Diagnostic Accuracy: CT Angiography vs Digital Subtraction Angiography
VerifiedAdded on 2022/11/25
|24
|7295
|75
Project
AI Summary
This research proposal investigates the diagnostic accuracy of Computed Tomography Angiography (CTA) compared to Digital Subtraction Angiography (DSA) in detecting cerebral aneurysms. The study aims to determine if CTA offers comparable or superior accuracy to DSA, the current gold standard, in neuro-interventional procedures. It employs a retrospective cohort study methodology, analyzing data from patients with intracranial aneurysms. The proposal outlines the introduction to the problem of cerebral aneurysms, the hypothesis, methodology, and a review of existing literature. The research will evaluate the sensitivity, specificity, and error rates of both CTA and DSA, considering factors like aneurysm size and location. The anticipated outcome is to demonstrate CTA's effectiveness, potentially establishing it as a more accessible and less invasive alternative to DSA. Ethical considerations and study design details are also included in the proposal.

CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
Research Proposal
On
CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
Name
Name of the University
Author’s Note
Research Proposal
On
CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
Name
Name of the University
Author’s Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
Table of Contents
Introduction................................................................................................................................2
Proposed hypothesis...................................................................................................................3
Methodology..............................................................................................................................3
Bibliographic review of literature..............................................................................................4
Analysis......................................................................................................................................8
Conclusion..................................................................................................................................9
Bibliography.............................................................................................................................10
Table of Contents
Introduction................................................................................................................................2
Proposed hypothesis...................................................................................................................3
Methodology..............................................................................................................................3
Bibliographic review of literature..............................................................................................4
Analysis......................................................................................................................................8
Conclusion..................................................................................................................................9
Bibliography.............................................................................................................................10
2CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
Introduction
The presence of a weak, bulging spot on the arteries circulating blood in the brain is
termed as Intracranial Cerebral Aneurysm (ICA). As the artery wall is fragile and thin, an
aneurysm can easily rupture causing ruptured aneurysm (RA) which leads to bleeding on the
brain’s surface. Example of such bleeding on the subarachnoid surface leads to serious, life-
threatening stroke called subarachnoid haemorrhage (SAH). Sophistication of interventional
tools like Computed Tomography angiography (CTA), Magnetic Resonance angiography
(MRA), Magnetic Resonance Imaging (MRI), and Digital Subtraction Angiography (DSA)
are empowering the analysis of brain lesions and anomalies, thereby increasing the number of
patients diagnosed with unruptured aneurysms (URA).
The unruptured aneurysms (URA) or acquired lesions affects 5-10% of general
population of which, URA affects 2.3% of general population with high prevalence (3.6%-
6.5%) observed among working age group (30-50 years) (Ambekar & Pandey, 2015).
Women are more likely to develop ICA when compared to men with occurrence ratio of 3:1.
Though majority (70%-75%) ICA occurs as single aneurysm, 25%-30% occurs as multiple
lesions. URA are rarely observed in children (0.5-4.6%) and develops with ageing. In the
USA, an estimated six million people are affected by URA and 30,000 suffer RA each year
however, occurrence of ICA is twice more common among African-Americans when
compared to Caucasians (Brain Aneurysm Foundation, 2019). Followed by African-
Americans, the incidence of RA is higher among Finnish and Japanese ancestry (Greving et
al., 2014). According to Ambekar (2015), In India, about 76,500 to 204,100 new incidences
of SAH occurs every year. In addition to smoking, alcohol consumption and high blood
pressure, familiar occurrence and heritable conditions such as autosomal dominant polycystic
kidney disease, Ehlers-Danlos syndrome type II and IV, hereditary hemorrhagic
Introduction
The presence of a weak, bulging spot on the arteries circulating blood in the brain is
termed as Intracranial Cerebral Aneurysm (ICA). As the artery wall is fragile and thin, an
aneurysm can easily rupture causing ruptured aneurysm (RA) which leads to bleeding on the
brain’s surface. Example of such bleeding on the subarachnoid surface leads to serious, life-
threatening stroke called subarachnoid haemorrhage (SAH). Sophistication of interventional
tools like Computed Tomography angiography (CTA), Magnetic Resonance angiography
(MRA), Magnetic Resonance Imaging (MRI), and Digital Subtraction Angiography (DSA)
are empowering the analysis of brain lesions and anomalies, thereby increasing the number of
patients diagnosed with unruptured aneurysms (URA).
The unruptured aneurysms (URA) or acquired lesions affects 5-10% of general
population of which, URA affects 2.3% of general population with high prevalence (3.6%-
6.5%) observed among working age group (30-50 years) (Ambekar & Pandey, 2015).
Women are more likely to develop ICA when compared to men with occurrence ratio of 3:1.
Though majority (70%-75%) ICA occurs as single aneurysm, 25%-30% occurs as multiple
lesions. URA are rarely observed in children (0.5-4.6%) and develops with ageing. In the
USA, an estimated six million people are affected by URA and 30,000 suffer RA each year
however, occurrence of ICA is twice more common among African-Americans when
compared to Caucasians (Brain Aneurysm Foundation, 2019). Followed by African-
Americans, the incidence of RA is higher among Finnish and Japanese ancestry (Greving et
al., 2014). According to Ambekar (2015), In India, about 76,500 to 204,100 new incidences
of SAH occurs every year. In addition to smoking, alcohol consumption and high blood
pressure, familiar occurrence and heritable conditions such as autosomal dominant polycystic
kidney disease, Ehlers-Danlos syndrome type II and IV, hereditary hemorrhagic
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
telangiectasia, Marfan syndrome, multiple endocrine neoplasia type I, neurofibromatosis type
I and pseudoxanthoma elasticum, are associated with ICA formation.
The computed tomography angiography (CTA) is a non-invasive, reliable and
convenient technique to detect and manage the intracranial aneurysms. In multiple previous
studies, it was reported that, the use of CTA in managing the aneurysms in intracranial or
cerebral region is very common. In another study by Backes et al. (2014), it is reported that,
the CTA is generally performed by using the multi detector helical 3D scanners that allow
taking images of the blood vessels in a more prominent manner by forming more sub
millimeter slices of the desired blood vessels during the tests.
The use of digital subtraction angiography (DSA), an invasive interventional
technique, is also common in detection of intracranial aneurysms. The main reason behind
the use of this system is the high spatial resolution of this technique. According to the study
of Wang et al. (2013), it is reported that the DSA is an invasive technique which requires
premium quality skill to achieve desired performance and is more complex as well thereby
heightening the probability of inaccuracy. However, DSA is referred to as the gold standard
due to the hemodynamic information such as collateral flow and flow direction which is
gained from DSA and cannot be detected using CTA.
The use of different neuro interventional imagery modalities is extremely valuable
along with their regular technological advancement and constant up gradation. The various
modalities used as non invasive imagers such as MRA shows high sensitivity whereas its
specificity is variable between 80 to 95 %. Majority of the false positive aneurysms detected
are less than 3 mm in size. It is important to correctly diagnose, the type, number of ruptures
to treat accordingly. Current neuro imaging techniques for diagnosing ICA include, non-
contrast enhanced computed tomography (NCE-CT), contrast enhanced- computed
telangiectasia, Marfan syndrome, multiple endocrine neoplasia type I, neurofibromatosis type
I and pseudoxanthoma elasticum, are associated with ICA formation.
The computed tomography angiography (CTA) is a non-invasive, reliable and
convenient technique to detect and manage the intracranial aneurysms. In multiple previous
studies, it was reported that, the use of CTA in managing the aneurysms in intracranial or
cerebral region is very common. In another study by Backes et al. (2014), it is reported that,
the CTA is generally performed by using the multi detector helical 3D scanners that allow
taking images of the blood vessels in a more prominent manner by forming more sub
millimeter slices of the desired blood vessels during the tests.
The use of digital subtraction angiography (DSA), an invasive interventional
technique, is also common in detection of intracranial aneurysms. The main reason behind
the use of this system is the high spatial resolution of this technique. According to the study
of Wang et al. (2013), it is reported that the DSA is an invasive technique which requires
premium quality skill to achieve desired performance and is more complex as well thereby
heightening the probability of inaccuracy. However, DSA is referred to as the gold standard
due to the hemodynamic information such as collateral flow and flow direction which is
gained from DSA and cannot be detected using CTA.
The use of different neuro interventional imagery modalities is extremely valuable
along with their regular technological advancement and constant up gradation. The various
modalities used as non invasive imagers such as MRA shows high sensitivity whereas its
specificity is variable between 80 to 95 %. Majority of the false positive aneurysms detected
are less than 3 mm in size. It is important to correctly diagnose, the type, number of ruptures
to treat accordingly. Current neuro imaging techniques for diagnosing ICA include, non-
contrast enhanced computed tomography (NCE-CT), contrast enhanced- computed
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
tomographic angiography (CE-CTA), magnetic resonance imaging and angiography (MRI
and MRA) and intra-arterial digital subtraction angiography (DSA). These techniques helps
to understand CIA in terms of aneurysm size, location, rupture status, number of aneurysms
and other imaging characteristics. When an aberration is detected, during the imaging
investigation, a team of neurosurgeons and neuro-interventional radiologists work together in
providing an optimal treatment for the particular situation at hand. The sensitivity of
Computed Tomography angiography (CTA) is known to be quite high however its specificity
is in question whereas the gold standard of reference for intracranial and neural imagery
Digital Subtraction Angiography (DSA) has a huge drawback for being an invasive technique
and requiring highly skilled professional for processing.
Proposed hypothesis
The Null Hypothesis H0: The diagnostic accuracy of the CTA is same as DSA in
detecting cerebral aneurysm.
The Proposed Alternative Hypothesis H1: The diagnostic accuracy of the CTA is
better than DSA in detecting cerebral aneurysm.
Methodology
This systematic study encompasses use of retrospective cohort study method for
obtaining the accuracy of the CT angiography and DSA for detecting the cerebral aneurysms
or cranial aneurysm. A retrospective cohort study is a specific type of observational study, in
which the researcher identifies a specific time frame and then collects the relevant data from
that specific time frame. In such cases, the researchers also can use the self-reported data of
the subject population during the study. According to the study of Setia (2016), it is reported
that, the cohort study type is a specific type of non-experimental study or rather an
tomographic angiography (CE-CTA), magnetic resonance imaging and angiography (MRI
and MRA) and intra-arterial digital subtraction angiography (DSA). These techniques helps
to understand CIA in terms of aneurysm size, location, rupture status, number of aneurysms
and other imaging characteristics. When an aberration is detected, during the imaging
investigation, a team of neurosurgeons and neuro-interventional radiologists work together in
providing an optimal treatment for the particular situation at hand. The sensitivity of
Computed Tomography angiography (CTA) is known to be quite high however its specificity
is in question whereas the gold standard of reference for intracranial and neural imagery
Digital Subtraction Angiography (DSA) has a huge drawback for being an invasive technique
and requiring highly skilled professional for processing.
Proposed hypothesis
The Null Hypothesis H0: The diagnostic accuracy of the CTA is same as DSA in
detecting cerebral aneurysm.
The Proposed Alternative Hypothesis H1: The diagnostic accuracy of the CTA is
better than DSA in detecting cerebral aneurysm.
Methodology
This systematic study encompasses use of retrospective cohort study method for
obtaining the accuracy of the CT angiography and DSA for detecting the cerebral aneurysms
or cranial aneurysm. A retrospective cohort study is a specific type of observational study, in
which the researcher identifies a specific time frame and then collects the relevant data from
that specific time frame. In such cases, the researchers also can use the self-reported data of
the subject population during the study. According to the study of Setia (2016), it is reported
that, the cohort study type is a specific type of non-experimental study or rather an
5CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
observational study as well. The study also identified that in a cohort study, the participants
or the subject population does not have the outcome of interest during the beginning of the
study. It is evident that, as per the levels of the exposure, the study population will be
selected. After the selection of the cohort population, the subject population will be followed
for a particular period of time (Plank et al., 2014).
In a cohort study, the participants of the study do not have the consequence of interest
to start with. The subject population of a particular cohort study will be based on a particular
limit of exposure of a specific thing. Thereby, it can be said that, in the overall selected
population of the study, a few people will be exposed to the specific criteria and a few will
not be at all exposed to the specific criteria as well during the initiation of the study. In most
of the cohort study cases, it is reported that, the selected subject population in the particular
cohort study, will be followed over time in order to evaluate the occurrence of the outcome of
the interest at the end of study. The study population who are exposed to the specific
stimulants is referred to as the exposed group of the study and on the other hand the
population who are not exposed to the specific stimulants are referred to as non-exposed
orcontrol group. Over the period of time (follow up time), the exposed individuals will
develop the specific outcome and other unexposed group of people will develop the outcome
of interest. The researcher of the study will analyze the outcome of the both groups (Brown
Jr, & Broderick, 2014)
In a prospective cohort study, the data of the study will be collected as a prospective
manner. The researcher of the study will define the population group that will be included in
the actual study. After this process the researcher will identify the potential exposure of the
interest and the participants are then classified into exposed and unexposed group of the
study. As a part of this process the researcher will follow the participants for a specific period
of time. At the end of the study and at the baseline level, the researchers collect information
observational study as well. The study also identified that in a cohort study, the participants
or the subject population does not have the outcome of interest during the beginning of the
study. It is evident that, as per the levels of the exposure, the study population will be
selected. After the selection of the cohort population, the subject population will be followed
for a particular period of time (Plank et al., 2014).
In a cohort study, the participants of the study do not have the consequence of interest
to start with. The subject population of a particular cohort study will be based on a particular
limit of exposure of a specific thing. Thereby, it can be said that, in the overall selected
population of the study, a few people will be exposed to the specific criteria and a few will
not be at all exposed to the specific criteria as well during the initiation of the study. In most
of the cohort study cases, it is reported that, the selected subject population in the particular
cohort study, will be followed over time in order to evaluate the occurrence of the outcome of
the interest at the end of study. The study population who are exposed to the specific
stimulants is referred to as the exposed group of the study and on the other hand the
population who are not exposed to the specific stimulants are referred to as non-exposed
orcontrol group. Over the period of time (follow up time), the exposed individuals will
develop the specific outcome and other unexposed group of people will develop the outcome
of interest. The researcher of the study will analyze the outcome of the both groups (Brown
Jr, & Broderick, 2014)
In a prospective cohort study, the data of the study will be collected as a prospective
manner. The researcher of the study will define the population group that will be included in
the actual study. After this process the researcher will identify the potential exposure of the
interest and the participants are then classified into exposed and unexposed group of the
study. As a part of this process the researcher will follow the participants for a specific period
of time. At the end of the study and at the baseline level, the researchers collect information
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
of the study participants along with the other factors related to the study result and these
factors are referred to as the confounding factors of the study (LeBlanc et al., 2015). On the
other hand in retrospective cohort, the data are collected from the records of past incidences.
Therefore it can be said that, the retrospective cohort study is mainly based on the past data
set. However, according to the study of Setia (2016), it is reported that although the outcome
of the retrospective study is based on the previous data set, the actual process is almost same
with the prospective study. So, in this method, the researcher will also take the baseline data
and the follow up data.
There are a few reasons of selecting this retrospective cohort study method for this
study. While analyzing the advantages of the cohort study, it can be said that, the cohort
study will help to study multiple outcome in the same exposure levels. However, if the
exposure is rare then cohort design is an effective method to examine the relation in between
the outcomes and the exposure levels. Moreover, in a retrospective cohort study, all the
process is completed within a small time period of time and it is mostly completed in low
expense as well. So, it is also evident that this study will also help the researchers in an
economic way. However, this retrospective cohort study has a few flaws or disadvantages as
well(LeBlanc et al., 2015). One of the major limitations of the retrospective cohort study is
that the outcome variables and the exposure are collected before the actual initiation of the
study. So, it may possible that the actual result may not accurate or not according to the
requirements of the study as well. Apart from that, as in the cohort study presence of multiple
subject population, it may possible that all the members of the cohort will not be exposed to
same level of the stimulant. Along with this, it is also quite possible that all the individuals
are not at all classified correctly. Therefore, the misclassification of the outcome or exposed
is not at all differential or may random in nature. Such condition may cause biasness in
between the two groups of the study as well and it will direct the study towards the null
of the study participants along with the other factors related to the study result and these
factors are referred to as the confounding factors of the study (LeBlanc et al., 2015). On the
other hand in retrospective cohort, the data are collected from the records of past incidences.
Therefore it can be said that, the retrospective cohort study is mainly based on the past data
set. However, according to the study of Setia (2016), it is reported that although the outcome
of the retrospective study is based on the previous data set, the actual process is almost same
with the prospective study. So, in this method, the researcher will also take the baseline data
and the follow up data.
There are a few reasons of selecting this retrospective cohort study method for this
study. While analyzing the advantages of the cohort study, it can be said that, the cohort
study will help to study multiple outcome in the same exposure levels. However, if the
exposure is rare then cohort design is an effective method to examine the relation in between
the outcomes and the exposure levels. Moreover, in a retrospective cohort study, all the
process is completed within a small time period of time and it is mostly completed in low
expense as well. So, it is also evident that this study will also help the researchers in an
economic way. However, this retrospective cohort study has a few flaws or disadvantages as
well(LeBlanc et al., 2015). One of the major limitations of the retrospective cohort study is
that the outcome variables and the exposure are collected before the actual initiation of the
study. So, it may possible that the actual result may not accurate or not according to the
requirements of the study as well. Apart from that, as in the cohort study presence of multiple
subject population, it may possible that all the members of the cohort will not be exposed to
same level of the stimulant. Along with this, it is also quite possible that all the individuals
are not at all classified correctly. Therefore, the misclassification of the outcome or exposed
is not at all differential or may random in nature. Such condition may cause biasness in
between the two groups of the study as well and it will direct the study towards the null
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
hypothesis. Therefore, it may possible that the association in between the outcome and the
exposure is understood by the researcher as well. Along with this, the researchers of the study
must ensure that, the follow up process of all the study participants must be same in case of
both groups (LeBlanc et al., 2015).
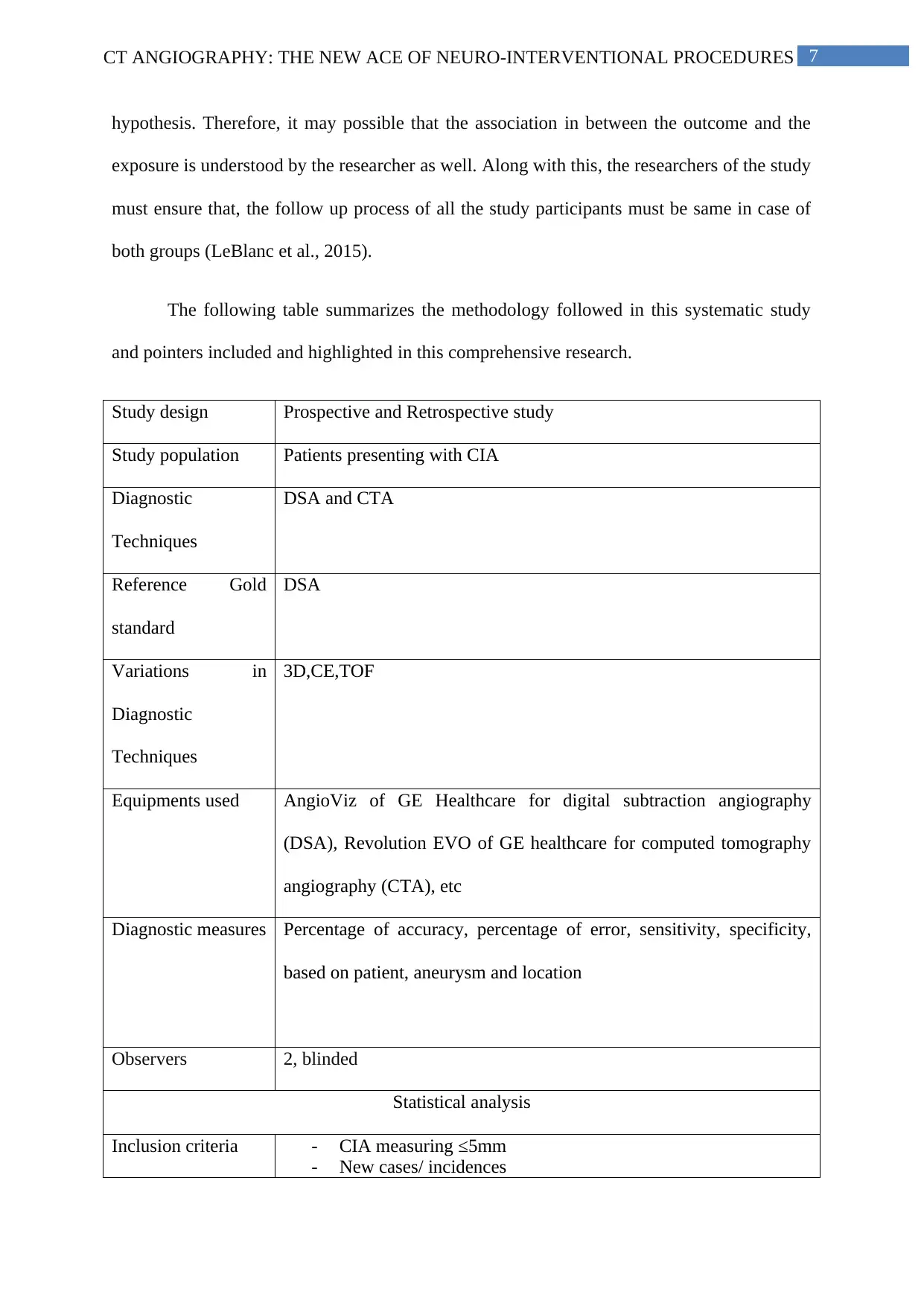
The following table summarizes the methodology followed in this systematic study
and pointers included and highlighted in this comprehensive research.
Study design Prospective and Retrospective study
Study population Patients presenting with CIA
Diagnostic
Techniques
DSA and CTA
Reference Gold
standard
DSA
Variations in
Diagnostic
Techniques
3D,CE,TOF
Equipments used AngioViz of GE Healthcare for digital subtraction angiography
(DSA), Revolution EVO of GE healthcare for computed tomography
angiography (CTA), etc
Diagnostic measures Percentage of accuracy, percentage of error, sensitivity, specificity,
based on patient, aneurysm and location
Observers 2, blinded
Statistical analysis
Inclusion criteria - CIA measuring ≤5mm
- New cases/ incidences
hypothesis. Therefore, it may possible that the association in between the outcome and the
exposure is understood by the researcher as well. Along with this, the researchers of the study
must ensure that, the follow up process of all the study participants must be same in case of
both groups (LeBlanc et al., 2015).
The following table summarizes the methodology followed in this systematic study
and pointers included and highlighted in this comprehensive research.
Study design Prospective and Retrospective study
Study population Patients presenting with CIA
Diagnostic
Techniques
DSA and CTA
Reference Gold
standard
DSA
Variations in
Diagnostic
Techniques
3D,CE,TOF
Equipments used AngioViz of GE Healthcare for digital subtraction angiography
(DSA), Revolution EVO of GE healthcare for computed tomography
angiography (CTA), etc
Diagnostic measures Percentage of accuracy, percentage of error, sensitivity, specificity,
based on patient, aneurysm and location
Observers 2, blinded
Statistical analysis
Inclusion criteria - CIA measuring ≤5mm
- New cases/ incidences
8CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
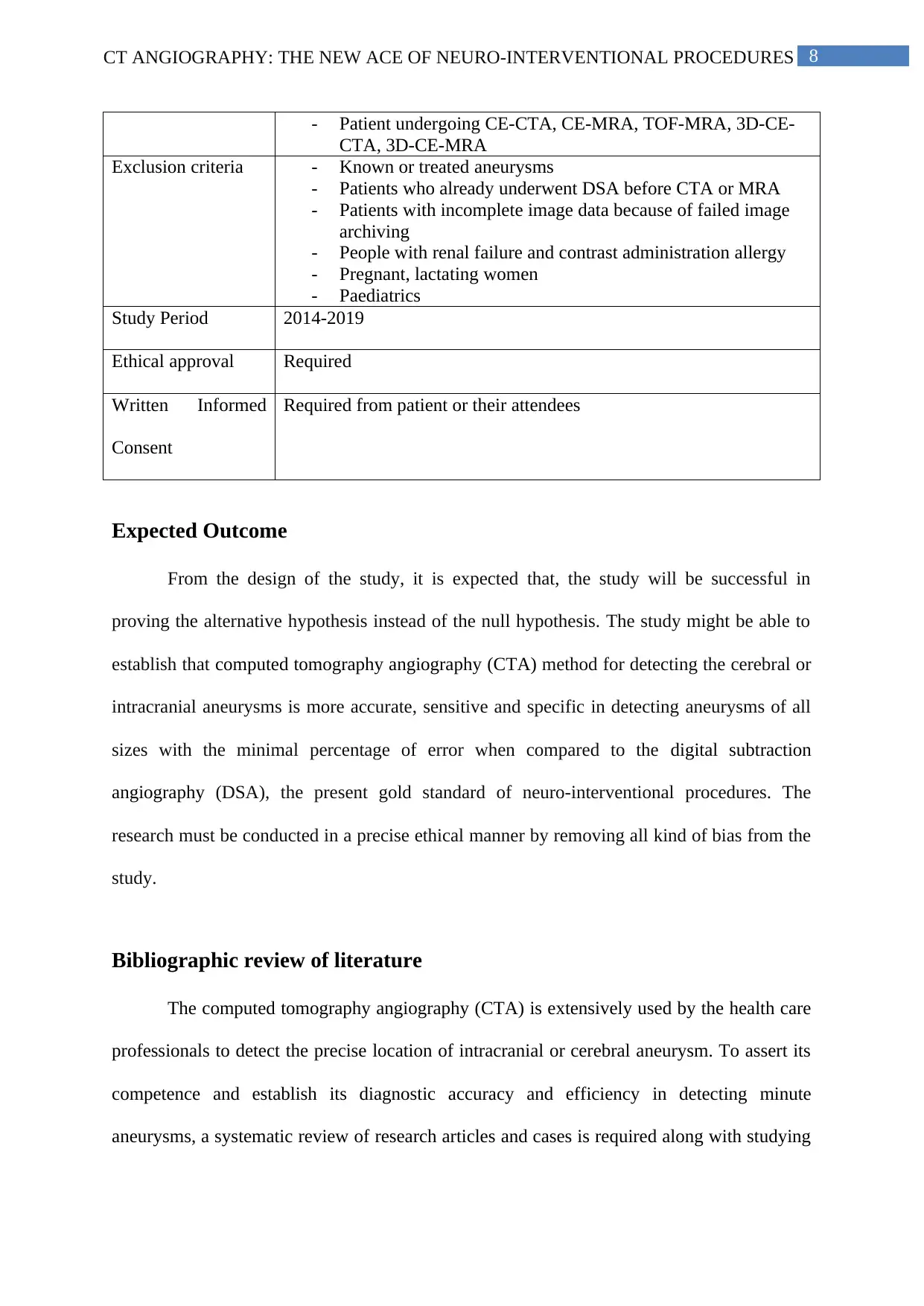
- Patient undergoing CE-CTA, CE-MRA, TOF-MRA, 3D-CE-
CTA, 3D-CE-MRA
Exclusion criteria - Known or treated aneurysms
- Patients who already underwent DSA before CTA or MRA
- Patients with incomplete image data because of failed image
archiving
- People with renal failure and contrast administration allergy
- Pregnant, lactating women
- Paediatrics
Study Period 2014-2019
Ethical approval Required
Written Informed
Consent
Required from patient or their attendees
Expected Outcome
From the design of the study, it is expected that, the study will be successful in
proving the alternative hypothesis instead of the null hypothesis. The study might be able to
establish that computed tomography angiography (CTA) method for detecting the cerebral or
intracranial aneurysms is more accurate, sensitive and specific in detecting aneurysms of all
sizes with the minimal percentage of error when compared to the digital subtraction
angiography (DSA), the present gold standard of neuro-interventional procedures. The
research must be conducted in a precise ethical manner by removing all kind of bias from the
study.
Bibliographic review of literature
The computed tomography angiography (CTA) is extensively used by the health care
professionals to detect the precise location of intracranial or cerebral aneurysm. To assert its
competence and establish its diagnostic accuracy and efficiency in detecting minute
aneurysms, a systematic review of research articles and cases is required along with studying
- Patient undergoing CE-CTA, CE-MRA, TOF-MRA, 3D-CE-
CTA, 3D-CE-MRA
Exclusion criteria - Known or treated aneurysms
- Patients who already underwent DSA before CTA or MRA
- Patients with incomplete image data because of failed image
archiving
- People with renal failure and contrast administration allergy
- Pregnant, lactating women
- Paediatrics
Study Period 2014-2019
Ethical approval Required
Written Informed
Consent
Required from patient or their attendees
Expected Outcome
From the design of the study, it is expected that, the study will be successful in
proving the alternative hypothesis instead of the null hypothesis. The study might be able to
establish that computed tomography angiography (CTA) method for detecting the cerebral or
intracranial aneurysms is more accurate, sensitive and specific in detecting aneurysms of all
sizes with the minimal percentage of error when compared to the digital subtraction
angiography (DSA), the present gold standard of neuro-interventional procedures. The
research must be conducted in a precise ethical manner by removing all kind of bias from the
study.
Bibliographic review of literature
The computed tomography angiography (CTA) is extensively used by the health care
professionals to detect the precise location of intracranial or cerebral aneurysm. To assert its
competence and establish its diagnostic accuracy and efficiency in detecting minute
aneurysms, a systematic review of research articles and cases is required along with studying
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
its precision in contrast with digital subtraction angiography (DSA) and other techniques in
use.
Yang et al. (2017) studied the accuracy of the computed tomographic angiography
(CTA) for critical diagnosis of <5 mm cerebral aneurysms in comparison to digital
subtraction angiography (DSA) used as the standard for reference with a patient sample size
of 1366, who initially underwent cerebral computed tomographic angiography followed by
digital subtraction angiography. Initially 1486 participants were chosen which finally made
the sample size of 1366 participants as the rest did not meet the inclusion criteria and were
patients who had undergone DSA prior to CTA or had more than one month between CTA
and DSA. So to avoid discrepancies, those with incomplete image data or with known or
treated aneurysms, only 1366 participants were taken for the study. Out of 1366 patients,
1187 of them were patients with intracranial hemorrhage, 908 patients had presented with de
novo aneurysms whereas 458 of the patients had presented without de novo aneurysms. Of
the 908 patients with de novo aneurysms, 329 patients had large de novo aneurysms and rest
had small to miniscule aneurysms. The acquired CTA images are transferred to dedicated
platforms for processing and reviewing by the use of Seimens Healthcare Multi Modality
Workplace™. By using DSA as the reference standard, the sensitivity, specificity, and
accuracy of CTA was verified by two separate readers. The workstation (Syngo 2008G;
Siemens) was used to generate the CTA images and the bone structures virtually removed by
Neuro-Syno™ application software and were reformatted with Syngo InSpace™ Siemens
software at the workstation. Two neuroradiologists who were kept blinded to all the clinical
data and the DSA results, analyzed the cerebral CTA images independently by using the
source files, maximizing the intensity projections, reformations of the multiplanar data and
reformatted images based on volume-rendering to determine the locations of the aneurysms
present. The CTA percentage of accuracy, error percentage, sensitivity and specificity were
its precision in contrast with digital subtraction angiography (DSA) and other techniques in
use.
Yang et al. (2017) studied the accuracy of the computed tomographic angiography
(CTA) for critical diagnosis of <5 mm cerebral aneurysms in comparison to digital
subtraction angiography (DSA) used as the standard for reference with a patient sample size
of 1366, who initially underwent cerebral computed tomographic angiography followed by
digital subtraction angiography. Initially 1486 participants were chosen which finally made
the sample size of 1366 participants as the rest did not meet the inclusion criteria and were
patients who had undergone DSA prior to CTA or had more than one month between CTA
and DSA. So to avoid discrepancies, those with incomplete image data or with known or
treated aneurysms, only 1366 participants were taken for the study. Out of 1366 patients,
1187 of them were patients with intracranial hemorrhage, 908 patients had presented with de
novo aneurysms whereas 458 of the patients had presented without de novo aneurysms. Of
the 908 patients with de novo aneurysms, 329 patients had large de novo aneurysms and rest
had small to miniscule aneurysms. The acquired CTA images are transferred to dedicated
platforms for processing and reviewing by the use of Seimens Healthcare Multi Modality
Workplace™. By using DSA as the reference standard, the sensitivity, specificity, and
accuracy of CTA was verified by two separate readers. The workstation (Syngo 2008G;
Siemens) was used to generate the CTA images and the bone structures virtually removed by
Neuro-Syno™ application software and were reformatted with Syngo InSpace™ Siemens
software at the workstation. Two neuroradiologists who were kept blinded to all the clinical
data and the DSA results, analyzed the cerebral CTA images independently by using the
source files, maximizing the intensity projections, reformations of the multiplanar data and
reformatted images based on volume-rendering to determine the locations of the aneurysms
present. The CTA percentage of accuracy, error percentage, sensitivity and specificity were
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
99.1%, 0.9%, 97.1% (95% confidence interval (CI), 94–100%) and 98.5% (95% CI, 95%–
99.7%) respectively. The research established that CTA had a higher accuracy for small (<5
mm) cerebral aneurysms detection compared to DSA, the reference standard used.
Rustemi et al. (2015) conducted an experimental study in order to evaluate the
diagnostic performance of 64-section computed tomography angiography in for determining
the cerebral aneurysm through comparison with the three-dimensional (3D) digital
subtraction angiography (DSA), which is a gold standard of diagnosis. In order to assess the
accuracy of the instruments, the researchers recruited 286 patients who underwent surgery
with both of the procedure such as 3D DSA and 64-section CTA for determining intracranial
aneurysm. The parameters for the evaluation were location, size, and shape of aneurysm and
it has drawn comparison with 3D DSA results where sensitivity was measured with the help
of standard protocol for each procedure. Considering, the reference standard, out of 145
patients, 118 patients were detected with aneurysms in 3D DSA. Considering the sensitivity
of CT angiography, it was observed that per-aneurysm, the sensitivity of CTA for uncovering
of the aneurysm was 95.8% with 97% specificity along with 98% accuracy and only 2% error
observed. Hence, in conclusion, it can be concluded that while considering 3D-DSA as a gold
standard for detecting aneurysm, 64-section CT angiography offers the heightened sensitivity
and specificity for detection of intracranial aneurysm.
Feng et al. (2016) conducted a systematic review and meta-analysis of 8 studies in
order to investigate the accuracy of subtraction computed tomography angiography (CTA) in
order to diagnosis intracranial aneurysms. The researchers conducted a meta-analysis of 8
selected studies which compared digital subtraction angiography with subtraction
tomography angiography (CTA). The researchers selected the research articles with the
inclusion criteria such as patients with clinically diagnosed intracranial aneurysm, diagnostic
index test bone subtraction CTA, the orientation standard was DSA or its combination with
99.1%, 0.9%, 97.1% (95% confidence interval (CI), 94–100%) and 98.5% (95% CI, 95%–
99.7%) respectively. The research established that CTA had a higher accuracy for small (<5
mm) cerebral aneurysms detection compared to DSA, the reference standard used.
Rustemi et al. (2015) conducted an experimental study in order to evaluate the
diagnostic performance of 64-section computed tomography angiography in for determining
the cerebral aneurysm through comparison with the three-dimensional (3D) digital
subtraction angiography (DSA), which is a gold standard of diagnosis. In order to assess the
accuracy of the instruments, the researchers recruited 286 patients who underwent surgery
with both of the procedure such as 3D DSA and 64-section CTA for determining intracranial
aneurysm. The parameters for the evaluation were location, size, and shape of aneurysm and
it has drawn comparison with 3D DSA results where sensitivity was measured with the help
of standard protocol for each procedure. Considering, the reference standard, out of 145
patients, 118 patients were detected with aneurysms in 3D DSA. Considering the sensitivity
of CT angiography, it was observed that per-aneurysm, the sensitivity of CTA for uncovering
of the aneurysm was 95.8% with 97% specificity along with 98% accuracy and only 2% error
observed. Hence, in conclusion, it can be concluded that while considering 3D-DSA as a gold
standard for detecting aneurysm, 64-section CT angiography offers the heightened sensitivity
and specificity for detection of intracranial aneurysm.
Feng et al. (2016) conducted a systematic review and meta-analysis of 8 studies in
order to investigate the accuracy of subtraction computed tomography angiography (CTA) in
order to diagnosis intracranial aneurysms. The researchers conducted a meta-analysis of 8
selected studies which compared digital subtraction angiography with subtraction
tomography angiography (CTA). The researchers selected the research articles with the
inclusion criteria such as patients with clinically diagnosed intracranial aneurysm, diagnostic
index test bone subtraction CTA, the orientation standard was DSA or its combination with
11CT ANGIOGRAPHY: THE NEW ACE OF NEURO-INTERVENTIONAL PROCEDURES
neurosurgical findings. The researchers estimated the eminence of the study with the help of
the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool which had 14
variable components for assessment. The CTA percentage of accuracy, error percentage,
sensitivity and specificity were 99.0%, 1%, pooled CTA sensitivity of 99% [95% confidence
interval (CI), 95–100%] and pooled CTA specificity of 94% (95% CI, 86–97%) respectively.
Hence, in conclusion, it can be said that subtraction CTA is highly sensitive in nature and it is
noninvasive as well as a specific method for evaluating as well as diagnosis of intracranial
aneurysm.
A prospective study by Gamal (2015) which compared the performance of CE-MRA
and CTA against DSA in detecting CIA showed that, of 25 patients, aneurysms was detected
in 18 patients of which 13 of 22 had CIA <5mm and 5 had CIA <3mm. Though, sensitivity
of detecting CIA ≤5mm was better with CE-MRA than with CTA, it was not statistically
significant. Hence, the study concluded that CE-MRA performed similar to CTA in detection
of SAH. A meta-analysis which compared performance of CTA with MRA reported that
diagnostic value of CTA was comparable to MRA in diagnosis of CIA (Chen et al., 2018). A
prospective study which compared the diagnostic performance of 3D CE-MRA with that of
3D TOF-MRA in diagnosing CIA >13mm, it was reported that 3T, 3D CE-MRA was better
in terms of diagnosing the sac, neck shape of aneurysm which was larger than 13mm
A meta-analysis by Sailer et al (2014) which compared the diagnostic performance of
different MRA in detection of RA and URA, reported combined sensitivity and specificity of
MRA was 95% and 89% respectively. It was found that MRA-3 Tesla showed better
performance than 1.5 Tesla MRA scanners in diagnosis of CIA ≤5mm. Though many
prospective, retrospective, meta-analysis have been conducted to compare the three neuro-
imaging techniques, it is obvious that each of these imaging techniques have their own
advantages and limitations in terms of detection of CIA <3mm, <5mm, >13mm, version of
neurosurgical findings. The researchers estimated the eminence of the study with the help of
the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool which had 14
variable components for assessment. The CTA percentage of accuracy, error percentage,
sensitivity and specificity were 99.0%, 1%, pooled CTA sensitivity of 99% [95% confidence
interval (CI), 95–100%] and pooled CTA specificity of 94% (95% CI, 86–97%) respectively.
Hence, in conclusion, it can be said that subtraction CTA is highly sensitive in nature and it is
noninvasive as well as a specific method for evaluating as well as diagnosis of intracranial
aneurysm.
A prospective study by Gamal (2015) which compared the performance of CE-MRA
and CTA against DSA in detecting CIA showed that, of 25 patients, aneurysms was detected
in 18 patients of which 13 of 22 had CIA <5mm and 5 had CIA <3mm. Though, sensitivity
of detecting CIA ≤5mm was better with CE-MRA than with CTA, it was not statistically
significant. Hence, the study concluded that CE-MRA performed similar to CTA in detection
of SAH. A meta-analysis which compared performance of CTA with MRA reported that
diagnostic value of CTA was comparable to MRA in diagnosis of CIA (Chen et al., 2018). A
prospective study which compared the diagnostic performance of 3D CE-MRA with that of
3D TOF-MRA in diagnosing CIA >13mm, it was reported that 3T, 3D CE-MRA was better
in terms of diagnosing the sac, neck shape of aneurysm which was larger than 13mm
A meta-analysis by Sailer et al (2014) which compared the diagnostic performance of
different MRA in detection of RA and URA, reported combined sensitivity and specificity of
MRA was 95% and 89% respectively. It was found that MRA-3 Tesla showed better
performance than 1.5 Tesla MRA scanners in diagnosis of CIA ≤5mm. Though many
prospective, retrospective, meta-analysis have been conducted to compare the three neuro-
imaging techniques, it is obvious that each of these imaging techniques have their own
advantages and limitations in terms of detection of CIA <3mm, <5mm, >13mm, version of
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 24
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.