Adoption and Use of EHR and Mobile Technology in Home Health Care
VerifiedAdded on 2023/06/13
|12
|9317
|93
Report
AI Summary
This report presents national estimates on the adoption and use of electronic health records (EHR) and mobile technology by home health and hospice care agencies in 2007, examining agency characteristics associated with adoption. The study, based on data from the National Home and Hospice Care Survey (NHHCS), reveals that 28% of agencies adopted both EHR and mobile technology, while 54% adopted neither. Adoption was associated with the number of patients served and agency type, with for-profit or jointly-owned agencies less likely to adopt either technology. Among agencies with EHR, commonly used functionalities included patient demographics and clinical notes. For mobile technology, functionalities for OASIS, e-mail, and appointment scheduling were prevalent. The report also discusses the potential for improved care coordination and timely decision-making through the integration of mobile technology with EHR systems.
Number 66 n May 20, 2013
Adoption and Use of Electronic Health Records
and Mobile Technology by Home Health and
Hospice Care Agencies
by Anita R. Bercovitz, Ph.D., M.P.H.; Eunice Park-Lee, Ph.D.;
and Eric Jamoom, Ph.D., M.P.H., M.S., Division of Health Care Statistics
Abstract
Objective—This report presents national estimates on the adoption and use
of electronic health records and mobile technology by home health and hospice
care agencies, as well as the agency characteristics associated with adoption.
Methods—Estimates are based on data from the 2007 National Home and
Hospice Care Survey, conducted by the Centers for Disease Control and
Prevention’s National Center for Health Statistics.
Results—In 2007, 28% of home health and hospice care agencies adopted
both electronic health records and mobile technology, while slightly over half
(54%) adopted neither. Sixteen percent of agencies adopted only electronic health
records. Adoption of both technologies was associated with number of patients
served and agency type. Agencies that were for-profit or were jointly owned with
a hospital were more likely to have adopted neither technology. Among agencies
with electronic health records, the most commonly used functionalities were
patient demographics and clinical notes. Among agencies with mobile
technology, functionalities for the Outcome and Assessment Information Set
(OASIS), e-mail, and appointment scheduling were the most commonly used.
Similar percentages of agencies with electronic health records or mobile
technology used clinical decision support systems, computerized physician order
entry, electronic reminders for tests, and viewing of test results.
Keywords: point-of-care documentation • health information technology •
interoperability • long-term care
Introduction
Use of health information
technology, especially at the point of
care, is often considered as a way to
improve care coordination and quality
(1). Mobile technology, such as tablet
computers and personal digital
assistants, represents an opportunity to
gather information at the point of care.
Collection of information at the care site
would be especially important in home
health and hospice care, where care is
provided predominantly at the patient’s
home rather than in an institutional
setting (2,3). If the agency also has an
electronic health record for the patient,
any information collected at the point of
care through mobile technology has the
potential to be integrated into the
electronic health record, making the
information available across provider
locations. Having this information
visible across all locations of care
supports timely decision making and
documentation. For example, having the
capability to view test results at the
point of care enables the provider to use
these results to make timely decisions
about treatment. Similarly, having the
capability to order medications,
treatments, or tests at the point of care
eliminates a time lag in both ordering
and documenting the treatment. Linkage
of the information gathered through
mobile technology to the electronic
health record may facilitate timely
decisions and concordance of patient
information across locations of care.
However, the utility of having both
electronic health records and mobile
technology is dependent on both
technologies having the same
functionalities and the ability to share
information.
Although the adoption of each type
of health information technology has
been examined independently (4–6),
little information is available on the
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Centers for Disease Control and Prevention
National Center for Health Statistics
Adoption and Use of Electronic Health Records
and Mobile Technology by Home Health and
Hospice Care Agencies
by Anita R. Bercovitz, Ph.D., M.P.H.; Eunice Park-Lee, Ph.D.;
and Eric Jamoom, Ph.D., M.P.H., M.S., Division of Health Care Statistics
Abstract
Objective—This report presents national estimates on the adoption and use
of electronic health records and mobile technology by home health and hospice
care agencies, as well as the agency characteristics associated with adoption.
Methods—Estimates are based on data from the 2007 National Home and
Hospice Care Survey, conducted by the Centers for Disease Control and
Prevention’s National Center for Health Statistics.
Results—In 2007, 28% of home health and hospice care agencies adopted
both electronic health records and mobile technology, while slightly over half
(54%) adopted neither. Sixteen percent of agencies adopted only electronic health
records. Adoption of both technologies was associated with number of patients
served and agency type. Agencies that were for-profit or were jointly owned with
a hospital were more likely to have adopted neither technology. Among agencies
with electronic health records, the most commonly used functionalities were
patient demographics and clinical notes. Among agencies with mobile
technology, functionalities for the Outcome and Assessment Information Set
(OASIS), e-mail, and appointment scheduling were the most commonly used.
Similar percentages of agencies with electronic health records or mobile
technology used clinical decision support systems, computerized physician order
entry, electronic reminders for tests, and viewing of test results.
Keywords: point-of-care documentation • health information technology •
interoperability • long-term care
Introduction
Use of health information
technology, especially at the point of
care, is often considered as a way to
improve care coordination and quality
(1). Mobile technology, such as tablet
computers and personal digital
assistants, represents an opportunity to
gather information at the point of care.
Collection of information at the care site
would be especially important in home
health and hospice care, where care is
provided predominantly at the patient’s
home rather than in an institutional
setting (2,3). If the agency also has an
electronic health record for the patient,
any information collected at the point of
care through mobile technology has the
potential to be integrated into the
electronic health record, making the
information available across provider
locations. Having this information
visible across all locations of care
supports timely decision making and
documentation. For example, having the
capability to view test results at the
point of care enables the provider to use
these results to make timely decisions
about treatment. Similarly, having the
capability to order medications,
treatments, or tests at the point of care
eliminates a time lag in both ordering
and documenting the treatment. Linkage
of the information gathered through
mobile technology to the electronic
health record may facilitate timely
decisions and concordance of patient
information across locations of care.
However, the utility of having both
electronic health records and mobile
technology is dependent on both
technologies having the same
functionalities and the ability to share
information.
Although the adoption of each type
of health information technology has
been examined independently (4–6),
little information is available on the
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Centers for Disease Control and Prevention
National Center for Health Statistics
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Page 2 National Health Statistics Reports n Number 66 n May 20, 2013
adoption of multiple types of health
information within one agency and the
agency characteristics associated with
adoption of multiple types. This report
builds on previous work and presents
data on co-use of electronic health
records and mobile technology by home
health and hospice care agencies, and on
agency characteristics associated with
adoption. Estimates are also presented
for the functionalities most often used in
mobile technology and electronic health
records, and among providers with both
technologies.
Methods
Estimates in this report are based on
data from the 2007 National Home and
Hospice Care survey (NHHCS),
conducted by the Centers for Disease
Control and Prevention’s (CDC)
National Center for Health Statistics
(NCHS). The 2007 NHHCS is one in a
series of nationally representative,
cross-sectional sample surveys of U.S.
home health and hospice care agencies.
It is designed to provide descriptive
information on these agencies, their staff
members, the services they provide, and
the people they serve. NHHCS was first
conducted in 1992 and was repeated in
1993, 1994, 1996, 1998, 2000, and
2007.
Information on NHHCS sampling,
design, and other methodology is
available in the Technical Notes at the
end of this report, as well as in other
reports (7) and online at http://
www.cdc.gov/nchs/nhhcs/nhhcs_
questionnaires.htm.
Data analysis
Bivariate (bivariate cross-tabulation)
and multivariate (multivariate logistic
regression) analyses were conducted to
examine home health and hospice care
agencies’ adoption of electronic health
records and mobile technology. The
following mutually exclusive variables
were created for the analyses:
+ Agencies that adopted both electronic
health records and mobile technology.
+ Agencies that adopted only electronic
health records.
+ Agencies that adopted neither
electronic health records nor mobile
technology.
The sample size for agencies that
adopted only mobile technology was too
small to create reliable estimates. Thus,
no analyses were conducted to identify
the factors associated with adoption of
only mobile technology, and these
agencies were excluded from the
bivariate and multivariate analyses.
Bivariate cross-tabulations were
used to determine the unadjusted
percentages of agencies that adopted
both electronic health records and
mobile technology, agencies that
adopted only electronic health records,
and agencies that adopted neither
technology, by selected agency
characteristics (Table 1). Adjusted
percentages controlling for agency
characteristics were calculated using
three multivariate logistic regression
models. The first model produces the
adjusted percentage of agencies that
adopted both technologies; the second
produces the adjusted percentage of
agencies that adopted only electronic
health records; and the third model
produces the adjusted percentage of
agencies that adopted neither
technology. In each model, agencies that
adopted only mobile technology were
excluded from the analyses.
Control variables in the models
include type of care offered, total
number of services offered, percentage
of revenue from Medicare, total number
of patients, administrator or director
tenure at the agency, joint ownership,
agency type, and chain affiliation. These
variables were chosen because in
previous research they were found to be
associated with adoption of electronic
health records (4–6). The regression
models are then used to predict marginal
probabilities (adjusted percentages) for
the average provider of home health or
hospice care, or both, with a given
characteristic (e.g., for-profit agencies)
and with the specific technology
adoption status (e.g., adoption of only
electronic health records), while
controlling for other variables in the
model.
Differences between the results of
bivariate (unadjusted) and adjusted
analyses are due to the significant
associations between the variables
included in the adjusted model. For
example, chain affiliation and type of
care offered are significantly associated
(8). Because significant associations
were seen among the control variables
included in the full models, additional
models were run. One set of models
included only the variables with
significant bivariate associations. In
another series of models, the variables
with the most correlations with other
variables were dropped sequentially, in
the following order: ownership, joint
ownership, percentage of revenue from
Medicare, and type of care offered. The
results of these additional models are
discussed but are not shown.
The percentages of agency adoption
of mobile technology and electronic
health record functionalities were
calculated for the following categories:
+ Agencies that adopted mobile
technology regardless of adoption of
electronic health records.
+ Agencies that adopted electronic
health records regardless of adoption
of mobile technology.
+ Agencies that adopted both
technologies.
The weighted percentages of
nonresponse (‘‘don’t know’’ and
‘‘refused’’) for all variables used in the
analyses were less than 10%. The
weighted percentage of cases with
missing data was less than 1% for
functionalities on electronic health
records and mobile technology; 1% for
total number of patients, joint
ownership, and total number of services
offered; 5% for whether the agency had
an electronic health record; 7% for
whether the agency had mobile
technology and for administrator or
director tenure at agency; and 8% for
the percentage of revenue from
Medicare. Agency type and type of care
offered had no cases with missing data.
Cases with missing information on any
of the variables used in the analyses
were dropped (67 cases were dropped,
resulting in a sample of 969 cases being
used in the analyses). This yielded a
adoption of multiple types of health
information within one agency and the
agency characteristics associated with
adoption of multiple types. This report
builds on previous work and presents
data on co-use of electronic health
records and mobile technology by home
health and hospice care agencies, and on
agency characteristics associated with
adoption. Estimates are also presented
for the functionalities most often used in
mobile technology and electronic health
records, and among providers with both
technologies.
Methods
Estimates in this report are based on
data from the 2007 National Home and
Hospice Care survey (NHHCS),
conducted by the Centers for Disease
Control and Prevention’s (CDC)
National Center for Health Statistics
(NCHS). The 2007 NHHCS is one in a
series of nationally representative,
cross-sectional sample surveys of U.S.
home health and hospice care agencies.
It is designed to provide descriptive
information on these agencies, their staff
members, the services they provide, and
the people they serve. NHHCS was first
conducted in 1992 and was repeated in
1993, 1994, 1996, 1998, 2000, and
2007.
Information on NHHCS sampling,
design, and other methodology is
available in the Technical Notes at the
end of this report, as well as in other
reports (7) and online at http://
www.cdc.gov/nchs/nhhcs/nhhcs_
questionnaires.htm.
Data analysis
Bivariate (bivariate cross-tabulation)
and multivariate (multivariate logistic
regression) analyses were conducted to
examine home health and hospice care
agencies’ adoption of electronic health
records and mobile technology. The
following mutually exclusive variables
were created for the analyses:
+ Agencies that adopted both electronic
health records and mobile technology.
+ Agencies that adopted only electronic
health records.
+ Agencies that adopted neither
electronic health records nor mobile
technology.
The sample size for agencies that
adopted only mobile technology was too
small to create reliable estimates. Thus,
no analyses were conducted to identify
the factors associated with adoption of
only mobile technology, and these
agencies were excluded from the
bivariate and multivariate analyses.
Bivariate cross-tabulations were
used to determine the unadjusted
percentages of agencies that adopted
both electronic health records and
mobile technology, agencies that
adopted only electronic health records,
and agencies that adopted neither
technology, by selected agency
characteristics (Table 1). Adjusted
percentages controlling for agency
characteristics were calculated using
three multivariate logistic regression
models. The first model produces the
adjusted percentage of agencies that
adopted both technologies; the second
produces the adjusted percentage of
agencies that adopted only electronic
health records; and the third model
produces the adjusted percentage of
agencies that adopted neither
technology. In each model, agencies that
adopted only mobile technology were
excluded from the analyses.
Control variables in the models
include type of care offered, total
number of services offered, percentage
of revenue from Medicare, total number
of patients, administrator or director
tenure at the agency, joint ownership,
agency type, and chain affiliation. These
variables were chosen because in
previous research they were found to be
associated with adoption of electronic
health records (4–6). The regression
models are then used to predict marginal
probabilities (adjusted percentages) for
the average provider of home health or
hospice care, or both, with a given
characteristic (e.g., for-profit agencies)
and with the specific technology
adoption status (e.g., adoption of only
electronic health records), while
controlling for other variables in the
model.
Differences between the results of
bivariate (unadjusted) and adjusted
analyses are due to the significant
associations between the variables
included in the adjusted model. For
example, chain affiliation and type of
care offered are significantly associated
(8). Because significant associations
were seen among the control variables
included in the full models, additional
models were run. One set of models
included only the variables with
significant bivariate associations. In
another series of models, the variables
with the most correlations with other
variables were dropped sequentially, in
the following order: ownership, joint
ownership, percentage of revenue from
Medicare, and type of care offered. The
results of these additional models are
discussed but are not shown.
The percentages of agency adoption
of mobile technology and electronic
health record functionalities were
calculated for the following categories:
+ Agencies that adopted mobile
technology regardless of adoption of
electronic health records.
+ Agencies that adopted electronic
health records regardless of adoption
of mobile technology.
+ Agencies that adopted both
technologies.
The weighted percentages of
nonresponse (‘‘don’t know’’ and
‘‘refused’’) for all variables used in the
analyses were less than 10%. The
weighted percentage of cases with
missing data was less than 1% for
functionalities on electronic health
records and mobile technology; 1% for
total number of patients, joint
ownership, and total number of services
offered; 5% for whether the agency had
an electronic health record; 7% for
whether the agency had mobile
technology and for administrator or
director tenure at agency; and 8% for
the percentage of revenue from
Medicare. Agency type and type of care
offered had no cases with missing data.
Cases with missing information on any
of the variables used in the analyses
were dropped (67 cases were dropped,
resulting in a sample of 969 cases being
used in the analyses). This yielded a
National Health Statistics Reports n Number 66 n May 20, 2013 Page 3
weighted sample size of 13,100 cases
(91% of the total weighted sample).
Weights that take into account the
sample stages with adjustments for
nonresponse were used to produce
national estimates of agencies providing
home health and hospice care.
Differences between subgroups were
evaluated with chi-square tests at the
p = 0.05 level for differences in
percentages and percent distributions.
All comparisons reported in the text are
statistically significant unless otherwise
indicated. Comparisons not mentioned
may or may not be statistically
significant. Data analyses were
performed using the statistical packages
SAS, version 9.2 (9) and SUDAAN,
version 10.0 (10). Because estimates
were rounded to the nearest hundred,
individual estimates may not sum to
totals.
Results
Adoption of electronic health
records and mobile
technology
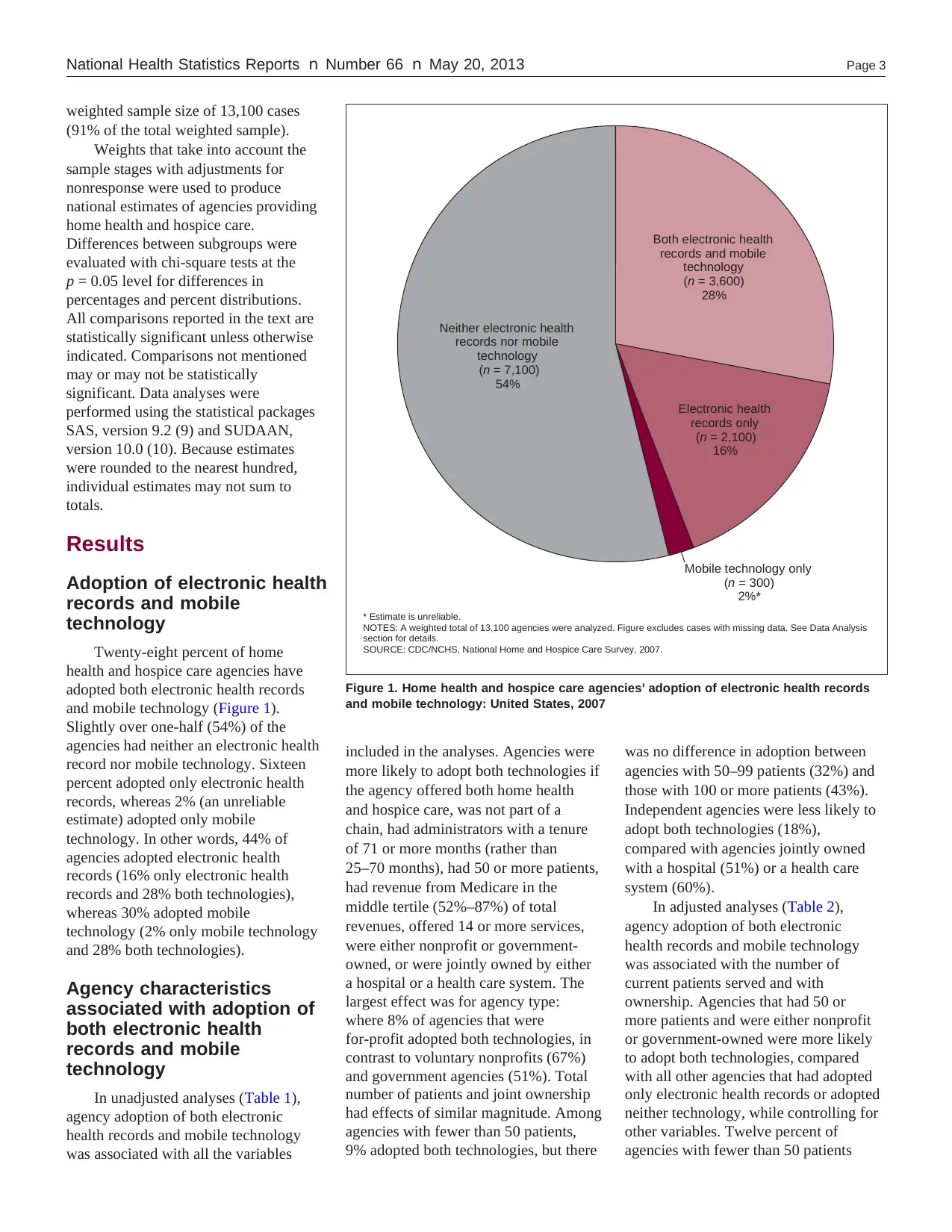
Twenty-eight percent of home
health and hospice care agencies have
adopted both electronic health records
and mobile technology (Figure 1).
Slightly over one-half (54%) of the
agencies had neither an electronic health
record nor mobile technology. Sixteen
percent adopted only electronic health
records, whereas 2% (an unreliable
estimate) adopted only mobile
technology. In other words, 44% of
agencies adopted electronic health
records (16% only electronic health
records and 28% both technologies),
whereas 30% adopted mobile
technology (2% only mobile technology
and 28% both technologies).
Agency characteristics
associated with adoption of
both electronic health
records and mobile
technology
In unadjusted analyses (Table 1),
agency adoption of both electronic
health records and mobile technology
was associated with all the variables
Electronic health
records only
(n = 2,100)
16%
Mobile technology only
(n = 300)
2%*
Both electronic health
records and mobile
technology
(n = 3,600)
28%
Neither electronic health
records nor mobile
technology
(n = 7,100)
54%
* Estimate is unreliable.
NOTES: A weighted total of 13,100 agencies were analyzed. Figure excludes cases with missing data. See Data Analysis
section for details.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Figure 1. Home health and hospice care agencies’ adoption of electronic health records
and mobile technology: United States, 2007
included in the analyses. Agencies were
more likely to adopt both technologies if
the agency offered both home health
and hospice care, was not part of a
chain, had administrators with a tenure
of 71 or more months (rather than
25–70 months), had 50 or more patients,
had revenue from Medicare in the
middle tertile (52%–87%) of total
revenues, offered 14 or more services,
were either nonprofit or government-
owned, or were jointly owned by either
a hospital or a health care system. The
largest effect was for agency type:
where 8% of agencies that were
for-profit adopted both technologies, in
contrast to voluntary nonprofits (67%)
and government agencies (51%). Total
number of patients and joint ownership
had effects of similar magnitude. Among
agencies with fewer than 50 patients,
9% adopted both technologies, but there
was no difference in adoption between
agencies with 50–99 patients (32%) and
those with 100 or more patients (43%).
Independent agencies were less likely to
adopt both technologies (18%),
compared with agencies jointly owned
with a hospital (51%) or a health care
system (60%).
In adjusted analyses (Table 2),
agency adoption of both electronic
health records and mobile technology
was associated with the number of
current patients served and with
ownership. Agencies that had 50 or
more patients and were either nonprofit
or government-owned were more likely
to adopt both technologies, compared
with all other agencies that had adopted
only electronic health records or adopted
neither technology, while controlling for
other variables. Twelve percent of
agencies with fewer than 50 patients
weighted sample size of 13,100 cases
(91% of the total weighted sample).
Weights that take into account the
sample stages with adjustments for
nonresponse were used to produce
national estimates of agencies providing
home health and hospice care.
Differences between subgroups were
evaluated with chi-square tests at the
p = 0.05 level for differences in
percentages and percent distributions.
All comparisons reported in the text are
statistically significant unless otherwise
indicated. Comparisons not mentioned
may or may not be statistically
significant. Data analyses were
performed using the statistical packages
SAS, version 9.2 (9) and SUDAAN,
version 10.0 (10). Because estimates
were rounded to the nearest hundred,
individual estimates may not sum to
totals.
Results
Adoption of electronic health
records and mobile
technology
Twenty-eight percent of home
health and hospice care agencies have
adopted both electronic health records
and mobile technology (Figure 1).
Slightly over one-half (54%) of the
agencies had neither an electronic health
record nor mobile technology. Sixteen
percent adopted only electronic health
records, whereas 2% (an unreliable
estimate) adopted only mobile
technology. In other words, 44% of
agencies adopted electronic health
records (16% only electronic health
records and 28% both technologies),
whereas 30% adopted mobile
technology (2% only mobile technology
and 28% both technologies).
Agency characteristics
associated with adoption of
both electronic health
records and mobile
technology
In unadjusted analyses (Table 1),
agency adoption of both electronic
health records and mobile technology
was associated with all the variables
Electronic health
records only
(n = 2,100)
16%
Mobile technology only
(n = 300)
2%*
Both electronic health
records and mobile
technology
(n = 3,600)
28%
Neither electronic health
records nor mobile
technology
(n = 7,100)
54%
* Estimate is unreliable.
NOTES: A weighted total of 13,100 agencies were analyzed. Figure excludes cases with missing data. See Data Analysis
section for details.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Figure 1. Home health and hospice care agencies’ adoption of electronic health records
and mobile technology: United States, 2007
included in the analyses. Agencies were
more likely to adopt both technologies if
the agency offered both home health
and hospice care, was not part of a
chain, had administrators with a tenure
of 71 or more months (rather than
25–70 months), had 50 or more patients,
had revenue from Medicare in the
middle tertile (52%–87%) of total
revenues, offered 14 or more services,
were either nonprofit or government-
owned, or were jointly owned by either
a hospital or a health care system. The
largest effect was for agency type:
where 8% of agencies that were
for-profit adopted both technologies, in
contrast to voluntary nonprofits (67%)
and government agencies (51%). Total
number of patients and joint ownership
had effects of similar magnitude. Among
agencies with fewer than 50 patients,
9% adopted both technologies, but there
was no difference in adoption between
agencies with 50–99 patients (32%) and
those with 100 or more patients (43%).
Independent agencies were less likely to
adopt both technologies (18%),
compared with agencies jointly owned
with a hospital (51%) or a health care
system (60%).
In adjusted analyses (Table 2),
agency adoption of both electronic
health records and mobile technology
was associated with the number of
current patients served and with
ownership. Agencies that had 50 or
more patients and were either nonprofit
or government-owned were more likely
to adopt both technologies, compared
with all other agencies that had adopted
only electronic health records or adopted
neither technology, while controlling for
other variables. Twelve percent of
agencies with fewer than 50 patients
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Page 4 National Health Statistics Reports n Number 66 n May 20, 2013
adopted both technologies, compared
with 31% of agencies with 50–99
patients and 32% of agencies with 100
or more patients. Ten percent of
for-profit agencies adopted both
technologies, compared with 54% of
voluntary nonprofit agencies and 50% of
government agencies.
Models in which ownership, joint
ownership, percentage of revenue from
Medicare, and agency type were
dropped sequentially from the full
model were also run. When ownership
was dropped, adopting both technologies
was associated with joint ownership,
administrator tenure, number of patients,
and chain membership. Percentage of
revenue from Medicare, number of
patients, administrator tenure, and chain
membership were significant when joint
ownership was also removed from the
model. When percentage of revenue
from Medicare was also removed, type
of care provided, number of patients,
administrator tenure, and chain
membership were significant. When all
four of the most closely associated
variables (ownership, joint ownership,
percentage of revenue from Medicare,
and type of care provided) were
removed from the model, the number of
services offered, number of patients,
administrator tenure, and chain
membership were all associated with
adopting both types of technology. (Data
not shown.)
Agency characteristics
associated with adoption of
only electronic health
records
In unadjusted analyses, adoption of
only electronic health records was
associated with type of care offered by
the agency, number of patients, agency
type, and joint ownership (Table 1).
Compared with all other agencies,
agencies that adopted only electronic
health records were more likely to offer
home health care only (18%) rather than
both home health and hospice care
(6%); to have fewer than 50 patients
(28%) rather than 50–99 patients (10%);
to be for-profit (21%) rather than
voluntary nonprofit (7%); or to be
independent (19%) rather than jointly
owned with a hospital (6%).
In adjusted analyses (Table 2), an
agency’s adoption of only electronic
health records (compared with adopting
both or neither technology) was not
associated with any of the variables
used in the analyses.
Adjusted analyses that included
only the four variables with significant
bivariate associations (type of care
offered by the agency, number of
patients, agency type, and joint
ownership) did not improve the overall
fit compared with the full model.
Similarly, when ownership, joint
ownership, percentage of revenue from
Medicare, and type of care offered were
dropped sequentially, none of those
models improved the fit. (Data not
shown.)
Agency characteristics
associated with adoption of
neither electronic health
records nor mobile
technology
In unadjusted analyses, agency
adoption of neither type of technology
was associated with type of care offered,
percentage of revenue from Medicare,
number of services offered, agency type,
and joint ownership (Table 1). Agencies
were more likely to adopt neither
technology if they provided either home
health care only or hospice care only
rather than both types of care; if their
percentage of revenue from Medicare
was in the highest tertile (88% or more)
of total revenues rather than the middle
tertile (52%–87%); if they offered
10–13 services rather than 14 or more;
if they were for-profit rather than
nonprofit or government-owned; and if
they were independent or jointly owned
with a hospital rather than jointly owned
with a health care system and other. The
largest effects were seen with agency
type, where 71% of for-profit agencies
adopted neither technology, compared
with 26% of voluntary nonprofits and
37% of government-owned agencies.
Joint ownership also showed strong
effects, with 62% of independent
agencies adopting neither technology,
compared with 44% of agencies
affiliated with a hospital and 23%
affiliated with a health care system.
In adjusted analyses, agency
adoption of neither type of technology,
rather than both or electronic health
records only (Table 2), was associated
with agency type and joint ownership.
Agencies that were for-profit and were
independent or jointly owned with a
hospital were more likely to have
adopted neither type of technology than
to have adopted both technologies or
only electronic health records.
In adjusted analyses, which
included only the variables with
significant bivariate associations with
adoption of neither technology (type of
care offered, percentage of revenue from
Medicare, number of services offered,
agency type, and joint ownership), the
same variables found significant in the
full model (agency type and joint
ownership) were significant in the
smaller model. The adjusted percentages
from this smaller model were very
similar to the adjusted percentages in
the full model. When ownership, joint
ownership, and percentage of revenue
from Medicare were dropped
sequentially, none of the remaining
variables were significant. However,
when type of care offered was dropped
as well, then the number of services
offered became significant. Adoption of
neither technology was associated with
offering 10–13 services, compared with
13 or more. (Data not shown.)
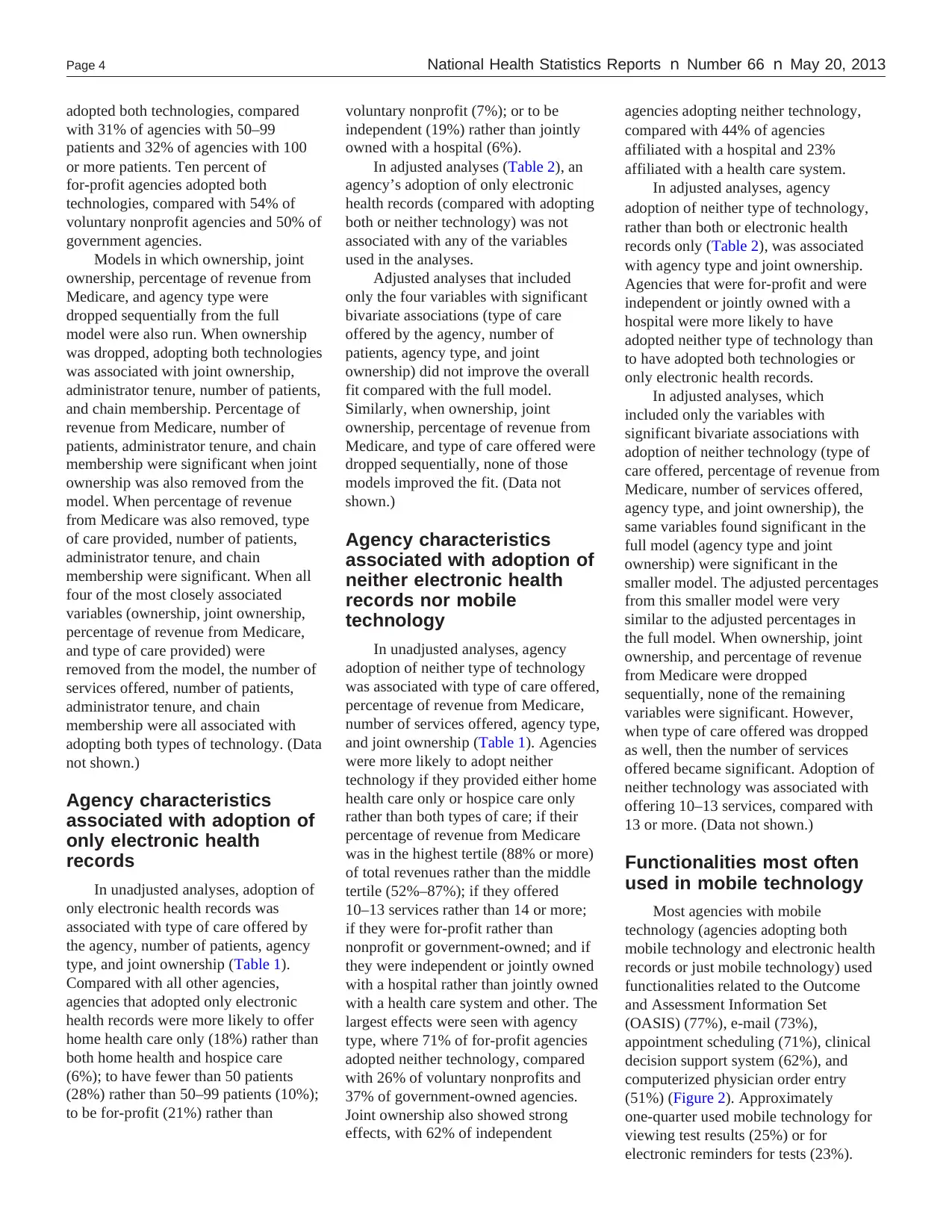
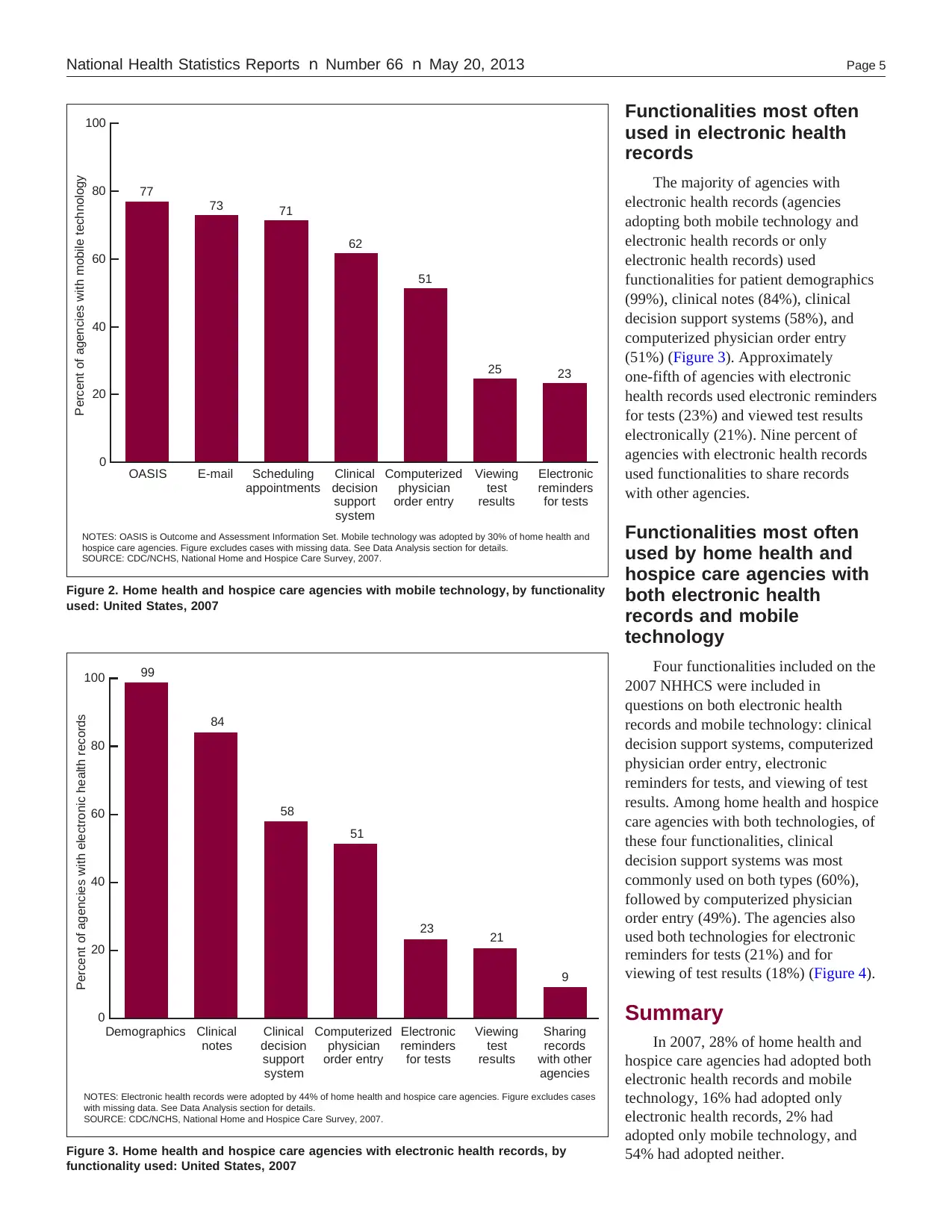
Functionalities most often
used in mobile technology
Most agencies with mobile
technology (agencies adopting both
mobile technology and electronic health
records or just mobile technology) used
functionalities related to the Outcome
and Assessment Information Set
(OASIS) (77%), e-mail (73%),
appointment scheduling (71%), clinical
decision support system (62%), and
computerized physician order entry
(51%) (Figure 2). Approximately
one-quarter used mobile technology for
viewing test results (25%) or for
electronic reminders for tests (23%).
adopted both technologies, compared
with 31% of agencies with 50–99
patients and 32% of agencies with 100
or more patients. Ten percent of
for-profit agencies adopted both
technologies, compared with 54% of
voluntary nonprofit agencies and 50% of
government agencies.
Models in which ownership, joint
ownership, percentage of revenue from
Medicare, and agency type were
dropped sequentially from the full
model were also run. When ownership
was dropped, adopting both technologies
was associated with joint ownership,
administrator tenure, number of patients,
and chain membership. Percentage of
revenue from Medicare, number of
patients, administrator tenure, and chain
membership were significant when joint
ownership was also removed from the
model. When percentage of revenue
from Medicare was also removed, type
of care provided, number of patients,
administrator tenure, and chain
membership were significant. When all
four of the most closely associated
variables (ownership, joint ownership,
percentage of revenue from Medicare,
and type of care provided) were
removed from the model, the number of
services offered, number of patients,
administrator tenure, and chain
membership were all associated with
adopting both types of technology. (Data
not shown.)
Agency characteristics
associated with adoption of
only electronic health
records
In unadjusted analyses, adoption of
only electronic health records was
associated with type of care offered by
the agency, number of patients, agency
type, and joint ownership (Table 1).
Compared with all other agencies,
agencies that adopted only electronic
health records were more likely to offer
home health care only (18%) rather than
both home health and hospice care
(6%); to have fewer than 50 patients
(28%) rather than 50–99 patients (10%);
to be for-profit (21%) rather than
voluntary nonprofit (7%); or to be
independent (19%) rather than jointly
owned with a hospital (6%).
In adjusted analyses (Table 2), an
agency’s adoption of only electronic
health records (compared with adopting
both or neither technology) was not
associated with any of the variables
used in the analyses.
Adjusted analyses that included
only the four variables with significant
bivariate associations (type of care
offered by the agency, number of
patients, agency type, and joint
ownership) did not improve the overall
fit compared with the full model.
Similarly, when ownership, joint
ownership, percentage of revenue from
Medicare, and type of care offered were
dropped sequentially, none of those
models improved the fit. (Data not
shown.)
Agency characteristics
associated with adoption of
neither electronic health
records nor mobile
technology
In unadjusted analyses, agency
adoption of neither type of technology
was associated with type of care offered,
percentage of revenue from Medicare,
number of services offered, agency type,
and joint ownership (Table 1). Agencies
were more likely to adopt neither
technology if they provided either home
health care only or hospice care only
rather than both types of care; if their
percentage of revenue from Medicare
was in the highest tertile (88% or more)
of total revenues rather than the middle
tertile (52%–87%); if they offered
10–13 services rather than 14 or more;
if they were for-profit rather than
nonprofit or government-owned; and if
they were independent or jointly owned
with a hospital rather than jointly owned
with a health care system and other. The
largest effects were seen with agency
type, where 71% of for-profit agencies
adopted neither technology, compared
with 26% of voluntary nonprofits and
37% of government-owned agencies.
Joint ownership also showed strong
effects, with 62% of independent
agencies adopting neither technology,
compared with 44% of agencies
affiliated with a hospital and 23%
affiliated with a health care system.
In adjusted analyses, agency
adoption of neither type of technology,
rather than both or electronic health
records only (Table 2), was associated
with agency type and joint ownership.
Agencies that were for-profit and were
independent or jointly owned with a
hospital were more likely to have
adopted neither type of technology than
to have adopted both technologies or
only electronic health records.
In adjusted analyses, which
included only the variables with
significant bivariate associations with
adoption of neither technology (type of
care offered, percentage of revenue from
Medicare, number of services offered,
agency type, and joint ownership), the
same variables found significant in the
full model (agency type and joint
ownership) were significant in the
smaller model. The adjusted percentages
from this smaller model were very
similar to the adjusted percentages in
the full model. When ownership, joint
ownership, and percentage of revenue
from Medicare were dropped
sequentially, none of the remaining
variables were significant. However,
when type of care offered was dropped
as well, then the number of services
offered became significant. Adoption of
neither technology was associated with
offering 10–13 services, compared with
13 or more. (Data not shown.)
Functionalities most often
used in mobile technology
Most agencies with mobile
technology (agencies adopting both
mobile technology and electronic health
records or just mobile technology) used
functionalities related to the Outcome
and Assessment Information Set
(OASIS) (77%), e-mail (73%),
appointment scheduling (71%), clinical
decision support system (62%), and
computerized physician order entry
(51%) (Figure 2). Approximately
one-quarter used mobile technology for
viewing test results (25%) or for
electronic reminders for tests (23%).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
National Health Statistics Reports n Number 66 n May 20, 2013 Page 5
NOTES: OASIS is Outcome and Assessment Information Set. Mobile technology was adopted by 30% of home health and
hospice care agencies. Figure excludes cases with missing data. See Data Analysis section for details.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Percent of agencies with mobile technology
77
73 71
62
51
25 23
0
20
40
60
80
100
OASIS E-mail Scheduling
appointments
Electronic
reminders
for tests
Clinical
decision
support
system
Computerized
physician
order entry
Viewing
test
results
Figure 2. Home health and hospice care agencies with mobile technology, by functionality
used: United States, 2007
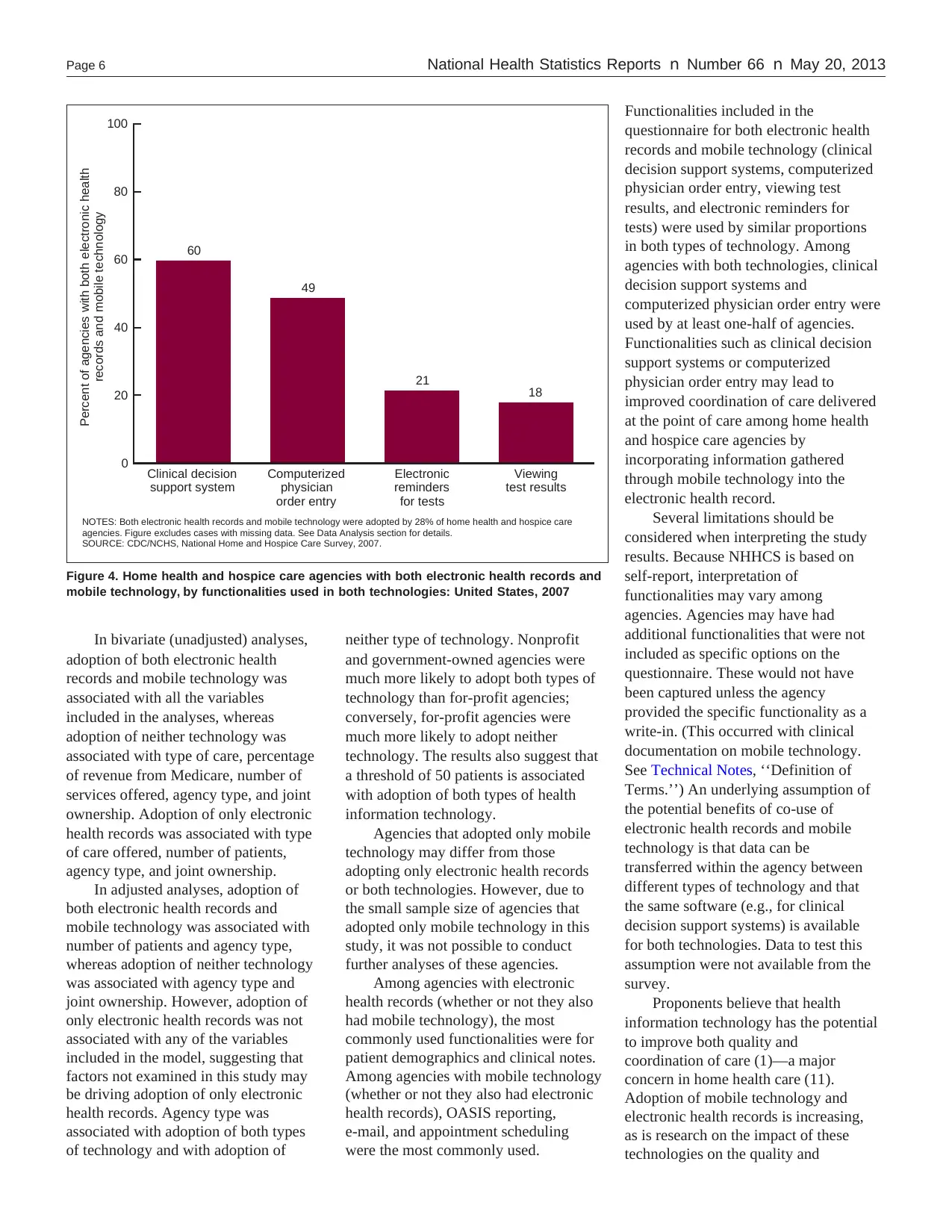
NOTES: Electronic health records were adopted by 44% of home health and hospice care agencies. Figure excludes cases
with missing data. See Data Analysis section for details.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Percent of agencies with electronic health records
99
84
58
51
23 21
9
0
20
40
60
80
100
Demographics Clinical
notes
Clinical
decision
support
system
Computerized
physician
order entry
Electronic
reminders
for tests
Viewing
test
results
Sharing
records
with other
agencies
Figure 3. Home health and hospice care agencies with electronic health records, by
functionality used: United States, 2007
Functionalities most often
used in electronic health
records
The majority of agencies with
electronic health records (agencies
adopting both mobile technology and
electronic health records or only
electronic health records) used
functionalities for patient demographics
(99%), clinical notes (84%), clinical
decision support systems (58%), and
computerized physician order entry
(51%) (Figure 3). Approximately
one-fifth of agencies with electronic
health records used electronic reminders
for tests (23%) and viewed test results
electronically (21%). Nine percent of
agencies with electronic health records
used functionalities to share records
with other agencies.
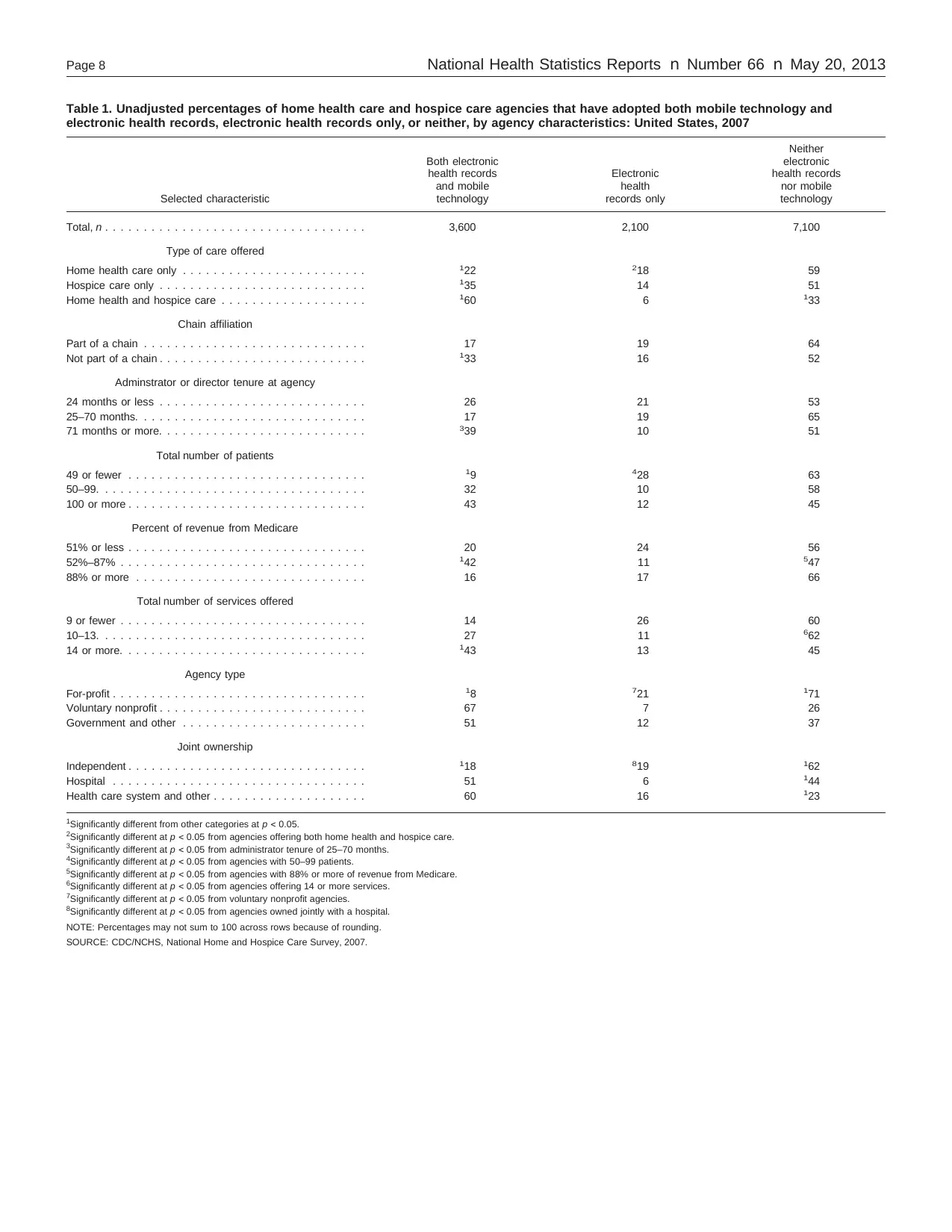
Functionalities most often
used by home health and
hospice care agencies with
both electronic health
records and mobile
technology
Four functionalities included on the
2007 NHHCS were included in
questions on both electronic health
records and mobile technology: clinical
decision support systems, computerized
physician order entry, electronic
reminders for tests, and viewing of test
results. Among home health and hospice
care agencies with both technologies, of
these four functionalities, clinical
decision support systems was most
commonly used on both types (60%),
followed by computerized physician
order entry (49%). The agencies also
used both technologies for electronic
reminders for tests (21%) and for
viewing of test results (18%) (Figure 4).
Summary
In 2007, 28% of home health and
hospice care agencies had adopted both
electronic health records and mobile
technology, 16% had adopted only
electronic health records, 2% had
adopted only mobile technology, and
54% had adopted neither.
NOTES: OASIS is Outcome and Assessment Information Set. Mobile technology was adopted by 30% of home health and
hospice care agencies. Figure excludes cases with missing data. See Data Analysis section for details.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Percent of agencies with mobile technology
77
73 71
62
51
25 23
0
20
40
60
80
100
OASIS E-mail Scheduling
appointments
Electronic
reminders
for tests
Clinical
decision
support
system
Computerized
physician
order entry
Viewing
test
results
Figure 2. Home health and hospice care agencies with mobile technology, by functionality
used: United States, 2007
NOTES: Electronic health records were adopted by 44% of home health and hospice care agencies. Figure excludes cases
with missing data. See Data Analysis section for details.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Percent of agencies with electronic health records
99
84
58
51
23 21
9
0
20
40
60
80
100
Demographics Clinical
notes
Clinical
decision
support
system
Computerized
physician
order entry
Electronic
reminders
for tests
Viewing
test
results
Sharing
records
with other
agencies
Figure 3. Home health and hospice care agencies with electronic health records, by
functionality used: United States, 2007
Functionalities most often
used in electronic health
records
The majority of agencies with
electronic health records (agencies
adopting both mobile technology and
electronic health records or only
electronic health records) used
functionalities for patient demographics
(99%), clinical notes (84%), clinical
decision support systems (58%), and
computerized physician order entry
(51%) (Figure 3). Approximately
one-fifth of agencies with electronic
health records used electronic reminders
for tests (23%) and viewed test results
electronically (21%). Nine percent of
agencies with electronic health records
used functionalities to share records
with other agencies.
Functionalities most often
used by home health and
hospice care agencies with
both electronic health
records and mobile
technology
Four functionalities included on the
2007 NHHCS were included in
questions on both electronic health
records and mobile technology: clinical
decision support systems, computerized
physician order entry, electronic
reminders for tests, and viewing of test
results. Among home health and hospice
care agencies with both technologies, of
these four functionalities, clinical
decision support systems was most
commonly used on both types (60%),
followed by computerized physician
order entry (49%). The agencies also
used both technologies for electronic
reminders for tests (21%) and for
viewing of test results (18%) (Figure 4).
Summary
In 2007, 28% of home health and
hospice care agencies had adopted both
electronic health records and mobile
technology, 16% had adopted only
electronic health records, 2% had
adopted only mobile technology, and
54% had adopted neither.
Page 6 National Health Statistics Reports n Number 66 n May 20, 2013
NOTES: Both electronic health records and mobile technology were adopted by 28% of home health and hospice care
agencies. Figure excludes cases with missing data. See Data Analysis section for details.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Percent of agencies with both electronic health
records and mobile technology
Clinical decision
support system
Computerized
physician
order entry
Electronic
reminders
for tests
Viewing
test results
60
49
21 18
0
20
40
60
80
100
Figure 4. Home health and hospice care agencies with both electronic health records and
mobile technology, by functionalities used in both technologies: United States, 2007
In bivariate (unadjusted) analyses,
adoption of both electronic health
records and mobile technology was
associated with all the variables
included in the analyses, whereas
adoption of neither technology was
associated with type of care, percentage
of revenue from Medicare, number of
services offered, agency type, and joint
ownership. Adoption of only electronic
health records was associated with type
of care offered, number of patients,
agency type, and joint ownership.
In adjusted analyses, adoption of
both electronic health records and
mobile technology was associated with
number of patients and agency type,
whereas adoption of neither technology
was associated with agency type and
joint ownership. However, adoption of
only electronic health records was not
associated with any of the variables
included in the model, suggesting that
factors not examined in this study may
be driving adoption of only electronic
health records. Agency type was
associated with adoption of both types
of technology and with adoption of
neither type of technology. Nonprofit
and government-owned agencies were
much more likely to adopt both types of
technology than for-profit agencies;
conversely, for-profit agencies were
much more likely to adopt neither
technology. The results also suggest that
a threshold of 50 patients is associated
with adoption of both types of health
information technology.
Agencies that adopted only mobile
technology may differ from those
adopting only electronic health records
or both technologies. However, due to
the small sample size of agencies that
adopted only mobile technology in this
study, it was not possible to conduct
further analyses of these agencies.
Among agencies with electronic
health records (whether or not they also
had mobile technology), the most
commonly used functionalities were for
patient demographics and clinical notes.
Among agencies with mobile technology
(whether or not they also had electronic
health records), OASIS reporting,
e-mail, and appointment scheduling
were the most commonly used.
Functionalities included in the
questionnaire for both electronic health
records and mobile technology (clinical
decision support systems, computerized
physician order entry, viewing test
results, and electronic reminders for
tests) were used by similar proportions
in both types of technology. Among
agencies with both technologies, clinical
decision support systems and
computerized physician order entry were
used by at least one-half of agencies.
Functionalities such as clinical decision
support systems or computerized
physician order entry may lead to
improved coordination of care delivered
at the point of care among home health
and hospice care agencies by
incorporating information gathered
through mobile technology into the
electronic health record.
Several limitations should be
considered when interpreting the study
results. Because NHHCS is based on
self-report, interpretation of
functionalities may vary among
agencies. Agencies may have had
additional functionalities that were not
included as specific options on the
questionnaire. These would not have
been captured unless the agency
provided the specific functionality as a
write-in. (This occurred with clinical
documentation on mobile technology.
See Technical Notes, ‘‘Definition of
Terms.’’) An underlying assumption of
the potential benefits of co-use of
electronic health records and mobile
technology is that data can be
transferred within the agency between
different types of technology and that
the same software (e.g., for clinical
decision support systems) is available
for both technologies. Data to test this
assumption were not available from the
survey.
Proponents believe that health
information technology has the potential
to improve both quality and
coordination of care (1)—a major
concern in home health care (11).
Adoption of mobile technology and
electronic health records is increasing,
as is research on the impact of these
technologies on the quality and
NOTES: Both electronic health records and mobile technology were adopted by 28% of home health and hospice care
agencies. Figure excludes cases with missing data. See Data Analysis section for details.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Percent of agencies with both electronic health
records and mobile technology
Clinical decision
support system
Computerized
physician
order entry
Electronic
reminders
for tests
Viewing
test results
60
49
21 18
0
20
40
60
80
100
Figure 4. Home health and hospice care agencies with both electronic health records and
mobile technology, by functionalities used in both technologies: United States, 2007
In bivariate (unadjusted) analyses,
adoption of both electronic health
records and mobile technology was
associated with all the variables
included in the analyses, whereas
adoption of neither technology was
associated with type of care, percentage
of revenue from Medicare, number of
services offered, agency type, and joint
ownership. Adoption of only electronic
health records was associated with type
of care offered, number of patients,
agency type, and joint ownership.
In adjusted analyses, adoption of
both electronic health records and
mobile technology was associated with
number of patients and agency type,
whereas adoption of neither technology
was associated with agency type and
joint ownership. However, adoption of
only electronic health records was not
associated with any of the variables
included in the model, suggesting that
factors not examined in this study may
be driving adoption of only electronic
health records. Agency type was
associated with adoption of both types
of technology and with adoption of
neither type of technology. Nonprofit
and government-owned agencies were
much more likely to adopt both types of
technology than for-profit agencies;
conversely, for-profit agencies were
much more likely to adopt neither
technology. The results also suggest that
a threshold of 50 patients is associated
with adoption of both types of health
information technology.
Agencies that adopted only mobile
technology may differ from those
adopting only electronic health records
or both technologies. However, due to
the small sample size of agencies that
adopted only mobile technology in this
study, it was not possible to conduct
further analyses of these agencies.
Among agencies with electronic
health records (whether or not they also
had mobile technology), the most
commonly used functionalities were for
patient demographics and clinical notes.
Among agencies with mobile technology
(whether or not they also had electronic
health records), OASIS reporting,
e-mail, and appointment scheduling
were the most commonly used.
Functionalities included in the
questionnaire for both electronic health
records and mobile technology (clinical
decision support systems, computerized
physician order entry, viewing test
results, and electronic reminders for
tests) were used by similar proportions
in both types of technology. Among
agencies with both technologies, clinical
decision support systems and
computerized physician order entry were
used by at least one-half of agencies.
Functionalities such as clinical decision
support systems or computerized
physician order entry may lead to
improved coordination of care delivered
at the point of care among home health
and hospice care agencies by
incorporating information gathered
through mobile technology into the
electronic health record.
Several limitations should be
considered when interpreting the study
results. Because NHHCS is based on
self-report, interpretation of
functionalities may vary among
agencies. Agencies may have had
additional functionalities that were not
included as specific options on the
questionnaire. These would not have
been captured unless the agency
provided the specific functionality as a
write-in. (This occurred with clinical
documentation on mobile technology.
See Technical Notes, ‘‘Definition of
Terms.’’) An underlying assumption of
the potential benefits of co-use of
electronic health records and mobile
technology is that data can be
transferred within the agency between
different types of technology and that
the same software (e.g., for clinical
decision support systems) is available
for both technologies. Data to test this
assumption were not available from the
survey.
Proponents believe that health
information technology has the potential
to improve both quality and
coordination of care (1)—a major
concern in home health care (11).
Adoption of mobile technology and
electronic health records is increasing,
as is research on the impact of these
technologies on the quality and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

National Health Statistics Reports n Number 66 n May 20, 2013 Page 7
coordination of care in home and
hospice (12–18).
References
1. Blumenthal D. Launching HITECH.
N Engl J Med 362(5):382–5. 2010.
2. Trescone D. Success at the point of
care. Caring 25(7):40–2. 2006.
3. Sanchez I. Implementation of a point
of care system in home health. Home
Healthc Nurse 227(10):623–9. 2009.
4. Bercovitz A, Sengupta M, Jamison P.
Electronic medical record adoption
and use in home health and hospice.
NCHS data brief, no. 45. Hyattsville,
MD: National Center for Health
Statistics. 2010. Available from:
http://www.cdc.gov/nchs/data/
databriefs/db45.pdf.
5. Philips national study on the future
of technology and telehealth in home
care. 2008. Available from:
http://www3.medical.philips.com/
resources/hsg/docs/en-us/custom/
PhilipsNationalStudyFullReport.pdf.
[Accessed 2010.]
6. Resnick HE, Alwan M. Use of health
information technology in home
health and hospice agencies:
United States, 2007. J Am Med
Inform Assoc 17(4):389–95. 2010.
7. Dwyer LL, Harris-Kojetin L,
Branden L, Shimizu IM. Redesign
and operation of the National Home
and Hospice Care Survey, 2007.
National Center for Health Statistics.
Vital Health Stat 1(53). 2010.
Available from: http://www.cdc.gov/
nchs/data/series/sr_01/sr01_053.pdf.
8. Park-Lee EY, Decker FH.
Comparison of home health and
hospice care agencies by
organizational characteristics and
services provided: United States,
2007. National health statistics
reports; no 30. Hyattsville, MD:
National Center for Health Statistics.
2010. Available from: http://www.
cdc.gov/nchs/data/nhsr/nhsr030.pdf.
9. SAS, release 9.2 [computer
software]. Cary, NC: SAS Institute.
2008.
10. SUDAAN, release 10.0 [computer
software]. Research Triangle Park,
NC: RTI International. 2008.
11. Boling PA. Care transitions and
home health care. Clin Geriatr Med
25(1):135–48, viii. 2009.
12. Stolee P, Steeves B, Glenny C,
Filsinger S. The use of electronic
health information systems in home
care: Facilitators and barriers. Home
Healthc Nurse 28(3):167–81. 2010.
13. Russell D, Rosenfeld P, Ames S,
Rosati RJ. Using technology to
enhance the quality of home health
care: Three case studies of health
information technology initiatives at
the Visiting Nurse Service of New
York. J Healthc Qual 32(5):22–9.
2010.
14. Buntin MB, Burke MF, Hoaglin MC,
Blumenthal D. The benefits of health
information technology: A review of
the recent literature shows
predominantly positive results.
Health Aff (Millwood) 30(3):464–71.
2011.
15. O’Malley AS, Grossman JM, Cohen
GR, Kemper NM, Pham HH. Are
electronic medical records helpful for
care coordination? Experiences of
physician practices. J Gen Intern
Med 25(3):177–85. 2010.
16. Wu RC, Straus SE. Evidence for
handheld electronic medical records
in improving care: A systematic
review. BMC Med Inform Decis
Mak 6:26. 2006.
17. Berner ES, Houston TK, Ray MN,
Alison JJ, Heudebert GR, Chatham
WW, et al. Improving ambulatory
prescribing safety with a handheld
decision support system: a
randomized controlled trial. J Am
Med Inform Assoc 13(2):171–9.
2006.
18. Feldman PH, Murtaugh CM, Pezzin
LE, McDonald MV, Peng TR.
Just-in-time evidence-based e-mail
‘‘reminders’’ in home health care:
Impact on patient outcomes. Health
Serv Res 40(3):865–85. 2005.
coordination of care in home and
hospice (12–18).
References
1. Blumenthal D. Launching HITECH.
N Engl J Med 362(5):382–5. 2010.
2. Trescone D. Success at the point of
care. Caring 25(7):40–2. 2006.
3. Sanchez I. Implementation of a point
of care system in home health. Home
Healthc Nurse 227(10):623–9. 2009.
4. Bercovitz A, Sengupta M, Jamison P.
Electronic medical record adoption
and use in home health and hospice.
NCHS data brief, no. 45. Hyattsville,
MD: National Center for Health
Statistics. 2010. Available from:
http://www.cdc.gov/nchs/data/
databriefs/db45.pdf.
5. Philips national study on the future
of technology and telehealth in home
care. 2008. Available from:
http://www3.medical.philips.com/
resources/hsg/docs/en-us/custom/
PhilipsNationalStudyFullReport.pdf.
[Accessed 2010.]
6. Resnick HE, Alwan M. Use of health
information technology in home
health and hospice agencies:
United States, 2007. J Am Med
Inform Assoc 17(4):389–95. 2010.
7. Dwyer LL, Harris-Kojetin L,
Branden L, Shimizu IM. Redesign
and operation of the National Home
and Hospice Care Survey, 2007.
National Center for Health Statistics.
Vital Health Stat 1(53). 2010.
Available from: http://www.cdc.gov/
nchs/data/series/sr_01/sr01_053.pdf.
8. Park-Lee EY, Decker FH.
Comparison of home health and
hospice care agencies by
organizational characteristics and
services provided: United States,
2007. National health statistics
reports; no 30. Hyattsville, MD:
National Center for Health Statistics.
2010. Available from: http://www.
cdc.gov/nchs/data/nhsr/nhsr030.pdf.
9. SAS, release 9.2 [computer
software]. Cary, NC: SAS Institute.
2008.
10. SUDAAN, release 10.0 [computer
software]. Research Triangle Park,
NC: RTI International. 2008.
11. Boling PA. Care transitions and
home health care. Clin Geriatr Med
25(1):135–48, viii. 2009.
12. Stolee P, Steeves B, Glenny C,
Filsinger S. The use of electronic
health information systems in home
care: Facilitators and barriers. Home
Healthc Nurse 28(3):167–81. 2010.
13. Russell D, Rosenfeld P, Ames S,
Rosati RJ. Using technology to
enhance the quality of home health
care: Three case studies of health
information technology initiatives at
the Visiting Nurse Service of New
York. J Healthc Qual 32(5):22–9.
2010.
14. Buntin MB, Burke MF, Hoaglin MC,
Blumenthal D. The benefits of health
information technology: A review of
the recent literature shows
predominantly positive results.
Health Aff (Millwood) 30(3):464–71.
2011.
15. O’Malley AS, Grossman JM, Cohen
GR, Kemper NM, Pham HH. Are
electronic medical records helpful for
care coordination? Experiences of
physician practices. J Gen Intern
Med 25(3):177–85. 2010.
16. Wu RC, Straus SE. Evidence for
handheld electronic medical records
in improving care: A systematic
review. BMC Med Inform Decis
Mak 6:26. 2006.
17. Berner ES, Houston TK, Ray MN,
Alison JJ, Heudebert GR, Chatham
WW, et al. Improving ambulatory
prescribing safety with a handheld
decision support system: a
randomized controlled trial. J Am
Med Inform Assoc 13(2):171–9.
2006.
18. Feldman PH, Murtaugh CM, Pezzin
LE, McDonald MV, Peng TR.
Just-in-time evidence-based e-mail
‘‘reminders’’ in home health care:
Impact on patient outcomes. Health
Serv Res 40(3):865–85. 2005.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Page 8 National Health Statistics Reports n Number 66 n May 20, 2013
Table 1. Unadjusted percentages of home health care and hospice care agencies that have adopted both mobile technology and
electronic health records, electronic health records only, or neither, by agency characteristics: United States, 2007
Neither
Both electronic electronic
health records Electronic health records
and mobile health nor mobile
Selected characteristic technology records only technology
Total, n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,600 2,100 7,100
Type of care offered
Home health care only . . . . . . . . . . . . . . . . . . . . . . . . 122 218 59
Hospice care only . . . . . . . . . . . . . . . . . . . . . . . . . . . 135 14 51
Home health and hospice care . . . . . . . . . . . . . . . . . . . 160 6 133
Chain affiliation
Part of a chain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17 19 64
Not part of a chain . . . . . . . . . . . . . . . . . . . . . . . . . . . 133 16 52
Adminstrator or director tenure at agency
24 months or less . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 21 53
25–70 months. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17 19 65
71 months or more. . . . . . . . . . . . . . . . . . . . . . . . . . . 339 10 51
Total number of patients
49 or fewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19 428 63
50–99. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32 10 58
100 or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43 12 45
Percent of revenue from Medicare
51% or less . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 24 56
52%–87% . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142 11 547
88% or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 17 66
Total number of services offered
9 or fewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 26 60
10–13. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 11 662
14 or more. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143 13 45
Agency type
For-profit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 721 171
Voluntary nonprofit . . . . . . . . . . . . . . . . . . . . . . . . . . . 67 7 26
Government and other . . . . . . . . . . . . . . . . . . . . . . . . 51 12 37
Joint ownership
Independent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118 819 162
Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51 6 144
Health care system and other . . . . . . . . . . . . . . . . . . . . 60 16 123
1Significantly different from other categories at p < 0.05.
2Significantly different at p < 0.05 from agencies offering both home health and hospice care.
3Significantly different at p < 0.05 from administrator tenure of 25–70 months.
4Significantly different at p < 0.05 from agencies with 50–99 patients.
5Significantly different at p < 0.05 from agencies with 88% or more of revenue from Medicare.
6Significantly different at p < 0.05 from agencies offering 14 or more services.
7Significantly different at p < 0.05 from voluntary nonprofit agencies.
8Significantly different at p < 0.05 from agencies owned jointly with a hospital.
NOTE: Percentages may not sum to 100 across rows because of rounding.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Table 1. Unadjusted percentages of home health care and hospice care agencies that have adopted both mobile technology and
electronic health records, electronic health records only, or neither, by agency characteristics: United States, 2007
Neither
Both electronic electronic
health records Electronic health records
and mobile health nor mobile
Selected characteristic technology records only technology
Total, n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,600 2,100 7,100
Type of care offered
Home health care only . . . . . . . . . . . . . . . . . . . . . . . . 122 218 59
Hospice care only . . . . . . . . . . . . . . . . . . . . . . . . . . . 135 14 51
Home health and hospice care . . . . . . . . . . . . . . . . . . . 160 6 133
Chain affiliation
Part of a chain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17 19 64
Not part of a chain . . . . . . . . . . . . . . . . . . . . . . . . . . . 133 16 52
Adminstrator or director tenure at agency
24 months or less . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 21 53
25–70 months. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17 19 65
71 months or more. . . . . . . . . . . . . . . . . . . . . . . . . . . 339 10 51
Total number of patients
49 or fewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19 428 63
50–99. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32 10 58
100 or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43 12 45
Percent of revenue from Medicare
51% or less . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 24 56
52%–87% . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142 11 547
88% or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 17 66
Total number of services offered
9 or fewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 26 60
10–13. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 11 662
14 or more. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143 13 45
Agency type
For-profit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 721 171
Voluntary nonprofit . . . . . . . . . . . . . . . . . . . . . . . . . . . 67 7 26
Government and other . . . . . . . . . . . . . . . . . . . . . . . . 51 12 37
Joint ownership
Independent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118 819 162
Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51 6 144
Health care system and other . . . . . . . . . . . . . . . . . . . . 60 16 123
1Significantly different from other categories at p < 0.05.
2Significantly different at p < 0.05 from agencies offering both home health and hospice care.
3Significantly different at p < 0.05 from administrator tenure of 25–70 months.
4Significantly different at p < 0.05 from agencies with 50–99 patients.
5Significantly different at p < 0.05 from agencies with 88% or more of revenue from Medicare.
6Significantly different at p < 0.05 from agencies offering 14 or more services.
7Significantly different at p < 0.05 from voluntary nonprofit agencies.
8Significantly different at p < 0.05 from agencies owned jointly with a hospital.
NOTE: Percentages may not sum to 100 across rows because of rounding.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
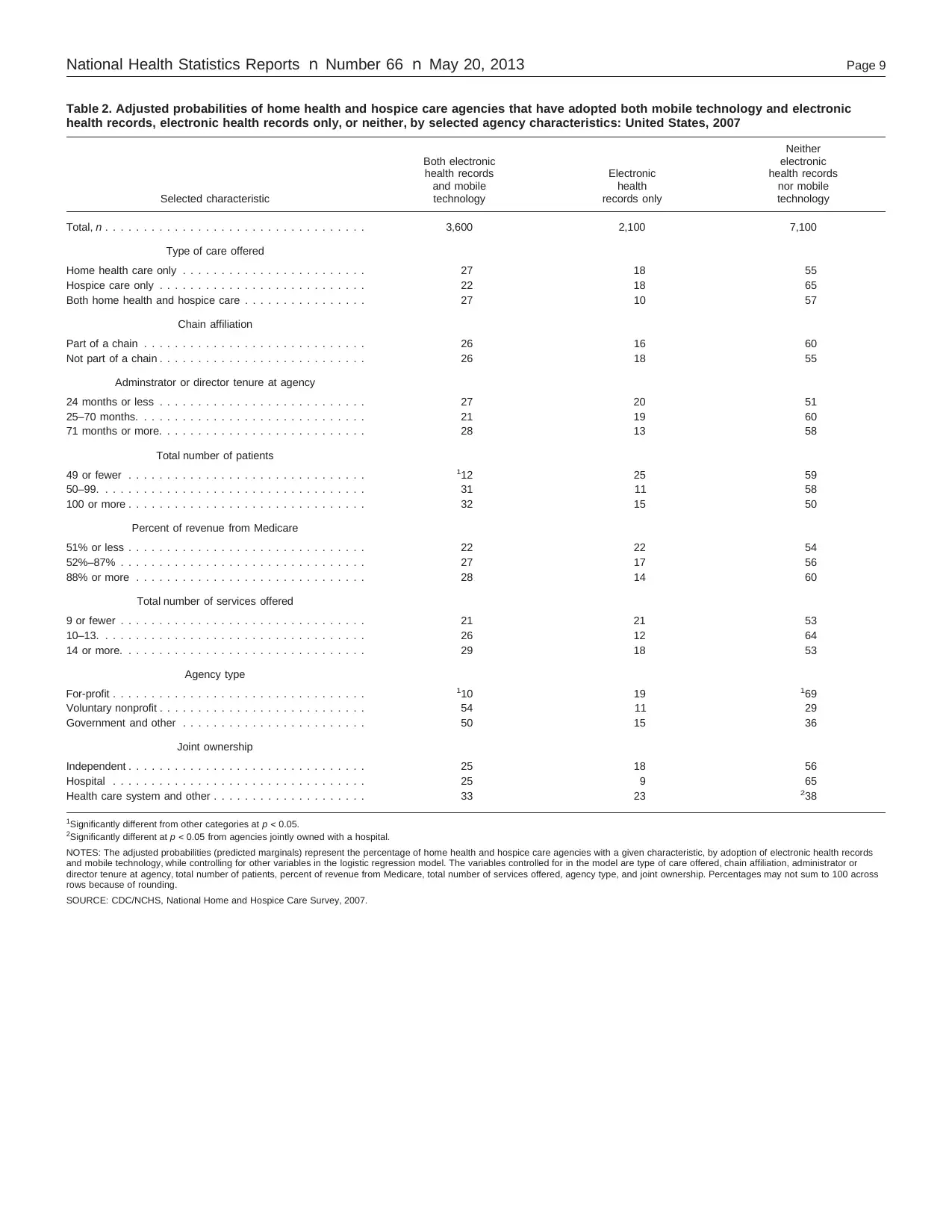
National Health Statistics Reports n Number 66 n May 20, 2013 Page 9
Table 2. Adjusted probabilities of home health and hospice care agencies that have adopted both mobile technology and electronic
health records, electronic health records only, or neither, by selected agency characteristics: United States, 2007
Neither
Both electronic electronic
health records Electronic health records
and mobile health nor mobile
Selected characteristic technology records only technology
Total, n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,600 2,100 7,100
Type of care offered
Home health care only . . . . . . . . . . . . . . . . . . . . . . . . 27 18 55
Hospice care only . . . . . . . . . . . . . . . . . . . . . . . . . . . 22 18 65
Both home health and hospice care . . . . . . . . . . . . . . . . 27 10 57
Chain affiliation
Part of a chain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 16 60
Not part of a chain . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 18 55
Adminstrator or director tenure at agency
24 months or less . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 20 51
25–70 months. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 19 60
71 months or more. . . . . . . . . . . . . . . . . . . . . . . . . . . 28 13 58
Total number of patients
49 or fewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 112 25 59
50–99. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 11 58
100 or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32 15 50
Percent of revenue from Medicare
51% or less . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22 22 54
52%–87% . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 17 56
88% or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28 14 60
Total number of services offered
9 or fewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 21 53
10–13. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 12 64
14 or more. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29 18 53
Agency type
For-profit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110 19 169
Voluntary nonprofit . . . . . . . . . . . . . . . . . . . . . . . . . . . 54 11 29
Government and other . . . . . . . . . . . . . . . . . . . . . . . . 50 15 36
Joint ownership
Independent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25 18 56
Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25 9 65
Health care system and other . . . . . . . . . . . . . . . . . . . . 33 23 238
1Significantly different from other categories at p < 0.05.
2Significantly different at p < 0.05 from agencies jointly owned with a hospital.
NOTES: The adjusted probabilities (predicted marginals) represent the percentage of home health and hospice care agencies with a given characteristic, by adoption of electronic health records
and mobile technology, while controlling for other variables in the logistic regression model. The variables controlled for in the model are type of care offered, chain affiliation, administrator or
director tenure at agency, total number of patients, percent of revenue from Medicare, total number of services offered, agency type, and joint ownership. Percentages may not sum to 100 across
rows because of rounding.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
Table 2. Adjusted probabilities of home health and hospice care agencies that have adopted both mobile technology and electronic
health records, electronic health records only, or neither, by selected agency characteristics: United States, 2007
Neither
Both electronic electronic
health records Electronic health records
and mobile health nor mobile
Selected characteristic technology records only technology
Total, n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,600 2,100 7,100
Type of care offered
Home health care only . . . . . . . . . . . . . . . . . . . . . . . . 27 18 55
Hospice care only . . . . . . . . . . . . . . . . . . . . . . . . . . . 22 18 65
Both home health and hospice care . . . . . . . . . . . . . . . . 27 10 57
Chain affiliation
Part of a chain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 16 60
Not part of a chain . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 18 55
Adminstrator or director tenure at agency
24 months or less . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 20 51
25–70 months. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 19 60
71 months or more. . . . . . . . . . . . . . . . . . . . . . . . . . . 28 13 58
Total number of patients
49 or fewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 112 25 59
50–99. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 11 58
100 or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32 15 50
Percent of revenue from Medicare
51% or less . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22 22 54
52%–87% . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 17 56
88% or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28 14 60
Total number of services offered
9 or fewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 21 53
10–13. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 12 64
14 or more. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29 18 53
Agency type
For-profit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110 19 169
Voluntary nonprofit . . . . . . . . . . . . . . . . . . . . . . . . . . . 54 11 29
Government and other . . . . . . . . . . . . . . . . . . . . . . . . 50 15 36
Joint ownership
Independent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25 18 56
Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25 9 65
Health care system and other . . . . . . . . . . . . . . . . . . . . 33 23 238
1Significantly different from other categories at p < 0.05.
2Significantly different at p < 0.05 from agencies jointly owned with a hospital.
NOTES: The adjusted probabilities (predicted marginals) represent the percentage of home health and hospice care agencies with a given characteristic, by adoption of electronic health records
and mobile technology, while controlling for other variables in the logistic regression model. The variables controlled for in the model are type of care offered, chain affiliation, administrator or
director tenure at agency, total number of patients, percent of revenue from Medicare, total number of services offered, agency type, and joint ownership. Percentages may not sum to 100 across
rows because of rounding.
SOURCE: CDC/NCHS, National Home and Hospice Care Survey, 2007.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Page 10 National Health Statistics Reports n Number 66 n May 20, 2013
Technical Notes
Data source and methods
Data from the 2007 NHHCS were
used for these analyses. The survey used
a stratified, two-stage probability design.
The first stage was the selection of
home health and hospice care agencies
from the sampling frame of over 15,000
agencies representing the universe of
agencies providing home health and
hospice care services in the United
States. Agencies affiliated with
hospitals, government entities,
retirement centers, or similar institutions
where the agencies maintained financial
and patient records independent of the
larger institution were included in the
frame. The primary sampling strata of
agencies were defined by agency type
and metropolitan statistical area status.
Within these sampling strata, agencies
were sorted by census region,
ownership, certification status, state,
county, ZIP code, and size (number of
employees). For the 2007 NHHCS,
1,545 agencies were sampled with
probability proportional to size.
Data collection
Data for the 2007 NHHCS were
collected through personal interviews
with agency directors and staff who
used administrative records to answer
questions about the agency, staff,
services, and programs. Interviews were
complete for 1,036 agencies. The
unweighted response rate was 71%. The
response rate weighted by the inverse of
the probability of selection was 59%. A
detailed description of the sampling
design, data collection, and response
rates for NHHCS is provided elsewhere
(7) and online at http://www.cdc.gov/
nchs/nhhcs/nhhcs_questionnaires.htm.
Estimation
Because NHHCS statistics are based
on a sample, they will differ somewhat
from the data that would have been
obtained if a complete census had been
taken using the same definitions,
instructions, and procedures. However,
the probability design of NHHCS
permits the calculation of sampling
errors. The standard error of a statistic is
primarily a measure of sampling
variability that occurs by chance
because only a sample, rather than the
entire population, is surveyed. The
standard error also reflects part of the
variation that arises in the measurement
process but does not include any
systematic bias that may be in the data
or any other nonsampling error. The
chances are about 95 in 100 that an
estimate from the sample differs from
the value that would be obtained from a
complete census by less than twice the
standard error. More information on
estimation is available at http://www.
cdc.gov/nchs/data/nhhcsd/NHHCS_
NHHAS_web_documentation.pdf.
Estimates are considered reliable if
they are based on 60 or more sample
cases and the relative standard error
(RSE) is less than 30%. Estimates based
on 30–59 cases, or based on more than
59 cases but with an RSE exceeding
30%, are indicated as unreliable in the
text, tables, and figures.
Definition of terms
Adoption of mobile technology—Based
on agency self-report at the time of
interview and defined by a ‘‘yes’’
response to the question, ‘‘Does this
agency’s staff use any system for
Electronic Point of Care
Documentation? Include PDAs (Personal
Digital Assistants), Notebook PCs, or
other portable handheld devices.’’
Mobile technology functionalities—
Based on agency self-report of use of
specific functionalities at the time of
interview and defined by a ‘‘yes’’
response to the question, ‘‘Are these
devices used for any of the following?’’
Options were ‘‘yes’’ or ‘‘no’’ for each
functionality. Functionalities included
computerized physician order entry for
prescriptions or pharmacy, laboratory
work, or tests; viewing of test results;
electronic reminders for tests; clinical
decision support systems or reference
systems; e-mail communication with
agency staff or other staff; scheduling
appointments or visits; OASIS reporting;
and other. Based on write-in responses
to the Other category, clinical
documentation was added as a
functionality; however, the estimate is
unreliable due to small sample size and
is not presented in this report.
Adoption of an electronic health
record system—Based on agency
self-report at the time of interview and
defined by a ‘‘yes’’ response to the
question, ‘‘Does this agency currently
have an Electronic Medical Records
system? This is a computerized version
of the patient’s medical information
used in the management of the patient’s
health care. Exclude electronic records
used only for billing purposes and
required documentation such as OASIS
files.’’
Electronic health record
functionalities—Based on agency
self-report of use of specific
functionalities at the time of interview
and defined by a ‘‘used’’ response to the
following: ‘‘With this agency’s current
electronic medical records system,
please indicate for each component
listed below, whether it is used,
available but not used, or not
available.’’ Functionalities included
computerized physician order entry for
prescriptions, laboratory work, and tests;
viewing of test results (e.g., chest
x-rays); patient demographics; electronic
reminders for tests (e.g., laboratory tests
and imaging); clinical decision support
systems of contraindications, allergies,
guidelines, etc.; clinical notes; public
health reporting (notifiable diseases);
and sharing medical records
electronically with other agencies. Of
the 1,036 agencies that participated in
the 2007 NHHCS, one agency reported
having an electronic health record
system but that none of the
functionalities were used, although they
were available. Because the question
about mobile technology asks about the
use of the functionality, only ‘‘used’’
responses for electronic health record
functionalities are included, to allow
clear comparison with mobile
technology functionality use.
Type of care offered—Indicates
whether the agency offered home health
care only, hospice care only, or both
home health and hospice care.
Chain affiliation—Indicates whether
the agency was part of a chain
Technical Notes
Data source and methods
Data from the 2007 NHHCS were
used for these analyses. The survey used
a stratified, two-stage probability design.
The first stage was the selection of
home health and hospice care agencies
from the sampling frame of over 15,000
agencies representing the universe of
agencies providing home health and
hospice care services in the United
States. Agencies affiliated with
hospitals, government entities,
retirement centers, or similar institutions
where the agencies maintained financial
and patient records independent of the
larger institution were included in the
frame. The primary sampling strata of
agencies were defined by agency type
and metropolitan statistical area status.
Within these sampling strata, agencies
were sorted by census region,
ownership, certification status, state,
county, ZIP code, and size (number of
employees). For the 2007 NHHCS,
1,545 agencies were sampled with
probability proportional to size.
Data collection
Data for the 2007 NHHCS were
collected through personal interviews
with agency directors and staff who
used administrative records to answer
questions about the agency, staff,
services, and programs. Interviews were
complete for 1,036 agencies. The
unweighted response rate was 71%. The
response rate weighted by the inverse of
the probability of selection was 59%. A
detailed description of the sampling
design, data collection, and response
rates for NHHCS is provided elsewhere
(7) and online at http://www.cdc.gov/
nchs/nhhcs/nhhcs_questionnaires.htm.
Estimation
Because NHHCS statistics are based
on a sample, they will differ somewhat
from the data that would have been
obtained if a complete census had been
taken using the same definitions,
instructions, and procedures. However,
the probability design of NHHCS
permits the calculation of sampling
errors. The standard error of a statistic is
primarily a measure of sampling
variability that occurs by chance
because only a sample, rather than the
entire population, is surveyed. The
standard error also reflects part of the
variation that arises in the measurement
process but does not include any
systematic bias that may be in the data
or any other nonsampling error. The
chances are about 95 in 100 that an
estimate from the sample differs from
the value that would be obtained from a
complete census by less than twice the
standard error. More information on
estimation is available at http://www.
cdc.gov/nchs/data/nhhcsd/NHHCS_
NHHAS_web_documentation.pdf.
Estimates are considered reliable if
they are based on 60 or more sample
cases and the relative standard error
(RSE) is less than 30%. Estimates based
on 30–59 cases, or based on more than
59 cases but with an RSE exceeding
30%, are indicated as unreliable in the
text, tables, and figures.
Definition of terms
Adoption of mobile technology—Based
on agency self-report at the time of
interview and defined by a ‘‘yes’’
response to the question, ‘‘Does this
agency’s staff use any system for
Electronic Point of Care
Documentation? Include PDAs (Personal
Digital Assistants), Notebook PCs, or
other portable handheld devices.’’
Mobile technology functionalities—
Based on agency self-report of use of
specific functionalities at the time of
interview and defined by a ‘‘yes’’
response to the question, ‘‘Are these
devices used for any of the following?’’
Options were ‘‘yes’’ or ‘‘no’’ for each
functionality. Functionalities included
computerized physician order entry for
prescriptions or pharmacy, laboratory
work, or tests; viewing of test results;
electronic reminders for tests; clinical
decision support systems or reference
systems; e-mail communication with
agency staff or other staff; scheduling
appointments or visits; OASIS reporting;
and other. Based on write-in responses
to the Other category, clinical
documentation was added as a
functionality; however, the estimate is
unreliable due to small sample size and
is not presented in this report.
Adoption of an electronic health
record system—Based on agency
self-report at the time of interview and
defined by a ‘‘yes’’ response to the
question, ‘‘Does this agency currently
have an Electronic Medical Records
system? This is a computerized version
of the patient’s medical information
used in the management of the patient’s
health care. Exclude electronic records
used only for billing purposes and
required documentation such as OASIS
files.’’
Electronic health record
functionalities—Based on agency
self-report of use of specific
functionalities at the time of interview
and defined by a ‘‘used’’ response to the
following: ‘‘With this agency’s current
electronic medical records system,
please indicate for each component
listed below, whether it is used,
available but not used, or not
available.’’ Functionalities included
computerized physician order entry for
prescriptions, laboratory work, and tests;
viewing of test results (e.g., chest
x-rays); patient demographics; electronic
reminders for tests (e.g., laboratory tests
and imaging); clinical decision support
systems of contraindications, allergies,
guidelines, etc.; clinical notes; public
health reporting (notifiable diseases);
and sharing medical records
electronically with other agencies. Of
the 1,036 agencies that participated in
the 2007 NHHCS, one agency reported
having an electronic health record
system but that none of the
functionalities were used, although they
were available. Because the question
about mobile technology asks about the
use of the functionality, only ‘‘used’’
responses for electronic health record
functionalities are included, to allow
clear comparison with mobile
technology functionality use.
Type of care offered—Indicates
whether the agency offered home health
care only, hospice care only, or both
home health and hospice care.
Chain affiliation—Indicates whether
the agency was part of a chain
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
National Health Statistics Reports n Number 66 n May 20, 2013 Page 11
of two or more agencies under one
ownership or operation.
Administrator or director tenure at
agency—Based on responses to the
question at the time of interview,
‘‘About how long has he/she been the
Director/Administrator at this agency?’’
Administrator tenure was converted
from continuous variables to a
categorical variable with three levels:
24 months or less, 25–70 months, and
71 months or more
Total number of patients—Refers to
the number of patients receiving care
from the agency at the time of
interview. For agencies providing both
home health and hospice care, the total
number of patients included both types
of patients. The total number of patients
was converted to a categorical variable
with three levels: 49 or fewer patients,
50–99 patients, and 100 or more
patients.
Percentage of revenue from
Medicare—Based on the agency’s
estimate of what percentage of its
overall patient care revenue was from
Medicare. This variable was divided into
three categories: 51% or less, 52%–
87%, and 88% or more.
Total number of services
offered—Calculated as the sum of
‘‘yes’’ responses when the agency was
asked whether they offered a specified
service. Services included
complementary and alternative medicine,
dietary and nutritional services,
enterostomal therapy, IV therapy,
physician services, podiatry services,
skilled nursing services, wound care,
durable medical equipment, pharmacy
services, occupational therapy, physical
therapy, respiratory therapy, speech
therapy or audiology, companion
services, continuous home care,
homemaker services, Meals on Wheels,
assistance with activities of daily living,
transportation services, volunteer
services, pastoral services, mental health
services, referral services, respite care,
medical social services, ethical issues
counseling, grief or bereavement
counseling, and other. The number of
services was converted from a
continuous variable to a three-level
categorical variable: 9 or fewer services,
10–13 services, and 14 or more services.
Agency type—This variable has three
categories: for-profit, voluntary
nonprofit, and government and other
(e.g., city, county, state, or federal
government, and Department of Veterans
Affairs).
Joint ownership—This variable was
collapsed into three categories:
independent, jointly owned with
hospital, and jointly owned with health
care system and other. Other includes
outpatient medical or surgical center,
managed care organization, and skilled
nursing facility.
of two or more agencies under one
ownership or operation.
Administrator or director tenure at
agency—Based on responses to the
question at the time of interview,
‘‘About how long has he/she been the
Director/Administrator at this agency?’’
Administrator tenure was converted
from continuous variables to a
categorical variable with three levels:
24 months or less, 25–70 months, and
71 months or more
Total number of patients—Refers to
the number of patients receiving care
from the agency at the time of
interview. For agencies providing both
home health and hospice care, the total
number of patients included both types
of patients. The total number of patients
was converted to a categorical variable
with three levels: 49 or fewer patients,
50–99 patients, and 100 or more
patients.
Percentage of revenue from
Medicare—Based on the agency’s
estimate of what percentage of its
overall patient care revenue was from
Medicare. This variable was divided into
three categories: 51% or less, 52%–
87%, and 88% or more.
Total number of services
offered—Calculated as the sum of
‘‘yes’’ responses when the agency was
asked whether they offered a specified
service. Services included
complementary and alternative medicine,
dietary and nutritional services,
enterostomal therapy, IV therapy,
physician services, podiatry services,
skilled nursing services, wound care,
durable medical equipment, pharmacy
services, occupational therapy, physical
therapy, respiratory therapy, speech
therapy or audiology, companion
services, continuous home care,
homemaker services, Meals on Wheels,
assistance with activities of daily living,
transportation services, volunteer
services, pastoral services, mental health
services, referral services, respite care,
medical social services, ethical issues
counseling, grief or bereavement
counseling, and other. The number of
services was converted from a
continuous variable to a three-level
categorical variable: 9 or fewer services,
10–13 services, and 14 or more services.
Agency type—This variable has three
categories: for-profit, voluntary
nonprofit, and government and other
(e.g., city, county, state, or federal
government, and Department of Veterans
Affairs).
Joint ownership—This variable was
collapsed into three categories:
independent, jointly owned with
hospital, and jointly owned with health
care system and other. Other includes
outpatient medical or surgical center,
managed care organization, and skilled
nursing facility.
U.S. DEPARTMENT OF
HEALTH & HUMAN SERVICES
Centers for Disease Control and Prevention
National Center for Health Statistics
3311 Toledo Road, Room 5419
Hyattsville, MD 20782
FIRST CLASS MAIL
POSTAGE& FEES PAID
CDC/NCHS
PERMIT NO. G-284
OFFICIAL BUSINESS
PENALTY FOR PRIVATE USE, $300
National Health Statistics Reports n Number 66 n May 20, 2013
Suggested citation
Bercovitz AR, Park-Lee E, Jamoom E.
Adoption and use of electronic health records
and mobile technology by home health and
hospice care agencies. National health
statistics reports; no 66. Hyattsville, MD:
National Center for Health Statistics. 2013.
Copyright information
All material appearing in this report is in the
public domain and may be reproduced or
copied without permission; citation as to
source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., Acting Director
Jennifer H. Madans, Ph.D., Associate Director
for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director
For e-mail updates on NCHS publication releases, subscribe online at: http://www.cdc.gov/nchs/govdelivery.htm.
For questions or general information about NCHS: Tel: 1–800–CDC–INFO (1–800–232–4636) • TTY: 1–888–232–6348
Internet: http://www.cdc.gov/nchs • Online request form: http://www.cdc.gov/cdc-info/requestform.html
DHHS Publication No. 2013–1250 • CS239260
HEALTH & HUMAN SERVICES
Centers for Disease Control and Prevention
National Center for Health Statistics
3311 Toledo Road, Room 5419
Hyattsville, MD 20782
FIRST CLASS MAIL
POSTAGE& FEES PAID
CDC/NCHS
PERMIT NO. G-284
OFFICIAL BUSINESS
PENALTY FOR PRIVATE USE, $300
National Health Statistics Reports n Number 66 n May 20, 2013
Suggested citation
Bercovitz AR, Park-Lee E, Jamoom E.
Adoption and use of electronic health records
and mobile technology by home health and
hospice care agencies. National health
statistics reports; no 66. Hyattsville, MD:
National Center for Health Statistics. 2013.
Copyright information
All material appearing in this report is in the
public domain and may be reproduced or
copied without permission; citation as to
source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., Acting Director
Jennifer H. Madans, Ph.D., Associate Director
for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director
For e-mail updates on NCHS publication releases, subscribe online at: http://www.cdc.gov/nchs/govdelivery.htm.
For questions or general information about NCHS: Tel: 1–800–CDC–INFO (1–800–232–4636) • TTY: 1–888–232–6348
Internet: http://www.cdc.gov/nchs • Online request form: http://www.cdc.gov/cdc-info/requestform.html
DHHS Publication No. 2013–1250 • CS239260
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.