Comprehensive Report on the Effects of Cardiovascular Diseases
VerifiedAdded on 2023/01/23
|7
|1820
|89
Report
AI Summary
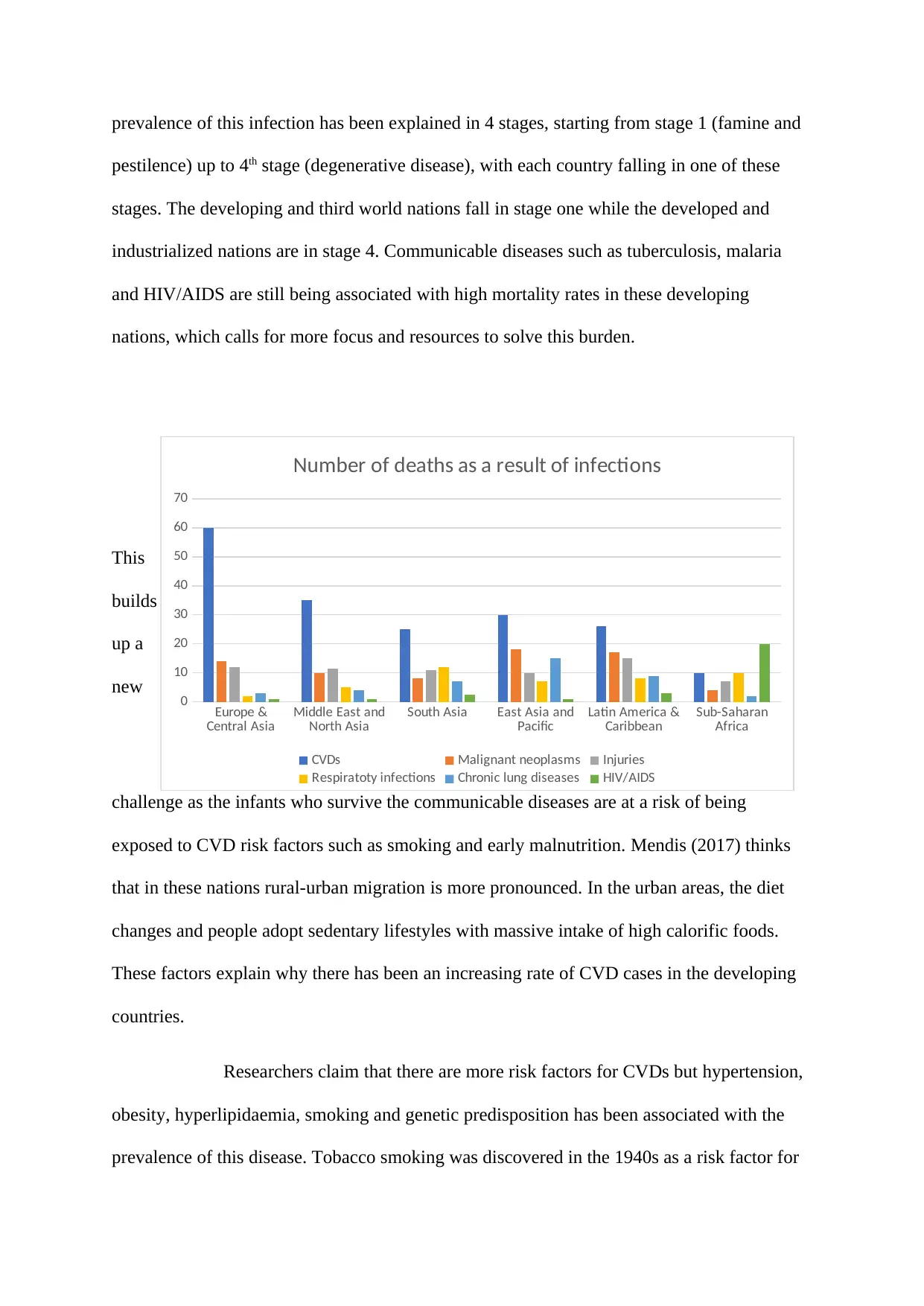
This report examines the multifaceted effects of cardiovascular diseases (CVDs) on global health, drawing upon various studies and reports. It highlights CVDs as a leading cause of death, emphasizing the significance of behavioral risk factors like obesity, smoking, and unhealthy diets. The report delves into the different types of CVDs, including coronary heart disease and stroke, and their impact on both developed and developing nations. It analyzes mortality rates, risk factors such as hypertension and genetic predisposition, and the economic burden associated with CVDs. The report also discusses prevention strategies, including quitting smoking, adopting healthy dietary habits, and regular exercise, to mitigate the impact of CVDs and improve public health outcomes. The study underscores the importance of addressing CVDs through comprehensive strategies to reduce its global impact.

1 out of 7
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.