University of Manchester Oral Health Education Dissertation
VerifiedAdded on 2022/08/13
|97
|19326
|435
Thesis and Dissertation
AI Summary
This dissertation, submitted to the University of Manchester by Yasser Khan, explores the effectiveness of verbal and nonverbal oral health clinical education in improving oral health in male and female Type 1 diabetic patients. The study, supervised by Azad Aziz, investigates whether a combined approach of verbal and nonverbal training enhances oral health compared to standard instructions. The research includes a literature review, methodology detailing study design, participant selection, randomization, and assessment tools (BOAS, MPS, and an oral health assessment tool). The dissertation outlines data management, statistical analysis, and ethical considerations. It aims to determine the impact of different training methods on oral health conditions, measured by dental caries, periodontal diseases, and other relevant metrics. The research utilizes a randomized control trial with pre- and post-test analysis to compare the outcomes of experimental and control groups, providing insights into the efficacy of comprehensive oral health education for diabetic patients.
1
The effectiveness of Verbal and Nonverbal Oral Health Clinical Education in improving Oral
Health in Male and Female Type 1 Diabetic Patients.
A dissertation submitted to the University of Manchester for the degree of Masters of
Restorative and Aesthetic Dentistry in the Faculty of Biology, Medicine and Health
2018-2020
Yasser khan
10328243
Supervised by
Azad Aziz
DIVISION OF DENTISTRY
The effectiveness of Verbal and Nonverbal Oral Health Clinical Education in improving Oral
Health in Male and Female Type 1 Diabetic Patients.
A dissertation submitted to the University of Manchester for the degree of Masters of
Restorative and Aesthetic Dentistry in the Faculty of Biology, Medicine and Health
2018-2020
Yasser khan
10328243
Supervised by
Azad Aziz
DIVISION OF DENTISTRY
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
Table of Contents
Abbreviation...............................................................................................................................6
Abstract......................................................................................................................................7
Declaration.................................................................................................................................8
Author information...................................................................................................................10
Background and Introduction...............................................................................................11
Definitions................................................................................................................................11
Hypotheses...............................................................................................................................15
Aims and objectives.................................................................................................................16
Research Question................................................................................................................16
Hypotheses...........................................................................................................................16
Research Aim.......................................................................................................................16
Objectives.............................................................................................................................16
Literature review......................................................................................................................17
Introduction/ Rationale.........................................................................................................17
Search strategy.....................................................................................................................19
Collection of the data...........................................................................................................20
Critique of the methodology used........................................................................................28
Assess for risk of bias..........................................................................................................34
Conclusion............................................................................................................................35
Study Design and methodology...............................................................................................37
Table of Contents
Abbreviation...............................................................................................................................6
Abstract......................................................................................................................................7
Declaration.................................................................................................................................8
Author information...................................................................................................................10
Background and Introduction...............................................................................................11
Definitions................................................................................................................................11
Hypotheses...............................................................................................................................15
Aims and objectives.................................................................................................................16
Research Question................................................................................................................16
Hypotheses...........................................................................................................................16
Research Aim.......................................................................................................................16
Objectives.............................................................................................................................16
Literature review......................................................................................................................17
Introduction/ Rationale.........................................................................................................17
Search strategy.....................................................................................................................19
Collection of the data...........................................................................................................20
Critique of the methodology used........................................................................................28
Assess for risk of bias..........................................................................................................34
Conclusion............................................................................................................................35
Study Design and methodology...............................................................................................37
3
Executive summary..................................................................................................................37
Table for abbreviations............................................................................................................38
Introduction..............................................................................................................................39
Literature review......................................................................................................................39
Research question.....................................................................................................................43
Research aim........................................................................................................................43
Research objectives..............................................................................................................43
Methodology............................................................................................................................43
Study design.........................................................................................................................43
Study population and sampling............................................................................................44
Randomisation......................................................................................................................45
Consent process....................................................................................................................45
Oral health training sessions................................................................................................46
Schedule of training.............................................................................................................47
Schedule of assessment........................................................................................................48
Data management.....................................................................................................................48
Data collection.................................................................................................................48
Data analysis....................................................................................................................51
Expected outcomes...................................................................................................................51
Ethical issues............................................................................................................................52
Roles and responsibilities of each team member.....................................................................52
Protocol ready..........................................................................................................................53
Executive summary..................................................................................................................37
Table for abbreviations............................................................................................................38
Introduction..............................................................................................................................39
Literature review......................................................................................................................39
Research question.....................................................................................................................43
Research aim........................................................................................................................43
Research objectives..............................................................................................................43
Methodology............................................................................................................................43
Study design.........................................................................................................................43
Study population and sampling............................................................................................44
Randomisation......................................................................................................................45
Consent process....................................................................................................................45
Oral health training sessions................................................................................................46
Schedule of training.............................................................................................................47
Schedule of assessment........................................................................................................48
Data management.....................................................................................................................48
Data collection.................................................................................................................48
Data analysis....................................................................................................................51
Expected outcomes...................................................................................................................51
Ethical issues............................................................................................................................52
Roles and responsibilities of each team member.....................................................................52
Protocol ready..........................................................................................................................53
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
Timeline of the study...............................................................................................................53
Data management, quality assurance and statistical analysis..................................................57
1. Data Collection and Management........................................................................................57
2. Quality Assurance................................................................................................................60
3. Sample size calculation........................................................................................................60
4. Hypotheses...........................................................................................................................62
5. Qualitative Analysis.............................................................................................................62
6. Statistical Analysis...............................................................................................................65
6. Critical Implication..............................................................................................................68
Ethics........................................................................................................................................69
Participant Information Sheet..................................................................................................69
Consent Form...........................................................................................................................73
Final Sections and Appendices................................................................................................74
Budget......................................................................................................................................74
Collaborations..........................................................................................................................75
References................................................................................................................................77
Appendix-A..............................................................................................................................85
Search results.......................................................................................................................85
Appendix-B..............................................................................................................................87
Interview questions..............................................................................................................87
Mucosal-Plaque Score (MPS)..............................................................................................88
Beck Oral Assessment Score (BOAS), modified.................................................................89
Timeline of the study...............................................................................................................53
Data management, quality assurance and statistical analysis..................................................57
1. Data Collection and Management........................................................................................57
2. Quality Assurance................................................................................................................60
3. Sample size calculation........................................................................................................60
4. Hypotheses...........................................................................................................................62
5. Qualitative Analysis.............................................................................................................62
6. Statistical Analysis...............................................................................................................65
6. Critical Implication..............................................................................................................68
Ethics........................................................................................................................................69
Participant Information Sheet..................................................................................................69
Consent Form...........................................................................................................................73
Final Sections and Appendices................................................................................................74
Budget......................................................................................................................................74
Collaborations..........................................................................................................................75
References................................................................................................................................77
Appendix-A..............................................................................................................................85
Search results.......................................................................................................................85
Appendix-B..............................................................................................................................87
Interview questions..............................................................................................................87
Mucosal-Plaque Score (MPS)..............................................................................................88
Beck Oral Assessment Score (BOAS), modified.................................................................89
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
Oral Health Assessment Tool...............................................................................................90
Mucosal-Plaque Score (MPS)..............................................................................................92
Beck Oral Assessment Score (BOAS), modified.................................................................93
Oral Health Assessment Tool...............................................................................................94
Introductory Letter...............................................................................................................95
Interview questions..............................................................................................................96
Abbreviation
T1D Type 1 diabetes
Oral Health Assessment Tool...............................................................................................90
Mucosal-Plaque Score (MPS)..............................................................................................92
Beck Oral Assessment Score (BOAS), modified.................................................................93
Oral Health Assessment Tool...............................................................................................94
Introductory Letter...............................................................................................................95
Interview questions..............................................................................................................96
Abbreviation
T1D Type 1 diabetes
6
HLA human leukocyte antigen
AIHW Australian Institute of Health and Welfare
DMFT Decay-missing- filled teeth
CPITN index Community Periodontal Index of Treatment
Needs index
CRP level C-Reactive Protein level
FPG Fasting Plasma Glucose
HbA1c glycosylated hemoglobin
PI Plaque Index
GI Gingival index
PD Pocket Depth
CAL Clinical Attachment Level
NSPT Non-Surgical Periodontal Treatment
OHI Oral Hygiene Instructions
RCT Randomized Control Trial
HLA human leukocyte antigen
AIHW Australian Institute of Health and Welfare
DMFT Decay-missing- filled teeth
CPITN index Community Periodontal Index of Treatment
Needs index
CRP level C-Reactive Protein level
FPG Fasting Plasma Glucose
HbA1c glycosylated hemoglobin
PI Plaque Index
GI Gingival index
PD Pocket Depth
CAL Clinical Attachment Level
NSPT Non-Surgical Periodontal Treatment
OHI Oral Hygiene Instructions
RCT Randomized Control Trial
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
Abstract
Type 1 diabetes (T1D) is prevalent among children and adolescents and creates an impact on
their health and wellbeing. People suffering from T1D are at an increased risk of developing
dry mouth, periodontitis, gingivitis, burning mouth syndrome and poor healing of the
damaged oral tissues. This research proposal aims to evaluate whether verbal and nonverbal
training helps in improving oral health of T1D patients, when compared to standard
instructions.
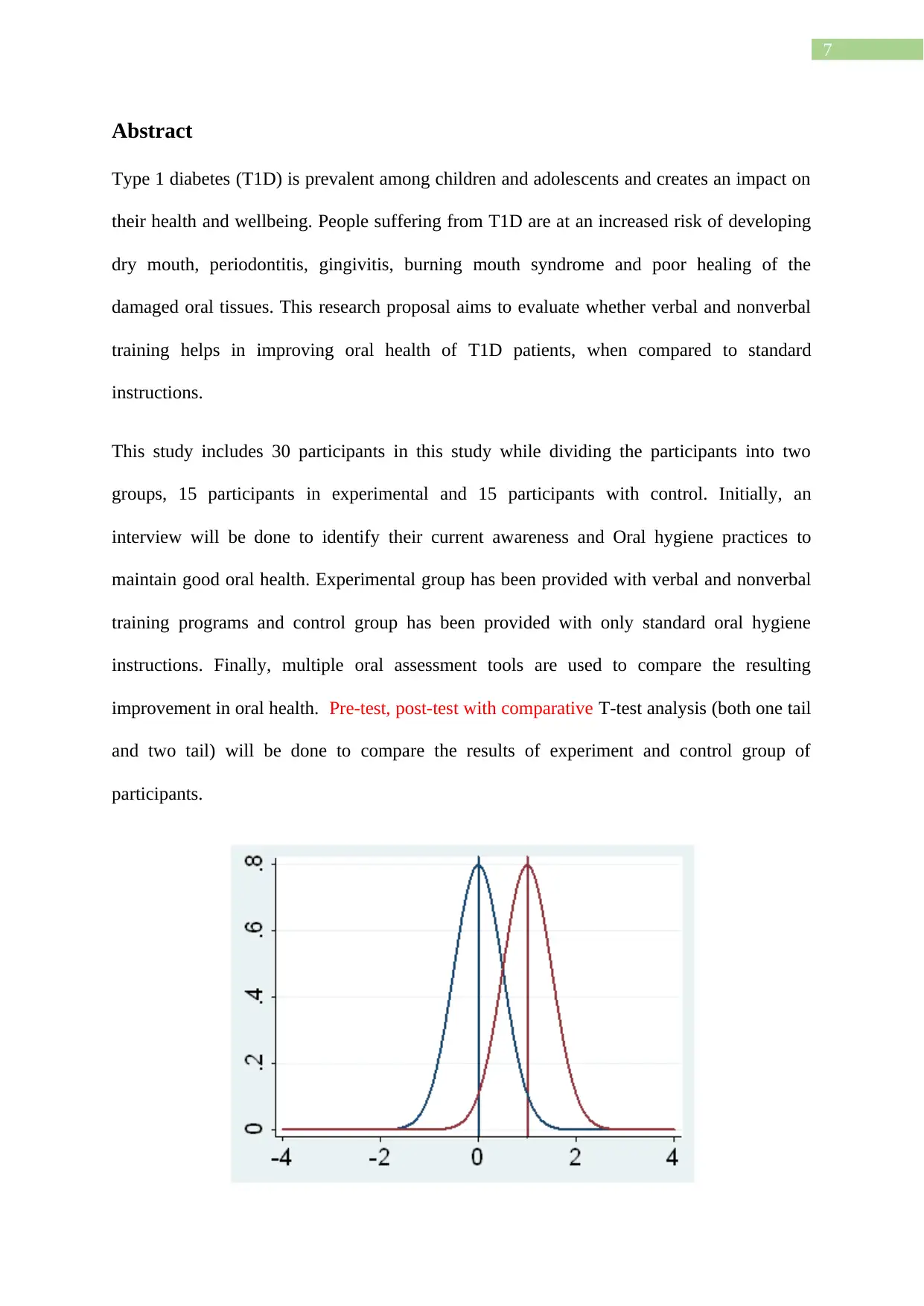
This study includes 30 participants in this study while dividing the participants into two
groups, 15 participants in experimental and 15 participants with control. Initially, an
interview will be done to identify their current awareness and Oral hygiene practices to
maintain good oral health. Experimental group has been provided with verbal and nonverbal
training programs and control group has been provided with only standard oral hygiene
instructions. Finally, multiple oral assessment tools are used to compare the resulting
improvement in oral health. Pre-test, post-test with comparative T-test analysis (both one tail
and two tail) will be done to compare the results of experiment and control group of
participants.
Abstract
Type 1 diabetes (T1D) is prevalent among children and adolescents and creates an impact on
their health and wellbeing. People suffering from T1D are at an increased risk of developing
dry mouth, periodontitis, gingivitis, burning mouth syndrome and poor healing of the
damaged oral tissues. This research proposal aims to evaluate whether verbal and nonverbal
training helps in improving oral health of T1D patients, when compared to standard
instructions.
This study includes 30 participants in this study while dividing the participants into two
groups, 15 participants in experimental and 15 participants with control. Initially, an
interview will be done to identify their current awareness and Oral hygiene practices to
maintain good oral health. Experimental group has been provided with verbal and nonverbal
training programs and control group has been provided with only standard oral hygiene
instructions. Finally, multiple oral assessment tools are used to compare the resulting
improvement in oral health. Pre-test, post-test with comparative T-test analysis (both one tail
and two tail) will be done to compare the results of experiment and control group of
participants.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

8
Figure 1
This figure shows two tailed t test with the significance (p value in x axis) and degree of
freedom (in y axis).
From this research it has been found that there is a significant difference in oral health
condition between the participants provided with extensive verbal and nonverbal training and
participants provided with only standard instruction. Therefore, it has been recommended that
through collaborative partnership of private and public organizations, verbal and non-verbal
training in Oral hygiene instruction for the patients with T1D helps in improving the Oral
health.
Declaration
No portion of the work referred to in the dissertation has been submitted in support of an
application for another degree or qualification of this or any other university or other institute
of learning.
Figure 1
This figure shows two tailed t test with the significance (p value in x axis) and degree of
freedom (in y axis).
From this research it has been found that there is a significant difference in oral health
condition between the participants provided with extensive verbal and nonverbal training and
participants provided with only standard instruction. Therefore, it has been recommended that
through collaborative partnership of private and public organizations, verbal and non-verbal
training in Oral hygiene instruction for the patients with T1D helps in improving the Oral
health.
Declaration
No portion of the work referred to in the dissertation has been submitted in support of an
application for another degree or qualification of this or any other university or other institute
of learning.
9
Intellectual property statement
i. The author of this dissertation (including any appendices and/or schedules to this
dissertation) owns certain copyright or related rights in it (the “Copyright”) and s/he
has given The University of Manchester certain rights to use such Copyright,
including for administrative purposes.
ii. Copies of this dissertation, either in full or in extracts and whether in hard or
electronic copy, may be made only in accordance with the Copyright, Designs and
Patents Act 1988 (as amended) and regulations issued under it or, where appropriate,
in accordance with licensing agreements which the University has entered into. This
page must form part of any such copies made.
iii. The ownership of certain Copyright, patents, designs, trademarks and other
intellectual property (the “Intellectual Property”) and any reproductions of copyright
works in the dissertation, for example graphs and tables (“Reproductions”), which
may be described in this dissertation, may not be owned by the author and may be
owned by third parties. Such Intellectual Property and Reproductions cannot and must
not be made available for use without the prior written permission of the owner(s) of
the relevant Intellectual Property and/or Reproductions.
Further information on the conditions under which disclosure, publication and
commercialization of this dissertation, the Copyright and any Intellectual Property and/or
Reproductions described in it may take place is available in the University IP Policy (see
http://documents.manchester.ac.uk/display.aspx?DocID=487), in any relevant Dissertation
restriction declarations deposited in the University Library, The University Library’s
regulations (see http://www.manchester.ac.uk/library/aboutus/regulations) and in The
University’s Guidance for the Presentation of Dissertations
Intellectual property statement
i. The author of this dissertation (including any appendices and/or schedules to this
dissertation) owns certain copyright or related rights in it (the “Copyright”) and s/he
has given The University of Manchester certain rights to use such Copyright,
including for administrative purposes.
ii. Copies of this dissertation, either in full or in extracts and whether in hard or
electronic copy, may be made only in accordance with the Copyright, Designs and
Patents Act 1988 (as amended) and regulations issued under it or, where appropriate,
in accordance with licensing agreements which the University has entered into. This
page must form part of any such copies made.
iii. The ownership of certain Copyright, patents, designs, trademarks and other
intellectual property (the “Intellectual Property”) and any reproductions of copyright
works in the dissertation, for example graphs and tables (“Reproductions”), which
may be described in this dissertation, may not be owned by the author and may be
owned by third parties. Such Intellectual Property and Reproductions cannot and must
not be made available for use without the prior written permission of the owner(s) of
the relevant Intellectual Property and/or Reproductions.
Further information on the conditions under which disclosure, publication and
commercialization of this dissertation, the Copyright and any Intellectual Property and/or
Reproductions described in it may take place is available in the University IP Policy (see
http://documents.manchester.ac.uk/display.aspx?DocID=487), in any relevant Dissertation
restriction declarations deposited in the University Library, The University Library’s
regulations (see http://www.manchester.ac.uk/library/aboutus/regulations) and in The
University’s Guidance for the Presentation of Dissertations
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
Author information
The principal investigator of the research is Dr Yasser Khan. Dr Khan completed his Bachelor of dental surgery
from the If you are making a statement on the outcome of the results you also need to provide a figure for the
statistical significance and confidence interval. This is a hypothetical scenario but need to look like real data.
in TN, India in 2004. After working 3 years in India, he went on to practice dentistry in
Melbourne Australia from 2008 till present. He is presently a student of the Msc programme
of Aesthetic and Restorative dentistry offered by the University of Manchester
His address is 65 high street, Kyneton, Victoria.
The contact details of the principal investigator is +61404211374.
Email ID of the principal investigator is Yasserkhan20@gmail.com.
Author information
The principal investigator of the research is Dr Yasser Khan. Dr Khan completed his Bachelor of dental surgery
from the If you are making a statement on the outcome of the results you also need to provide a figure for the
statistical significance and confidence interval. This is a hypothetical scenario but need to look like real data.
in TN, India in 2004. After working 3 years in India, he went on to practice dentistry in
Melbourne Australia from 2008 till present. He is presently a student of the Msc programme
of Aesthetic and Restorative dentistry offered by the University of Manchester
His address is 65 high street, Kyneton, Victoria.
The contact details of the principal investigator is +61404211374.
Email ID of the principal investigator is Yasserkhan20@gmail.com.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
Title of the study
The effectiveness of verbal and nonverbal oral health clinical education in improving oral
health in male and female Type 1 Diabetic patients.
Background and Introduction
Diabetic patients are often at risk of developing oral health challenges. The most common of
these problems include dry mouth, dental caries, tooth loss and periodontal diseases, among
others (Nazir et al., 2018). The proposed study seeks to assess the efficacy of verbal and
nonverbal oral health training on Type 1diabetic patients in comparison to standard verbal
oral health instructions without any verbal or non-verbal training. The aim of the study is to
discover the effectiveness of dental health knowledge among Type 1 diabetic patients, over a
period of 2 years. The primary objective of this study to examine determine efficacy of verbal
and non-verbal training. The secondary objective is to compare the efficacy of both of the
training with the references of different scores.
Definitions
Dental Health Clinical Training
Dental Health Clinical Training helps patients with dental problems to prevent the
consequences caused by the poor oral health. In these types of training the dental health
workers support the patient clinically or non-clinically to prevent oral disease and poor oral
health practices (Dwiel et al., 2019). The clinical interventions are related to different
medications whereas the non-clinical interventions are related to several health educational
programs and presentation or graphical representation of different training programs. Public
Health Dentistry is one of the better ways of dental heath training which helps general public
to get better oral health.
Type 1 diabetes
Title of the study
The effectiveness of verbal and nonverbal oral health clinical education in improving oral
health in male and female Type 1 Diabetic patients.
Background and Introduction
Diabetic patients are often at risk of developing oral health challenges. The most common of
these problems include dry mouth, dental caries, tooth loss and periodontal diseases, among
others (Nazir et al., 2018). The proposed study seeks to assess the efficacy of verbal and
nonverbal oral health training on Type 1diabetic patients in comparison to standard verbal
oral health instructions without any verbal or non-verbal training. The aim of the study is to
discover the effectiveness of dental health knowledge among Type 1 diabetic patients, over a
period of 2 years. The primary objective of this study to examine determine efficacy of verbal
and non-verbal training. The secondary objective is to compare the efficacy of both of the
training with the references of different scores.
Definitions
Dental Health Clinical Training
Dental Health Clinical Training helps patients with dental problems to prevent the
consequences caused by the poor oral health. In these types of training the dental health
workers support the patient clinically or non-clinically to prevent oral disease and poor oral
health practices (Dwiel et al., 2019). The clinical interventions are related to different
medications whereas the non-clinical interventions are related to several health educational
programs and presentation or graphical representation of different training programs. Public
Health Dentistry is one of the better ways of dental heath training which helps general public
to get better oral health.
Type 1 diabetes
12
Type 1 diabetes is a health condition where the pancreas do not produce sufficient
insulin and as a result the level of glucose is increased in blood(Katsarou et al., 2017).
This type of diabetes is also known as juvenile diabetes. Thirst, frequent urination, blurred
vision and hunger fatigue are some symptoms of type 1 diabetes.
Standard oral hygiene instructions
The standard oral hygiene instructions are aimed to improve the oral health practices and
to prevent different oral diseases. There are a few good practices which will help a person to
maintain good oral hygiene. The standard oral instructions are
One should brush his or her teeth twice a day
One should practice flossing to clean in between the teeth once daily.
An individual should avoid sweets or sugar rich foods in his or her diet.
An individual should visit the dentist on regular basis to evaluate his or her oral
health.
One should not smoke for better oral health.
Nonverbal Training
Nonverbal training consists of graphical representation of objectives of oral health
maintenance in diabetes type 1 patient. The training consists of power point presentation,
graphical presentations, Picture Exchange Communication System, motivational toys,
cartoons and slides, colour posters and written instructions or the diagrams of definite oral
health practices. It can also include techniques such as Tell show do and role play.Moreover,
usage of artefacts and touching behaviour will also be incorporated in the nonverbal training
sessions that will focus on the steps that need to be maintained for enhancing oral health.
Dental Caries
Type 1 diabetes is a health condition where the pancreas do not produce sufficient
insulin and as a result the level of glucose is increased in blood(Katsarou et al., 2017).
This type of diabetes is also known as juvenile diabetes. Thirst, frequent urination, blurred
vision and hunger fatigue are some symptoms of type 1 diabetes.
Standard oral hygiene instructions
The standard oral hygiene instructions are aimed to improve the oral health practices and
to prevent different oral diseases. There are a few good practices which will help a person to
maintain good oral hygiene. The standard oral instructions are
One should brush his or her teeth twice a day
One should practice flossing to clean in between the teeth once daily.
An individual should avoid sweets or sugar rich foods in his or her diet.
An individual should visit the dentist on regular basis to evaluate his or her oral
health.
One should not smoke for better oral health.
Nonverbal Training
Nonverbal training consists of graphical representation of objectives of oral health
maintenance in diabetes type 1 patient. The training consists of power point presentation,
graphical presentations, Picture Exchange Communication System, motivational toys,
cartoons and slides, colour posters and written instructions or the diagrams of definite oral
health practices. It can also include techniques such as Tell show do and role play.Moreover,
usage of artefacts and touching behaviour will also be incorporated in the nonverbal training
sessions that will focus on the steps that need to be maintained for enhancing oral health.
Dental Caries
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 97


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.