Analysis of Health and Social Care Inequalities: Diabetes in India
VerifiedAdded on 2021/01/01
|18
|6616
|445
Report
AI Summary
This report examines health and social care inequalities, specifically focusing on the disparities in diabetes experiences within the Indian adult population. The introduction highlights the issue of health inequalities, emphasizing the need for equal opportunities for a healthy life, and sets the context for the study on type 2 diabetes in India. The report delves into health outcomes, comparing diabetes-related outcomes globally and nationally, including a discussion on the rising prevalence among women in India. It explores determinants like socioeconomic status, gender, age, lifestyle, and health behaviors that influence health. The report also presents policy responses aimed at addressing the identified gaps in health and social care, and concludes by emphasizing the importance of addressing health inequalities to achieve better health outcomes. The report provides statistical data, facts, and figures to support its arguments, including the global and national statistics on diabetes and its impact on different demographics.
Health and Social Care
Inequalities
Inequalities
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
TABLE OF CONTENTS
INTRODUCTION...........................................................................................................................1
PROBLEM STATEMENT .............................................................................................................1
SECTION 2: HEALTH OUTCOMES.............................................................................................4
Describing Diabetes related outcomes globally and nationally.............................................4
Diabetes patient in India rising with women..........................................................................5
Diabetes related Facts at global level.....................................................................................6
SECTION 3: DETERMINANTS WHICH AFFECTS GENDER, SOCIO ECONOMIC
STATUS, AGE, LIFESTYLE AND HEALTH BEHAVIOUR......................................................6
Socio-economic status as a determinant of health .................................................................7
Determinant of health......................................................................................................................9
Determinant that affects Health Behaviour............................................................................9
SECTION 4: PRESENTING THE POLICY, RESPOND TO GAP...............................................9
CONCLUSION..............................................................................................................................11
REFERENCES .............................................................................................................................13
INTRODUCTION...........................................................................................................................1
PROBLEM STATEMENT .............................................................................................................1
SECTION 2: HEALTH OUTCOMES.............................................................................................4
Describing Diabetes related outcomes globally and nationally.............................................4
Diabetes patient in India rising with women..........................................................................5
Diabetes related Facts at global level.....................................................................................6
SECTION 3: DETERMINANTS WHICH AFFECTS GENDER, SOCIO ECONOMIC
STATUS, AGE, LIFESTYLE AND HEALTH BEHAVIOUR......................................................6
Socio-economic status as a determinant of health .................................................................7
Determinant of health......................................................................................................................9
Determinant that affects Health Behaviour............................................................................9
SECTION 4: PRESENTING THE POLICY, RESPOND TO GAP...............................................9
CONCLUSION..............................................................................................................................11
REFERENCES .............................................................................................................................13
INTRODUCTION
PROBLEM STATEMENT
Reducing health inequalities means giving everyone the same opportunities to lead a
healthy life, no matter where they live or who they are. The term inequalities exist across the
range of dimensions such as socio economic deprivation and personal characteristics like age and
sex. Present essay will be based on the topic of Health and Social care Inequalities with the issue
of inequalities in experience of 2 types of diabetes in Indian Adult population where the study is
presenting in-depth knowledge regarding inequalities of health and social sector goals (Thomas,
M. Cooper and Zimmet, 2016). Health and inequalities have been instrumental and most
attentive matter for vulnerable groups in India. As per the different researches, health inequalities
develop societal disparities in health and healthcare. Present study will be based on the topic of
“Inequalities in experience of type 2 Diabetes in India Adult Population”. As per the statistics,
India ranked at number 101th out of 131 countries.
In India, cases of Diabetes have rapidly increased from the last past quarter century. India
has contributed a major part of global burden for growing non-communicable diseases (Adler,
and et.al., 2016). However, study will be going to present in study about health outcomes
through making comparison on the basis of age, gender, etc. in order to describe the diabetes
related outcomes globally and nationally. Besides, it will also be presenting the possible effects
that will be going to affect human body such as lifestyle, health behaviour and age factor.
Besides, at the end of section, assignment will be going through to explain possible action
policies taken by company in order to fill the gap. Motivation for studying health inequalities in
order to meet out the best goal oriented process and effective management task. For that,
government needs to evaluate and enhance the opportunities of social, economic and historical
factor which contributing to inequalities in health (Agyemang and et.al., 2016).
Apart from that, Government also need to organise surveys and taking care of the
requirements of people in order to reduce the possibilities of effective management targets.
Reducing Inequalities should be followed or applied to undertake some serious cases and also
affect the better effective challenges and goals. Reducing the inequalities in health proposes in
order to meet out the long terms sources and effective management task and effective purposeful
1
PROBLEM STATEMENT
Reducing health inequalities means giving everyone the same opportunities to lead a
healthy life, no matter where they live or who they are. The term inequalities exist across the
range of dimensions such as socio economic deprivation and personal characteristics like age and
sex. Present essay will be based on the topic of Health and Social care Inequalities with the issue
of inequalities in experience of 2 types of diabetes in Indian Adult population where the study is
presenting in-depth knowledge regarding inequalities of health and social sector goals (Thomas,
M. Cooper and Zimmet, 2016). Health and inequalities have been instrumental and most
attentive matter for vulnerable groups in India. As per the different researches, health inequalities
develop societal disparities in health and healthcare. Present study will be based on the topic of
“Inequalities in experience of type 2 Diabetes in India Adult Population”. As per the statistics,
India ranked at number 101th out of 131 countries.
In India, cases of Diabetes have rapidly increased from the last past quarter century. India
has contributed a major part of global burden for growing non-communicable diseases (Adler,
and et.al., 2016). However, study will be going to present in study about health outcomes
through making comparison on the basis of age, gender, etc. in order to describe the diabetes
related outcomes globally and nationally. Besides, it will also be presenting the possible effects
that will be going to affect human body such as lifestyle, health behaviour and age factor.
Besides, at the end of section, assignment will be going through to explain possible action
policies taken by company in order to fill the gap. Motivation for studying health inequalities in
order to meet out the best goal oriented process and effective management task. For that,
government needs to evaluate and enhance the opportunities of social, economic and historical
factor which contributing to inequalities in health (Agyemang and et.al., 2016).
Apart from that, Government also need to organise surveys and taking care of the
requirements of people in order to reduce the possibilities of effective management targets.
Reducing Inequalities should be followed or applied to undertake some serious cases and also
affect the better effective challenges and goals. Reducing the inequalities in health proposes in
order to meet out the long terms sources and effective management task and effective purposeful
1
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
return. It has been analysed that 50% of the people were come from the side of Bangladesh and
Pakistan and lived in England 2011 (Vanstone and et.al., 2017).
Accordingly, there are two types of diabetic damages which is describe by different
definition. Type 1 diabetic is known as Insulin-dependent juvenile which is characterized insulin
production and requires a daily diagnosis by insulin (Vanstone and et.al., 2017). This type of
diabetic is curable and preventable. On the other side, second type of diabetes secretory defect on
the background of insulin resistance (World Health Organization, 2014). This type of diabetes
patient are highly exist around the world by the result of excess body weight and physical
inactivity. In order to analyse the scenario of India, People under age 44 are majorly suffered
from Diabetes (Weng and et.al., 2017).
Diabetes is a medical status in which level of sugar in the blood becomes too high. There
are majorly two types of diabetes i.e. Type 1 and Type 2. Type 1 diabetes has elevated when
body stops making enough insulin (Arcaya, Arcaya and Subramanian, 2015). This type of
diabetes hits at the age of 40 years. Type 1 diabetes can be treated by proper diet and with the
help of daily insulin. On the other hand, second type of diabetes is highly common. It occurs
when body still making some short of insulin in the body. This diabetes happened above the age
of 40 years.
Globally, it has been found that 422 million adults whose age more than above 18 are
living with diabetes mellitus as per the current research of 2016 from World Health Organisation
(WHO). This health issue is increasing the number of patients across world. India is ranking on
the sixth position of the IDF SEA region (IDF SEA Members, 2018). 425 million people
diagnosed with diabetes in the world and 82 million people in the SEA region. Total number of
cases suffering from this health issue are 72.946.400 in India 2017. Present essay will be going
to explain the inequalities of diabetes among adults (Age above 18) of India. In this, essay will
be presenting facts and figures about Indian adult goals and objectives in order to meet the aim
of essay. Further, study will be presenting the health outcomes by using comparison using age,
gender etc. To describe diabetes related outcomes globally and nationally. Moreover, other
significant determinates are also going to be presented which affects gender, age, lifestyle and
health behaviour that affect the human body and their perception level (Batterham and et.al.,
2016).
2
Pakistan and lived in England 2011 (Vanstone and et.al., 2017).
Accordingly, there are two types of diabetic damages which is describe by different
definition. Type 1 diabetic is known as Insulin-dependent juvenile which is characterized insulin
production and requires a daily diagnosis by insulin (Vanstone and et.al., 2017). This type of
diabetic is curable and preventable. On the other side, second type of diabetes secretory defect on
the background of insulin resistance (World Health Organization, 2014). This type of diabetes
patient are highly exist around the world by the result of excess body weight and physical
inactivity. In order to analyse the scenario of India, People under age 44 are majorly suffered
from Diabetes (Weng and et.al., 2017).
Diabetes is a medical status in which level of sugar in the blood becomes too high. There
are majorly two types of diabetes i.e. Type 1 and Type 2. Type 1 diabetes has elevated when
body stops making enough insulin (Arcaya, Arcaya and Subramanian, 2015). This type of
diabetes hits at the age of 40 years. Type 1 diabetes can be treated by proper diet and with the
help of daily insulin. On the other hand, second type of diabetes is highly common. It occurs
when body still making some short of insulin in the body. This diabetes happened above the age
of 40 years.
Globally, it has been found that 422 million adults whose age more than above 18 are
living with diabetes mellitus as per the current research of 2016 from World Health Organisation
(WHO). This health issue is increasing the number of patients across world. India is ranking on
the sixth position of the IDF SEA region (IDF SEA Members, 2018). 425 million people
diagnosed with diabetes in the world and 82 million people in the SEA region. Total number of
cases suffering from this health issue are 72.946.400 in India 2017. Present essay will be going
to explain the inequalities of diabetes among adults (Age above 18) of India. In this, essay will
be presenting facts and figures about Indian adult goals and objectives in order to meet the aim
of essay. Further, study will be presenting the health outcomes by using comparison using age,
gender etc. To describe diabetes related outcomes globally and nationally. Moreover, other
significant determinates are also going to be presented which affects gender, age, lifestyle and
health behaviour that affect the human body and their perception level (Batterham and et.al.,
2016).
2
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Inequalities in diabetes has become the major concern or issue in western countries. In
India, there are large inequalities of diabetes found among the youth whose between 15 to 24.
Because of the early age diabetes are highly diagnosed in younger age due to improper diet plan,
insufficient sources and improper life of quality (Batterham and et.al., 2016). At the age of 10-19
years, the rate highly diagnosed cases of Type 2 diabetes.
Health inequalities are the most unfair and avoidable cause for people across social
groups and in between different population groups (Kapilashrami, Hill and Meer, 2015). The
main causes behind these health inequalities are unequal distribution of power, income or wealth.
This is the reason due to which poverty and marginalisation of people arise in the society.
Further, this unequal distribution process may lead to enhance and influence the health issues,
work, education and good quality housing.
Some of the necessary determinants of health approaches are social decisive in order to
reduce the inequalities among people. People should reduce the disparities from place where
people get tortured on the basis of their race, ethnicity and gender. In order to reduce these
issues, it is highly required to increasing the social and structural conditions needed for good
health. Government should also take development and collaborative actions to make healthy
environment for the needed people (Nambiar and et.al., 2015). Overall, people should adopt
collaborative and proactive approaches in order to reduce health inequalities among and in
between population.
Type 2 Diabetes involves greater risk of chronic health in human body, which could be
the cause of blindness, amputation, kidney and depression (Zhu and Zhang, 2016). Besides,
Diabetes could be very harmful and involve the risk of cardiovascular disease. Present study will
be helpful to explore the importance of urgent major policies in order to build up better growth
policy targets. Diabetes is the very serious concern for the people that must be operated with the
help of some measure effective treatment. Another issue that, sometimes people ignored their
health concern due to having issue of lack of money or resources as well (Bartley, 2016). For
that, Government should need to take some action and offer some measure support services to
people in their bad health.
3
India, there are large inequalities of diabetes found among the youth whose between 15 to 24.
Because of the early age diabetes are highly diagnosed in younger age due to improper diet plan,
insufficient sources and improper life of quality (Batterham and et.al., 2016). At the age of 10-19
years, the rate highly diagnosed cases of Type 2 diabetes.
Health inequalities are the most unfair and avoidable cause for people across social
groups and in between different population groups (Kapilashrami, Hill and Meer, 2015). The
main causes behind these health inequalities are unequal distribution of power, income or wealth.
This is the reason due to which poverty and marginalisation of people arise in the society.
Further, this unequal distribution process may lead to enhance and influence the health issues,
work, education and good quality housing.
Some of the necessary determinants of health approaches are social decisive in order to
reduce the inequalities among people. People should reduce the disparities from place where
people get tortured on the basis of their race, ethnicity and gender. In order to reduce these
issues, it is highly required to increasing the social and structural conditions needed for good
health. Government should also take development and collaborative actions to make healthy
environment for the needed people (Nambiar and et.al., 2015). Overall, people should adopt
collaborative and proactive approaches in order to reduce health inequalities among and in
between population.
Type 2 Diabetes involves greater risk of chronic health in human body, which could be
the cause of blindness, amputation, kidney and depression (Zhu and Zhang, 2016). Besides,
Diabetes could be very harmful and involve the risk of cardiovascular disease. Present study will
be helpful to explore the importance of urgent major policies in order to build up better growth
policy targets. Diabetes is the very serious concern for the people that must be operated with the
help of some measure effective treatment. Another issue that, sometimes people ignored their
health concern due to having issue of lack of money or resources as well (Bartley, 2016). For
that, Government should need to take some action and offer some measure support services to
people in their bad health.
3
SECTION 2: HEALTH OUTCOMES
Describing Diabetes related outcomes globally and nationally.
Like many other different developing countries, India is also facing some threats in
several communicable diseases due to different lifestyles. As per the current scenario of India, in
next 20 years, India will be on the place where one-fifth population will be diagnosed with
diabetic (Type 2 Diabetes in India: Challenges and Possible Solutions, 2018).
There are some issues posed by type 2 diabetes mellitus in India like:
High rate of population is covered by urban and rural areas
High range of pre diabetic patients (Beck and et.al., 2016).
Involves high generic and environmental challenges
Generates high prevalence among the public
Low awareness of cure among the population due to lack of education system Rapid increase in the rate of diabetes complications.
Rising Prevalence among youth (Age group between 15-24)
It has been noted that in India, rate of type of diabetes mellitus has common in youth
(Age group between 15-24) of India. The possibilities of diabetes in young age leads high
chances of complications relatively and enhances the severe morbidity in productive year of life.
(As per the Type 2 Diabetes in India: Challenges and Possible Solutions, 2018). In terms of
Obesity related type 2 diabetes which account for a considerable ratio of identified diabetes in
the young age group people. The ratio of this possibilities has been increased nowadays. In order
to that, Government needs to take some measures in order to reduce the obesity in young people.
The main issue is increasing fat level among youth (Age group between 15-24) that are
highly lead to diabetes issues. The reasons due to which this rate has been increased are improper
diet and rate of insulin resistance as well as abnormalities among healthy adolescences due to
which people are gaining overweight and children are becoming obese.
According to International Diabetes federation (IDF), it was estimated that in 2010, five
countries where people at largest are diagnosed with diabetes are India, China, US, Russia and
Brazil. It has also presented that number of people were more influencing and encouraging
towards the better development growth and outcomes due to improper carring of his own health
outcomes. For an example: Smoking is one of the major key drivers of poor health and prior
impermanence which leads to increase health inequalities in between population. It has been
4
Describing Diabetes related outcomes globally and nationally.
Like many other different developing countries, India is also facing some threats in
several communicable diseases due to different lifestyles. As per the current scenario of India, in
next 20 years, India will be on the place where one-fifth population will be diagnosed with
diabetic (Type 2 Diabetes in India: Challenges and Possible Solutions, 2018).
There are some issues posed by type 2 diabetes mellitus in India like:
High rate of population is covered by urban and rural areas
High range of pre diabetic patients (Beck and et.al., 2016).
Involves high generic and environmental challenges
Generates high prevalence among the public
Low awareness of cure among the population due to lack of education system Rapid increase in the rate of diabetes complications.
Rising Prevalence among youth (Age group between 15-24)
It has been noted that in India, rate of type of diabetes mellitus has common in youth
(Age group between 15-24) of India. The possibilities of diabetes in young age leads high
chances of complications relatively and enhances the severe morbidity in productive year of life.
(As per the Type 2 Diabetes in India: Challenges and Possible Solutions, 2018). In terms of
Obesity related type 2 diabetes which account for a considerable ratio of identified diabetes in
the young age group people. The ratio of this possibilities has been increased nowadays. In order
to that, Government needs to take some measures in order to reduce the obesity in young people.
The main issue is increasing fat level among youth (Age group between 15-24) that are
highly lead to diabetes issues. The reasons due to which this rate has been increased are improper
diet and rate of insulin resistance as well as abnormalities among healthy adolescences due to
which people are gaining overweight and children are becoming obese.
According to International Diabetes federation (IDF), it was estimated that in 2010, five
countries where people at largest are diagnosed with diabetes are India, China, US, Russia and
Brazil. It has also presented that number of people were more influencing and encouraging
towards the better development growth and outcomes due to improper carring of his own health
outcomes. For an example: Smoking is one of the major key drivers of poor health and prior
impermanence which leads to increase health inequalities in between population. It has been
4
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
observed that, Public Health England is using the PHOF indicators to monitor progress to reduce
health inequalities in England (Betancourt and et.al., 2016). On the other side, only 3% of Asian
women are smoking.
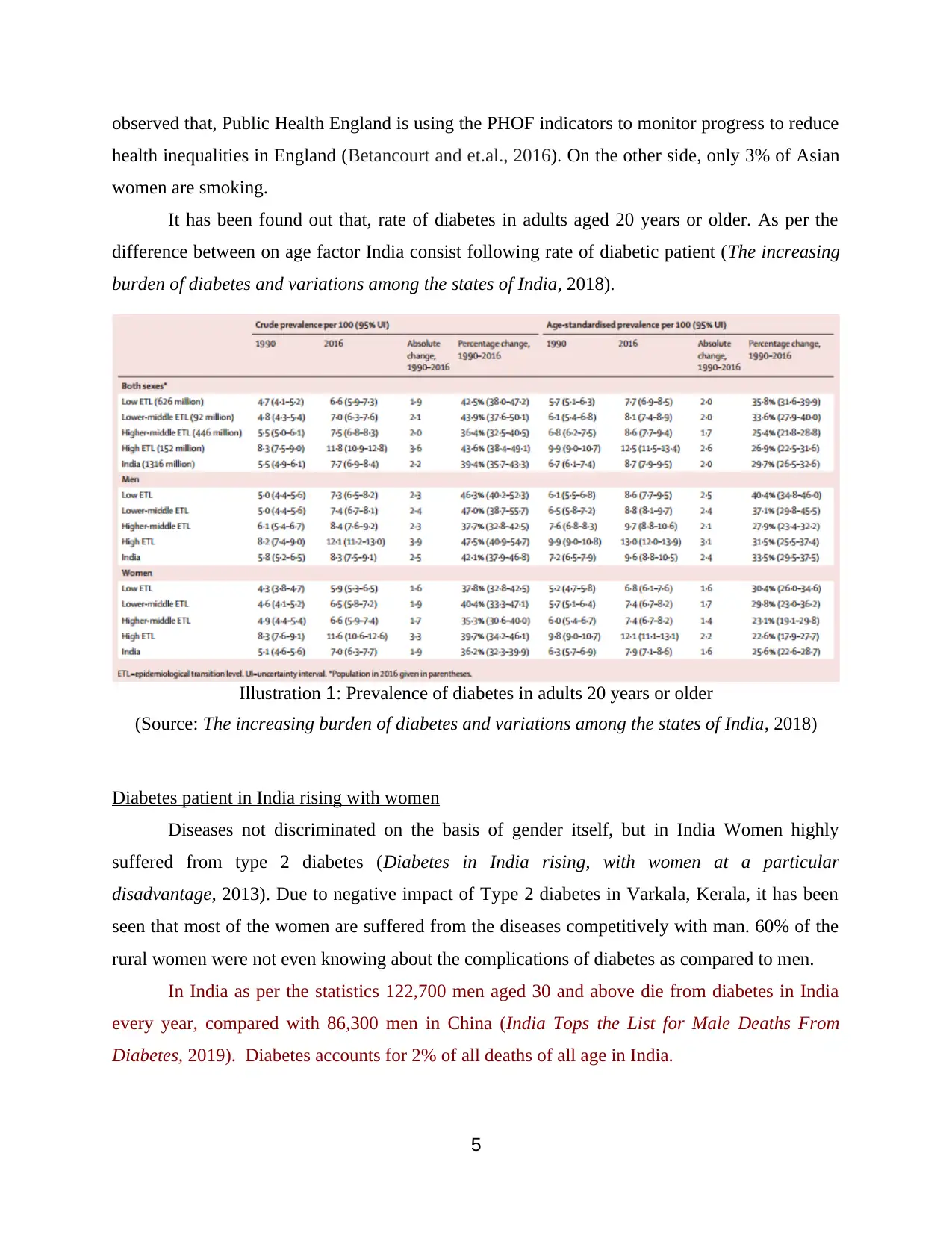
It has been found out that, rate of diabetes in adults aged 20 years or older. As per the
difference between on age factor India consist following rate of diabetic patient (The increasing
burden of diabetes and variations among the states of India, 2018).
Diabetes patient in India rising with women
Diseases not discriminated on the basis of gender itself, but in India Women highly
suffered from type 2 diabetes (Diabetes in India rising, with women at a particular
disadvantage, 2013). Due to negative impact of Type 2 diabetes in Varkala, Kerala, it has been
seen that most of the women are suffered from the diseases competitively with man. 60% of the
rural women were not even knowing about the complications of diabetes as compared to men.
In India as per the statistics 122,700 men aged 30 and above die from diabetes in India
every year, compared with 86,300 men in China (India Tops the List for Male Deaths From
Diabetes, 2019). Diabetes accounts for 2% of all deaths of all age in India.
5
Illustration 1: Prevalence of diabetes in adults 20 years or older
(Source: The increasing burden of diabetes and variations among the states of India, 2018)
health inequalities in England (Betancourt and et.al., 2016). On the other side, only 3% of Asian
women are smoking.
It has been found out that, rate of diabetes in adults aged 20 years or older. As per the
difference between on age factor India consist following rate of diabetic patient (The increasing
burden of diabetes and variations among the states of India, 2018).
Diabetes patient in India rising with women
Diseases not discriminated on the basis of gender itself, but in India Women highly
suffered from type 2 diabetes (Diabetes in India rising, with women at a particular
disadvantage, 2013). Due to negative impact of Type 2 diabetes in Varkala, Kerala, it has been
seen that most of the women are suffered from the diseases competitively with man. 60% of the
rural women were not even knowing about the complications of diabetes as compared to men.
In India as per the statistics 122,700 men aged 30 and above die from diabetes in India
every year, compared with 86,300 men in China (India Tops the List for Male Deaths From
Diabetes, 2019). Diabetes accounts for 2% of all deaths of all age in India.
5
Illustration 1: Prevalence of diabetes in adults 20 years or older
(Source: The increasing burden of diabetes and variations among the states of India, 2018)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Diabetes related Facts at global level
As per the facts of World Health Organisation (WHO), the total number of people risen
by diabetes in 1980s was approx. 108 million and 422 million in 2014.
As per the age consideration, almost half of all deaths are caused due to high blood
glucose involved in or before the age of 70 years. As per WHO, diabetes is taking
seventh position in high leading death in 2016 (World Health Organisation, 2018).
Globally, as per the age factor, diabetes is majorly found in between the age of people 20
and 79 years or others. It has been found that 175 million people have unknown Type 2
diabetes (World Health Organisation, 2018).
SECTION 3: DETERMINANTS WHICH AFFECTS GENDER, SOCIO
ECONOMIC STATUS, AGE, LIFESTYLE AND HEALTH
BEHAVIOUR
In present world non communicable diseases are the most affected cause and disability
across the world (Brown and et.al., 2016). Worldwide, large number of people dying due to
having some incurable diseases due to improper environment, awareness, resources etc. The
most current chronic diseases are connected with some common reasons such as smoking or
unhealthy nutrition, underlying social economy, due to different culture, political environment
determinants and other some interventions as well. These are the influences determinant that
affect the people health issues in different manner (Society, the individual and medicine, 2017).
There are several kinds of determinants that influence human behaviour and there health
outcomes.
Good health is a result factors other than costly health care, although people living in
most wealthy countries to enjoy their life into more efficiently. On the other hand, infant
mortality is the best way to indicate life into more appropriate model. This factor affected by
decreasing the level of income and health spending.
There are some social determinants that affect people socio economic status and health
status as well. These also helps to promoting living factors rather than individual risk. Overall, it
makes the people perspective and ineffective outcomes level. There are some list of determinants
factors that affect people factors (Castañeda and et.al., 2015).
6
As per the facts of World Health Organisation (WHO), the total number of people risen
by diabetes in 1980s was approx. 108 million and 422 million in 2014.
As per the age consideration, almost half of all deaths are caused due to high blood
glucose involved in or before the age of 70 years. As per WHO, diabetes is taking
seventh position in high leading death in 2016 (World Health Organisation, 2018).
Globally, as per the age factor, diabetes is majorly found in between the age of people 20
and 79 years or others. It has been found that 175 million people have unknown Type 2
diabetes (World Health Organisation, 2018).
SECTION 3: DETERMINANTS WHICH AFFECTS GENDER, SOCIO
ECONOMIC STATUS, AGE, LIFESTYLE AND HEALTH
BEHAVIOUR
In present world non communicable diseases are the most affected cause and disability
across the world (Brown and et.al., 2016). Worldwide, large number of people dying due to
having some incurable diseases due to improper environment, awareness, resources etc. The
most current chronic diseases are connected with some common reasons such as smoking or
unhealthy nutrition, underlying social economy, due to different culture, political environment
determinants and other some interventions as well. These are the influences determinant that
affect the people health issues in different manner (Society, the individual and medicine, 2017).
There are several kinds of determinants that influence human behaviour and there health
outcomes.
Good health is a result factors other than costly health care, although people living in
most wealthy countries to enjoy their life into more efficiently. On the other hand, infant
mortality is the best way to indicate life into more appropriate model. This factor affected by
decreasing the level of income and health spending.
There are some social determinants that affect people socio economic status and health
status as well. These also helps to promoting living factors rather than individual risk. Overall, it
makes the people perspective and ineffective outcomes level. There are some list of determinants
factors that affect people factors (Castañeda and et.al., 2015).
6
Socio-economic status as a determinant of health
Socio economic status are the determinants factors which represents the individual rank,
position or esteem in society. It affects the better developing and effective working outcomes.
Socio economic determinants evaluated in terms of income, kind of occupation, education level,
wealth etc. As per the upper class group of people, lower or poor class people majorly suffered
from the diseases and dying due to illness (Eldredge and et.al., 2016).
Inequalities in health occurs in India majorly in rural areas, due to lack of education,
social exclusion, unemployment and low income. All these determinants and factors affect the
people status and health issues, due to which they not enough capable to cope up with their
diseases. It affects majorly the growth of the system and effective working outcomes related to
health (Vanstone and et.al., 2017).
Poverty is the major cause and higher prevalence of several health conditions.
Impoverishment is the main reason behind any uncertain situation happened with the people. On
the other hand, majorly poor people suffered by chronic disease, injury, deprived infant
development, stress, anxiety and depression (Fedeli and et.al., 2018).
It also has been emphasised that, due to income inequality and individual occupation
showing the better development growth for the company development process into more
appropriate manner of growth.
On the other hand, there are some determinants which affect health of an individual and
communities as well. Those determinants includes factors where people live, genetics, income,
relationship with family friends which is considerably affect the individual health. There are
some common determinants which affect the health of the person are given as below:
Social and economic environment.
Physical environment (Green and Thorogood, 2018).
Person individual characteristics and behaviours.
Income and social status: This is another concerning factor that also affect health into
negative manner in case people does not earn that much enough money (Health Impact
Assessment (HIA), 2018). If people are rich and enough capable to afford their medical expenses,
they can easily survive in comparison to those who do not have enough money to afford their
medical bills.
7
Socio economic status are the determinants factors which represents the individual rank,
position or esteem in society. It affects the better developing and effective working outcomes.
Socio economic determinants evaluated in terms of income, kind of occupation, education level,
wealth etc. As per the upper class group of people, lower or poor class people majorly suffered
from the diseases and dying due to illness (Eldredge and et.al., 2016).
Inequalities in health occurs in India majorly in rural areas, due to lack of education,
social exclusion, unemployment and low income. All these determinants and factors affect the
people status and health issues, due to which they not enough capable to cope up with their
diseases. It affects majorly the growth of the system and effective working outcomes related to
health (Vanstone and et.al., 2017).
Poverty is the major cause and higher prevalence of several health conditions.
Impoverishment is the main reason behind any uncertain situation happened with the people. On
the other hand, majorly poor people suffered by chronic disease, injury, deprived infant
development, stress, anxiety and depression (Fedeli and et.al., 2018).
It also has been emphasised that, due to income inequality and individual occupation
showing the better development growth for the company development process into more
appropriate manner of growth.
On the other hand, there are some determinants which affect health of an individual and
communities as well. Those determinants includes factors where people live, genetics, income,
relationship with family friends which is considerably affect the individual health. There are
some common determinants which affect the health of the person are given as below:
Social and economic environment.
Physical environment (Green and Thorogood, 2018).
Person individual characteristics and behaviours.
Income and social status: This is another concerning factor that also affect health into
negative manner in case people does not earn that much enough money (Health Impact
Assessment (HIA), 2018). If people are rich and enough capable to afford their medical expenses,
they can easily survive in comparison to those who do not have enough money to afford their
medical bills.
7
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Education: It is another determinant which affect age, socio economic status and gender
as well as health behaviour of an individual. Likewise, less educated people linked with poor
health as compare to educated people (Nambiar and et.al., 2015).
Physical environment: Healthy environment create more fresh air, purify water, healthy
workplace and clean communities as well as roads. That helps people to keep their respiratory
system balanced and quite well. On the contrary, people who lived around dirt, or villages those
comes directly in the contact of diseases and unhealthy behaviour (Health Impact Assessment
(HIA), 2018).
Social support networks: This is another factor or determinant that affect the health
behaviour and socio economic status of the people (Heckley, Gerdtham and Kjellsson, 2016).
Such as people supported by their families, friends and communities that linked with better
surrounding and lived happy and healthy life. Besides, those people who lived alone and survive
by their own level can affected by unhealthy diseases (Health Impact Assessment (HIA), 2018).
Overall, it has been cleared that different health factor get affected by distinct culture, customs,
and traditions of the family and societies.
Genetics: It is another major determinant that affect social economic status and health
behaviour of an individual person. Due to inheritance is the most helpful to determining the
lifespan, healthiness and likelihood of illness (Health Impact Assessment (HIA), 2018). For an
example, keeping fit and strong, proper diet plan, smoking, drinking all these activities of life
decides the level of health of an individual.
Health Services: This determinant affect where people using the services in access
manner in order to prevent and treat diseases influences health services and growth.
Gender: Men and women suffer from different types of diseases at different kinds of
ages. This is another determinant factor that affect the social economic and health behaviour on
the basis of male and females (Health Impact Assessment (HIA), 2018).
Researcher suggested that diabetes more likely develop in men than woman. It is clearly
found that with men developing type 2 diabetes at a lower BMI than women of similar age.
Another observation, that men grab type 2 diabetes at a higher rate than their female
counterparts. It is worrying that men develop type 2 diabetes at a higher rate than their female
counterparts.
8
as well as health behaviour of an individual. Likewise, less educated people linked with poor
health as compare to educated people (Nambiar and et.al., 2015).
Physical environment: Healthy environment create more fresh air, purify water, healthy
workplace and clean communities as well as roads. That helps people to keep their respiratory
system balanced and quite well. On the contrary, people who lived around dirt, or villages those
comes directly in the contact of diseases and unhealthy behaviour (Health Impact Assessment
(HIA), 2018).
Social support networks: This is another factor or determinant that affect the health
behaviour and socio economic status of the people (Heckley, Gerdtham and Kjellsson, 2016).
Such as people supported by their families, friends and communities that linked with better
surrounding and lived happy and healthy life. Besides, those people who lived alone and survive
by their own level can affected by unhealthy diseases (Health Impact Assessment (HIA), 2018).
Overall, it has been cleared that different health factor get affected by distinct culture, customs,
and traditions of the family and societies.
Genetics: It is another major determinant that affect social economic status and health
behaviour of an individual person. Due to inheritance is the most helpful to determining the
lifespan, healthiness and likelihood of illness (Health Impact Assessment (HIA), 2018). For an
example, keeping fit and strong, proper diet plan, smoking, drinking all these activities of life
decides the level of health of an individual.
Health Services: This determinant affect where people using the services in access
manner in order to prevent and treat diseases influences health services and growth.
Gender: Men and women suffer from different types of diseases at different kinds of
ages. This is another determinant factor that affect the social economic and health behaviour on
the basis of male and females (Health Impact Assessment (HIA), 2018).
Researcher suggested that diabetes more likely develop in men than woman. It is clearly
found that with men developing type 2 diabetes at a lower BMI than women of similar age.
Another observation, that men grab type 2 diabetes at a higher rate than their female
counterparts. It is worrying that men develop type 2 diabetes at a higher rate than their female
counterparts.
8
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Determinant of health
There are so many determinant that affect the individual health system such as transports,
food and agriculture, housing, waste, energy, urbanisations, water, radiation, nutrition and health
etc. these are the determinants affected the people health in different manner. For an example,
Tobacco farming is the most impactful factor that cause heart disease, stroke and certain cancers
etc (Jacklin and et.al., 2017). so these are the another some incurable diseases which might affect
the people health system growth.
On the basis of above discussed following determinants that affect different factors of
human health that affect the human bodies (Barry and et.al., 201). Living a healthy lifestyle is
depends upon the person and it is up to their surroundings as well. Social environmental
determines different factors that affect the health such as gender, age, social networks, family
background etc.
Determinant that affects Health Behaviour
Health behaviour is the big term in this report that affects directly to the individual
physical health. People have both positive and negative health behaviour (Gibson and Segal,
2015). For an example of positive health behaviour are taking yoga, exercises, health regular
check-ups, this is the best way to control the better and behavioural checks and better
advantageous goals (Jayasinghe, 2015). On the other side, Negative behaviour of health involves
high risk, health problem, health impairing etc. these all negative health behaviour has come out
due to having excess use of smoking, drinking, driving too fast, eating junk food etc. all these
reason has increasing the chances of high Diabetes. Determinants that affect health behaviour
including behavioural stages. Behaviour can be identified through several components like,
action, time, target, context etc. On the other hand, it has been seen that higher level of attitudes
are associated with higher level of behaviour in terms of making good impact on the behavioural
goals. Mixed design is refers to evaluate the repeated measures of attitude and behaviour are
measured in a simple of individual (Jacobs-Wingo and et.al., 2016).
SECTION 4: PRESENTING THE POLICY, RESPOND TO GAP
World Health organisation Country office for India mentioned some of the major
implications and process in order to develop the major result goals and effective leading
9
There are so many determinant that affect the individual health system such as transports,
food and agriculture, housing, waste, energy, urbanisations, water, radiation, nutrition and health
etc. these are the determinants affected the people health in different manner. For an example,
Tobacco farming is the most impactful factor that cause heart disease, stroke and certain cancers
etc (Jacklin and et.al., 2017). so these are the another some incurable diseases which might affect
the people health system growth.
On the basis of above discussed following determinants that affect different factors of
human health that affect the human bodies (Barry and et.al., 201). Living a healthy lifestyle is
depends upon the person and it is up to their surroundings as well. Social environmental
determines different factors that affect the health such as gender, age, social networks, family
background etc.
Determinant that affects Health Behaviour
Health behaviour is the big term in this report that affects directly to the individual
physical health. People have both positive and negative health behaviour (Gibson and Segal,
2015). For an example of positive health behaviour are taking yoga, exercises, health regular
check-ups, this is the best way to control the better and behavioural checks and better
advantageous goals (Jayasinghe, 2015). On the other side, Negative behaviour of health involves
high risk, health problem, health impairing etc. these all negative health behaviour has come out
due to having excess use of smoking, drinking, driving too fast, eating junk food etc. all these
reason has increasing the chances of high Diabetes. Determinants that affect health behaviour
including behavioural stages. Behaviour can be identified through several components like,
action, time, target, context etc. On the other hand, it has been seen that higher level of attitudes
are associated with higher level of behaviour in terms of making good impact on the behavioural
goals. Mixed design is refers to evaluate the repeated measures of attitude and behaviour are
measured in a simple of individual (Jacobs-Wingo and et.al., 2016).
SECTION 4: PRESENTING THE POLICY, RESPOND TO GAP
World Health organisation Country office for India mentioned some of the major
implications and process in order to develop the major result goals and effective leading
9
strategies to prevent the inequalities in experience of Type 2 Diabetes in India Adult population
(Meeks and et.al., 2016).
In order to significant, public health challenge diabetes also causes considerable
economic burden on the individual and the family. It also affect the better quality and effective
management task in order to meet out the best developing results in order to sustained the better
health environment and goals (Little and et.al., 2016).
Diabetes is the chronic disease that happened when Pancreas do not produce enough
insulin for the body. Due to which, human body gets some other failure of nerves system and
blood vessels (Nicklett and et.al., 2017).
Health System responses to diabetes in India
Health Care System
India has been fight against National Programme for NCDs in place for the past few
years. The need of good policy is required to making better task and development goals in order
to meet out the best productive outcomes and goals (Subica and et.al., 2017). This is the reason
for National Health Policy, which intends to reduce premature mortality from cardiovascular
diseases, cancer, diabetes or chronic respiratory diseases by 25% by 2025 (Diabetes Scale up
Prevention, strengthen care and enhance surveillance. 2016).
In order to prevent the inequalities growth or to control the Cancer, Diabetes,
Cardiovascular Disease and stroke (NPCDCS). India initiated the National Programme in 2010,
which covered by approx. 350 districts of the country. In all the district level, NCD clinics
recommended to deal with every patient with one attending community health centres, In order
to meet out the basic requirements of the people and effective working outcomes as well. (Subica
and et.al., 2017). That time, private hospitals are the predominant source of treatment with
government entities.
All resources should be used in an appropriate manner. People should have sustainable
health and financial resources in order to access the basic diagnostics essential medicines and
machines. All certain cells and health care centres are proactive, should be patient centred and
sustainable in order to evaluate the better task oriented task and better result outcomes (The
increasing burden of diabetes and variations among the states of India, 2018).
Quality of Care
10
(Meeks and et.al., 2016).
In order to significant, public health challenge diabetes also causes considerable
economic burden on the individual and the family. It also affect the better quality and effective
management task in order to meet out the best developing results in order to sustained the better
health environment and goals (Little and et.al., 2016).
Diabetes is the chronic disease that happened when Pancreas do not produce enough
insulin for the body. Due to which, human body gets some other failure of nerves system and
blood vessels (Nicklett and et.al., 2017).
Health System responses to diabetes in India
Health Care System
India has been fight against National Programme for NCDs in place for the past few
years. The need of good policy is required to making better task and development goals in order
to meet out the best productive outcomes and goals (Subica and et.al., 2017). This is the reason
for National Health Policy, which intends to reduce premature mortality from cardiovascular
diseases, cancer, diabetes or chronic respiratory diseases by 25% by 2025 (Diabetes Scale up
Prevention, strengthen care and enhance surveillance. 2016).
In order to prevent the inequalities growth or to control the Cancer, Diabetes,
Cardiovascular Disease and stroke (NPCDCS). India initiated the National Programme in 2010,
which covered by approx. 350 districts of the country. In all the district level, NCD clinics
recommended to deal with every patient with one attending community health centres, In order
to meet out the basic requirements of the people and effective working outcomes as well. (Subica
and et.al., 2017). That time, private hospitals are the predominant source of treatment with
government entities.
All resources should be used in an appropriate manner. People should have sustainable
health and financial resources in order to access the basic diagnostics essential medicines and
machines. All certain cells and health care centres are proactive, should be patient centred and
sustainable in order to evaluate the better task oriented task and better result outcomes (The
increasing burden of diabetes and variations among the states of India, 2018).
Quality of Care
10
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 18
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.