PUBH7600 Assessment 2: General Practice and Ischemic Heart Disease
VerifiedAdded on 2023/01/04
|13
|3308
|97
Homework Assignment
AI Summary
This assignment analyzes a population-based case-control study examining the relationship between depression and ischemic heart disease (IHD) in men. The study, conducted by Hippisley-Cox et al., investigates whether depression, anxiety, and antidepressant use are associated with the onset of IHD. The study involved 5623 patients from a general practice, with 188 male cases and 139 female cases of IHD, matched with controls. Key findings indicate a three-fold higher risk of IHD among men with a recorded diagnosis of depression. The assignment critically evaluates the study's methodology, including the selection of cases and controls, potential biases, and confounding factors such as cholesterol levels, smoking, and other health conditions. The analysis explores the study's limitations, generalizability, and the authors' attempts to examine dose-response relationships. The assignment also includes an assessment of the study's key messages and the implications of its findings for public health and clinical practice, emphasizing the need for further research to establish a definitive causal link between depression and IHD, particularly in men.

PUBH7600 ASSESMENT 2
S TUDENT ID:
0
S TUDENT ID:
0
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
PUBH7600 ASSESMENT 2...........................................................................................................0
S TUDENT ID:................................................................................................................................0
Table of Contents.............................................................................................................................1
Question 2........................................................................................................................................2
Question 3........................................................................................................................................3
Question 4........................................................................................................................................3
Question 6........................................................................................................................................3
Question 7........................................................................................................................................3
Question 8........................................................................................................................................4
Question 9........................................................................................................................................4
Question 10......................................................................................................................................4
Question 11......................................................................................................................................5
Question 12......................................................................................................................................5
Question 13......................................................................................................................................6
Question 14:.....................................................................................................................................6
Question 16......................................................................................................................................8
Question 17......................................................................................................................................8
Question 18......................................................................................................................................9
Question 19......................................................................................................................................9
1
PUBH7600 ASSESMENT 2...........................................................................................................0
S TUDENT ID:................................................................................................................................0
Table of Contents.............................................................................................................................1
Question 2........................................................................................................................................2
Question 3........................................................................................................................................3
Question 4........................................................................................................................................3
Question 6........................................................................................................................................3
Question 7........................................................................................................................................3
Question 8........................................................................................................................................4
Question 9........................................................................................................................................4
Question 10......................................................................................................................................4
Question 11......................................................................................................................................5
Question 12......................................................................................................................................5
Question 13......................................................................................................................................6
Question 14:.....................................................................................................................................6
Question 16......................................................................................................................................8
Question 17......................................................................................................................................8
Question 18......................................................................................................................................9
Question 19......................................................................................................................................9
1
Question 20 [3 marks].....................................................................................................................9
Establishment of temporal relationship.........................................................................................10
References:....................................................................................................................................11
Question 1
The main topic or the research question is to study of having depression as a risk factor for
having Ischaemic heart diseases in men especially. The study is based on the population based
case (Nikkheslat et al.,2015).
Question 2
The main findings of the case study were that the risk of ischaemic heart diseases was higher in
men about three times than the women. The main factor being depression as per the study. It had
been found out that men with depression proceeding more than 10 years will be more at risk.
The reason for depression leading to coronary diseases like ischaemic heart leads to the fact that
the patients need to take trycyclic anti depressants which may lead to heart diseases. On the
other hand it has been shown that the depression is more prevalent in patients with pro
arrhythmogenic heart diseases because the sympathetic nerves and the parasympathetic nerves
alternate their functions. The former increases and the later decreases. The findings of the study
cannot bank on the facts as depression being the cause of Ischaemic heart disease but it did find
several interrelated cause and effect relations between the two. It has been agreed that the finding
do not prove the main research question and the data had been in sufficient(Hu etal.,2015)..
2
Establishment of temporal relationship.........................................................................................10
References:....................................................................................................................................11
Question 1
The main topic or the research question is to study of having depression as a risk factor for
having Ischaemic heart diseases in men especially. The study is based on the population based
case (Nikkheslat et al.,2015).
Question 2
The main findings of the case study were that the risk of ischaemic heart diseases was higher in
men about three times than the women. The main factor being depression as per the study. It had
been found out that men with depression proceeding more than 10 years will be more at risk.
The reason for depression leading to coronary diseases like ischaemic heart leads to the fact that
the patients need to take trycyclic anti depressants which may lead to heart diseases. On the
other hand it has been shown that the depression is more prevalent in patients with pro
arrhythmogenic heart diseases because the sympathetic nerves and the parasympathetic nerves
alternate their functions. The former increases and the later decreases. The findings of the study
cannot bank on the facts as depression being the cause of Ischaemic heart disease but it did find
several interrelated cause and effect relations between the two. It has been agreed that the finding
do not prove the main research question and the data had been in sufficient(Hu etal.,2015)..
2
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Question 3
The case study was conducted in the rural dispensing areas where mainly trainings take place. A
total of 5623 male and female patients were taken as sample population. This was done on the
borders of Nottinghamshire and Lincolnshire.
Question 4
The basic case s was identified from the practice computer where the data bases of the patients
were included. The patients were selected on the basis of the reports of ischaemic heart diseases
who were receiving repeated treatments and the recent prescriptions were taken into
consideration(Correll,et al.,2015).
The controls were taken by deciding on 299 sample patients where for each patient 2 controls
were decided for the onset of depression before the diagnosis of ischaemic heart disease. The age
of the patients were all more or less above 80, per two controls and total number of patients were
327. But since the unavailability of the controls in the specific age group a ten year age gap was
considered and was divided into male and female patients(Correll,et al.,2015).
Question 6
The process of selecting the controls were though correct but the problem mainly posed when
the proper age group controls could not be obtain due to scarcity in the age group of 80 years and
above. So, the controls could not be evenly distributed .hence it may have hindered the study.
Secondly, the way of obtaining cases like this have several drawbacks. The major among them is
the fact that it is based on the personal recalls of the patient and his previous conditions in this
case often they forget the minute details and thus important data is lost(Dhar and Barton , 2016)..
Question 7
It is evident from the study that the whole sample crowd for the study was taken from the camp
treating general medicines and the practitioners are general practioners. Hence, it is very much
3
The case study was conducted in the rural dispensing areas where mainly trainings take place. A
total of 5623 male and female patients were taken as sample population. This was done on the
borders of Nottinghamshire and Lincolnshire.
Question 4
The basic case s was identified from the practice computer where the data bases of the patients
were included. The patients were selected on the basis of the reports of ischaemic heart diseases
who were receiving repeated treatments and the recent prescriptions were taken into
consideration(Correll,et al.,2015).
The controls were taken by deciding on 299 sample patients where for each patient 2 controls
were decided for the onset of depression before the diagnosis of ischaemic heart disease. The age
of the patients were all more or less above 80, per two controls and total number of patients were
327. But since the unavailability of the controls in the specific age group a ten year age gap was
considered and was divided into male and female patients(Correll,et al.,2015).
Question 6
The process of selecting the controls were though correct but the problem mainly posed when
the proper age group controls could not be obtain due to scarcity in the age group of 80 years and
above. So, the controls could not be evenly distributed .hence it may have hindered the study.
Secondly, the way of obtaining cases like this have several drawbacks. The major among them is
the fact that it is based on the personal recalls of the patient and his previous conditions in this
case often they forget the minute details and thus important data is lost(Dhar and Barton , 2016)..
Question 7
It is evident from the study that the whole sample crowd for the study was taken from the camp
treating general medicines and the practitioners are general practioners. Hence, it is very much
3
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
evident that the records mainly speak of the general condition of the patients and depression state
is often not given much importance or had been treated as a separate case (Correll,et al.,2015).
Question 8
The very notion of control study or what is called the cross over trials have been defined where
the actually affected patients were compared with those who do not have the symptoms and
consequences. The subjects were selected to get two types of treatments at the same time. And
then results were measured and contrasted (Correll,et al.,2015).
Question 9
The main positive side that avoided any kind of bias in this study is the absence of any
specialized treatments as the samples were from a generalist treatment camp and such camps do
not have any bias in the epidemiological studies of the morbidity of the patient(Dhar and Barton ,
2016)..
Question 10
a) The bias in case control study mainly occurs in the cases here the ratio of the cases versus
the controls is not proportionate. In this case though the data obtained was very generalist, but
the age groups were disproportionate, Controls over 80 years of age were not found compared
to other age groups. Moreover, the cases of depression as diagnosed by general practitioners
occur only when they are severe enough. In that case most cases go unnoticed.
4
is often not given much importance or had been treated as a separate case (Correll,et al.,2015).
Question 8
The very notion of control study or what is called the cross over trials have been defined where
the actually affected patients were compared with those who do not have the symptoms and
consequences. The subjects were selected to get two types of treatments at the same time. And
then results were measured and contrasted (Correll,et al.,2015).
Question 9
The main positive side that avoided any kind of bias in this study is the absence of any
specialized treatments as the samples were from a generalist treatment camp and such camps do
not have any bias in the epidemiological studies of the morbidity of the patient(Dhar and Barton ,
2016)..
Question 10
a) The bias in case control study mainly occurs in the cases here the ratio of the cases versus
the controls is not proportionate. In this case though the data obtained was very generalist, but
the age groups were disproportionate, Controls over 80 years of age were not found compared
to other age groups. Moreover, the cases of depression as diagnosed by general practitioners
occur only when they are severe enough. In that case most cases go unnoticed.
4
b) Yes, the bias is generally misclassified as the population from where the samples have been
taken have been practiced solely by the particular medical camp. But the significant bias is seen
in the measurement of the data statistically as the difference in the cases and the controls
proportions. A particular age group was losing its population that is one with more than 80
years. Secondly, the camp being a general practitioner did not give much importance to the
mental condition and attended the physical conditions more.( Dhar and Barton , 2016).
Question 11
It is seen in the men (Table 3), that the men with the
Heart disease of ischaemia, have recorded onset of depression after the heart disease ((2.20; 1.28
to 3.79; P = 0.005). as compared to the men without the heart diseases. On the other hand,
depression prior to heart disease was calculated as :( adjusted 2.42; 1.39 to 4.21; P = 0.002). And
the heart disease before depression is calculated as (adjusted 0.70; 0.15 to 3.16, P = 0.64). For
women, the rate of depression without heart disease is twice than the men (adjusted 1.86;
1.10 to 3.16; P = 0.02).
Question 12
The main confounders found in the relational study between depression s the cause of
ischaemic heart disease, is cholesterol. Where some evidences have shown the presence of
increased cholesterol as the reason for the heart disease, on the other hand, to has been seen that
low cholesterol can be reason for depression and suicidal tendencies. So , the complex relation
may bring us it this conclusion that if high cholesterol is associated with heart disease and low
cholesterol with depression then patients with ischaemc heart disease would have low depression
because of high cholesterol and vice versa.
Again in women there has been no correlation between the depression and heart diseases.
Women with depression do not show any ischaemic heart disease rather other diseases like
anxiety , was associated with depression and not necessarily ischaemic heart disease was the
effect of anxiety.
5
taken have been practiced solely by the particular medical camp. But the significant bias is seen
in the measurement of the data statistically as the difference in the cases and the controls
proportions. A particular age group was losing its population that is one with more than 80
years. Secondly, the camp being a general practitioner did not give much importance to the
mental condition and attended the physical conditions more.( Dhar and Barton , 2016).
Question 11
It is seen in the men (Table 3), that the men with the
Heart disease of ischaemia, have recorded onset of depression after the heart disease ((2.20; 1.28
to 3.79; P = 0.005). as compared to the men without the heart diseases. On the other hand,
depression prior to heart disease was calculated as :( adjusted 2.42; 1.39 to 4.21; P = 0.002). And
the heart disease before depression is calculated as (adjusted 0.70; 0.15 to 3.16, P = 0.64). For
women, the rate of depression without heart disease is twice than the men (adjusted 1.86;
1.10 to 3.16; P = 0.02).
Question 12
The main confounders found in the relational study between depression s the cause of
ischaemic heart disease, is cholesterol. Where some evidences have shown the presence of
increased cholesterol as the reason for the heart disease, on the other hand, to has been seen that
low cholesterol can be reason for depression and suicidal tendencies. So , the complex relation
may bring us it this conclusion that if high cholesterol is associated with heart disease and low
cholesterol with depression then patients with ischaemc heart disease would have low depression
because of high cholesterol and vice versa.
Again in women there has been no correlation between the depression and heart diseases.
Women with depression do not show any ischaemic heart disease rather other diseases like
anxiety , was associated with depression and not necessarily ischaemic heart disease was the
effect of anxiety.
5
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Third confounders were dead patients whose history was relevant for study but they were not
available for present diagnosis((Correll,et al.,2015).
Question 13
No, the authors did not account for all the e confounders for the study of ischaemic heart disease
as the effect of depressions. The confounders are anxiety, smoking, cholesterol and the women
health that may affect the diagnosis of ishchaemic heart disease and its relation to depression. It
is very evident than in men, it has been found that they are more prone to ischaemic heart
diseases twice as much as women with the onset of depression over more than 10 years. Women
on the other hand are more prone to anxiety than depression and it is does not lead to any heart
diseases in them. On the other hand the authors did not consider the presence of cholesterol, bad
smoking habits, and other health conditions like diabetes or hyper tension(Dhar and Barton ,
2016).
Question 14:
Table 3 exhibit the results of the univariate and multivariate examination for men with and
without ischaemic heart disease. On univariate examination, men with an analysis of depression
were three times more feasible than controls of the same age to build up ischaemic heart disease
(odds ratio 3.09; 95% confidence interval1.33 to 7.21; P = 0.009). The danger of ischaemic heart
disease continue when smoking status, diabetes, hypertension, and deprivation score were
included in the calculations (adjusted 2.75; 1.13 to 6.69; P = 0.03).The data were re examined by
assessing the mean values for each group of controls with the value for their relevant case by
using the Wilcox on signed rankest. Men with ischaemic heart disease had a high score for
6
available for present diagnosis((Correll,et al.,2015).
Question 13
No, the authors did not account for all the e confounders for the study of ischaemic heart disease
as the effect of depressions. The confounders are anxiety, smoking, cholesterol and the women
health that may affect the diagnosis of ishchaemic heart disease and its relation to depression. It
is very evident than in men, it has been found that they are more prone to ischaemic heart
diseases twice as much as women with the onset of depression over more than 10 years. Women
on the other hand are more prone to anxiety than depression and it is does not lead to any heart
diseases in them. On the other hand the authors did not consider the presence of cholesterol, bad
smoking habits, and other health conditions like diabetes or hyper tension(Dhar and Barton ,
2016).
Question 14:
Table 3 exhibit the results of the univariate and multivariate examination for men with and
without ischaemic heart disease. On univariate examination, men with an analysis of depression
were three times more feasible than controls of the same age to build up ischaemic heart disease
(odds ratio 3.09; 95% confidence interval1.33 to 7.21; P = 0.009). The danger of ischaemic heart
disease continue when smoking status, diabetes, hypertension, and deprivation score were
included in the calculations (adjusted 2.75; 1.13 to 6.69; P = 0.03).The data were re examined by
assessing the mean values for each group of controls with the value for their relevant case by
using the Wilcox on signed rankest. Men with ischaemic heart disease had a high score for
6
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
depression than the controls did (P = 0.01).This is unswerving with the results of the provisional
logistic regression analysis.
Table 4, of the study shows the univariate and the multivariate analysis of the relation between
depression and ischaemic heart disease among women. It was found that depression and
ischaemic heart disease was not interrelated with women. In fact the men were at twice the risk
of getting the heart disease than the women with the onset of depression( Freeland et al.,20
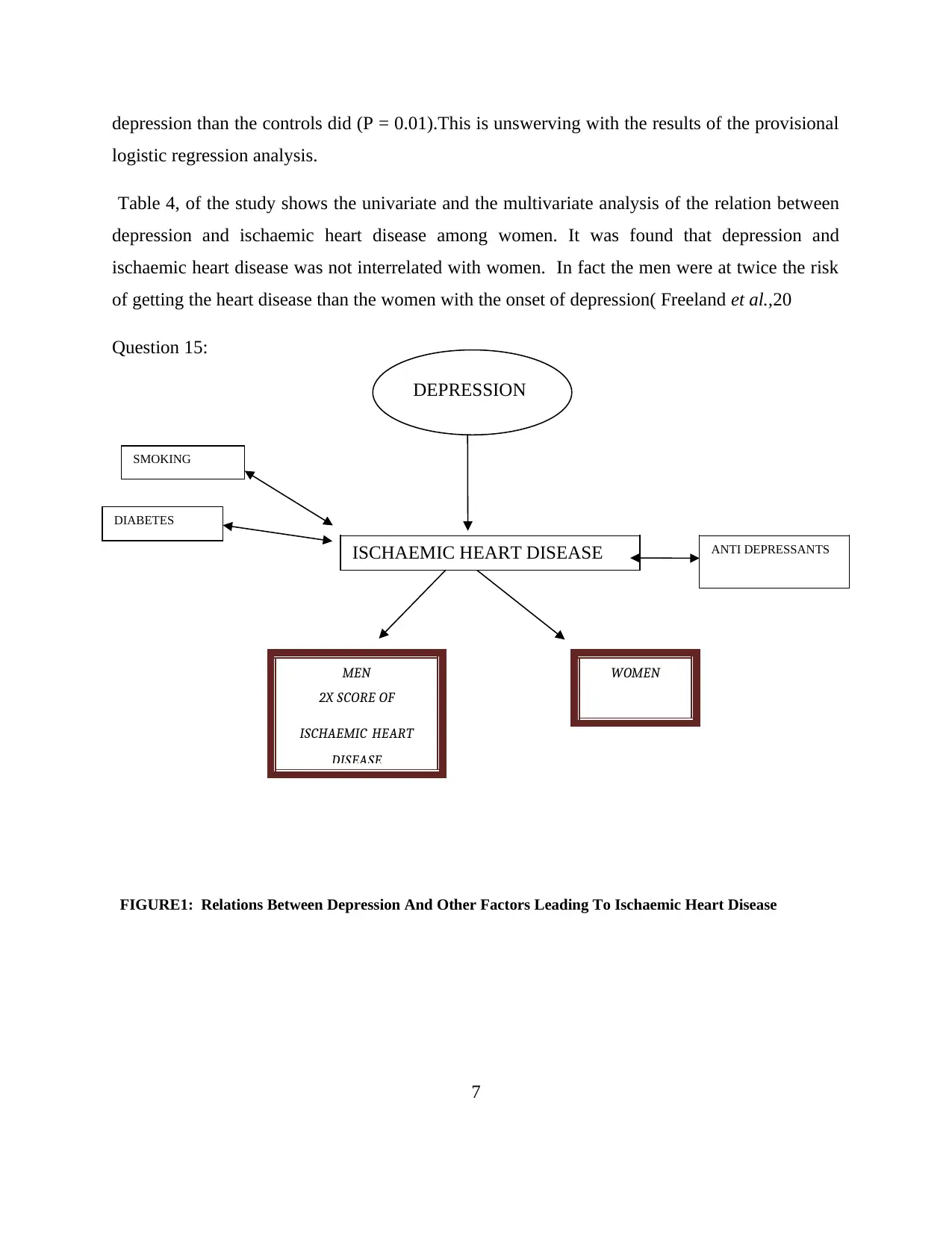
Question 15:
FIGURE1: Relations Between Depression And Other Factors Leading To Ischaemic Heart Disease
7
DEPRESSION
ISCHAEMIC HEART DISEASE
WOMEN
ANTI DEPRESSANTS
SMOKING
DIABETES
MEN
2X SCORE OF
ISCHAEMIC HEART
DISEASE
logistic regression analysis.
Table 4, of the study shows the univariate and the multivariate analysis of the relation between
depression and ischaemic heart disease among women. It was found that depression and
ischaemic heart disease was not interrelated with women. In fact the men were at twice the risk
of getting the heart disease than the women with the onset of depression( Freeland et al.,20
Question 15:
FIGURE1: Relations Between Depression And Other Factors Leading To Ischaemic Heart Disease
7
DEPRESSION
ISCHAEMIC HEART DISEASE
WOMEN
ANTI DEPRESSANTS
SMOKING
DIABETES
MEN
2X SCORE OF
ISCHAEMIC HEART
DISEASE
Question 16
The study by “Julia HippisleyCox, Katherine Fielding, Mike Pringle”, has given us few key
messages, like there has been no research to study the interrelation between myocardial disease
and depression. The study found put that there is a relation between the ischaemic heart disease
and the onset of depression resulting in the disease. But again the study does not ensure that this
is the only reason for it.
Depression showed a reason to be the cause of ischaemic heart for the men but not for the
women. And there may be other reasons for the heart disease. So, this study is not enough for
implementing the fact that depression is the main reason for the onset of the ishchaemic heart
disease in humans despite of age, sex and gender.
The study did not have any specific reason to prove the relation between anti depressants and
heart disease. Last but not the least there is a doubt in diagnosing whether depression is really
happening or is it only a confused state of vital exhaustion. The separate cofounding reasons may
also be present for depression as well as heart disease. So, tough the study did give us a few
good ideas and assumptions but it really did not provide us any cause effect relation between
depression and ischaemic heart disease( Dhar and Barton , 2016)..
Question 17
Yes, the findings are generaisable to other populations too. As, the general practice camps has
been taken into consideration for the study where the general treatments are done mainly and
specialized treatments are relocated to hospitals. The cause effect relationship of the depression
causing an onset of ischaemic heart disease is a common problem and can be studied devoid of
all areas region, age gaps and gender. The cross over trials as discussed in the article has been
said can be followed by all communities without any bias. But on the other hand such studies are
8
The study by “Julia HippisleyCox, Katherine Fielding, Mike Pringle”, has given us few key
messages, like there has been no research to study the interrelation between myocardial disease
and depression. The study found put that there is a relation between the ischaemic heart disease
and the onset of depression resulting in the disease. But again the study does not ensure that this
is the only reason for it.
Depression showed a reason to be the cause of ischaemic heart for the men but not for the
women. And there may be other reasons for the heart disease. So, this study is not enough for
implementing the fact that depression is the main reason for the onset of the ishchaemic heart
disease in humans despite of age, sex and gender.
The study did not have any specific reason to prove the relation between anti depressants and
heart disease. Last but not the least there is a doubt in diagnosing whether depression is really
happening or is it only a confused state of vital exhaustion. The separate cofounding reasons may
also be present for depression as well as heart disease. So, tough the study did give us a few
good ideas and assumptions but it really did not provide us any cause effect relation between
depression and ischaemic heart disease( Dhar and Barton , 2016)..
Question 17
Yes, the findings are generaisable to other populations too. As, the general practice camps has
been taken into consideration for the study where the general treatments are done mainly and
specialized treatments are relocated to hospitals. The cause effect relationship of the depression
causing an onset of ischaemic heart disease is a common problem and can be studied devoid of
all areas region, age gaps and gender. The cross over trials as discussed in the article has been
said can be followed by all communities without any bias. But on the other hand such studies are
8
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
good for short term treatment cycles and where you do not have to keep a watch over a period of
time(Correll,et al.,2015).
Question 18
Yes, the authors did attempt to explore a dose response relationship in this case study by giving
then patients anti depressants and comparing them with patients, who do not take anti
depressants. But however, it has been seen that the doses of anti depressants do not determine the
cause of the heart disease. Rather it has been found out that without the anti depressant the
disease were present in many patients(Chen, Edmonson ,Kronish,2017).
Question 19
The present study has been agreed upon by the authors as not very powerful. As the conclusion
could not be proved that the onset of depression leads to the ischaemic heart disease. The john
Hopkins society did find out that every one in 10 American aged 18 and older have depression
but with no heart disease. However, it is found by them that the heart disease is the cause of
depression among many Americans sine it restricts their daily activities. According to Iowa
cardiologist, Geisha, heart disease and depression have two way cause and effect relationship.
A number of factors again have shown that depression is more of a genetic disease. The causes
range from biological, environmental and psychological. Depressions are more common in
women and s they take greater responsibilities of home and also the work front. Moreover, child
bearing, and nurturing causes them stress and trauma leading to depression( Carney et al.,2016).
Question 20 [3 marks]
The Bradford – Hill’s criteria of temporality, give s us a set of 9 principles in a cause effect
relationship between diseases. These are
9
time(Correll,et al.,2015).
Question 18
Yes, the authors did attempt to explore a dose response relationship in this case study by giving
then patients anti depressants and comparing them with patients, who do not take anti
depressants. But however, it has been seen that the doses of anti depressants do not determine the
cause of the heart disease. Rather it has been found out that without the anti depressant the
disease were present in many patients(Chen, Edmonson ,Kronish,2017).
Question 19
The present study has been agreed upon by the authors as not very powerful. As the conclusion
could not be proved that the onset of depression leads to the ischaemic heart disease. The john
Hopkins society did find out that every one in 10 American aged 18 and older have depression
but with no heart disease. However, it is found by them that the heart disease is the cause of
depression among many Americans sine it restricts their daily activities. According to Iowa
cardiologist, Geisha, heart disease and depression have two way cause and effect relationship.
A number of factors again have shown that depression is more of a genetic disease. The causes
range from biological, environmental and psychological. Depressions are more common in
women and s they take greater responsibilities of home and also the work front. Moreover, child
bearing, and nurturing causes them stress and trauma leading to depression( Carney et al.,2016).
Question 20 [3 marks]
The Bradford – Hill’s criteria of temporality, give s us a set of 9 principles in a cause effect
relationship between diseases. These are
9
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Strength- it is not evident that a small association will lead us to the actual facts. The
more the bigger the better. Here in the study the association was quite small
comparatively.
Consistency- consistent findings yield result. Here, consistency was missing due to a
smaller group and a particular age group us not consistent.
Specificity- it was there in this study as a specific camp as taken into consideration.
Temporality- the timing. The effect as to occur after the cause. But in this study it was
not seen like that. Temporality was inconsistent and in some cases the effects were
present in an individurate of depression along with iscalistic manner.
Biological gradient- the gradation of the cause effect has to be consistent. In this study
there was no consistency as the level of depressions were more among women with no
heart diseases.
Plausibility- cause and effect mechanism should be prominent.
Coherence- there should be a unity between the laboratory findings and real findings
Experiment- experiments are sometimes important
Reversibility- the findings of the study do not show the appearance of cause with the
appearance of effect. There are cases where each one id presents without the cause or the
effect.( Carney, Freedland , 2017).
Establishment of temporal relationship
There a record of ishcaemic heart disease and depression being the most common diseases in
developed countries. However, this study has failed to establish the relationship between tehe
two. Though it has been proved that the depression is most common along with coronary disease
in men twice than the females but it does not hold strong the fact that both are interrelated.
Depression may lead to myocardial infarction but mortality rates are even same without any
depression along with it (Bradley SM, Rumsfeld JS,2015).
10
more the bigger the better. Here in the study the association was quite small
comparatively.
Consistency- consistent findings yield result. Here, consistency was missing due to a
smaller group and a particular age group us not consistent.
Specificity- it was there in this study as a specific camp as taken into consideration.
Temporality- the timing. The effect as to occur after the cause. But in this study it was
not seen like that. Temporality was inconsistent and in some cases the effects were
present in an individurate of depression along with iscalistic manner.
Biological gradient- the gradation of the cause effect has to be consistent. In this study
there was no consistency as the level of depressions were more among women with no
heart diseases.
Plausibility- cause and effect mechanism should be prominent.
Coherence- there should be a unity between the laboratory findings and real findings
Experiment- experiments are sometimes important
Reversibility- the findings of the study do not show the appearance of cause with the
appearance of effect. There are cases where each one id presents without the cause or the
effect.( Carney, Freedland , 2017).
Establishment of temporal relationship
There a record of ishcaemic heart disease and depression being the most common diseases in
developed countries. However, this study has failed to establish the relationship between tehe
two. Though it has been proved that the depression is most common along with coronary disease
in men twice than the females but it does not hold strong the fact that both are interrelated.
Depression may lead to myocardial infarction but mortality rates are even same without any
depression along with it (Bradley SM, Rumsfeld JS,2015).
10
References:
Bradley SM, Rumsfeld JS. Depression and cardiovascular disease. Trends in Cardiovascular
Medicine. 2015 Oct 1;25(7):614-22.
Carney RM, Freedland KE, Steinmeyer BC, Rubin EH, Stein PK, Rich MW. Nighttime heart
rate predicts response to depression treatment in patients with coronary heart disease. Journal of
affective disorders. 2016 Aug 1;200:165-71.
Carney RM, Freedland KE. Depression and coronary heart disease. Nature Reviews Cardiology.
2017 Mar;14(3):145.
Cohen BE, Edmondson D, Kronish IM. State of the art review: depression, stress, anxiety, and
cardiovascular disease. American journal of hypertension. 2015 Apr 24;28(11):1295-302.
Correll CU, Detraux J, De Lepeleire J, De Hert M. Effects of antipsychotics, antidepressants and
mood stabilizers on risk for physical diseases in people with schizophrenia, depression and
bipolar disorder. World psychiatry. 2015 Jun;14(2):119-36.
11
Bradley SM, Rumsfeld JS. Depression and cardiovascular disease. Trends in Cardiovascular
Medicine. 2015 Oct 1;25(7):614-22.
Carney RM, Freedland KE, Steinmeyer BC, Rubin EH, Stein PK, Rich MW. Nighttime heart
rate predicts response to depression treatment in patients with coronary heart disease. Journal of
affective disorders. 2016 Aug 1;200:165-71.
Carney RM, Freedland KE. Depression and coronary heart disease. Nature Reviews Cardiology.
2017 Mar;14(3):145.
Cohen BE, Edmondson D, Kronish IM. State of the art review: depression, stress, anxiety, and
cardiovascular disease. American journal of hypertension. 2015 Apr 24;28(11):1295-302.
Correll CU, Detraux J, De Lepeleire J, De Hert M. Effects of antipsychotics, antidepressants and
mood stabilizers on risk for physical diseases in people with schizophrenia, depression and
bipolar disorder. World psychiatry. 2015 Jun;14(2):119-36.
11
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.