting of white Australians. For instance,
boys were forcefully removed and taken to Kinchela Boys home while girls were taken to
Coontamundra girl. The other theme in this policy era was poor living conditions. The
indigenous people were provided with poor conditions that included meager rations of products
such as sugar, flour, tea and other substance (Muller, 2014). This affected the indigenous people
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

accessibility of adequate food and living conditions that adversely affected their health.
Therefore, the protection through segregation policy era had adverse social and health effects to
the indigenous people of Australia.
The protection through segregation topic was an outstanding case of traumatizing events in
relation to my life experiences, my culture, and professional practice. Before this course, I had
limited understanding of this policy era that I feel had profound health impact that can be
observed even today in indigenous communities. Fro0m my culture and professional value, I
think and feel several issues were not right in the protection through segregation policy era. First,
the issue of forceful separation of parent and their children is a stressful event. From a
worldview, parent to kid separation is a painful and stressful event to both the parent and the kid.
Forceful separation destroys special connectivity that indigenous people had to family and
kinship that made up their society (Muller, 2014). Secondly, the protection through segregation
undermined the indigenous people human rights. From my life experience, human rights are
basic for human survival and dignity. Undermining human rights is oppression that causes
mental illness. The indigenous people were denied right to self determinations. Their lives were
controlled by Board who determined what they do and how they do it. As a human being, I can
relate to an instance where my right for self determination and privacy are undermined. This
means living under oppression when one cannot work towards personal goals and attain
fulfillment out of their achievement. From professional practice, self determination is an
important part to delivering holistic health care. Denying self determination therefore means that
holistic approach to health care delivery cannot be attained. Thirdly, the issues of equity are
critical in the society today. The notion that indigenous people were inferior compared other
Australians encouraged stigmatization, racism and social disadvantage in the society (Durey &
Thompson, 2012). From my life experience, people feel bad when they are neglected or looked
down as inferior. I believe there is no race that is superior to the other and the difference in
societies is not a weakness by diversity to be respected (Maddison, 2013). In the professional
practice, equity provision of health care is paramount to meeting high quality health care. Lastly,
provision of poor living condition exposed indigenous people to risk of contracting infections.
Living in poor conditions make an individual more susceptible to infections compare to an
individual living on good conditions. In professional practice, an individual social, economic,
environment factors contribute to their health. Poor living conditions make an individual
Therefore, the protection through segregation policy era had adverse social and health effects to
the indigenous people of Australia.
The protection through segregation topic was an outstanding case of traumatizing events in
relation to my life experiences, my culture, and professional practice. Before this course, I had
limited understanding of this policy era that I feel had profound health impact that can be
observed even today in indigenous communities. Fro0m my culture and professional value, I
think and feel several issues were not right in the protection through segregation policy era. First,
the issue of forceful separation of parent and their children is a stressful event. From a
worldview, parent to kid separation is a painful and stressful event to both the parent and the kid.
Forceful separation destroys special connectivity that indigenous people had to family and
kinship that made up their society (Muller, 2014). Secondly, the protection through segregation
undermined the indigenous people human rights. From my life experience, human rights are
basic for human survival and dignity. Undermining human rights is oppression that causes
mental illness. The indigenous people were denied right to self determinations. Their lives were
controlled by Board who determined what they do and how they do it. As a human being, I can
relate to an instance where my right for self determination and privacy are undermined. This
means living under oppression when one cannot work towards personal goals and attain
fulfillment out of their achievement. From professional practice, self determination is an
important part to delivering holistic health care. Denying self determination therefore means that
holistic approach to health care delivery cannot be attained. Thirdly, the issues of equity are
critical in the society today. The notion that indigenous people were inferior compared other
Australians encouraged stigmatization, racism and social disadvantage in the society (Durey &
Thompson, 2012). From my life experience, people feel bad when they are neglected or looked
down as inferior. I believe there is no race that is superior to the other and the difference in
societies is not a weakness by diversity to be respected (Maddison, 2013). In the professional
practice, equity provision of health care is paramount to meeting high quality health care. Lastly,
provision of poor living condition exposed indigenous people to risk of contracting infections.
Living in poor conditions make an individual more susceptible to infections compare to an
individual living on good conditions. In professional practice, an individual social, economic,
environment factors contribute to their health. Poor living conditions make an individual
susceptible to infections hence contracting diseases (Muller, 2014). Following this understanding
of protection through segregation, I have acknowledged the impact of history to indigenous
people health. First, I understand some of the problems that exist among indigenous people are
as a result of trauma and loss experiences in the past that affect their health up to date (Whyte,
2016). Secondly, I have understood and appreciated the role of family and kinship among
Aboriginals and recognition of diversity that should be protected. Lastly, I have appreciated and
accepted the concept of holistic health care among indigenous communities. Therefore, the study
on protection through segregation was unfavorable experience and could have caused health
implication to any population.
Dominant cultural paradigm has influence and shape perceptions. The dominant culture
assumption and view point on protection through segmentation issues are driven by the objective
of providing quality health care and respect to human dignity (Artuso, Cargo, Brown & Daniel,
2013). The first viewpoint of dominant culture is respect for culture and diversity. This refers to
appreciation and acceptable of difference in cultures and need to preserve diversity. Cultures are
not looked down but they are used to providing person centered health care. This viewpoint
enhances by perception to appreciate culture and diversity and it role in providing health care.
The second dominant viewpoint is respect to human life. Human life is viewed as sacred and
should be sustained. No human being should take away another person’s life. This view
enhances the dignity of human life. This view point enhances my interaction with first and
objective to treating their life with utmost dignity when providing health care. The third
dominant view point is equity in provision of services. Equality is an important part to the
dominant cultures and all human beings are supposed to be treated the same (Runciman et al.,
2012). This enhances my interaction with indigenous people when providing health services. The
fourth dominant culture viewpoint is self determinant of a person. People have a say on their
health and professional practitioners should incorporate patients wish in the administration of
health care (Aspin et al., 20112). This viewpoint influences my perception toward incorporating
patient views when administering health care to indigenous people. The last predominant culture
relating to issues of protection through segregation policy era is holistic health care approach. A
holistic approach goes behold physical and mental treatment and includes cultures and spiritual
wellness. This viewpoint influences my perception and future interaction with indigenous people
with an objective of providing a holistic health care that lead to holistic wellbeing.
of protection through segregation, I have acknowledged the impact of history to indigenous
people health. First, I understand some of the problems that exist among indigenous people are
as a result of trauma and loss experiences in the past that affect their health up to date (Whyte,
2016). Secondly, I have understood and appreciated the role of family and kinship among
Aboriginals and recognition of diversity that should be protected. Lastly, I have appreciated and
accepted the concept of holistic health care among indigenous communities. Therefore, the study
on protection through segregation was unfavorable experience and could have caused health
implication to any population.
Dominant cultural paradigm has influence and shape perceptions. The dominant culture
assumption and view point on protection through segmentation issues are driven by the objective
of providing quality health care and respect to human dignity (Artuso, Cargo, Brown & Daniel,
2013). The first viewpoint of dominant culture is respect for culture and diversity. This refers to
appreciation and acceptable of difference in cultures and need to preserve diversity. Cultures are
not looked down but they are used to providing person centered health care. This viewpoint
enhances by perception to appreciate culture and diversity and it role in providing health care.
The second dominant viewpoint is respect to human life. Human life is viewed as sacred and
should be sustained. No human being should take away another person’s life. This view
enhances the dignity of human life. This view point enhances my interaction with first and
objective to treating their life with utmost dignity when providing health care. The third
dominant view point is equity in provision of services. Equality is an important part to the
dominant cultures and all human beings are supposed to be treated the same (Runciman et al.,
2012). This enhances my interaction with indigenous people when providing health services. The
fourth dominant culture viewpoint is self determinant of a person. People have a say on their
health and professional practitioners should incorporate patients wish in the administration of
health care (Aspin et al., 20112). This viewpoint influences my perception toward incorporating
patient views when administering health care to indigenous people. The last predominant culture
relating to issues of protection through segregation policy era is holistic health care approach. A
holistic approach goes behold physical and mental treatment and includes cultures and spiritual
wellness. This viewpoint influences my perception and future interaction with indigenous people
with an objective of providing a holistic health care that lead to holistic wellbeing.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
The reflection process has enabled me to learn by focusing what I knew, what happened, and
what other people say about the issues as a result of protection through segregation. This enabled
me to get a deeper understanding of the underlying issues in indigenous people health. First, I
have learnt that human rights of indigenous people need to be recognized to enhance human
dignity among the community in order to deliver health care. Secondly, I have learnt the central
role of self determination in providing health services to indigenous people. In my practice, I will
allow patients to comment on their treatment so that I can incorporate their views in the
treatment. Thirdly, I have learnt that the trauma caused in the past continue to contribute to
impairment in the indigenous health and culture. The forceful separation of children from their
parents and land was a traumatic event that affected the mental wellness of the indigenous
people. Family and kinship is an important part of the indigenous people and part of wellbeing
(Jeffreys, 2015). In my professional practice, I will involve indigenous people’s family. I have
also learned that racism, adversity, stigma, and social disadvantage led to health problem
experienced by the population. To address this issue in my professional practice, I will advocate
for equality to indigenous people in Australia. Lastly, I have learnt about the holistic approach to
health care. This approach incorporates more aspect of wellness beyond physical health and
mental wellness. I will adopt holistic approach of health care.
From the critical reflection process, I have gained significant knowledge and skills that will
transform my practice in health care. First I have gained knowledge on cultural awareness. I have
been able to assess my knowledge on indigenous people, their customs, and history. I am now
aware and I can take responsibility of my stereotype, assumptions, values and biases in relation
to indigenous health. Secondly, I have attained cultural respect for indigenous people. I can
recognize, protect, and advance inherent rights, traditions and cultures of indigenous people. This
will enable in achieving equitable health outcome. Lastly, I have acquired cultural competence
skills that I will continuous advance effective intercultural interactions with indigenous people. I
have aligned my knowledge, attitude, and skills to work effectively with indigenous people and
meet high quality health care.
From the essay, protection through segregation had profound effects to indigenous people health.
It led to traumatic experiences as result of forceful separation, provision of poor living condition,
culture disharmony, alienation of the indigenous people culture, and perceived inferiority. These
what other people say about the issues as a result of protection through segregation. This enabled
me to get a deeper understanding of the underlying issues in indigenous people health. First, I
have learnt that human rights of indigenous people need to be recognized to enhance human
dignity among the community in order to deliver health care. Secondly, I have learnt the central
role of self determination in providing health services to indigenous people. In my practice, I will
allow patients to comment on their treatment so that I can incorporate their views in the
treatment. Thirdly, I have learnt that the trauma caused in the past continue to contribute to
impairment in the indigenous health and culture. The forceful separation of children from their
parents and land was a traumatic event that affected the mental wellness of the indigenous
people. Family and kinship is an important part of the indigenous people and part of wellbeing
(Jeffreys, 2015). In my professional practice, I will involve indigenous people’s family. I have
also learned that racism, adversity, stigma, and social disadvantage led to health problem
experienced by the population. To address this issue in my professional practice, I will advocate
for equality to indigenous people in Australia. Lastly, I have learnt about the holistic approach to
health care. This approach incorporates more aspect of wellness beyond physical health and
mental wellness. I will adopt holistic approach of health care.
From the critical reflection process, I have gained significant knowledge and skills that will
transform my practice in health care. First I have gained knowledge on cultural awareness. I have
been able to assess my knowledge on indigenous people, their customs, and history. I am now
aware and I can take responsibility of my stereotype, assumptions, values and biases in relation
to indigenous health. Secondly, I have attained cultural respect for indigenous people. I can
recognize, protect, and advance inherent rights, traditions and cultures of indigenous people. This
will enable in achieving equitable health outcome. Lastly, I have acquired cultural competence
skills that I will continuous advance effective intercultural interactions with indigenous people. I
have aligned my knowledge, attitude, and skills to work effectively with indigenous people and
meet high quality health care.
From the essay, protection through segregation had profound effects to indigenous people health.
It led to traumatic experiences as result of forceful separation, provision of poor living condition,
culture disharmony, alienation of the indigenous people culture, and perceived inferiority. These
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

issues are extreme cases that undermined indigenous Australian health care. According to my
experience, dominant culture, protection through segregation issues undermined human rights,
human dignity, discriminated and self determination. From the essay, I have learnt several
lessons that will improve my profession practice through cultural competency.
experience, dominant culture, protection through segregation issues undermined human rights,
human dignity, discriminated and self determination. From the essay, I have learnt several
lessons that will improve my profession practice through cultural competency.
References
Artuso, S., Cargo, M., Brown, A., & Daniel, M. (2013). Factors influencing health care
utilisation among Aboriginal cardiac patients in central Australia: a qualitative study.
BMC Health Services Research, 13(1), 83.
Aspin, C., Brown, N., Jowsey, T., Yen, L., & Leeder, S. (2012). Strategic approaches to
enhanced health service delivery for Aboriginal and Torres Strait Islander people with
chronic illness: a qualitative study. BMC health services research, 12(1), 143.
Durey, A., & Thompson, S. C. (2012). Reducing the health disparities of Indigenous Australians:
time to change focus. BMC health services research, 12(1), 151.
Jeffreys, M. R. (2015). Teaching cultural competence in nursing and health care: Inquiry,
action, and innovation. Springer Publishing Company.
Kirmayer, L. J. (2012). Rethinking cultural competence.
Long, T. B. (2012). Overview of teaching strategies for cultural competence in nursing students.
Journal of Cultural Diversity, 19(3), 102.
Maddison, S. (2013). Indigenous identity,‘authenticity’and the structural violence of settler
colonialism. Identities, 20(3), 288-303.
Muller, L. (2014). A theory for Indigenous Australian health and human service work. Allen &
Unwin.
Runciman, W. B., Hunt, T. D., Hannaford, N. A., Hibbert, P. D., Westbrook, J. I., Coiera, E.
W., ... & Braithwaite, J. (2012). CareTrack: assessing the appropriateness of health care
delivery in Australia. Medical Journal of Australia, 197(2), 100.
Scott, E. M., Hermens, D. F., Glozier, N., Naismith, S. L., Guastella, A. J., & Hickie, I. B.
(2012). Targeted primary care-based mental health services for young Australians. Med
J Aust, 196(2), 136-40.
Whyte, K. (2016). Indigenous food systems, environmental justice, and settler-industrial states.
Artuso, S., Cargo, M., Brown, A., & Daniel, M. (2013). Factors influencing health care
utilisation among Aboriginal cardiac patients in central Australia: a qualitative study.
BMC Health Services Research, 13(1), 83.
Aspin, C., Brown, N., Jowsey, T., Yen, L., & Leeder, S. (2012). Strategic approaches to
enhanced health service delivery for Aboriginal and Torres Strait Islander people with
chronic illness: a qualitative study. BMC health services research, 12(1), 143.
Durey, A., & Thompson, S. C. (2012). Reducing the health disparities of Indigenous Australians:
time to change focus. BMC health services research, 12(1), 151.
Jeffreys, M. R. (2015). Teaching cultural competence in nursing and health care: Inquiry,
action, and innovation. Springer Publishing Company.
Kirmayer, L. J. (2012). Rethinking cultural competence.
Long, T. B. (2012). Overview of teaching strategies for cultural competence in nursing students.
Journal of Cultural Diversity, 19(3), 102.
Maddison, S. (2013). Indigenous identity,‘authenticity’and the structural violence of settler
colonialism. Identities, 20(3), 288-303.
Muller, L. (2014). A theory for Indigenous Australian health and human service work. Allen &
Unwin.
Runciman, W. B., Hunt, T. D., Hannaford, N. A., Hibbert, P. D., Westbrook, J. I., Coiera, E.
W., ... & Braithwaite, J. (2012). CareTrack: assessing the appropriateness of health care
delivery in Australia. Medical Journal of Australia, 197(2), 100.
Scott, E. M., Hermens, D. F., Glozier, N., Naismith, S. L., Guastella, A. J., & Hickie, I. B.
(2012). Targeted primary care-based mental health services for young Australians. Med
J Aust, 196(2), 136-40.
Whyte, K. (2016). Indigenous food systems, environmental justice, and settler-industrial states.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.