Review of Diabetes Prevalence and Risk Factors in UK Ethnic Groups
VerifiedAdded on 2021/04/17
|10
|3333
|35
Report
AI Summary
This report provides a comprehensive review of diabetes prevalence and associated risk factors within various ethnic groups in the UK. It begins with an abstract summarizing the increasing global presence of diabetes, particularly type 2, and highlights the disproportionate impact on certain ethnic groups, especially those of South Asian and Caribbean origin. The introduction emphasizes the role of ethnicity in chronic disease development and sets the stage for a literature review that explores genetic predispositions, lifestyle factors, and dietary habits contributing to higher diabetes rates in specific populations. The report examines research findings on the prevalence of diabetes in different ethnic groups, including South Asians, African Caribbeans, and Chinese populations, as well as the impact of obesity and socioeconomic factors. It discusses the challenges faced by healthcare organizations in the UK in developing culturally appropriate treatment programs and addresses the importance of lifestyle changes, such as diet control and increased physical activity, to mitigate the risk of diabetes. The report also covers the role of insulin resistance, hypertension, and genetic factors in diabetes development. It concludes by summarizing the key findings and emphasizing the need for targeted interventions to address the growing diabetes epidemic in diverse ethnic communities. The report stresses the need for diet control and physical activity to manage diabetes risk.
HEALTH
AND
SOCIAL CARE
AND
SOCIAL CARE
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

1
ABSTRACT
The global presence of diabetes is increasing at much faster rate. It has reached to
around 2.8% of the total population of the whole world. In this also the Type 2 diabetes
accounts to around 90% of the total diabetic patients. In some of the ethnic groups this
problem has got worsen. They are at higher risk to develop diabetes at any stage of the life.
This is the challenge for the health care services in UK which has a diverse ethnic population.
This problem has got worsen at new school age children. The prevalence of diabetes in some
of the ethnic groups is due to several kinds of factors. This review clearly illustrates the risk
of diabetes in some of the ethnic group being higher than that of the other groups. The global
presence of diabetes in various ethnic groups needs to be properly examined. Reason for their
less secretion of insulin has also been reviewed.
ABSTRACT
The global presence of diabetes is increasing at much faster rate. It has reached to
around 2.8% of the total population of the whole world. In this also the Type 2 diabetes
accounts to around 90% of the total diabetic patients. In some of the ethnic groups this
problem has got worsen. They are at higher risk to develop diabetes at any stage of the life.
This is the challenge for the health care services in UK which has a diverse ethnic population.
This problem has got worsen at new school age children. The prevalence of diabetes in some
of the ethnic groups is due to several kinds of factors. This review clearly illustrates the risk
of diabetes in some of the ethnic group being higher than that of the other groups. The global
presence of diabetes in various ethnic groups needs to be properly examined. Reason for their
less secretion of insulin has also been reviewed.
2
Contents
ABSTRACT..............................................................................................................................................1
Introduction...........................................................................................................................................2
Literature review...................................................................................................................................3
Conclusion.............................................................................................................................................6
Recommendations.................................................................................................................................6
REFERENCES......................................................................................................................................7
APPENDICES..........................................................................................................................................9
Introduction
In the modern lifestyle people are getting more prone to the chronic diseases. Many
researches have shown that ethnicity plays a very greater role in the development of these
diseases (Khan, et al., 2011). People belonging to any particular ethnical group are more
likely to have certain kind of chronic disease. This is due to various types of factors like their
particular lifestyle, their eating habits, believes and approach towards facing any disease. In
UK there are people that are coming from different regions of the world. Some of these
Contents
ABSTRACT..............................................................................................................................................1
Introduction...........................................................................................................................................2
Literature review...................................................................................................................................3
Conclusion.............................................................................................................................................6
Recommendations.................................................................................................................................6
REFERENCES......................................................................................................................................7
APPENDICES..........................................................................................................................................9
Introduction
In the modern lifestyle people are getting more prone to the chronic diseases. Many
researches have shown that ethnicity plays a very greater role in the development of these
diseases (Khan, et al., 2011). People belonging to any particular ethnical group are more
likely to have certain kind of chronic disease. This is due to various types of factors like their
particular lifestyle, their eating habits, believes and approach towards facing any disease. In
UK there are people that are coming from different regions of the world. Some of these
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
ethnic groups are more likely to get different types of diabetes. In the later section of this
report proper details about those particular groups have been illustrated.
Literature review
In the particular section of the people in particular regions it has been seen that they
have developed a common type of disease. This is due to the fact that they have a particular
type of genes in them. In the views of Zizi, et al., (2012) diabetes is most common in the UK
in a particular ethnic group coming from south Asia and Caribbean origin. These groups of
people are at more risk of developing diabetes as compared to the people from other origins.
In the people of South Asian descent the chances of developing Type 2 diabetes is up to 6
times then the people having other origins. In African and Africa Caribbean people the risk of
developing the Type 2 diabetes is three times more likely than that of people from other
origins.
On the contrary Chiu, et Al., (2011) has a view that in UK there are large number of people
that have come from the India and China. These countries have been considered as the
diabetes capitals of the world. The people that are having the black and Hispanic race are
more likely to have diabetes as compared to that of non-Hispanic whites. Some of the
minorities like American Indian and the natives of Alaska are more prone to develop
diabetes. Apart from this the Asian American and Pacific Islanders have also been found to
develop this disease. Development of this disease in the ethnic minorities has created
problems for the health care organizations in UK. The treatment policies have to be designed
as per their need. Developing culturally appropriate treatment programs can be helpful in this
regards Mostafa, et al., (2012).
On the other hand Menke, et al., (2014) worldwide prevalence of diabetes for all age groups
was calculated to be 2.8%. The total number of people that will be affected by this disease is
expected to rise from 171 million in 2000 to 366 million in 2030. In the regions of Asia and
Africa the rate of increase is expected to be two to three times. The major three countries that
are affected by this disease is USA, China and India and in future some other capitals for
diabetes is expected to come up like Brazil, Indonesia, Pakistan, Japan and Bangladesh. In
most of the people are affected by the Type two diabetes. It is approximately 90% of the total
cases.
ethnic groups are more likely to get different types of diabetes. In the later section of this
report proper details about those particular groups have been illustrated.
Literature review
In the particular section of the people in particular regions it has been seen that they
have developed a common type of disease. This is due to the fact that they have a particular
type of genes in them. In the views of Zizi, et al., (2012) diabetes is most common in the UK
in a particular ethnic group coming from south Asia and Caribbean origin. These groups of
people are at more risk of developing diabetes as compared to the people from other origins.
In the people of South Asian descent the chances of developing Type 2 diabetes is up to 6
times then the people having other origins. In African and Africa Caribbean people the risk of
developing the Type 2 diabetes is three times more likely than that of people from other
origins.
On the contrary Chiu, et Al., (2011) has a view that in UK there are large number of people
that have come from the India and China. These countries have been considered as the
diabetes capitals of the world. The people that are having the black and Hispanic race are
more likely to have diabetes as compared to that of non-Hispanic whites. Some of the
minorities like American Indian and the natives of Alaska are more prone to develop
diabetes. Apart from this the Asian American and Pacific Islanders have also been found to
develop this disease. Development of this disease in the ethnic minorities has created
problems for the health care organizations in UK. The treatment policies have to be designed
as per their need. Developing culturally appropriate treatment programs can be helpful in this
regards Mostafa, et al., (2012).
On the other hand Menke, et al., (2014) worldwide prevalence of diabetes for all age groups
was calculated to be 2.8%. The total number of people that will be affected by this disease is
expected to rise from 171 million in 2000 to 366 million in 2030. In the regions of Asia and
Africa the rate of increase is expected to be two to three times. The major three countries that
are affected by this disease is USA, China and India and in future some other capitals for
diabetes is expected to come up like Brazil, Indonesia, Pakistan, Japan and Bangladesh. In
most of the people are affected by the Type two diabetes. It is approximately 90% of the total
cases.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
In the views of Carolan, et al., (2012) Type 1 diabetes is more likely to be found in the people
belonging from temperate regions. It calculates to around 30-35 per 100000 children and
reduces while reaching towards equator. On the other hand Type 2 diabetes is more likely to
be found in the European and Asian communities. People who are living in the countries like
UK and belonging from the Asian region are most likely to get affected by this disease. In the
people who are from Indian sub continents and are above the age group of 40 years or so are
more influenced by this disease. The obesity is considered as one of the prime regions for this
rapid increase in the number of diabetic patients. American-Indian origins are the major
example of this. In the White UK children, Maturity onset diabetes of the young (MODY)
has also been found. This version of diabetes is same likely to be present in the white UK
children as the Type 2 version. The prevalence of diabetes in the Chinese people is not
different from the people in UK.
On the contrary Mørkrid, et al., (2012) believes that obesity is the reason for having higher
rate of Type 2 diabetes in South Asian community. The centralized fat distribution of the
body act as the insulin barrier. This is less in the white people. Apart from this it has also
been seen that the intake of folate and Vitamin B12 due to long cooking of the vegetables are
also the major reason for this. Along with this, a lower level of physical activity is also a
reason for it. In the UK and Finland a hypothesis suggests that growth restriction in utero in
the early life gives rise to metabolic programming which may result in the greater risk of
developing diabetes. Mean insulin and Central adiposity concentration was higher in South
Asian people but the glucose concentration were similar reflecting that there is higher
chances of developing diabetes at even younger ages. In the study it was found that some of
the children from Indian origin had phenotype with higher proportional central fat and higher
cord blood insulin concentration than the white children in UK. Obesity has been found as the
core reason for developing the Type 2 diabetes as these people has reduced insulin
sensitivity. In the UK schools the chances of black student developing diabetes is 15-20 %
more than that of white students. This is due to the lifestyle that both the ethnic groups lead.
On the other hand Tahrani, et al., (2012) states that people suffering from Dyslipidaemia is
more likely develop Type 2 diabetes due to poor glycemic control. The enhanced synthesis of
plasma lipoprotein and overall cholesterol at the time of hyperglycaemia, adds to the
acceleration of atherosclerosis found in Type 2 disease.
In the views of Carolan, et al., (2012) Type 1 diabetes is more likely to be found in the people
belonging from temperate regions. It calculates to around 30-35 per 100000 children and
reduces while reaching towards equator. On the other hand Type 2 diabetes is more likely to
be found in the European and Asian communities. People who are living in the countries like
UK and belonging from the Asian region are most likely to get affected by this disease. In the
people who are from Indian sub continents and are above the age group of 40 years or so are
more influenced by this disease. The obesity is considered as one of the prime regions for this
rapid increase in the number of diabetic patients. American-Indian origins are the major
example of this. In the White UK children, Maturity onset diabetes of the young (MODY)
has also been found. This version of diabetes is same likely to be present in the white UK
children as the Type 2 version. The prevalence of diabetes in the Chinese people is not
different from the people in UK.
On the contrary Mørkrid, et al., (2012) believes that obesity is the reason for having higher
rate of Type 2 diabetes in South Asian community. The centralized fat distribution of the
body act as the insulin barrier. This is less in the white people. Apart from this it has also
been seen that the intake of folate and Vitamin B12 due to long cooking of the vegetables are
also the major reason for this. Along with this, a lower level of physical activity is also a
reason for it. In the UK and Finland a hypothesis suggests that growth restriction in utero in
the early life gives rise to metabolic programming which may result in the greater risk of
developing diabetes. Mean insulin and Central adiposity concentration was higher in South
Asian people but the glucose concentration were similar reflecting that there is higher
chances of developing diabetes at even younger ages. In the study it was found that some of
the children from Indian origin had phenotype with higher proportional central fat and higher
cord blood insulin concentration than the white children in UK. Obesity has been found as the
core reason for developing the Type 2 diabetes as these people has reduced insulin
sensitivity. In the UK schools the chances of black student developing diabetes is 15-20 %
more than that of white students. This is due to the lifestyle that both the ethnic groups lead.
On the other hand Tahrani, et al., (2012) states that people suffering from Dyslipidaemia is
more likely develop Type 2 diabetes due to poor glycemic control. The enhanced synthesis of
plasma lipoprotein and overall cholesterol at the time of hyperglycaemia, adds to the
acceleration of atherosclerosis found in Type 2 disease.
5
Hussen, Persson and Moradi, (2015) states that rising blood pressure due to the hypertension
is one of the major reason why some of the ethnic people has any type of diabetes. These
people have their poor vital functionality which leads to restriction in insulin secretion. In the
case of Hyper tension obesity is always noticed which results in increase in the chances of
diabetes.
Glucose tolerance in both Pakistani and European people is less and hence a low insulin
resistance is noticed. It is also due to the fact that there are many people that are coming to
the Europe have more chances of gaining weights and hence their glucose tolerance is less.
Their different metabolism is also a major factor why the person of some ethnic groups
develops diabetes.
In the view of Robinson, Agarwal and Nerenberg, (2011) people from India are having the
eating habits that include more oil reach food. Such a heavy cooking always leads to decrease
in the amount of insulin secreted from the pancreas which is a major reason for such
predominanace of this disease in this area. The number of cases of diabetic patient in the
south Asian region increased in last few decades (Everett, Frithsen and Player, (2011). This is
due to the reason that there food habits have changes as well as the people are still preferring
to eat highly oil reach food while the workouts have not been adequate. India has a large
population of diabetic patients. One interesting fact about the spread of this disease in India is
that most of the people who have this disease are rich or medium class families. This is due to
the reason because they do not give proper care to the physical activity which leads to
increase in the internal fat. In the countries like UK it can be seen that in the younger age the
people are highly conscious about their health and hence are indulging in some of the
physical activities. On the other hand in the countries like India the people are trained to
become a professional from the early ages and hence they are unable to get participate in any
of the physical activity (Sinha, et al., (2014). This starts at the school age where the students
are not promoted towards the extra-curricular activity since their primary focus is on studies.
This leads to increase in hyper tension which is another important factor of developing
diabetes at early ages. In the early part of the 20th century this problem started to worsen in
many of the people from these regions.
Davis, Coleman and Holman, (2014) states that the spread of the diabetes was not been
controlled at the earlier stages. In the early 20th century a health program related to such
chronic diseases was needed. This can also be seen in the African countries which also has a
Hussen, Persson and Moradi, (2015) states that rising blood pressure due to the hypertension
is one of the major reason why some of the ethnic people has any type of diabetes. These
people have their poor vital functionality which leads to restriction in insulin secretion. In the
case of Hyper tension obesity is always noticed which results in increase in the chances of
diabetes.
Glucose tolerance in both Pakistani and European people is less and hence a low insulin
resistance is noticed. It is also due to the fact that there are many people that are coming to
the Europe have more chances of gaining weights and hence their glucose tolerance is less.
Their different metabolism is also a major factor why the person of some ethnic groups
develops diabetes.
In the view of Robinson, Agarwal and Nerenberg, (2011) people from India are having the
eating habits that include more oil reach food. Such a heavy cooking always leads to decrease
in the amount of insulin secreted from the pancreas which is a major reason for such
predominanace of this disease in this area. The number of cases of diabetic patient in the
south Asian region increased in last few decades (Everett, Frithsen and Player, (2011). This is
due to the reason that there food habits have changes as well as the people are still preferring
to eat highly oil reach food while the workouts have not been adequate. India has a large
population of diabetic patients. One interesting fact about the spread of this disease in India is
that most of the people who have this disease are rich or medium class families. This is due to
the reason because they do not give proper care to the physical activity which leads to
increase in the internal fat. In the countries like UK it can be seen that in the younger age the
people are highly conscious about their health and hence are indulging in some of the
physical activities. On the other hand in the countries like India the people are trained to
become a professional from the early ages and hence they are unable to get participate in any
of the physical activity (Sinha, et al., (2014). This starts at the school age where the students
are not promoted towards the extra-curricular activity since their primary focus is on studies.
This leads to increase in hyper tension which is another important factor of developing
diabetes at early ages. In the early part of the 20th century this problem started to worsen in
many of the people from these regions.
Davis, Coleman and Holman, (2014) states that the spread of the diabetes was not been
controlled at the earlier stages. In the early 20th century a health program related to such
chronic diseases was needed. This can also be seen in the African countries which also has a
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
low quality health services. This has led to increase in the number of diabetic cases.
According to the fourth national survey on health it was noticed that in UK the patients that
are manual workers had less chances of developing diabetes while the people that are non-
manual workers are more likely to develop this disease. In the countries like UK it was
noticed that diabetes was more common in the no full time workers irrespective of their
current socioeconomic position.
On the contrary Khoo, et al., (2011) believes that people of these ethnic groups were highly
uneducated about the initial symptoms of this disease. They also give no response to the intial
sign of developing this disease. In the country like the population explosion has been fast and
the health care needs of the country has not been properly addressed by the government
which has made the situations worst. In some of the cases it was noticed that both the types of
diabetes were genetic. This is due to the reason that after a certain age these people were
unable to make so much of insulin as required (Oldroyd, et al., 2017). The change in the life
style has made this situation worst. Many children from the South Asian origin develop this
disease because their mother or father has this disease. In India the situation is illustrated by
many examples. The Indian food habits like the intake of large amount of glucose in their
food have worsened this problem (Diabetes, (2017).
Conclusion
From the above section of this literature review it can be seen that In UK there are
many people present who are from different origins. The ethnic groups from south Asian and
African region are more likely to develop this disease. This is due to various types of reason
in which Lifestyle and food habits plays a more vital role. These people need a diet control
that can help them in reducing the risk of the progression to diabetes. Apart from this a
various surveys have shown that this disease was developed in the children at the early age
and most of them were non-white. Their upbringing played a very crucial role in this regards.
A proper health plan is needed for removing this disease especially in the mixed population
like UK.
Recommendations
A proper care is needed for the children whose family had a long history of diabetes patients.
This is the only way that such a genetic failure can be controlled. A variety of drugs is
available in the market for the recovery of such patients. It was also noticed that lifestyle
low quality health services. This has led to increase in the number of diabetic cases.
According to the fourth national survey on health it was noticed that in UK the patients that
are manual workers had less chances of developing diabetes while the people that are non-
manual workers are more likely to develop this disease. In the countries like UK it was
noticed that diabetes was more common in the no full time workers irrespective of their
current socioeconomic position.
On the contrary Khoo, et al., (2011) believes that people of these ethnic groups were highly
uneducated about the initial symptoms of this disease. They also give no response to the intial
sign of developing this disease. In the country like the population explosion has been fast and
the health care needs of the country has not been properly addressed by the government
which has made the situations worst. In some of the cases it was noticed that both the types of
diabetes were genetic. This is due to the reason that after a certain age these people were
unable to make so much of insulin as required (Oldroyd, et al., 2017). The change in the life
style has made this situation worst. Many children from the South Asian origin develop this
disease because their mother or father has this disease. In India the situation is illustrated by
many examples. The Indian food habits like the intake of large amount of glucose in their
food have worsened this problem (Diabetes, (2017).
Conclusion
From the above section of this literature review it can be seen that In UK there are
many people present who are from different origins. The ethnic groups from south Asian and
African region are more likely to develop this disease. This is due to various types of reason
in which Lifestyle and food habits plays a more vital role. These people need a diet control
that can help them in reducing the risk of the progression to diabetes. Apart from this a
various surveys have shown that this disease was developed in the children at the early age
and most of them were non-white. Their upbringing played a very crucial role in this regards.
A proper health plan is needed for removing this disease especially in the mixed population
like UK.
Recommendations
A proper care is needed for the children whose family had a long history of diabetes patients.
This is the only way that such a genetic failure can be controlled. A variety of drugs is
available in the market for the recovery of such patients. It was also noticed that lifestyle
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

7
intervention is more effective than that of drug intervention. The lifestyle change will helps
more in removing this problem as compared to the drug the use. In the country like UK a
special program for the removal of such disease in some ethnic group is needed. Some of the
most common problem that arises in the removal of this disease is the life style and the age
old thinking of these ethnic groups towards this disease. Once this barrier is removed it would
be easy to provide better health care services to these ethnic communities in UK. It is also to
be made sure that the people have a diet maintained at early ages so that such health concern
does not occurs. Even though the removal of Type 1 disease is more difficult then also an
approach towards this disease needs to change in the African and South Asian Region.
REFERENCES
Carolan, M., Davey, M.A., Biro, M.A. and Kealy, M., (2012) Maternal age, ethnicity and
gestational diabetes mellitus. Midwifery, 28(6), pp.778-783.
Chiu, M., Austin, P.C., Manuel, D.G., Shah, B.R. and Tu, J.V., (2011) Deriving ethnic-
specific BMI cutoff points for assessing diabetes risk. Diabetes care, 34(8), pp.1741-1748.
Davis, T.M.E., Coleman, R.L. and Holman, R.R., (2014) Ethnicity and long‐term vascular
outcomes in Type 2 diabetes: a prospective observational study (UKPDS 83). Diabetic
Medicine, 31(2), pp.200-207.
Diabetes, (2017), diabetes and ethnicity, [Online]. Available at:
https://www.diabetes.co.uk/diabetes-and-ethnicity.html. [Accessed on: 20th March 2018].
Everett, C.J., Frithsen, I. and Player, M., (2011) Relationship of polychlorinated biphenyls
with type 2 diabetes and hypertension. Journal of Environmental Monitoring, 13(2), pp.241-
251.
Hussen, H.I., Persson, M. and Moradi, T., (2015) Maternal overweight and obesity are
associated with increased risk of type 1 diabetes in offspring of parents without diabetes
regardless of ethnicity. Diabetologia, 58(7), pp.1464-1473.
Khan, N.A., Wang, H., Anand, S., Jin, Y., Campbell, N.R., Pilote, L. and Quan, H., (2011)
Ethnicity and sex affect diabetes incidence and outcomes. Diabetes care, 34(1), pp.96-101.
Khoo, C.M., Sairazi, S., Taslim, S., Gardner, D., Wu, Y., Lee, J., van Dam, R.M. and Tai,
E.S., (2011) Ethnicity modifies the relationships of insulin resistance, inflammation, and
intervention is more effective than that of drug intervention. The lifestyle change will helps
more in removing this problem as compared to the drug the use. In the country like UK a
special program for the removal of such disease in some ethnic group is needed. Some of the
most common problem that arises in the removal of this disease is the life style and the age
old thinking of these ethnic groups towards this disease. Once this barrier is removed it would
be easy to provide better health care services to these ethnic communities in UK. It is also to
be made sure that the people have a diet maintained at early ages so that such health concern
does not occurs. Even though the removal of Type 1 disease is more difficult then also an
approach towards this disease needs to change in the African and South Asian Region.
REFERENCES
Carolan, M., Davey, M.A., Biro, M.A. and Kealy, M., (2012) Maternal age, ethnicity and
gestational diabetes mellitus. Midwifery, 28(6), pp.778-783.
Chiu, M., Austin, P.C., Manuel, D.G., Shah, B.R. and Tu, J.V., (2011) Deriving ethnic-
specific BMI cutoff points for assessing diabetes risk. Diabetes care, 34(8), pp.1741-1748.
Davis, T.M.E., Coleman, R.L. and Holman, R.R., (2014) Ethnicity and long‐term vascular
outcomes in Type 2 diabetes: a prospective observational study (UKPDS 83). Diabetic
Medicine, 31(2), pp.200-207.
Diabetes, (2017), diabetes and ethnicity, [Online]. Available at:
https://www.diabetes.co.uk/diabetes-and-ethnicity.html. [Accessed on: 20th March 2018].
Everett, C.J., Frithsen, I. and Player, M., (2011) Relationship of polychlorinated biphenyls
with type 2 diabetes and hypertension. Journal of Environmental Monitoring, 13(2), pp.241-
251.
Hussen, H.I., Persson, M. and Moradi, T., (2015) Maternal overweight and obesity are
associated with increased risk of type 1 diabetes in offspring of parents without diabetes
regardless of ethnicity. Diabetologia, 58(7), pp.1464-1473.
Khan, N.A., Wang, H., Anand, S., Jin, Y., Campbell, N.R., Pilote, L. and Quan, H., (2011)
Ethnicity and sex affect diabetes incidence and outcomes. Diabetes care, 34(1), pp.96-101.
Khoo, C.M., Sairazi, S., Taslim, S., Gardner, D., Wu, Y., Lee, J., van Dam, R.M. and Tai,
E.S., (2011) Ethnicity modifies the relationships of insulin resistance, inflammation, and
8
adiponectin with obesity in a multiethnic Asian population. Diabetes Care, 34(5), pp.1120-
1126.
Menke, A., Rust, K.F., Fradkin, J., Cheng, Y.J. and Cowie, C.C., (2014) Associations
between trends in race/ethnicity, aging, and body mass index with diabetes prevalence in the
United States: a series of cross-sectional studies. Annals of internal medicine, 161(5), pp.328-
335.
Mørkrid, K., Jenum, A.K., Sletner, L., Vårdal, M.H., Waage, C.W., Nakstad, B., Vangen, S.
and Birkeland, K.I., (2012) Failure to increase insulin secretory capacity during pregnancy-
induced insulin resistance is associated with ethnicity and gestational diabetes. European
journal of endocrinology, 167(4), pp.579-588.
Mostafa, S.A., Davies, M.J., Webb, D.R., Srinivasan, B.T., Gray, L.J. and Khunti, K., (2012)
Independent effect of ethnicity on glycemia in South Asians and white Europeans. Diabetes
Care, 35(8), pp.1746-1748.
Oldroyd, J., Banerjee, M., Heald, A. and Cruickshank, K, (2017), Diabetes and ethnic
minorities, [Online]. Available at: http://pmj.bmj.com/content/81/958/486. [Accessed on: 20th
March 2018].
Robinson, C.A., Agarwal, G. and Nerenberg, K., (2011) Validating the CANRISK prognostic
model for assessing diabetes risk in Canada's multi-ethnic population. Chronic diseases and
injuries in Canada, 32(1).
Sinha, S.K., Shaheen, M., Rajavashisth, T.B., Pan, D., Norris, K.C. and Nicholas, S.B.,
(2014) Association of race/ethnicity, inflammation, and albuminuria in patients with diabetes
and early chronic kidney disease. Diabetes Care, 37(4), pp.1060-1068.
Tahrani, A.A., Ali, A., Raymond, N.T., Begum, S., Dubb, K., Mughal, S., Jose, B., Piya,
M.K., Barnett, A.H. and Stevens, M.J., (2012) Obstructive sleep apnea and diabetic
neuropathy: a novel association in patients with type 2 diabetes. American journal of
respiratory and critical care medicine, 186(5), pp.434-441.
Zizi, F., Pandey, A., Murrray-Bachmann, R., Vincent, M., McFarlane, S., Ogedegbe, G. and
Jean-Louis, G., (2012) Race/ethnicity, sleep duration, and diabetes mellitus: analysis of the
National Health Interview Survey. The American journal of medicine, 125(2), pp.162-167.
adiponectin with obesity in a multiethnic Asian population. Diabetes Care, 34(5), pp.1120-
1126.
Menke, A., Rust, K.F., Fradkin, J., Cheng, Y.J. and Cowie, C.C., (2014) Associations
between trends in race/ethnicity, aging, and body mass index with diabetes prevalence in the
United States: a series of cross-sectional studies. Annals of internal medicine, 161(5), pp.328-
335.
Mørkrid, K., Jenum, A.K., Sletner, L., Vårdal, M.H., Waage, C.W., Nakstad, B., Vangen, S.
and Birkeland, K.I., (2012) Failure to increase insulin secretory capacity during pregnancy-
induced insulin resistance is associated with ethnicity and gestational diabetes. European
journal of endocrinology, 167(4), pp.579-588.
Mostafa, S.A., Davies, M.J., Webb, D.R., Srinivasan, B.T., Gray, L.J. and Khunti, K., (2012)
Independent effect of ethnicity on glycemia in South Asians and white Europeans. Diabetes
Care, 35(8), pp.1746-1748.
Oldroyd, J., Banerjee, M., Heald, A. and Cruickshank, K, (2017), Diabetes and ethnic
minorities, [Online]. Available at: http://pmj.bmj.com/content/81/958/486. [Accessed on: 20th
March 2018].
Robinson, C.A., Agarwal, G. and Nerenberg, K., (2011) Validating the CANRISK prognostic
model for assessing diabetes risk in Canada's multi-ethnic population. Chronic diseases and
injuries in Canada, 32(1).
Sinha, S.K., Shaheen, M., Rajavashisth, T.B., Pan, D., Norris, K.C. and Nicholas, S.B.,
(2014) Association of race/ethnicity, inflammation, and albuminuria in patients with diabetes
and early chronic kidney disease. Diabetes Care, 37(4), pp.1060-1068.
Tahrani, A.A., Ali, A., Raymond, N.T., Begum, S., Dubb, K., Mughal, S., Jose, B., Piya,
M.K., Barnett, A.H. and Stevens, M.J., (2012) Obstructive sleep apnea and diabetic
neuropathy: a novel association in patients with type 2 diabetes. American journal of
respiratory and critical care medicine, 186(5), pp.434-441.
Zizi, F., Pandey, A., Murrray-Bachmann, R., Vincent, M., McFarlane, S., Ogedegbe, G. and
Jean-Louis, G., (2012) Race/ethnicity, sleep duration, and diabetes mellitus: analysis of the
National Health Interview Survey. The American journal of medicine, 125(2), pp.162-167.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
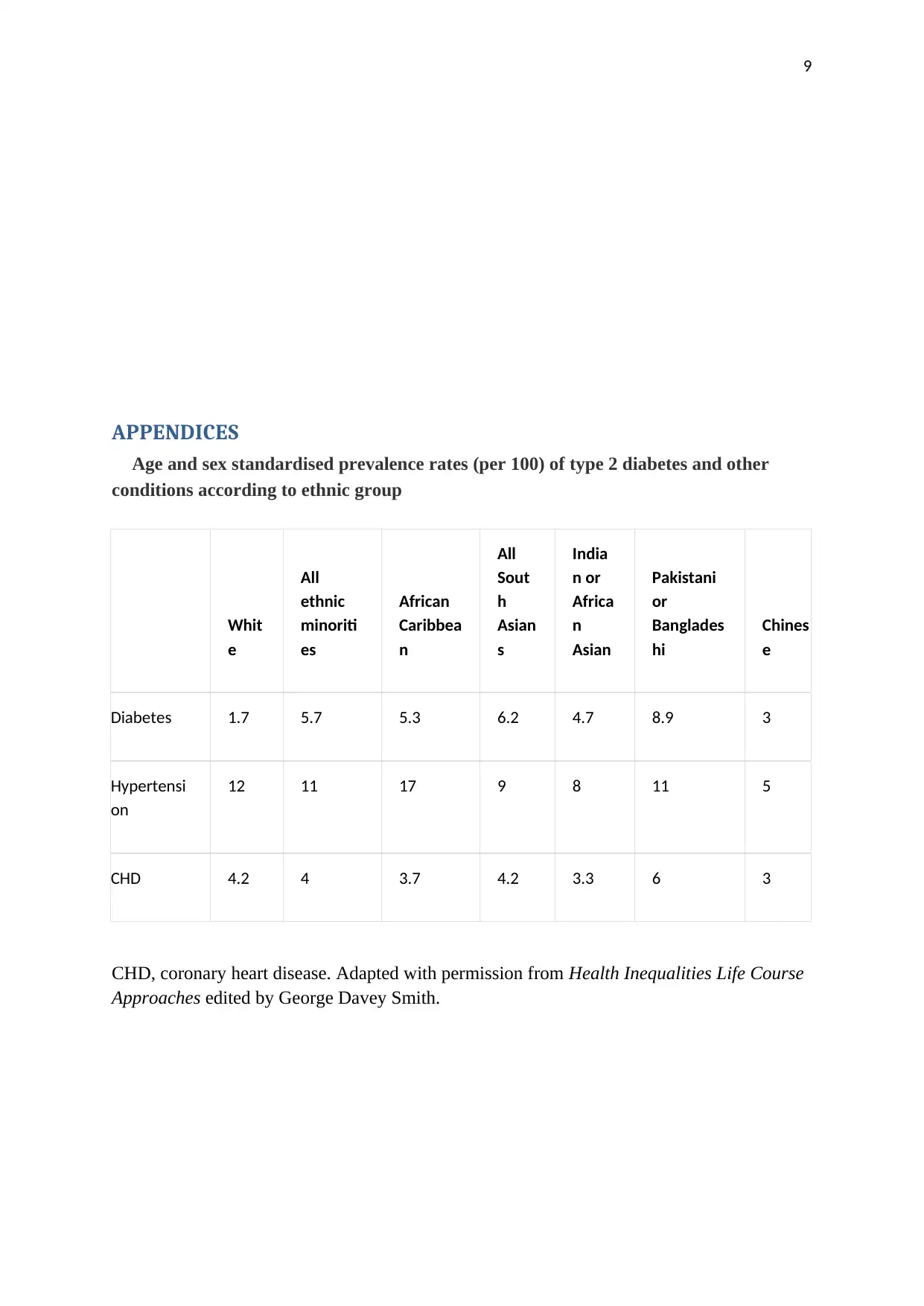
APPENDICES
Age and sex standardised prevalence rates (per 100) of type 2 diabetes and other
conditions according to ethnic group
Whit
e
All
ethnic
minoriti
es
African
Caribbea
n
All
Sout
h
Asian
s
India
n or
Africa
n
Asian
Pakistani
or
Banglades
hi
Chines
e
Diabetes 1.7 5.7 5.3 6.2 4.7 8.9 3
Hypertensi
on
12 11 17 9 8 11 5
CHD 4.2 4 3.7 4.2 3.3 6 3
CHD, coronary heart disease. Adapted with permission from Health Inequalities Life Course
Approaches edited by George Davey Smith.
APPENDICES
Age and sex standardised prevalence rates (per 100) of type 2 diabetes and other
conditions according to ethnic group
Whit
e
All
ethnic
minoriti
es
African
Caribbea
n
All
Sout
h
Asian
s
India
n or
Africa
n
Asian
Pakistani
or
Banglades
hi
Chines
e
Diabetes 1.7 5.7 5.3 6.2 4.7 8.9 3
Hypertensi
on
12 11 17 9 8 11 5
CHD 4.2 4 3.7 4.2 3.3 6 3
CHD, coronary heart disease. Adapted with permission from Health Inequalities Life Course
Approaches edited by George Davey Smith.
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.