Comprehensive Nursing Care Report: Managing Type 2 Diabetes Mellitus
VerifiedAdded on 2022/01/08
|13
|3156
|74
Report
AI Summary
This report provides a comprehensive overview of nursing care for Type 2 Diabetes Mellitus (T2DM), detailing the pathophysiology, risk factors, and management strategies. It includes an analysis of a patient case study, highlighting the genetic and environmental factors contributing to the development of T2DM, such as insulin resistance and impaired insulin secretion. The report discusses various treatment options, including lifestyle modifications (diet and exercise), pharmacological interventions (Metformin and Glipizide), and non-pharmacological interventions (stress management). It also compares Type 1 and Type 2 diabetes, examines the reasons for high blood glucose levels (BGL) in the patient, and evaluates the effectiveness of different medications and diagnostic tests like HbA1c and BGL tests in managing T2DM. The report concludes by emphasizing the importance of personalized care and continuous monitoring in diabetes management.

Running head: NURSING CARE DIABETES
Nursing Care Diabetes
Name of the Student
Name of the University
Author Note
Nursing Care Diabetes
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
NURSING CARE DIABETES
Part 1
Answer 1
Diabetes is defined as a group of metabolic disorder which is characterised by severe
hyperglycaemic conditions resulting from lack of proper functioning of insulin hormone.
Type 2 diabetes mellitus (T2DM) results from the combination of genetic factors associated
with impaired secretion of insulin hormone from the beta cells of pancreas and environmental
factors like obesity, lack of proper physical exercise, over-eating, increased level of stress and
aging (Kahn, Cooper & Del Prato, 2014). In the case study, both the genetic and the
environmental factors found significance behind the diabetes development. As per the case
study, both the mother and older sister of the patient were diagnosed with T2DM during their
early 50s. This presence of genetic history of T2DM makes patient genetically pre-disposed
to T2DM. Case study further highlighted that patient is over-weight (105 kilogram, normal
weight for 167 cm woman is 70 kilogram maximum) (Hall, 2015). She also has no significant
physical activity due to pain in the joint area arising out of Baker’s cyst and is lately passing
through over-eating due to over-consumption of ice-creams in order to manage stress. Thus it
can be said that the environmental factors are also pronounced in the patient, which lead to
the development of T2DM. The main pathophysiology underlying the development of T2DM
is development of insulin resistance and impaired insulin secretion.
NURSING CARE DIABETES
Part 1
Answer 1
Diabetes is defined as a group of metabolic disorder which is characterised by severe
hyperglycaemic conditions resulting from lack of proper functioning of insulin hormone.
Type 2 diabetes mellitus (T2DM) results from the combination of genetic factors associated
with impaired secretion of insulin hormone from the beta cells of pancreas and environmental
factors like obesity, lack of proper physical exercise, over-eating, increased level of stress and
aging (Kahn, Cooper & Del Prato, 2014). In the case study, both the genetic and the
environmental factors found significance behind the diabetes development. As per the case
study, both the mother and older sister of the patient were diagnosed with T2DM during their
early 50s. This presence of genetic history of T2DM makes patient genetically pre-disposed
to T2DM. Case study further highlighted that patient is over-weight (105 kilogram, normal
weight for 167 cm woman is 70 kilogram maximum) (Hall, 2015). She also has no significant
physical activity due to pain in the joint area arising out of Baker’s cyst and is lately passing
through over-eating due to over-consumption of ice-creams in order to manage stress. Thus it
can be said that the environmental factors are also pronounced in the patient, which lead to
the development of T2DM. The main pathophysiology underlying the development of T2DM
is development of insulin resistance and impaired insulin secretion.
2
NURSING CARE DIABETES
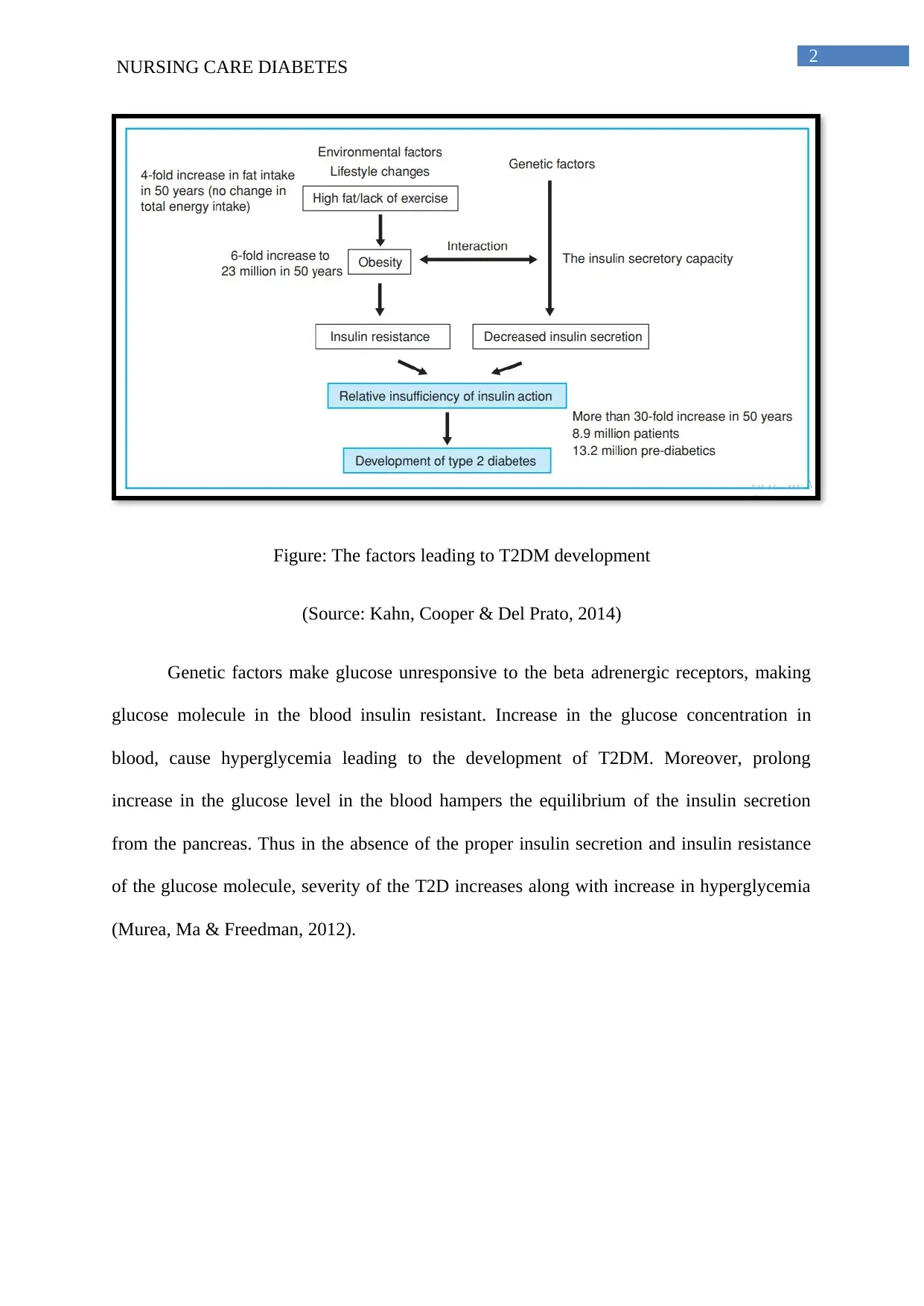
Figure: The factors leading to T2DM development
(Source: Kahn, Cooper & Del Prato, 2014)
Genetic factors make glucose unresponsive to the beta adrenergic receptors, making
glucose molecule in the blood insulin resistant. Increase in the glucose concentration in
blood, cause hyperglycemia leading to the development of T2DM. Moreover, prolong
increase in the glucose level in the blood hampers the equilibrium of the insulin secretion
from the pancreas. Thus in the absence of the proper insulin secretion and insulin resistance
of the glucose molecule, severity of the T2D increases along with increase in hyperglycemia
(Murea, Ma & Freedman, 2012).
NURSING CARE DIABETES
Figure: The factors leading to T2DM development
(Source: Kahn, Cooper & Del Prato, 2014)
Genetic factors make glucose unresponsive to the beta adrenergic receptors, making
glucose molecule in the blood insulin resistant. Increase in the glucose concentration in
blood, cause hyperglycemia leading to the development of T2DM. Moreover, prolong
increase in the glucose level in the blood hampers the equilibrium of the insulin secretion
from the pancreas. Thus in the absence of the proper insulin secretion and insulin resistance
of the glucose molecule, severity of the T2D increases along with increase in hyperglycemia
(Murea, Ma & Freedman, 2012).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

3
NURSING CARE DIABETES
Figure: Pathophysiology and progression of T2DM
(Source: Kahn, Cooper & Del Prato, 2014)
Apart from hyperglycemia, the possible complications arising out of T2DM include
diabetic retinopathy which results loss of vision, foot complications known as diabetic foot
disease, difficulty in wound healing, increase in blood pressure level, increased tendency of
developing cardiovascular disease (Ozougwu et al., 2013). Patient has high level of blood
glucose which is evident from her 22.9 mmol/L of BGL and HbA1c: 11%. The increase
threats of cardiovascular disease is evident from high blood pressure (140/80 mmHg) and
moderately high respiratory rate (22 breaths/minute) (Hall, 2015).
The main treatment options for the management of T2DM include effective lifestyle
modifications along with effective use of pharmacological interventions and non-
pharmacological interventions (Kahn, Cooper & Del Prato, 2014).
NURSING CARE DIABETES
Figure: Pathophysiology and progression of T2DM
(Source: Kahn, Cooper & Del Prato, 2014)
Apart from hyperglycemia, the possible complications arising out of T2DM include
diabetic retinopathy which results loss of vision, foot complications known as diabetic foot
disease, difficulty in wound healing, increase in blood pressure level, increased tendency of
developing cardiovascular disease (Ozougwu et al., 2013). Patient has high level of blood
glucose which is evident from her 22.9 mmol/L of BGL and HbA1c: 11%. The increase
threats of cardiovascular disease is evident from high blood pressure (140/80 mmHg) and
moderately high respiratory rate (22 breaths/minute) (Hall, 2015).
The main treatment options for the management of T2DM include effective lifestyle
modifications along with effective use of pharmacological interventions and non-
pharmacological interventions (Kahn, Cooper & Del Prato, 2014).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
NURSING CARE DIABETES
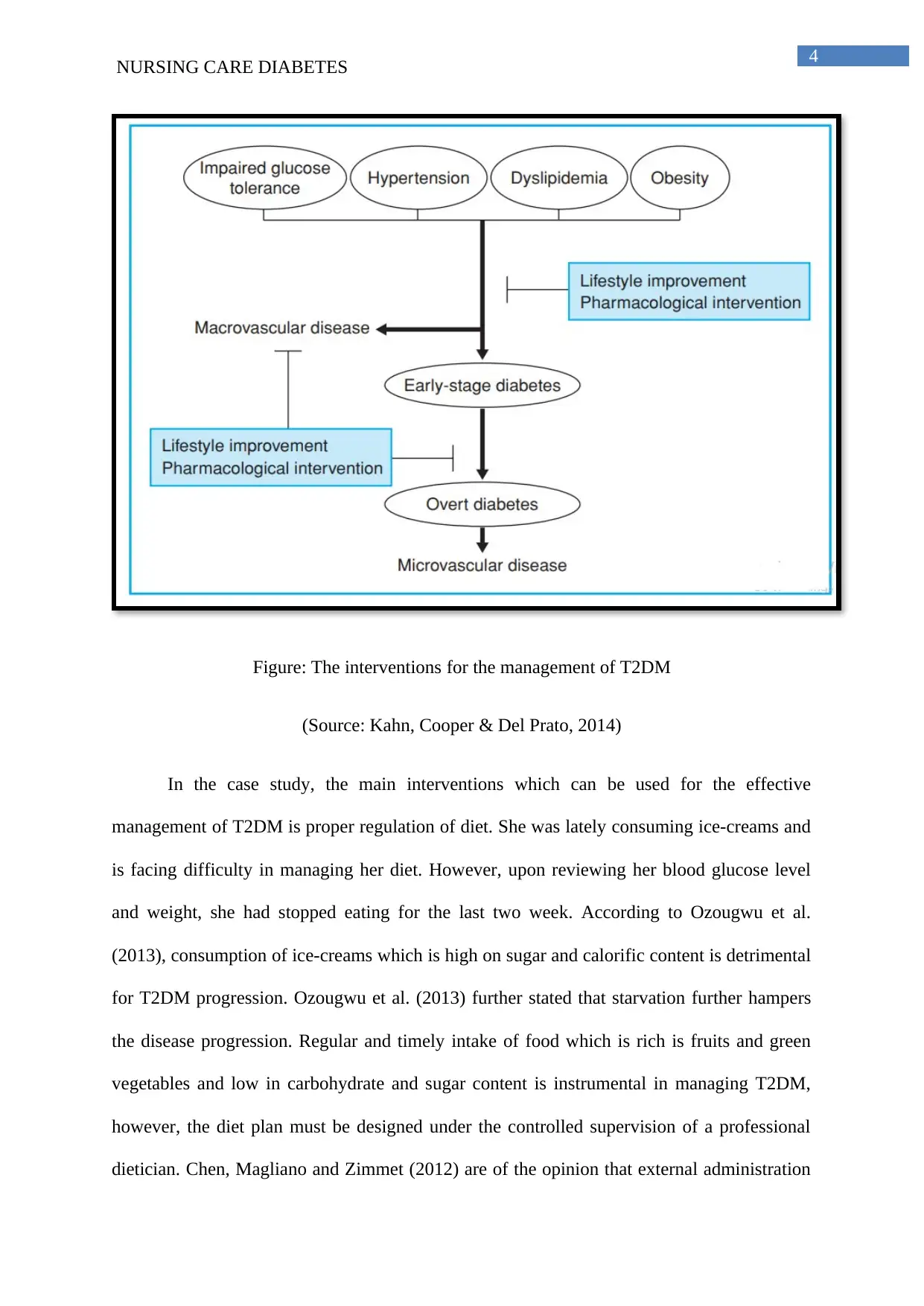
Figure: The interventions for the management of T2DM
(Source: Kahn, Cooper & Del Prato, 2014)
In the case study, the main interventions which can be used for the effective
management of T2DM is proper regulation of diet. She was lately consuming ice-creams and
is facing difficulty in managing her diet. However, upon reviewing her blood glucose level
and weight, she had stopped eating for the last two week. According to Ozougwu et al.
(2013), consumption of ice-creams which is high on sugar and calorific content is detrimental
for T2DM progression. Ozougwu et al. (2013) further stated that starvation further hampers
the disease progression. Regular and timely intake of food which is rich is fruits and green
vegetables and low in carbohydrate and sugar content is instrumental in managing T2DM,
however, the diet plan must be designed under the controlled supervision of a professional
dietician. Chen, Magliano and Zimmet (2012) are of the opinion that external administration
NURSING CARE DIABETES
Figure: The interventions for the management of T2DM
(Source: Kahn, Cooper & Del Prato, 2014)
In the case study, the main interventions which can be used for the effective
management of T2DM is proper regulation of diet. She was lately consuming ice-creams and
is facing difficulty in managing her diet. However, upon reviewing her blood glucose level
and weight, she had stopped eating for the last two week. According to Ozougwu et al.
(2013), consumption of ice-creams which is high on sugar and calorific content is detrimental
for T2DM progression. Ozougwu et al. (2013) further stated that starvation further hampers
the disease progression. Regular and timely intake of food which is rich is fruits and green
vegetables and low in carbohydrate and sugar content is instrumental in managing T2DM,
however, the diet plan must be designed under the controlled supervision of a professional
dietician. Chen, Magliano and Zimmet (2012) are of the opinion that external administration
5
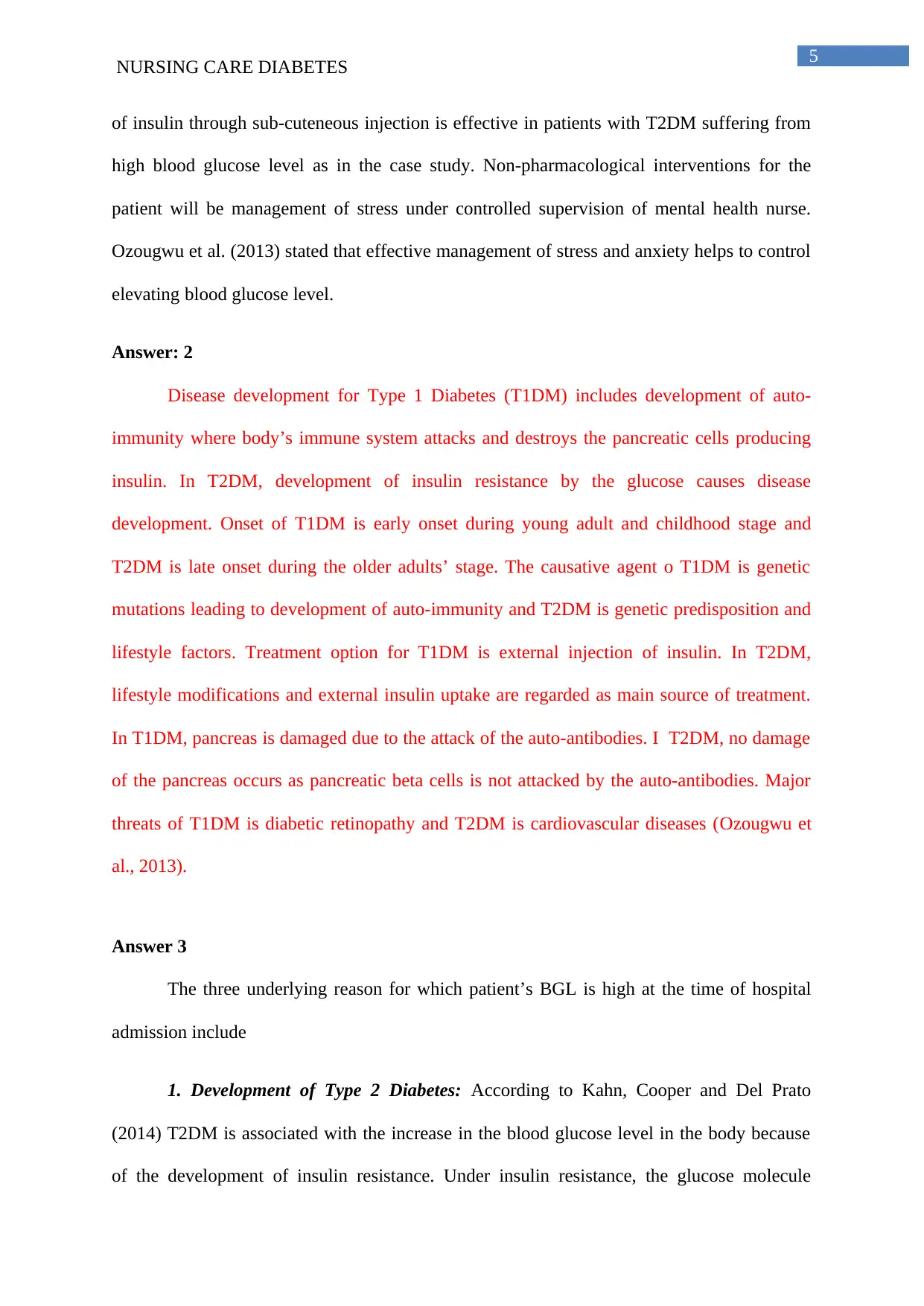
NURSING CARE DIABETES
of insulin through sub-cuteneous injection is effective in patients with T2DM suffering from
high blood glucose level as in the case study. Non-pharmacological interventions for the
patient will be management of stress under controlled supervision of mental health nurse.
Ozougwu et al. (2013) stated that effective management of stress and anxiety helps to control
elevating blood glucose level.
Answer: 2
Disease development for Type 1 Diabetes (T1DM) includes development of auto-
immunity where body’s immune system attacks and destroys the pancreatic cells producing
insulin. In T2DM, development of insulin resistance by the glucose causes disease
development. Onset of T1DM is early onset during young adult and childhood stage and
T2DM is late onset during the older adults’ stage. The causative agent o T1DM is genetic
mutations leading to development of auto-immunity and T2DM is genetic predisposition and
lifestyle factors. Treatment option for T1DM is external injection of insulin. In T2DM,
lifestyle modifications and external insulin uptake are regarded as main source of treatment.
In T1DM, pancreas is damaged due to the attack of the auto-antibodies. I T2DM, no damage
of the pancreas occurs as pancreatic beta cells is not attacked by the auto-antibodies. Major
threats of T1DM is diabetic retinopathy and T2DM is cardiovascular diseases (Ozougwu et
al., 2013).
Answer 3
The three underlying reason for which patient’s BGL is high at the time of hospital
admission include
1. Development of Type 2 Diabetes: According to Kahn, Cooper and Del Prato
(2014) T2DM is associated with the increase in the blood glucose level in the body because
of the development of insulin resistance. Under insulin resistance, the glucose molecule
NURSING CARE DIABETES
of insulin through sub-cuteneous injection is effective in patients with T2DM suffering from
high blood glucose level as in the case study. Non-pharmacological interventions for the
patient will be management of stress under controlled supervision of mental health nurse.
Ozougwu et al. (2013) stated that effective management of stress and anxiety helps to control
elevating blood glucose level.
Answer: 2
Disease development for Type 1 Diabetes (T1DM) includes development of auto-
immunity where body’s immune system attacks and destroys the pancreatic cells producing
insulin. In T2DM, development of insulin resistance by the glucose causes disease
development. Onset of T1DM is early onset during young adult and childhood stage and
T2DM is late onset during the older adults’ stage. The causative agent o T1DM is genetic
mutations leading to development of auto-immunity and T2DM is genetic predisposition and
lifestyle factors. Treatment option for T1DM is external injection of insulin. In T2DM,
lifestyle modifications and external insulin uptake are regarded as main source of treatment.
In T1DM, pancreas is damaged due to the attack of the auto-antibodies. I T2DM, no damage
of the pancreas occurs as pancreatic beta cells is not attacked by the auto-antibodies. Major
threats of T1DM is diabetic retinopathy and T2DM is cardiovascular diseases (Ozougwu et
al., 2013).
Answer 3
The three underlying reason for which patient’s BGL is high at the time of hospital
admission include
1. Development of Type 2 Diabetes: According to Kahn, Cooper and Del Prato
(2014) T2DM is associated with the increase in the blood glucose level in the body because
of the development of insulin resistance. Under insulin resistance, the glucose molecule
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
NURSING CARE DIABETES
present in the blood fail to respond to the insulin hormone due to inability to bind with the
insulin receptors (adnergic receptors) leading to high blood glucose level (BGL). Kahn,
Cooper and Del Prato (2014) stated that unmanaged T2DM like lack of proper medication
further increase BGL. The patient takes no specific medications for T2DM management and
this further heightened the BGL.
2. Poor lifestyle habits: Murea, Ma and Freedman (2012) are of the opinion that one
of the sole parameters for the management of BGL in case of T2DM is effective management
of the lifestyles. Under lifestyle management, the first preference is given to diet plan.
Patient’s physicians also advised her to “watch” what she eats. However, due to her mood
fluctuations she use to consume ice-creams which might have increased her BGL. Murea, Ma
and Freedman (2012) stated that ice-creams are high calorie food which scores high on
calorific value of glucose content. Due to the development of Baker’s Cyst, the patient in the
case study was unable to perform regular exercise, the sedentary lifestyle promoted a rise in
BGL.
3. High level of stress: Asmat, Abad and Ismail (2016) stated that the majority of the
depressed patients are sickened from diabetes-specific emotional stress. The consequences of
stress hamper the endocrine system bringing change in the glucose metabolism process and
insulin resistance and thereby causing hyperglycemia. Stress increases the secretion of
dopamine catecholamine neurotransmitter and its sustained stimulation leads to
hyperglycemia. In the case study, the patient was suffering from anxiety and stress due to her
impending surgery for Baker’s cyst and weight gain. The stress and anxiety factor lead to
high BGL.
NURSING CARE DIABETES
present in the blood fail to respond to the insulin hormone due to inability to bind with the
insulin receptors (adnergic receptors) leading to high blood glucose level (BGL). Kahn,
Cooper and Del Prato (2014) stated that unmanaged T2DM like lack of proper medication
further increase BGL. The patient takes no specific medications for T2DM management and
this further heightened the BGL.
2. Poor lifestyle habits: Murea, Ma and Freedman (2012) are of the opinion that one
of the sole parameters for the management of BGL in case of T2DM is effective management
of the lifestyles. Under lifestyle management, the first preference is given to diet plan.
Patient’s physicians also advised her to “watch” what she eats. However, due to her mood
fluctuations she use to consume ice-creams which might have increased her BGL. Murea, Ma
and Freedman (2012) stated that ice-creams are high calorie food which scores high on
calorific value of glucose content. Due to the development of Baker’s Cyst, the patient in the
case study was unable to perform regular exercise, the sedentary lifestyle promoted a rise in
BGL.
3. High level of stress: Asmat, Abad and Ismail (2016) stated that the majority of the
depressed patients are sickened from diabetes-specific emotional stress. The consequences of
stress hamper the endocrine system bringing change in the glucose metabolism process and
insulin resistance and thereby causing hyperglycemia. Stress increases the secretion of
dopamine catecholamine neurotransmitter and its sustained stimulation leads to
hyperglycemia. In the case study, the patient was suffering from anxiety and stress due to her
impending surgery for Baker’s cyst and weight gain. The stress and anxiety factor lead to
high BGL.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
NURSING CARE DIABETES
Part 2
Answer: 1
Cortisone injections (Kenacort-A 40)
According to Frush and Noyes (2015), injection of corticosteroid (cortisone) directly
into the joint or the soft tissue liming next to the painful joint which is also known as bursa
helps in the reduction of inflammation and to provide pain relief. The reduction in the pain
relief helps in the effective implementation of the successful physical therapy. Frush and
Noyes (2015) are of the opinion that cyst aspiration done with corticosteroid injection helps
to get effective pain relief and reduction in the cyst volume of patients suffering from Baker’s
cyst and concomitant knee osteoarthritis. However, the use of corticosteroid is associated
with numerous complications. Frush and Noyes (2015) stated that prolong injection with
corticosteroid like cortisone leads to crystallization of the cortisone inside the body. The
crystalline cortisone gets deposited in the joints thus negatively acting on knee pain. It also
caused elevation in the blood glucose level. Increase in the BGL is detrimental for her as she
is suffering from T2DM and has high blood pressure.
Metformin (APO-Metformin Tabs)
According to Huang, Castelino and Peterson (2014), metformin is an extended release
table that is used as an oral antihyperglycemic drug for the management of T2DM.
Metformin improve the glucose tolerance of patient’s with T2DM by lowering both the
postprandial plasma glucose concentration and basal glucose concentration. Metformin
mainly decreases the production of glucose from the hepatic cells along with decrease in the
intestinal absorption of glucose. This activity helps in the improvement of insulin sensitivity
through increase in the peripheral glucose uptake and utilization and thereby helping to
reduce BGL. Under metformin medication, the insulin secretion remains unchanged but the
NURSING CARE DIABETES
Part 2
Answer: 1
Cortisone injections (Kenacort-A 40)
According to Frush and Noyes (2015), injection of corticosteroid (cortisone) directly
into the joint or the soft tissue liming next to the painful joint which is also known as bursa
helps in the reduction of inflammation and to provide pain relief. The reduction in the pain
relief helps in the effective implementation of the successful physical therapy. Frush and
Noyes (2015) are of the opinion that cyst aspiration done with corticosteroid injection helps
to get effective pain relief and reduction in the cyst volume of patients suffering from Baker’s
cyst and concomitant knee osteoarthritis. However, the use of corticosteroid is associated
with numerous complications. Frush and Noyes (2015) stated that prolong injection with
corticosteroid like cortisone leads to crystallization of the cortisone inside the body. The
crystalline cortisone gets deposited in the joints thus negatively acting on knee pain. It also
caused elevation in the blood glucose level. Increase in the BGL is detrimental for her as she
is suffering from T2DM and has high blood pressure.
Metformin (APO-Metformin Tabs)
According to Huang, Castelino and Peterson (2014), metformin is an extended release
table that is used as an oral antihyperglycemic drug for the management of T2DM.
Metformin improve the glucose tolerance of patient’s with T2DM by lowering both the
postprandial plasma glucose concentration and basal glucose concentration. Metformin
mainly decreases the production of glucose from the hepatic cells along with decrease in the
intestinal absorption of glucose. This activity helps in the improvement of insulin sensitivity
through increase in the peripheral glucose uptake and utilization and thereby helping to
reduce BGL. Under metformin medication, the insulin secretion remains unchanged but the
8
NURSING CARE DIABETES
fasting insulin conditions and the day-long plasma insulin response might decrease gradually.
However, Huang, Castelino and Peterson (2014) highlighted that prolong use of metformin
for a considerable period of time leads to the generation of physical weakness and muscle
pain. The weakness and pain might be debilitating for the patient as it might hamper her
healthy living and quality of life making per unable to perform mild to moderate physical
activity. Other side-effects of metformin include sudden lowering of the blood glucose level
and thus glucose level must be monitored and the adjustment of the dosage must be done
accordingly. Metformin also includes constipation, bloating and abdominal distention. Ng et
al. (2014) are of the opinion that long-term use of metformin cause cognitive decline among
the older adults.
Glipizide
Glipizide is used along with regular physical activity and proper diet plan in order to
control the high blood sugar level of people who are suffering from type 2 diabetes mellitus.
The side-effects of Glupizide includes nausea, loss of appetite, vomiting, diarrhea, stomach
upset, constipation, instant gain in weight and headache. Gain in weight can generate serious
health issues, as she is already obese. Thus in order to get quality results from Glipizide use,
effective management of the diet plan and physical activity is important (Hong et al., 2013).
Answer 2
HbA1c test
HbA1c is used to test the presence of glycated haemoglobin and thereby helping to an
overview of the level of glucose molecule in the blood that is present in a bounded form with
the red blood cells. HbA1c test is mainly helpful in getting a brief overview of the level of
blood sugar for the last 2 to 3 months as the average life expectancy of RBC is 3 months.
High blood glucose level indicates high HbA1c test results. The normal range of HbA1c test
NURSING CARE DIABETES
fasting insulin conditions and the day-long plasma insulin response might decrease gradually.
However, Huang, Castelino and Peterson (2014) highlighted that prolong use of metformin
for a considerable period of time leads to the generation of physical weakness and muscle
pain. The weakness and pain might be debilitating for the patient as it might hamper her
healthy living and quality of life making per unable to perform mild to moderate physical
activity. Other side-effects of metformin include sudden lowering of the blood glucose level
and thus glucose level must be monitored and the adjustment of the dosage must be done
accordingly. Metformin also includes constipation, bloating and abdominal distention. Ng et
al. (2014) are of the opinion that long-term use of metformin cause cognitive decline among
the older adults.
Glipizide
Glipizide is used along with regular physical activity and proper diet plan in order to
control the high blood sugar level of people who are suffering from type 2 diabetes mellitus.
The side-effects of Glupizide includes nausea, loss of appetite, vomiting, diarrhea, stomach
upset, constipation, instant gain in weight and headache. Gain in weight can generate serious
health issues, as she is already obese. Thus in order to get quality results from Glipizide use,
effective management of the diet plan and physical activity is important (Hong et al., 2013).
Answer 2
HbA1c test
HbA1c is used to test the presence of glycated haemoglobin and thereby helping to an
overview of the level of glucose molecule in the blood that is present in a bounded form with
the red blood cells. HbA1c test is mainly helpful in getting a brief overview of the level of
blood sugar for the last 2 to 3 months as the average life expectancy of RBC is 3 months.
High blood glucose level indicates high HbA1c test results. The normal range of HbA1c test
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
NURSING CARE DIABETES
is between 4% to 5.6%. HbA1c level within 5.7% and 6.4 % indicates higher chances of
developing diabetes and levels higher than 6.5% indicates diabetes (Gailliot & Baumeister,
2018).
BGL test
It is used to get an instant overview of the blood sugar level and thus also known as
random blood glucose test. It can be done through the use of glucometer. The normal blood
glucose level range, during fasting condition was in between 4.0 to 5.4 mmol/L (72 to 99
mg/dL. When BGL is done after meal, the normal range is up to 7.8 mmol/L (140 mg/dL)
(Gailliot & Baumeister, 2018).
The blood test report after the administration of Metformin and Glipizide is BGL
8.8/L; HbA1c:8%. This indicates the blood glucose level though under the diabetic band in
comparison to the normal units, the blood glucose level has decreased significantly from the
previous instances (blood glucose level (BGL) was 22.9 mmol/L; HbA1c: 11%) during the
fasting condition. the main reason behind the decrease in the BGL is administration of anti-
hyperglycemic medications.
Answer 3
Generally T2DM is referred as insulin independent diabetes mellitus and T1DM is
regarded as insulin independent. However, at present such classifications do not hold
prominent patho-physiological significance as T2DM are at times insulin dependent.
Moreover, the concept of early and late onset in diabetes mellitus is also extinct. Previously
T2DM is classified as mature onset and T1DM is classified as early onset. However, the
survey conducted by Dabelea et al. (2014) highlighted that unhealthy lifestyle among the
young adults and the children have increased the tendency of developing T2DM. The
unhealthy lifestyles that have prompted the development of T2DM among the children and
NURSING CARE DIABETES
is between 4% to 5.6%. HbA1c level within 5.7% and 6.4 % indicates higher chances of
developing diabetes and levels higher than 6.5% indicates diabetes (Gailliot & Baumeister,
2018).
BGL test
It is used to get an instant overview of the blood sugar level and thus also known as
random blood glucose test. It can be done through the use of glucometer. The normal blood
glucose level range, during fasting condition was in between 4.0 to 5.4 mmol/L (72 to 99
mg/dL. When BGL is done after meal, the normal range is up to 7.8 mmol/L (140 mg/dL)
(Gailliot & Baumeister, 2018).
The blood test report after the administration of Metformin and Glipizide is BGL
8.8/L; HbA1c:8%. This indicates the blood glucose level though under the diabetic band in
comparison to the normal units, the blood glucose level has decreased significantly from the
previous instances (blood glucose level (BGL) was 22.9 mmol/L; HbA1c: 11%) during the
fasting condition. the main reason behind the decrease in the BGL is administration of anti-
hyperglycemic medications.
Answer 3
Generally T2DM is referred as insulin independent diabetes mellitus and T1DM is
regarded as insulin independent. However, at present such classifications do not hold
prominent patho-physiological significance as T2DM are at times insulin dependent.
Moreover, the concept of early and late onset in diabetes mellitus is also extinct. Previously
T2DM is classified as mature onset and T1DM is classified as early onset. However, the
survey conducted by Dabelea et al. (2014) highlighted that unhealthy lifestyle among the
young adults and the children have increased the tendency of developing T2DM. The
unhealthy lifestyles that have prompted the development of T2DM among the children and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
NURSING CARE DIABETES
the young adults include higher consumption of junk food, early onset of smoking, drinking,
and sedentary lifestyle.
Answer 4
Teach-back method is a way to confirm the level of understanding of the service users
in their own words. This method generates an opportunity for effective communication with
the healthcare professionals (Tamura-Lis, 2013). Tamura-Lis (2013) are of the opinion that it
is helpful to use written/visual material to reinforce the teaching points in order to improve
the service users level of satisfaction and understanding.
Under teach back method, I will introduce working principle of BGL machine and
will demonstrate a live manual regarding how to use the machine. After demonstrating the
entire action, I will ask the patient to give her overview regarding why she things the use of
BGL machine is important for her T2DM management. Then I will ask her to provide a
demonstration of the machine usage. If I find that she is unable to use the machine, I will
again help her with the process of usage. If the patient is scared of the pain about the sudden
pricking of the thumb then I will help her to overcome this phobia. Repeating the information
will help to close the gap in understanding. I will again ask her to repeat the process and will
indulge in effective patient-centred communication to iron out any additional confusion or
query regarding the machine usage.
NURSING CARE DIABETES
the young adults include higher consumption of junk food, early onset of smoking, drinking,
and sedentary lifestyle.
Answer 4
Teach-back method is a way to confirm the level of understanding of the service users
in their own words. This method generates an opportunity for effective communication with
the healthcare professionals (Tamura-Lis, 2013). Tamura-Lis (2013) are of the opinion that it
is helpful to use written/visual material to reinforce the teaching points in order to improve
the service users level of satisfaction and understanding.
Under teach back method, I will introduce working principle of BGL machine and
will demonstrate a live manual regarding how to use the machine. After demonstrating the
entire action, I will ask the patient to give her overview regarding why she things the use of
BGL machine is important for her T2DM management. Then I will ask her to provide a
demonstration of the machine usage. If I find that she is unable to use the machine, I will
again help her with the process of usage. If the patient is scared of the pain about the sudden
pricking of the thumb then I will help her to overcome this phobia. Repeating the information
will help to close the gap in understanding. I will again ask her to repeat the process and will
indulge in effective patient-centred communication to iron out any additional confusion or
query regarding the machine usage.
11
NURSING CARE DIABETES
References
Asmat, U., Abad, K., & Ismail, K. (2016). Diabetes mellitus and oxidative stress—a concise
review. Saudi Pharmaceutical Journal, 24(5), 547-553..
Chen, L., Magliano, D. J., & Zimmet, P. Z. (2012). The worldwide epidemiology of type 2
diabetes mellitus—present and future perspectives. Nature reviews
endocrinology, 8(4), 228.
Dabelea, D., Mayer-Davis, E. J., Saydah, S., Imperatore, G., Linder, B., Divers, J., ... &
Liese, A. D. (2014). Prevalence of type 1 and type 2 diabetes among children and
adolescents from 2001 to 2009. Jama, 311(17), 1778-1786.
Frush, T. J., & Noyes, F. R. (2015). Baker’s cyst: diagnostic and surgical
considerations. Sports health, 7(4), 359-365.
Gailliot, M. T., & Baumeister, R. F. (2018). The physiology of willpower: Linking blood
glucose to self-control. In Self-Regulation and Self-Control (pp. 137-180). Routledge
Hall, J. E. (2015). Guyton and Hall textbook of medical physiology e-Book. Elsevier Health
Sciences.
Hong, J., Zhang, Y., Lai, S., Lv, A., Su, Q., Dong, Y., ... & Zou, D. (2013). Effects of
metformin versus glipizide on cardiovascular outcomes in patients with type 2
diabetes and coronary artery disease. Diabetes care, 36(5), 1304-1311.
Huang, W., Castelino, R. L., & Peterson, G. M. (2014). Metformin usage in type 2 diabetes
mellitus: are safety guidelines adhered to?. Internal medicine journal, 44(3), 266-272.
NURSING CARE DIABETES
References
Asmat, U., Abad, K., & Ismail, K. (2016). Diabetes mellitus and oxidative stress—a concise
review. Saudi Pharmaceutical Journal, 24(5), 547-553..
Chen, L., Magliano, D. J., & Zimmet, P. Z. (2012). The worldwide epidemiology of type 2
diabetes mellitus—present and future perspectives. Nature reviews
endocrinology, 8(4), 228.
Dabelea, D., Mayer-Davis, E. J., Saydah, S., Imperatore, G., Linder, B., Divers, J., ... &
Liese, A. D. (2014). Prevalence of type 1 and type 2 diabetes among children and
adolescents from 2001 to 2009. Jama, 311(17), 1778-1786.
Frush, T. J., & Noyes, F. R. (2015). Baker’s cyst: diagnostic and surgical
considerations. Sports health, 7(4), 359-365.
Gailliot, M. T., & Baumeister, R. F. (2018). The physiology of willpower: Linking blood
glucose to self-control. In Self-Regulation and Self-Control (pp. 137-180). Routledge
Hall, J. E. (2015). Guyton and Hall textbook of medical physiology e-Book. Elsevier Health
Sciences.
Hong, J., Zhang, Y., Lai, S., Lv, A., Su, Q., Dong, Y., ... & Zou, D. (2013). Effects of
metformin versus glipizide on cardiovascular outcomes in patients with type 2
diabetes and coronary artery disease. Diabetes care, 36(5), 1304-1311.
Huang, W., Castelino, R. L., & Peterson, G. M. (2014). Metformin usage in type 2 diabetes
mellitus: are safety guidelines adhered to?. Internal medicine journal, 44(3), 266-272.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.