Analysis of Type 2 Diabetes in Children: Risk Factors & Solutions
VerifiedAdded on 2023/06/11
|10
|1724
|165
Report
AI Summary
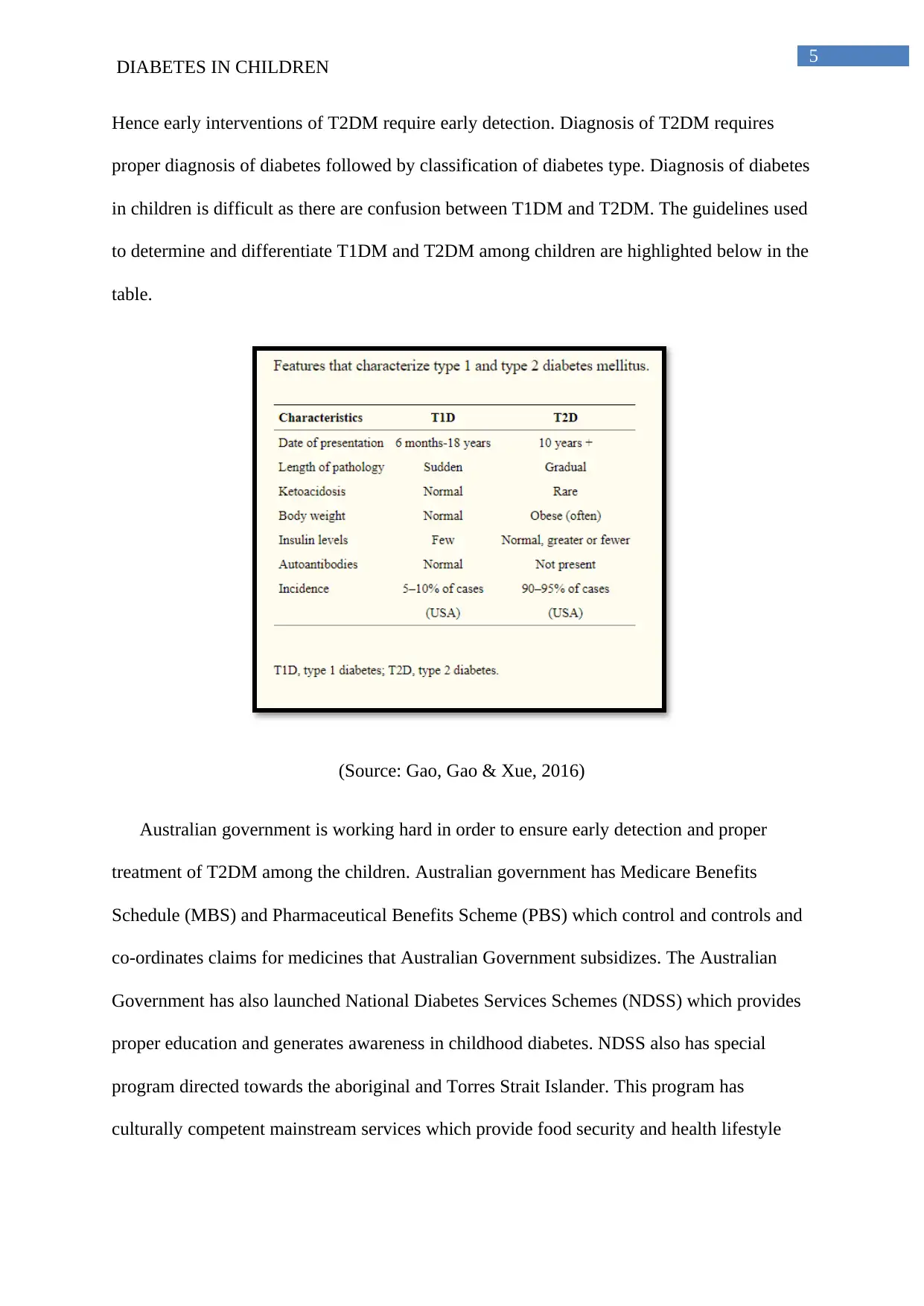
This report examines the prevalence and causes of Type 2 Diabetes Mellitus (T2DM) among children in Australia, where approximately 31,000 individuals aged 10-24 are affected. The report highlights that indigenous Australian children have an eight-times higher occurrence rate compared to non-indigenous children. Key non-modifiable risk factors include genetic predisposition, exposure to maternal diabetes, and increased plasma insulin levels during puberty. Modifiable risk factors identified are childhood obesity, lack of physical activity, and unhealthy diets. The suggested solutions involve lifestyle modifications, such as increased physical activity and balanced diets, alongside pharmacological interventions like metformin and insulin treatment. The Australian government's initiatives, including the National Diabetes Services Schemes (NDSS), aim to raise awareness and provide subsidized medicines. The report concludes by recommending improved monitoring systems to capture unreported diabetes cases, especially among aboriginal populations, and better detection systems to differentiate between type 1 and type 2 diabetes, ensuring early and appropriate treatment.


1 out of 10
Related Documents



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.