BSD113 Economics: Evaluating Child Immunisation Policies in Australia
VerifiedAdded on 2023/04/22
|9
|2140
|105
Report
AI Summary
This report provides an overview of child immunisation rates in Australia, examining government policies and their impact on public health. It references economic theories related to welfare and externalities to analyze the effectiveness of current immunisation programs, including the 'No Jab No Pay' policy. The report critically assesses the recent trends in immunisation coverage, highlighting a decline after 2017, and proposes policy recommendations such as penalties for non-compliant centres and awareness campaigns to improve vaccination rates. It further discusses the ethical considerations of exclusionary policies and suggests a quota policy to balance social benefits and costs, aiming to achieve optimal immunisation coverage in Australia.
1
BSD113 ECONOMICS: ASSESSMENT ITEM TWO
BSD113 ECONOMICS: ASSESSMENT ITEM TWO
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
Contents
Introduction................................................................................................................................3
Part A- Overview of child immunisation rate in Australia........................................................3
Part B- Economic theory that links the policy with efficiency..................................................4
Part C- Critical analysis.............................................................................................................5
Conclusion..................................................................................................................................5
Reference....................................................................................................................................7
Contents
Introduction................................................................................................................................3
Part A- Overview of child immunisation rate in Australia........................................................3
Part B- Economic theory that links the policy with efficiency..................................................4
Part C- Critical analysis.............................................................................................................5
Conclusion..................................................................................................................................5
Reference....................................................................................................................................7
3
Introduction
Immunisation is a process to protect the citizen of the country from various diseases. This is
important to maintain a healthy and productive labour force in the future. The government
provides free vaccines for different diseases to different age group to make sure it does not
harm the health of the people. The government also carries out a regular revision of the
policies to incorporate new diseases and the use of technology. However, despite the efforts,
the government has hardly made any impact in terms of the result. The aim of this paper is to
discuss the immunisation policies of the government referring different economy theories that
bring about efficiency in the economy.
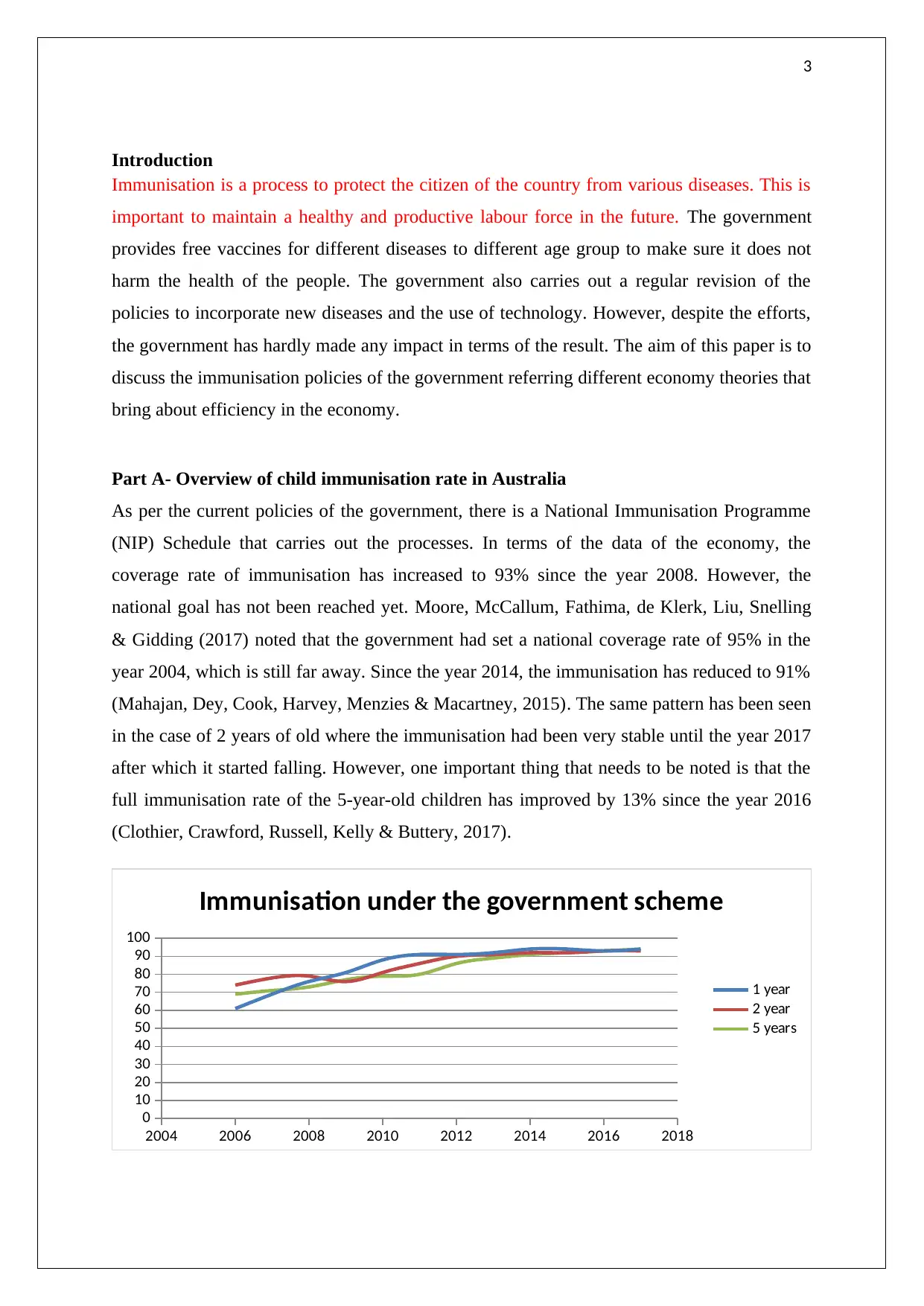
Part A- Overview of child immunisation rate in Australia
As per the current policies of the government, there is a National Immunisation Programme
(NIP) Schedule that carries out the processes. In terms of the data of the economy, the
coverage rate of immunisation has increased to 93% since the year 2008. However, the
national goal has not been reached yet. Moore, McCallum, Fathima, de Klerk, Liu, Snelling
& Gidding (2017) noted that the government had set a national coverage rate of 95% in the
year 2004, which is still far away. Since the year 2014, the immunisation has reduced to 91%
(Mahajan, Dey, Cook, Harvey, Menzies & Macartney, 2015). The same pattern has been seen
in the case of 2 years of old where the immunisation had been very stable until the year 2017
after which it started falling. However, one important thing that needs to be noted is that the
full immunisation rate of the 5-year-old children has improved by 13% since the year 2016
(Clothier, Crawford, Russell, Kelly & Buttery, 2017).
2004 2006 2008 2010 2012 2014 2016 2018
0
10
20
30
40
50
60
70
80
90
100
Immunisation under the government scheme
1 year
2 year
5 years
Introduction
Immunisation is a process to protect the citizen of the country from various diseases. This is
important to maintain a healthy and productive labour force in the future. The government
provides free vaccines for different diseases to different age group to make sure it does not
harm the health of the people. The government also carries out a regular revision of the
policies to incorporate new diseases and the use of technology. However, despite the efforts,
the government has hardly made any impact in terms of the result. The aim of this paper is to
discuss the immunisation policies of the government referring different economy theories that
bring about efficiency in the economy.
Part A- Overview of child immunisation rate in Australia
As per the current policies of the government, there is a National Immunisation Programme
(NIP) Schedule that carries out the processes. In terms of the data of the economy, the
coverage rate of immunisation has increased to 93% since the year 2008. However, the
national goal has not been reached yet. Moore, McCallum, Fathima, de Klerk, Liu, Snelling
& Gidding (2017) noted that the government had set a national coverage rate of 95% in the
year 2004, which is still far away. Since the year 2014, the immunisation has reduced to 91%
(Mahajan, Dey, Cook, Harvey, Menzies & Macartney, 2015). The same pattern has been seen
in the case of 2 years of old where the immunisation had been very stable until the year 2017
after which it started falling. However, one important thing that needs to be noted is that the
full immunisation rate of the 5-year-old children has improved by 13% since the year 2016
(Clothier, Crawford, Russell, Kelly & Buttery, 2017).
2004 2006 2008 2010 2012 2014 2016 2018
0
10
20
30
40
50
60
70
80
90
100
Immunisation under the government scheme
1 year
2 year
5 years
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
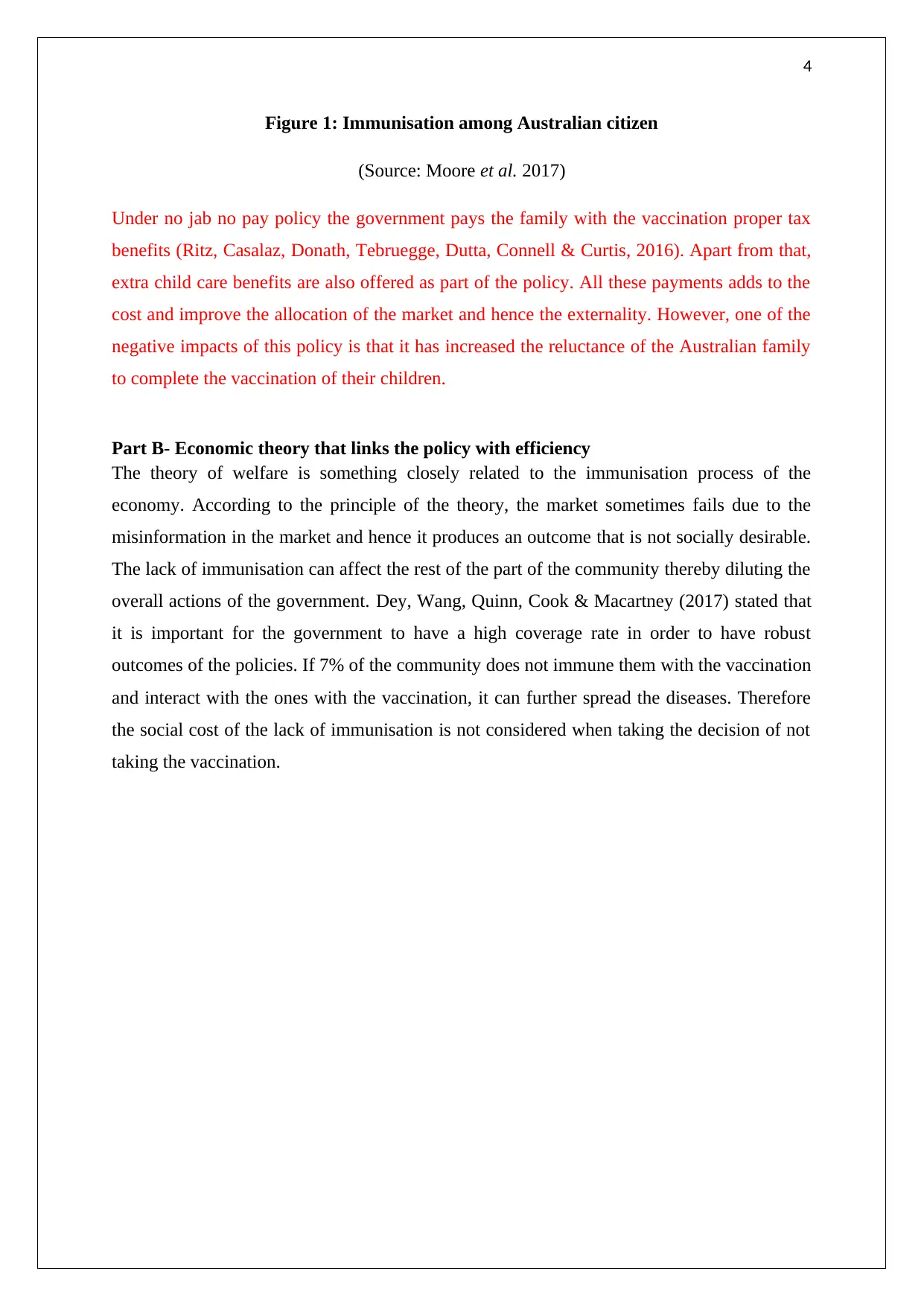
Figure 1: Immunisation among Australian citizen
(Source: Moore et al. 2017)
Under no jab no pay policy the government pays the family with the vaccination proper tax
benefits (Ritz, Casalaz, Donath, Tebruegge, Dutta, Connell & Curtis, 2016). Apart from that,
extra child care benefits are also offered as part of the policy. All these payments adds to the
cost and improve the allocation of the market and hence the externality. However, one of the
negative impacts of this policy is that it has increased the reluctance of the Australian family
to complete the vaccination of their children.
Part B- Economic theory that links the policy with efficiency
The theory of welfare is something closely related to the immunisation process of the
economy. According to the principle of the theory, the market sometimes fails due to the
misinformation in the market and hence it produces an outcome that is not socially desirable.
The lack of immunisation can affect the rest of the part of the community thereby diluting the
overall actions of the government. Dey, Wang, Quinn, Cook & Macartney (2017) stated that
it is important for the government to have a high coverage rate in order to have robust
outcomes of the policies. If 7% of the community does not immune them with the vaccination
and interact with the ones with the vaccination, it can further spread the diseases. Therefore
the social cost of the lack of immunisation is not considered when taking the decision of not
taking the vaccination.
Figure 1: Immunisation among Australian citizen
(Source: Moore et al. 2017)
Under no jab no pay policy the government pays the family with the vaccination proper tax
benefits (Ritz, Casalaz, Donath, Tebruegge, Dutta, Connell & Curtis, 2016). Apart from that,
extra child care benefits are also offered as part of the policy. All these payments adds to the
cost and improve the allocation of the market and hence the externality. However, one of the
negative impacts of this policy is that it has increased the reluctance of the Australian family
to complete the vaccination of their children.
Part B- Economic theory that links the policy with efficiency
The theory of welfare is something closely related to the immunisation process of the
economy. According to the principle of the theory, the market sometimes fails due to the
misinformation in the market and hence it produces an outcome that is not socially desirable.
The lack of immunisation can affect the rest of the part of the community thereby diluting the
overall actions of the government. Dey, Wang, Quinn, Cook & Macartney (2017) stated that
it is important for the government to have a high coverage rate in order to have robust
outcomes of the policies. If 7% of the community does not immune them with the vaccination
and interact with the ones with the vaccination, it can further spread the diseases. Therefore
the social cost of the lack of immunisation is not considered when taking the decision of not
taking the vaccination.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
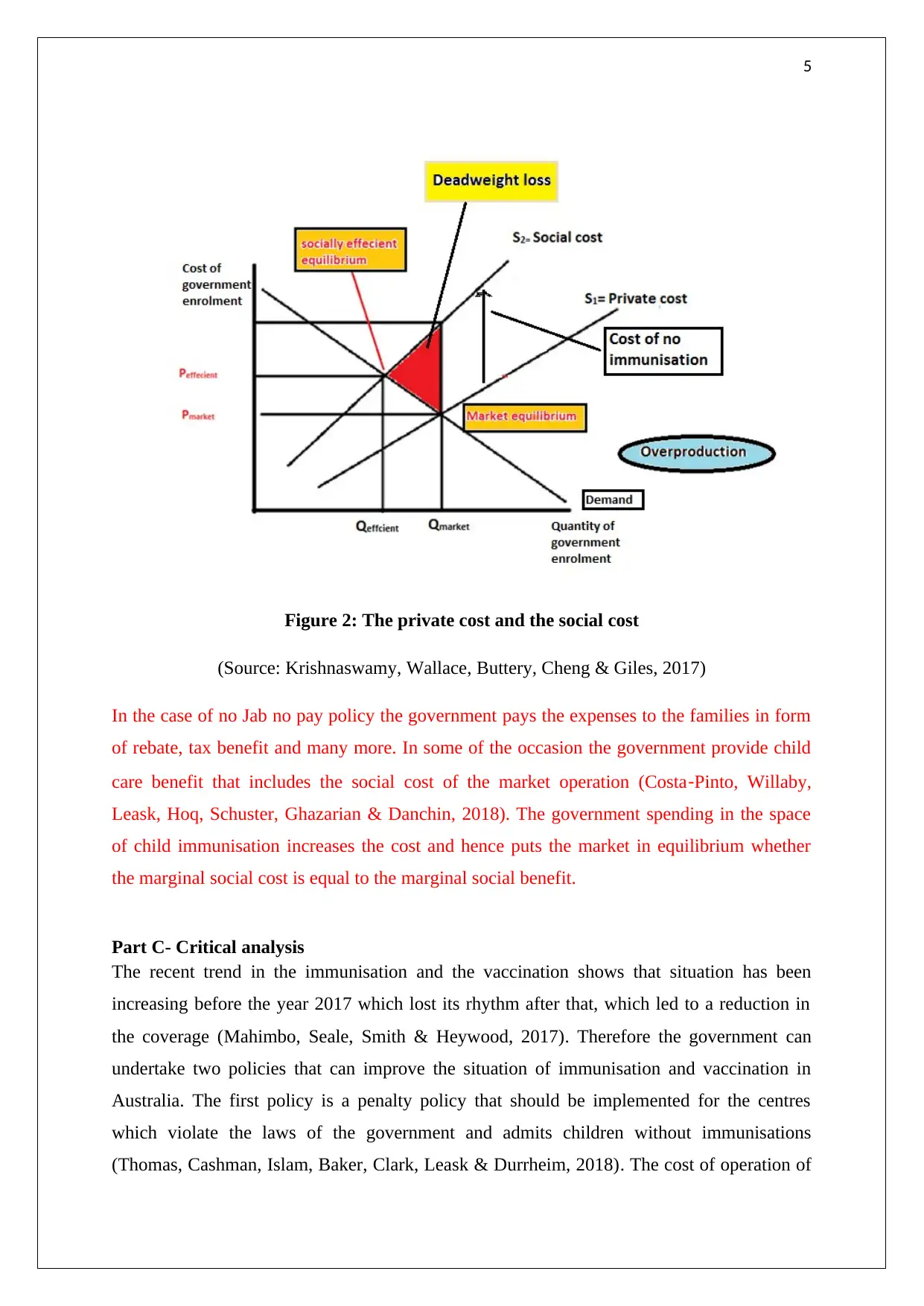
Figure 2: The private cost and the social cost
(Source: Krishnaswamy, Wallace, Buttery, Cheng & Giles, 2017)
In the case of no Jab no pay policy the government pays the expenses to the families in form
of rebate, tax benefit and many more. In some of the occasion the government provide child
care benefit that includes the social cost of the market operation (Costa‐Pinto, Willaby,
Leask, Hoq, Schuster, Ghazarian & Danchin, 2018). The government spending in the space
of child immunisation increases the cost and hence puts the market in equilibrium whether
the marginal social cost is equal to the marginal social benefit.
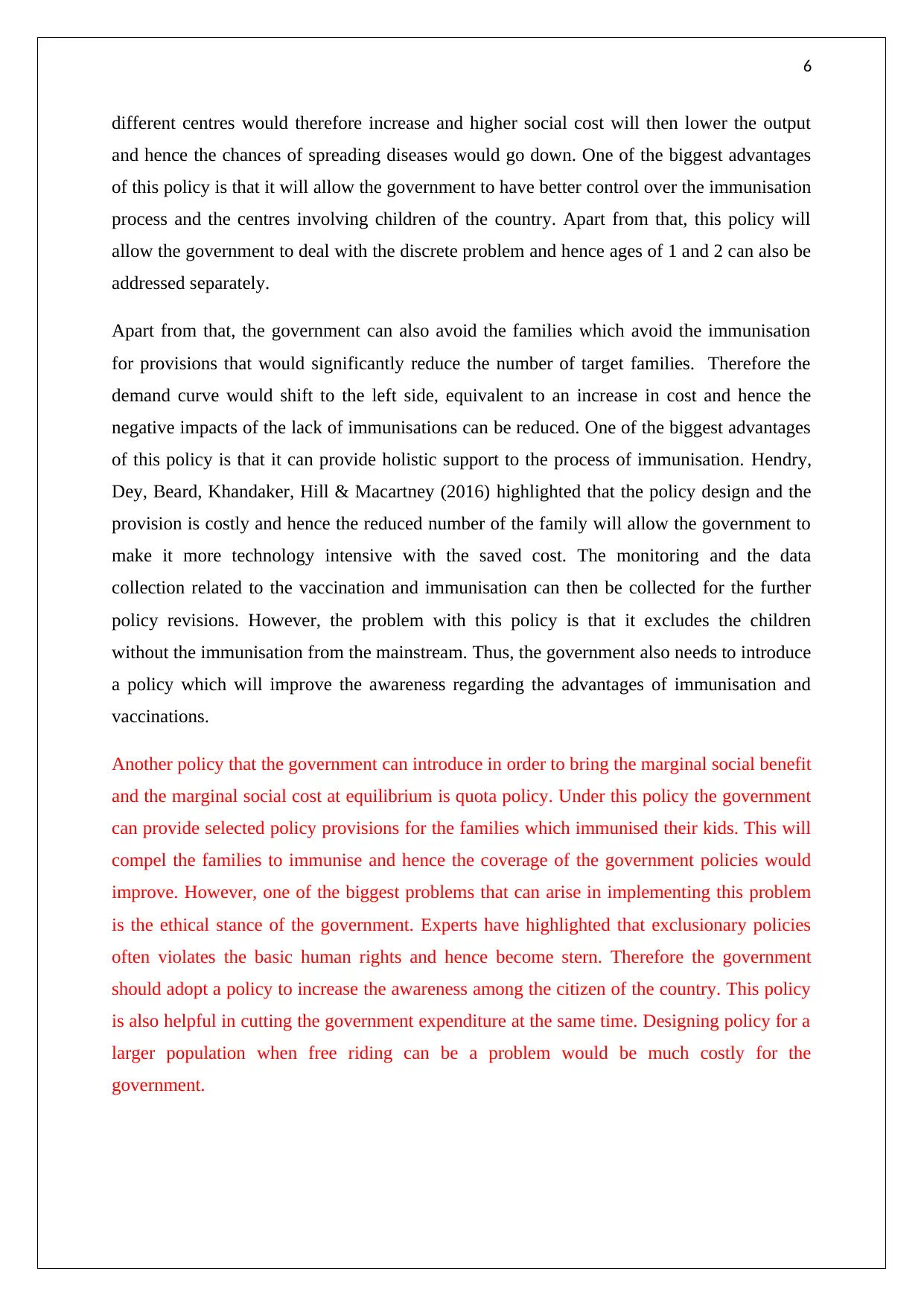
Part C- Critical analysis
The recent trend in the immunisation and the vaccination shows that situation has been
increasing before the year 2017 which lost its rhythm after that, which led to a reduction in
the coverage (Mahimbo, Seale, Smith & Heywood, 2017). Therefore the government can
undertake two policies that can improve the situation of immunisation and vaccination in
Australia. The first policy is a penalty policy that should be implemented for the centres
which violate the laws of the government and admits children without immunisations
(Thomas, Cashman, Islam, Baker, Clark, Leask & Durrheim, 2018). The cost of operation of
Figure 2: The private cost and the social cost
(Source: Krishnaswamy, Wallace, Buttery, Cheng & Giles, 2017)
In the case of no Jab no pay policy the government pays the expenses to the families in form
of rebate, tax benefit and many more. In some of the occasion the government provide child
care benefit that includes the social cost of the market operation (Costa‐Pinto, Willaby,
Leask, Hoq, Schuster, Ghazarian & Danchin, 2018). The government spending in the space
of child immunisation increases the cost and hence puts the market in equilibrium whether
the marginal social cost is equal to the marginal social benefit.
Part C- Critical analysis
The recent trend in the immunisation and the vaccination shows that situation has been
increasing before the year 2017 which lost its rhythm after that, which led to a reduction in
the coverage (Mahimbo, Seale, Smith & Heywood, 2017). Therefore the government can
undertake two policies that can improve the situation of immunisation and vaccination in
Australia. The first policy is a penalty policy that should be implemented for the centres
which violate the laws of the government and admits children without immunisations
(Thomas, Cashman, Islam, Baker, Clark, Leask & Durrheim, 2018). The cost of operation of
6
different centres would therefore increase and higher social cost will then lower the output
and hence the chances of spreading diseases would go down. One of the biggest advantages
of this policy is that it will allow the government to have better control over the immunisation
process and the centres involving children of the country. Apart from that, this policy will
allow the government to deal with the discrete problem and hence ages of 1 and 2 can also be
addressed separately.
Apart from that, the government can also avoid the families which avoid the immunisation
for provisions that would significantly reduce the number of target families. Therefore the
demand curve would shift to the left side, equivalent to an increase in cost and hence the
negative impacts of the lack of immunisations can be reduced. One of the biggest advantages
of this policy is that it can provide holistic support to the process of immunisation. Hendry,
Dey, Beard, Khandaker, Hill & Macartney (2016) highlighted that the policy design and the
provision is costly and hence the reduced number of the family will allow the government to
make it more technology intensive with the saved cost. The monitoring and the data
collection related to the vaccination and immunisation can then be collected for the further
policy revisions. However, the problem with this policy is that it excludes the children
without the immunisation from the mainstream. Thus, the government also needs to introduce
a policy which will improve the awareness regarding the advantages of immunisation and
vaccinations.
Another policy that the government can introduce in order to bring the marginal social benefit
and the marginal social cost at equilibrium is quota policy. Under this policy the government
can provide selected policy provisions for the families which immunised their kids. This will
compel the families to immunise and hence the coverage of the government policies would
improve. However, one of the biggest problems that can arise in implementing this problem
is the ethical stance of the government. Experts have highlighted that exclusionary policies
often violates the basic human rights and hence become stern. Therefore the government
should adopt a policy to increase the awareness among the citizen of the country. This policy
is also helpful in cutting the government expenditure at the same time. Designing policy for a
larger population when free riding can be a problem would be much costly for the
government.
different centres would therefore increase and higher social cost will then lower the output
and hence the chances of spreading diseases would go down. One of the biggest advantages
of this policy is that it will allow the government to have better control over the immunisation
process and the centres involving children of the country. Apart from that, this policy will
allow the government to deal with the discrete problem and hence ages of 1 and 2 can also be
addressed separately.
Apart from that, the government can also avoid the families which avoid the immunisation
for provisions that would significantly reduce the number of target families. Therefore the
demand curve would shift to the left side, equivalent to an increase in cost and hence the
negative impacts of the lack of immunisations can be reduced. One of the biggest advantages
of this policy is that it can provide holistic support to the process of immunisation. Hendry,
Dey, Beard, Khandaker, Hill & Macartney (2016) highlighted that the policy design and the
provision is costly and hence the reduced number of the family will allow the government to
make it more technology intensive with the saved cost. The monitoring and the data
collection related to the vaccination and immunisation can then be collected for the further
policy revisions. However, the problem with this policy is that it excludes the children
without the immunisation from the mainstream. Thus, the government also needs to introduce
a policy which will improve the awareness regarding the advantages of immunisation and
vaccinations.
Another policy that the government can introduce in order to bring the marginal social benefit
and the marginal social cost at equilibrium is quota policy. Under this policy the government
can provide selected policy provisions for the families which immunised their kids. This will
compel the families to immunise and hence the coverage of the government policies would
improve. However, one of the biggest problems that can arise in implementing this problem
is the ethical stance of the government. Experts have highlighted that exclusionary policies
often violates the basic human rights and hence become stern. Therefore the government
should adopt a policy to increase the awareness among the citizen of the country. This policy
is also helpful in cutting the government expenditure at the same time. Designing policy for a
larger population when free riding can be a problem would be much costly for the
government.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

7
Conclusion
Australia is among the very few countries in the world to introduce immunisation processes
at a very early stage. Due to the presence of various diseases, the government has introduced
a number of policies to mitigate the problems. The policies have worked towards the goal of
the government in the initial stages; however, with time the preferences of the Australian
families have changed which has reflected in the poor coverage of the government initiatives.
It has contributed to the negative externalities of reducing the productivity of the children of
the country. Taxing the violator is one of the major theories that are used to solve this kind of
problem. The basic notion of the theory is too compelling the violators to internalise the
social cost so that a socially optimum output can be generated. The policies furnished in the
paper also talks about how the government can mitigate the problems in line with the
theories.
Conclusion
Australia is among the very few countries in the world to introduce immunisation processes
at a very early stage. Due to the presence of various diseases, the government has introduced
a number of policies to mitigate the problems. The policies have worked towards the goal of
the government in the initial stages; however, with time the preferences of the Australian
families have changed which has reflected in the poor coverage of the government initiatives.
It has contributed to the negative externalities of reducing the productivity of the children of
the country. Taxing the violator is one of the major theories that are used to solve this kind of
problem. The basic notion of the theory is too compelling the violators to internalise the
social cost so that a socially optimum output can be generated. The policies furnished in the
paper also talks about how the government can mitigate the problems in line with the
theories.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
Reference
Clothier, H. J., Crawford, N. W., Russell, M., Kelly, H., & Buttery, J. P. (2017). Evaluation
of ‘SAEFVIC’, A Pharmacovigilance Surveillance Scheme for the Spontaneous
Reporting of Adverse Events Following Immunisation in Victoria, Australia. Drug
Safety, 40(6), 483-495.
Costa‐Pinto, J. C., Willaby, H. W., Leask, J., Hoq, M., Schuster, T., Ghazarian, A., ... &
Danchin, M. H. (2018). Parental Immunisation Needs and Attitudes Survey in
paediatric hospital clinics and community maternal and child health centres in
Melbourne, Australia. Journal of paediatrics and child health, 54(5), 522-529.
Dey, A., Wang, H., Quinn, H., Cook, J., & Macartney, K. (2017). Surveillance of adverse
events following immunisation in Australia, 2015. Communicable diseases
intelligence quarterly report, 41(3), E264-E278.
Hendry, A. J., Dey, A., Beard, F. H., Khandaker, G., Hill, R., & Macartney, K. K. (2016).
Adverse events following immunisation with bacille Calmette-Guérin vaccination:
baseline data to inform monitoring in Australia following the introduction of new
unregistered BCG vaccine. safety, 40(4), E470-E474.
Krishnaswamy, S., Wallace, E. M., Buttery, J., Cheng, A. C., & Giles, M. (2017). Protecting
newborns from pertussis: the role of cocooning in the era of maternal immunisation: a
survey of parental vaccination in melbourne, australia. American Journal of
Obstetrics and Gynecology, 217(6), 722.
Mahajan, D., Dey, A., Cook, J., Harvey, B., Menzies, R., & Macartney, K. (2015).
Surveillance of adverse events following immunisation in Australia annual report,
2013. Commun Dis Intell Q Rep, 9(3039), 3.
Mahimbo, A., Seale, H., Smith, M., & Heywood, A. (2017). Challenges in immunisation
service delivery for refugees in Australia: A health system
perspective. Vaccine, 35(38), 5148-5155.
Moore, H., McCallum, L., Fathima, P., de Klerk, N., Liu, B., Snelling, T & Gidding, H.
(2017). Linking the Australian Childhood Immunisation Register to population-based
Reference
Clothier, H. J., Crawford, N. W., Russell, M., Kelly, H., & Buttery, J. P. (2017). Evaluation
of ‘SAEFVIC’, A Pharmacovigilance Surveillance Scheme for the Spontaneous
Reporting of Adverse Events Following Immunisation in Victoria, Australia. Drug
Safety, 40(6), 483-495.
Costa‐Pinto, J. C., Willaby, H. W., Leask, J., Hoq, M., Schuster, T., Ghazarian, A., ... &
Danchin, M. H. (2018). Parental Immunisation Needs and Attitudes Survey in
paediatric hospital clinics and community maternal and child health centres in
Melbourne, Australia. Journal of paediatrics and child health, 54(5), 522-529.
Dey, A., Wang, H., Quinn, H., Cook, J., & Macartney, K. (2017). Surveillance of adverse
events following immunisation in Australia, 2015. Communicable diseases
intelligence quarterly report, 41(3), E264-E278.
Hendry, A. J., Dey, A., Beard, F. H., Khandaker, G., Hill, R., & Macartney, K. K. (2016).
Adverse events following immunisation with bacille Calmette-Guérin vaccination:
baseline data to inform monitoring in Australia following the introduction of new
unregistered BCG vaccine. safety, 40(4), E470-E474.
Krishnaswamy, S., Wallace, E. M., Buttery, J., Cheng, A. C., & Giles, M. (2017). Protecting
newborns from pertussis: the role of cocooning in the era of maternal immunisation: a
survey of parental vaccination in melbourne, australia. American Journal of
Obstetrics and Gynecology, 217(6), 722.
Mahajan, D., Dey, A., Cook, J., Harvey, B., Menzies, R., & Macartney, K. (2015).
Surveillance of adverse events following immunisation in Australia annual report,
2013. Commun Dis Intell Q Rep, 9(3039), 3.
Mahimbo, A., Seale, H., Smith, M., & Heywood, A. (2017). Challenges in immunisation
service delivery for refugees in Australia: A health system
perspective. Vaccine, 35(38), 5148-5155.
Moore, H., McCallum, L., Fathima, P., de Klerk, N., Liu, B., Snelling, T & Gidding, H.
(2017). Linking the Australian Childhood Immunisation Register to population-based

9
perinatal datasets to assess coverage in at-risk groups. International Journal of
Population Data Science, 1(1). 45-96
Ritz, N., Casalaz, D., Donath, S., Tebruegge, M., Dutta, B., Connell, T. G., ... & Curtis, N.
(2016). Comparable CD4 and CD8 T cell responses and cytokine release after at-birth
and delayed BCG immunisation in infants born in Australia. Vaccine, 34(35), 4132-
4139.
Thomas, S., Cashman, P., Islam, F., Baker, L., Clark, K., Leask, J., ... & Durrheim, D. N.
(2018). Tailoring immunisation service delivery in a disadvantaged community in
Australia; views of health providers and parents. Vaccine, 36(19), 2596-2603.
perinatal datasets to assess coverage in at-risk groups. International Journal of
Population Data Science, 1(1). 45-96
Ritz, N., Casalaz, D., Donath, S., Tebruegge, M., Dutta, B., Connell, T. G., ... & Curtis, N.
(2016). Comparable CD4 and CD8 T cell responses and cytokine release after at-birth
and delayed BCG immunisation in infants born in Australia. Vaccine, 34(35), 4132-
4139.
Thomas, S., Cashman, P., Islam, F., Baker, L., Clark, K., Leask, J., ... & Durrheim, D. N.
(2018). Tailoring immunisation service delivery in a disadvantaged community in
Australia; views of health providers and parents. Vaccine, 36(19), 2596-2603.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.