Comprehensive Report: Diabetic Ketoacidosis (DKA) and Cerebral Oedema
VerifiedAdded on 2019/09/22
|14
|3817
|251
Report
AI Summary
This report provides a comprehensive overview of Diabetic Ketoacidosis (DKA) and cerebral oedema, focusing on epidemiology, recent research findings, and effective interventions. It begins with an introduction to DKA, explaining its causes and the role of insulin deficiency. The report then delves into the epidemiology of DKA and cerebral oedema, highlighting their prevalence in children and adolescents, and the associated mortality rates. Recent research findings are discussed, including risk factors, symptoms, and the importance of early detection. The core of the report focuses on interventions, including inpatient and outpatient care, fluid replacement strategies, insulin replacement protocols, and electrolyte management, with detailed explanations of each. The report also addresses the treatment of cerebral oedema and the use of osmotic diuretics. The report underscores the importance of close monitoring and early intervention in managing these conditions, drawing on guidelines and studies to provide a clear picture of the current best practices in the field.

Running Header: DIABETIC KETOACIDOSIS (DKA) AND CEREBRAL OEDEMA
1
Diabetic Ketoacidosis (DKA) and Cerebral Oedema
1
Diabetic Ketoacidosis (DKA) and Cerebral Oedema
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 2
Contents
1. Introduction............................................................................................................................3
2. Epidemiology of DKA and cerebral oedema due to DKA....................................................3
3. Recent research findings........................................................................................................4
4. Interventions...........................................................................................................................5
5. Conclusion..............................................................................................................................9
Contents
1. Introduction............................................................................................................................3
2. Epidemiology of DKA and cerebral oedema due to DKA....................................................3
3. Recent research findings........................................................................................................4
4. Interventions...........................................................................................................................5
5. Conclusion..............................................................................................................................9
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 3
1. Introduction
Diabetic ketoacidosis as per Savage et al (2011), results when cells in the body are deprived
of glucose due to low secretion of insulin. This sugar or glucose unable to get into the body
cells remains into the blood. Although kidneys filter some of this glucose but maximum
remains present in the blood and on the other hand as the body cells are deprived of the
energy, they break down stored fats and muscles to get the required energy. This gives rise to
ketone bodies due to the chemical imbalance that is incurred due to abnormality of insulin
and this gives rise to a condition called DKA.
Cerebral oedema is refereed to excessive accumulation of fluid in both intercellular and
extracellular spaces of the brain. Is one of the major complications in DKA in children that
even lead to death.
2. Epidemiology of DKA and cerebral oedema due to DKA
DKA in children in US and UK are one of the most common conditions of severe mortality
and morbidity. Cerebral oedema is one of the critical complication of DKA that are
commonly observed in children and in adolescents. DKA can result in the children with both
type 1 and type 2 diabetes (Glaser et al, 2013). A health care professional trained in children
diabetes management must go through the guidelines provided in Canadian Diabetes
Association 2003 for preventing and managing children diabetes in a proper manner. It has
been reported that cerebral oedema is present in 1% of all the children with DKA. Almost 50-
60% of children deaths with DKA occur due to cerebral oedema. It is established that DKA
risk increases from 1% to 10% per patient each year and the risk is higher in adolescent and
peripubertal girls who have poor metabolic control or have DKA, difficult family
circumstances and psychiatric disorders (Becker, 2017). Type 1 diabetes or T1D Exchange
1. Introduction
Diabetic ketoacidosis as per Savage et al (2011), results when cells in the body are deprived
of glucose due to low secretion of insulin. This sugar or glucose unable to get into the body
cells remains into the blood. Although kidneys filter some of this glucose but maximum
remains present in the blood and on the other hand as the body cells are deprived of the
energy, they break down stored fats and muscles to get the required energy. This gives rise to
ketone bodies due to the chemical imbalance that is incurred due to abnormality of insulin
and this gives rise to a condition called DKA.
Cerebral oedema is refereed to excessive accumulation of fluid in both intercellular and
extracellular spaces of the brain. Is one of the major complications in DKA in children that
even lead to death.
2. Epidemiology of DKA and cerebral oedema due to DKA
DKA in children in US and UK are one of the most common conditions of severe mortality
and morbidity. Cerebral oedema is one of the critical complication of DKA that are
commonly observed in children and in adolescents. DKA can result in the children with both
type 1 and type 2 diabetes (Glaser et al, 2013). A health care professional trained in children
diabetes management must go through the guidelines provided in Canadian Diabetes
Association 2003 for preventing and managing children diabetes in a proper manner. It has
been reported that cerebral oedema is present in 1% of all the children with DKA. Almost 50-
60% of children deaths with DKA occur due to cerebral oedema. It is established that DKA
risk increases from 1% to 10% per patient each year and the risk is higher in adolescent and
peripubertal girls who have poor metabolic control or have DKA, difficult family
circumstances and psychiatric disorders (Becker, 2017). Type 1 diabetes or T1D Exchange
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 4
researchers from the largest multinational analysis of diabetic ketoacidosis found out in 2015
that there are some common risk factors of DKA across five countries and although the
condition is preventable but it remains a serious threat to the patients with type 1 diabetes.
Researchers has estimated that annual costs of treating DKA accounts for $90 million
annually as more than 12,700 paediatric patients gets diagnosed with DKA each year in the
US.
It is clinically significant as per a recent research conducted in 2017, that more or less 1% of
DKA episodes in paediatric patients bears a mortality rate of 20-90% (Watts and Edge,
2014). The overall mortality rates in suffering children and adolescents remains between 0.15
to 0.51% as per the national population study in the United States and Canada, UK.
3. Recent research findings
As per a recent research conducted by DeCourcey et al (2013), it was seen in a population
based study in UK that presence of cerebral oedema is three times more common to the
children with new onset diabetes rather than those who have been detected with diabetes
earlier. A multicentre study was conducted with 61 children suffering from cerebral oedema
and it was seen treatment with bicarbonate are common with these cases. The researchers
also found out that patients who have low serum sodium concentration with low blood
glucose level are also prone to this disease.
Patient with diabetes are more prone to develop DKA in future. The initial symptoms are
polyuria and polydipsia which often goes unnoticed by the parents (Cameron et al., 2014).
When diabetes progresses, it may precipitates other complications that can be fatal to the
suffering child’s life if it is not treated in time. The symptoms of DKA includes
researchers from the largest multinational analysis of diabetic ketoacidosis found out in 2015
that there are some common risk factors of DKA across five countries and although the
condition is preventable but it remains a serious threat to the patients with type 1 diabetes.
Researchers has estimated that annual costs of treating DKA accounts for $90 million
annually as more than 12,700 paediatric patients gets diagnosed with DKA each year in the
US.
It is clinically significant as per a recent research conducted in 2017, that more or less 1% of
DKA episodes in paediatric patients bears a mortality rate of 20-90% (Watts and Edge,
2014). The overall mortality rates in suffering children and adolescents remains between 0.15
to 0.51% as per the national population study in the United States and Canada, UK.
3. Recent research findings
As per a recent research conducted by DeCourcey et al (2013), it was seen in a population
based study in UK that presence of cerebral oedema is three times more common to the
children with new onset diabetes rather than those who have been detected with diabetes
earlier. A multicentre study was conducted with 61 children suffering from cerebral oedema
and it was seen treatment with bicarbonate are common with these cases. The researchers
also found out that patients who have low serum sodium concentration with low blood
glucose level are also prone to this disease.
Patient with diabetes are more prone to develop DKA in future. The initial symptoms are
polyuria and polydipsia which often goes unnoticed by the parents (Cameron et al., 2014).
When diabetes progresses, it may precipitates other complications that can be fatal to the
suffering child’s life if it is not treated in time. The symptoms of DKA includes
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 5
Hyperglycemia- polydipsia, polyuria, nocturia, muscle cramps and pain and rapid weight
loss are noticed.
Acidosis and dehydration- abdominal pain can be so intense, the patient may require
surgical emergency (Watts and Edge, 2014). Shortness of breath are easily
underestimated with primary respiratory problems. In extreme cases the condition can
lead confusion and coma with unrecognized head injury.
Cerebral oedema- it is one of the major complications that occur in paediatric patients
with diabetes mellitus. As per a recent research, it is said that viability of cerebral oedema
varies. In most cases it appears in 4-12 hours after treatment gets started. Initially it would
be seen that the child is improving his health but all of a sudden his health condition
begins to deteriorate. Symptoms included dilated and fixed pupils, increasing coma and
lastly he dies with respiratory arrest. Occasionally cerebral oedema arises before
treatment begins. Ghetti et al (2010) told that the neurologic status of the children going
under treatment must be monitored frequently so that early changes can be detected. The
clinical signs of cerebral oedema can be categorised into three divisions-
1. Diagnostic criteria- symptoms includes decerebrate posture, cranial nerve palsy,
abnormal verbal or motor response to pain, abnormal neurogenic breathing pattern like
Cheyne-Stokes, apneusis.
2. Major criteria- includes fluctuating consciousness, altered mentation, inappropriate
bradycardia and incontinence which is not age appropriate.
3. Minor criteria- includes abnormal drowsiness, headache, vomiting and diastolic
hypertension (>90 mm Hg).
Hyperglycemia- polydipsia, polyuria, nocturia, muscle cramps and pain and rapid weight
loss are noticed.
Acidosis and dehydration- abdominal pain can be so intense, the patient may require
surgical emergency (Watts and Edge, 2014). Shortness of breath are easily
underestimated with primary respiratory problems. In extreme cases the condition can
lead confusion and coma with unrecognized head injury.
Cerebral oedema- it is one of the major complications that occur in paediatric patients
with diabetes mellitus. As per a recent research, it is said that viability of cerebral oedema
varies. In most cases it appears in 4-12 hours after treatment gets started. Initially it would
be seen that the child is improving his health but all of a sudden his health condition
begins to deteriorate. Symptoms included dilated and fixed pupils, increasing coma and
lastly he dies with respiratory arrest. Occasionally cerebral oedema arises before
treatment begins. Ghetti et al (2010) told that the neurologic status of the children going
under treatment must be monitored frequently so that early changes can be detected. The
clinical signs of cerebral oedema can be categorised into three divisions-
1. Diagnostic criteria- symptoms includes decerebrate posture, cranial nerve palsy,
abnormal verbal or motor response to pain, abnormal neurogenic breathing pattern like
Cheyne-Stokes, apneusis.
2. Major criteria- includes fluctuating consciousness, altered mentation, inappropriate
bradycardia and incontinence which is not age appropriate.
3. Minor criteria- includes abnormal drowsiness, headache, vomiting and diastolic
hypertension (>90 mm Hg).
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 6
4. Interventions
Now, with this increasing rate of DKA in US, the researchers have identified various
treatment and interventions which can manage this condition and can prevent the patient from
falling victim of cerebral oedema. The initial principals of resuscitation in this treatment
approaches contains airway, breathing and circulation or ABCs (Rosenbloom et al., 2010).
Children are to be treated with close observation and monitoring so that any small changes do
not get unnoticed.
As per a recent study conducted by a group of researchers, it is said that Fluid, insulin and
electrolyte replacement are essential for treating diabetic ketoacidosis. As per the research of
(Savage et al., 2011), with the initiation of the treatment of this disease, the child experiences
extensive loss of fluid due to high blood sugar levels and his condition can deteriorate. Strict
measurement has to be undertaken at this phase so that essential fluids can be restored.
Continuous subcutaneous insulin infusion therapy must not be administered to the child with
an insulin pump when treatment of DKA will go on.
The researchers has suggested some approach consideration during treatment of DKA and
these will be discussed below-
Inpatient care-
Children having altered consciousness due to severe acidosis (pH <7.1) should attain care
from paediatric intensive care unit. The patient after making recovery should be guided by
diabetes team who can educate the patient and his family about managing diabetes and its
complications. The patient when comes round from DKA will require subcutaneous insulin
therapy.
4. Interventions
Now, with this increasing rate of DKA in US, the researchers have identified various
treatment and interventions which can manage this condition and can prevent the patient from
falling victim of cerebral oedema. The initial principals of resuscitation in this treatment
approaches contains airway, breathing and circulation or ABCs (Rosenbloom et al., 2010).
Children are to be treated with close observation and monitoring so that any small changes do
not get unnoticed.
As per a recent study conducted by a group of researchers, it is said that Fluid, insulin and
electrolyte replacement are essential for treating diabetic ketoacidosis. As per the research of
(Savage et al., 2011), with the initiation of the treatment of this disease, the child experiences
extensive loss of fluid due to high blood sugar levels and his condition can deteriorate. Strict
measurement has to be undertaken at this phase so that essential fluids can be restored.
Continuous subcutaneous insulin infusion therapy must not be administered to the child with
an insulin pump when treatment of DKA will go on.
The researchers has suggested some approach consideration during treatment of DKA and
these will be discussed below-
Inpatient care-
Children having altered consciousness due to severe acidosis (pH <7.1) should attain care
from paediatric intensive care unit. The patient after making recovery should be guided by
diabetes team who can educate the patient and his family about managing diabetes and its
complications. The patient when comes round from DKA will require subcutaneous insulin
therapy.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Diabetic Ketoacidosis (DKA) and Cerebral Oedema 7
Outpatient care-
This type of care is provided by the paediatric diabetes care management team and it includes
consultations, diets, and guidelines to tackle this condition of DKA.
Fluid replacement-
There has been extensive researches regarding fluid replacement. Various approaches had
been conducted over the years and various researchers had proposed various regimes also but
among all of them the best result was obtained only by using isotonic sodium chloride
solution or half strength sodium chloride solution during first replacement and resuscitation
(Vavilala et al., 2010). This mechanism is safe and efficient and it corrects fluid deficit over
2days and unlike rapid rehydration is a gradual and a steady process which requires following
regimens to be taken under consideration by the doctors before administering this
mechanism. The regimens are as follows-
1. The fluid deficit has to be calculated by clinical assessment or by measuring the degree of
weight loss to a maximum 8% of body weight.
2. A child having excessive acidosis can be administered with 10-20 ml/kg of isotonic
sodium chloride solution (0.9%) for over 30 minutes.
3. The amount of initial resuscitation fluid boluses given to the child must be subtracted
from the total calculated deficit.
4. The fluid deficit must be corrected gradually for over 48 hours with provision of normal
maintenance liquid along with calculated deficit after resuscitation.
5. Isotonic sodium chloride solution must be administered until blood glucose levels drops
to 250-300 mg/dL (Glaser et al., 2013). Just at this time fluids containing glucose must be
introduced (5% glucose with 0.45% saline or 5% glucose with 0.9% saline). This
administration of dextrose saline must be continued until the child comes back to normal
state to have drinks and foods in a normal manner.
Outpatient care-
This type of care is provided by the paediatric diabetes care management team and it includes
consultations, diets, and guidelines to tackle this condition of DKA.
Fluid replacement-
There has been extensive researches regarding fluid replacement. Various approaches had
been conducted over the years and various researchers had proposed various regimes also but
among all of them the best result was obtained only by using isotonic sodium chloride
solution or half strength sodium chloride solution during first replacement and resuscitation
(Vavilala et al., 2010). This mechanism is safe and efficient and it corrects fluid deficit over
2days and unlike rapid rehydration is a gradual and a steady process which requires following
regimens to be taken under consideration by the doctors before administering this
mechanism. The regimens are as follows-
1. The fluid deficit has to be calculated by clinical assessment or by measuring the degree of
weight loss to a maximum 8% of body weight.
2. A child having excessive acidosis can be administered with 10-20 ml/kg of isotonic
sodium chloride solution (0.9%) for over 30 minutes.
3. The amount of initial resuscitation fluid boluses given to the child must be subtracted
from the total calculated deficit.
4. The fluid deficit must be corrected gradually for over 48 hours with provision of normal
maintenance liquid along with calculated deficit after resuscitation.
5. Isotonic sodium chloride solution must be administered until blood glucose levels drops
to 250-300 mg/dL (Glaser et al., 2013). Just at this time fluids containing glucose must be
introduced (5% glucose with 0.45% saline or 5% glucose with 0.9% saline). This
administration of dextrose saline must be continued until the child comes back to normal
state to have drinks and foods in a normal manner.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 8
6. Now, if cerebral oedema disrupts the process, the fluid replacement has to be restricted to
2/3rd of normal maintenance and the process of fluid replacement must be continued for
48 hours and longer.
7. It is normally not necessary to replace the loss of fluid but fluid balance must be strictly
assessed (Vavilala et al., 2010).
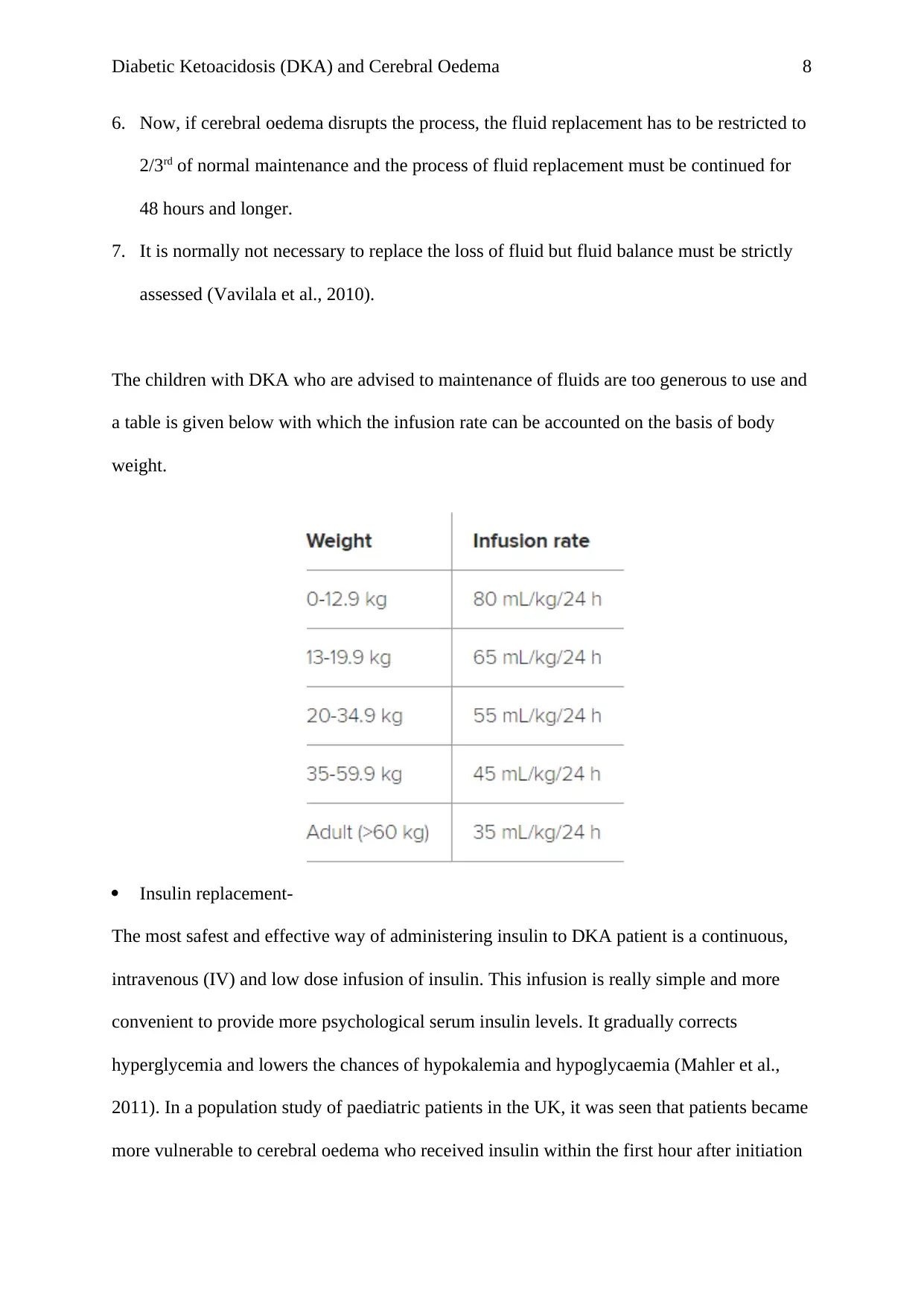
The children with DKA who are advised to maintenance of fluids are too generous to use and
a table is given below with which the infusion rate can be accounted on the basis of body
weight.
Insulin replacement-
The most safest and effective way of administering insulin to DKA patient is a continuous,
intravenous (IV) and low dose infusion of insulin. This infusion is really simple and more
convenient to provide more psychological serum insulin levels. It gradually corrects
hyperglycemia and lowers the chances of hypokalemia and hypoglycaemia (Mahler et al.,
2011). In a population study of paediatric patients in the UK, it was seen that patients became
more vulnerable to cerebral oedema who received insulin within the first hour after initiation
6. Now, if cerebral oedema disrupts the process, the fluid replacement has to be restricted to
2/3rd of normal maintenance and the process of fluid replacement must be continued for
48 hours and longer.
7. It is normally not necessary to replace the loss of fluid but fluid balance must be strictly
assessed (Vavilala et al., 2010).
The children with DKA who are advised to maintenance of fluids are too generous to use and
a table is given below with which the infusion rate can be accounted on the basis of body
weight.
Insulin replacement-
The most safest and effective way of administering insulin to DKA patient is a continuous,
intravenous (IV) and low dose infusion of insulin. This infusion is really simple and more
convenient to provide more psychological serum insulin levels. It gradually corrects
hyperglycemia and lowers the chances of hypokalemia and hypoglycaemia (Mahler et al.,
2011). In a population study of paediatric patients in the UK, it was seen that patients became
more vulnerable to cerebral oedema who received insulin within the first hour after initiation
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 9
of their treatment. Now with this instance as a guide, the researcher suggested to start insulin
therapy an hour after fluid retention comes to a prudent state, especially for those who are
newly diagnosed with DKA.
Now, still there is a huge debate regarding the infusion of correct dose of insulin in treating
DKA. Generally 0.1U/kg/h is administered but Chua et al (2010) in his recent research
suggested that a lower dose of 0.05U/kg/h is sufficient to prevent gluconeogenesis and it also
delays the fall of blood glucose levels.
The researchers claimed that blood glucose levels doesn’t drop down faster than
90mg%/hour. As the blood glucose level lowers, the infusion rate of insulin has to be lowered
too but it should not go below 0.05U/kg/h so that ketosis doesn’t reappear again (Al and
Shann, 2011). This infusion must not be disrupted until the child has recovered his
subcutaneous insulin. When blood glucose levels will fall below 120 mg % then
concentration of infused glucose has to be increased to prevent hypoglycaemia. Insulin
infusions if prolonged for more than 36 hours then ketosis gets cleared more quickly.
Children who are suffering from mild to moderate ketoacidosis are able to bear oral fluids
and they are subjected to hourly subcutaneous injections. They are given fast acting analogue
insulin (0.1U/kg. it is regarded as an effective IV insulin.
Electrolyte Replacement
Potassium- patients suffering from DKA always suffer from low potassium. If renal output of
a patients is maintained after initial resuscitation and if it is seen that plasma levels are lower
than 5 mEq/L then potassium must be added to all replacement fluids (Klingensmith et al.,
2013).
of their treatment. Now with this instance as a guide, the researcher suggested to start insulin
therapy an hour after fluid retention comes to a prudent state, especially for those who are
newly diagnosed with DKA.
Now, still there is a huge debate regarding the infusion of correct dose of insulin in treating
DKA. Generally 0.1U/kg/h is administered but Chua et al (2010) in his recent research
suggested that a lower dose of 0.05U/kg/h is sufficient to prevent gluconeogenesis and it also
delays the fall of blood glucose levels.
The researchers claimed that blood glucose levels doesn’t drop down faster than
90mg%/hour. As the blood glucose level lowers, the infusion rate of insulin has to be lowered
too but it should not go below 0.05U/kg/h so that ketosis doesn’t reappear again (Al and
Shann, 2011). This infusion must not be disrupted until the child has recovered his
subcutaneous insulin. When blood glucose levels will fall below 120 mg % then
concentration of infused glucose has to be increased to prevent hypoglycaemia. Insulin
infusions if prolonged for more than 36 hours then ketosis gets cleared more quickly.
Children who are suffering from mild to moderate ketoacidosis are able to bear oral fluids
and they are subjected to hourly subcutaneous injections. They are given fast acting analogue
insulin (0.1U/kg. it is regarded as an effective IV insulin.
Electrolyte Replacement
Potassium- patients suffering from DKA always suffer from low potassium. If renal output of
a patients is maintained after initial resuscitation and if it is seen that plasma levels are lower
than 5 mEq/L then potassium must be added to all replacement fluids (Klingensmith et al.,
2013).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 10
Bicarbonate – there has been a great debate during positive and negative effects of
bicarbonate administration to DKA patients as there is no evidence which says that IV
sodium bicarbonate improves a patient’s health status rather the evidences show that IV
bicarbonate results in deterioration of DKA and delays recovery.
Treatment of cerebral oedema
When a patient is suspected with cerebral oedema and when hypoglycaemia gets excluded,
effective and adequate treatment with an osmotic diuretic must be administered. It is then
followed by a CT scan and the patients gets referred to a neurosurgeon. The patient remains
in hyperventilation, intubation and intracranial pressure. All these improves the patient’s
health status.
As per Foster et al (2011), manitol is the most common osmotic diuretic. But there are
experimental reasons found in the present researches regarding use of 3% hypertonic saline.
Yaneva et al (2016) told that usually the amount of manitol that is used to treat cerebral
oedema is generally 0.5-1 g/kg and this infusion continues for more than 30 minutes. This
infusion can be repeated after an hour if necessary. After this infusion 5-10mL/kg hypertonic
saline is administered for over 30 minutes and this can again be repeated after one hour.
Research shows that extreme signs of deterioration are seen in half of the paediatric patients
who suffer from cerebral oedema due to DKA. Young children are more prone to respiratory
arrest and their outcomes are naturally devastating. A research of United Kingdom study
shows that children who faced respiratory arrest either died or are left with neurologic
problems which cannot be abolished totally.
Monitoring
Like it is mentioned above, monitoring forms an important part of treatment of the paediatrics
patient suffering from DKA and cerebral oedema. All the details of the health status must be
Bicarbonate – there has been a great debate during positive and negative effects of
bicarbonate administration to DKA patients as there is no evidence which says that IV
sodium bicarbonate improves a patient’s health status rather the evidences show that IV
bicarbonate results in deterioration of DKA and delays recovery.
Treatment of cerebral oedema
When a patient is suspected with cerebral oedema and when hypoglycaemia gets excluded,
effective and adequate treatment with an osmotic diuretic must be administered. It is then
followed by a CT scan and the patients gets referred to a neurosurgeon. The patient remains
in hyperventilation, intubation and intracranial pressure. All these improves the patient’s
health status.
As per Foster et al (2011), manitol is the most common osmotic diuretic. But there are
experimental reasons found in the present researches regarding use of 3% hypertonic saline.
Yaneva et al (2016) told that usually the amount of manitol that is used to treat cerebral
oedema is generally 0.5-1 g/kg and this infusion continues for more than 30 minutes. This
infusion can be repeated after an hour if necessary. After this infusion 5-10mL/kg hypertonic
saline is administered for over 30 minutes and this can again be repeated after one hour.
Research shows that extreme signs of deterioration are seen in half of the paediatric patients
who suffer from cerebral oedema due to DKA. Young children are more prone to respiratory
arrest and their outcomes are naturally devastating. A research of United Kingdom study
shows that children who faced respiratory arrest either died or are left with neurologic
problems which cannot be abolished totally.
Monitoring
Like it is mentioned above, monitoring forms an important part of treatment of the paediatrics
patient suffering from DKA and cerebral oedema. All the details of the health status must be
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 11
monitored with great attention for a good outcome. As per Patel et al (2016), status must be
monitored carefully so that complications from hypokalemia can be avoided.
If adequate monitoring is continued, hypoglycaemia cannot result but if glucose falls below
200 mg/dL then insulin infusion together with dextrose is administered.
As mentioned earlier cerebral oedema results after imitation of DKA treatment and the
symptoms get noticed after several hours of insulin infusion and administration with
intravenous fluids. Recent researches also show that majority of paediatric patient with DKA
have mild subclinical cerebral oedema (Rosenbloom, 2010). As per a recent research the
children who are suffering from severe acidosis, dehydration and severe hypocapnia are
viable to cerebral oedema. The risk intensifies when blood glucose levels fall in DKA
treatment. These chances are more common to the younger children although there remains a
huge confusion regarding DKA related cerebral oedema. Earlier, many investigators declared
that decline in serum osmolality from intensive infusion of hypotonic intravenous fluids
results in cerebral oedema but data accumulated from clinical and laboratory studies don’t
suggest so. Parmar et al (2017) completely refused this connection of osmolality and cerebral
oedema. The recent research shows that cerebral hypoperfusion before initiation of DKA
treatment may lead to cerebral oedema. Moreover cerebral oedema is also connected with
additional injury related to reperfusion which occur when the patients are administered with
the infusion of intravenous fluids and insulin. Very recent studies also claimed that if a
patient has elevated amount of inflammatory mediators or other substances affecting blood
brain barrier then his condition will lead to cerebral oedema.
5. Conclusion
Now in conclusion it can be said that as even now also it is unclear about how to prevent
DKA related cerebral oedema in paediatric patients. A large group of researchers are still
monitored with great attention for a good outcome. As per Patel et al (2016), status must be
monitored carefully so that complications from hypokalemia can be avoided.
If adequate monitoring is continued, hypoglycaemia cannot result but if glucose falls below
200 mg/dL then insulin infusion together with dextrose is administered.
As mentioned earlier cerebral oedema results after imitation of DKA treatment and the
symptoms get noticed after several hours of insulin infusion and administration with
intravenous fluids. Recent researches also show that majority of paediatric patient with DKA
have mild subclinical cerebral oedema (Rosenbloom, 2010). As per a recent research the
children who are suffering from severe acidosis, dehydration and severe hypocapnia are
viable to cerebral oedema. The risk intensifies when blood glucose levels fall in DKA
treatment. These chances are more common to the younger children although there remains a
huge confusion regarding DKA related cerebral oedema. Earlier, many investigators declared
that decline in serum osmolality from intensive infusion of hypotonic intravenous fluids
results in cerebral oedema but data accumulated from clinical and laboratory studies don’t
suggest so. Parmar et al (2017) completely refused this connection of osmolality and cerebral
oedema. The recent research shows that cerebral hypoperfusion before initiation of DKA
treatment may lead to cerebral oedema. Moreover cerebral oedema is also connected with
additional injury related to reperfusion which occur when the patients are administered with
the infusion of intravenous fluids and insulin. Very recent studies also claimed that if a
patient has elevated amount of inflammatory mediators or other substances affecting blood
brain barrier then his condition will lead to cerebral oedema.
5. Conclusion
Now in conclusion it can be said that as even now also it is unclear about how to prevent
DKA related cerebral oedema in paediatric patients. A large group of researchers are still
Diabetic Ketoacidosis (DKA) and Cerebral Oedema 12
investigating into its depth. Some claims that DKA related oedma can be prevented by using
particular intravenous fluids like insulin during ongoing treatment of DKA. This study is
undertaken by the Paediatric Emergency Care Applied Research Network FLUID study but
the result is still known as the research has not yet concluded a result (Yaneva et al., 2016).
As the severity of cerebral oedema due to DKA remains a terror both in US and in UK, the
treatment of the patients must be initiated with prompt recognition of DKA. Children
suffering from diabetes must be educated and their parents must also be made knowledgeable
enough regarding preventing its complications. They should be made aware of the ketosis and
its required treatment. They also must be made aware to undergo treatment after detection of
ketosis and with no further delay.
investigating into its depth. Some claims that DKA related oedma can be prevented by using
particular intravenous fluids like insulin during ongoing treatment of DKA. This study is
undertaken by the Paediatric Emergency Care Applied Research Network FLUID study but
the result is still known as the research has not yet concluded a result (Yaneva et al., 2016).
As the severity of cerebral oedema due to DKA remains a terror both in US and in UK, the
treatment of the patients must be initiated with prompt recognition of DKA. Children
suffering from diabetes must be educated and their parents must also be made knowledgeable
enough regarding preventing its complications. They should be made aware of the ketosis and
its required treatment. They also must be made aware to undergo treatment after detection of
ketosis and with no further delay.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.