MGT603: System Thinking Report: Emergency Department Analysis
VerifiedAdded on 2022/09/29
|14
|3925
|43
Report
AI Summary
This report, based on a hypothetical scenario, examines the operational challenges within a public hospital's emergency department (ED). It identifies key issues such as long patient wait times, analyzed through the lens of system archetypes, including attractiveness principle, shifting the burden, fixes that fail, limits to success, and drifting goal. The report analyzes the current state value stream map, highlighting how these archetypes contribute to inefficiencies. A new state value stream map is proposed, emphasizing triage based on the Emergency Severity Index (ESI) levels to streamline patient flow and reduce turnaround time. The suggested map directs patients to specific care units (Critical, Intermediate, Alterna) based on their injury severity, followed by diagnostic testing and physician assessment. The report underscores the importance of addressing root causes rather than applying short-term fixes and concludes with recommendations to improve ED performance.

Running head: SYSTEM THINKING 1
System Thinking
Student’s Name
Institutional Affiliation
System Thinking
Student’s Name
Institutional Affiliation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
SYSTEM THINKING 2
System Thinking
Executive Summary
This report provides an overview of the hypothetical problem. Various archetypes are
known to affect the performance in the emergency department. This report seeks to identify
those archetypes that affect the performance in the emergency department of a public hospital
and closely examine them. This is done by first covering the complexities that exist in the
management of the emergency depart operations. The themes that are key in the management
of emergency operations are then identified. The report goes further to uses the system
thinking lens to propose an ideal solution to the problem before mentioning both the intended
and unintended consequences of the proposed solution. The report concludes with clear
recommendations that should be adopted to better performance in the emergency department.
Introduction
The scenario that this paper is based on requires one to consider himself as a member
of a team tasked to manage the emergency department operations in a public hospital. It’s the
routine for the public hospital’s emergency department to receive feedback from the patients
as a way of evaluating their services. Based on the patients’ feedback, most patients agree
that there is a need for waiting time in the emergency department to be improved. For the
waiting time to be improved, the functioning of the whole department needs to be examined.
The functioning of the department of the whole department is provided in the hospital’s value
map which provides both the material and the information flow in the hospital. The
functioning of the organization can be analyzed using System Archetypes. The use of system
archetypes to analyze the organization performance is necessary because it provides a view of
the organization’s behavior and links the system to the organization’s underlying structure
(Sujan, Huang & Braithwaite, 2017). The performance of the organization can be examined
System Thinking
Executive Summary
This report provides an overview of the hypothetical problem. Various archetypes are
known to affect the performance in the emergency department. This report seeks to identify
those archetypes that affect the performance in the emergency department of a public hospital
and closely examine them. This is done by first covering the complexities that exist in the
management of the emergency depart operations. The themes that are key in the management
of emergency operations are then identified. The report goes further to uses the system
thinking lens to propose an ideal solution to the problem before mentioning both the intended
and unintended consequences of the proposed solution. The report concludes with clear
recommendations that should be adopted to better performance in the emergency department.
Introduction
The scenario that this paper is based on requires one to consider himself as a member
of a team tasked to manage the emergency department operations in a public hospital. It’s the
routine for the public hospital’s emergency department to receive feedback from the patients
as a way of evaluating their services. Based on the patients’ feedback, most patients agree
that there is a need for waiting time in the emergency department to be improved. For the
waiting time to be improved, the functioning of the whole department needs to be examined.
The functioning of the department of the whole department is provided in the hospital’s value
map which provides both the material and the information flow in the hospital. The
functioning of the organization can be analyzed using System Archetypes. The use of system
archetypes to analyze the organization performance is necessary because it provides a view of
the organization’s behavior and links the system to the organization’s underlying structure
(Sujan, Huang & Braithwaite, 2017). The performance of the organization can be examined
SYSTEM THINKING 3
diagnostically. Also, the managers can use archetypes to recognize the patterns of behaviors
that currently exist in the organization (Behl & Ferreira, 2014).
Identification and analysis of the System Archetypes that may impede performance
As mentioned above system archetypes define the patterns in which the system
behaves. To understand how the system functions or operates and what affects its
performance, it’s important to identify and analyze system archetypes. Various types of
system archetypes that can affect the performance of an organization exits. In this paper, five
system archetypes that are capable of affecting performance in any organization are
discussed. Attractiveness principle is one of the system archetypes that can impede
performance. The attractiveness principle system archetype is taken to mean that since it’s
not possible to please all the people at the same time, one will be required to make choices by
taking sides (Bal, Ceylan & Taçoğlu, 2017). For example, some companies are known to rank
high on service delivery and price, but very low on quality. The general attractiveness of such
a company will be zero. From this description, its right to say that attractiveness principle
system archetype affects the performance of the organization by limiting the growth since an
organization cannot equally address all the limits to its system. Another archetype is shifting
the burden system archetype. In shifting the burden archetype, the existing problem in an
organization is solved by bringing an intervener (Doğan & Unutulmaz, 2016). However, the
intervener solves the problem by improving the situation on a short time basis after which the
problem worsens again. This is so because by bring an intervener, the root cause of the
problem is not identified and addressed properly (Dal Forno et al., 2014). This gives the
problem time to grow and worsen the situation in the company. This will affect the
performance in the company as more time will be wasted to address the problem using the
intervener on a short-time basis while the real problem is not solved.
diagnostically. Also, the managers can use archetypes to recognize the patterns of behaviors
that currently exist in the organization (Behl & Ferreira, 2014).
Identification and analysis of the System Archetypes that may impede performance
As mentioned above system archetypes define the patterns in which the system
behaves. To understand how the system functions or operates and what affects its
performance, it’s important to identify and analyze system archetypes. Various types of
system archetypes that can affect the performance of an organization exits. In this paper, five
system archetypes that are capable of affecting performance in any organization are
discussed. Attractiveness principle is one of the system archetypes that can impede
performance. The attractiveness principle system archetype is taken to mean that since it’s
not possible to please all the people at the same time, one will be required to make choices by
taking sides (Bal, Ceylan & Taçoğlu, 2017). For example, some companies are known to rank
high on service delivery and price, but very low on quality. The general attractiveness of such
a company will be zero. From this description, its right to say that attractiveness principle
system archetype affects the performance of the organization by limiting the growth since an
organization cannot equally address all the limits to its system. Another archetype is shifting
the burden system archetype. In shifting the burden archetype, the existing problem in an
organization is solved by bringing an intervener (Doğan & Unutulmaz, 2016). However, the
intervener solves the problem by improving the situation on a short time basis after which the
problem worsens again. This is so because by bring an intervener, the root cause of the
problem is not identified and addressed properly (Dal Forno et al., 2014). This gives the
problem time to grow and worsen the situation in the company. This will affect the
performance in the company as more time will be wasted to address the problem using the
intervener on a short-time basis while the real problem is not solved.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
SYSTEM THINKING 4
The third system archetype is the fixes that fail. In fixes that fail archetype, the urgent
problem in the organization is addressed using a rapidly implemented solution (Henrique et al.,
2016). This rapidly implemented solution is meant to quickly fix the problem. However, more
often, the problem is not fixed but instead, unintended consequences are produced (Henrique
et al., 2016). These consequences are not evident at first but with time, they cause serious
problems to the operations of the company. This will negatively affect the performance in the
company because the company will have to input a lot of resources and time to deal with the
unintended consequences that are produced by the quick fixes. The fourth system archetype is
limits to success. In limits to access the efforts that are applied to improve performance in the
company initially generate positive performance. But as time goes on, the general
performance in the company are slowed down as the efforts applied are affected by negative
forces in the organization (Jimmerson, 2017). The fifth system archetype that is drifting goal
archetype. The drifting goal archetype happens when an organization realizes that there is a
gap between its actual performance and its goals. Since the actual performance of the
organization cannot meet the set goal, the organization will be forced to lower its goal (Masys,
2015). This affects performance because by lowering the goal, the organization is promoting
low performance that can meet the lowered goals.
Analysis of the current State Value Stream Map of the emergency department based on
System Archetypes
Examining the current system value map of the emergency department provided, it’s
evident that various system archetypes affect the performance in the department. One such
system archetype is the goal drifting archetype. As mentioned above, the goal drifting
archetypes results when the performance of the organization is parallel to the set goals. From
the value stream map given, it can be understood that the main goal of the emergency
department is to provide effective emergency care to the patients at the shortest time possible
The third system archetype is the fixes that fail. In fixes that fail archetype, the urgent
problem in the organization is addressed using a rapidly implemented solution (Henrique et al.,
2016). This rapidly implemented solution is meant to quickly fix the problem. However, more
often, the problem is not fixed but instead, unintended consequences are produced (Henrique
et al., 2016). These consequences are not evident at first but with time, they cause serious
problems to the operations of the company. This will negatively affect the performance in the
company because the company will have to input a lot of resources and time to deal with the
unintended consequences that are produced by the quick fixes. The fourth system archetype is
limits to success. In limits to access the efforts that are applied to improve performance in the
company initially generate positive performance. But as time goes on, the general
performance in the company are slowed down as the efforts applied are affected by negative
forces in the organization (Jimmerson, 2017). The fifth system archetype that is drifting goal
archetype. The drifting goal archetype happens when an organization realizes that there is a
gap between its actual performance and its goals. Since the actual performance of the
organization cannot meet the set goal, the organization will be forced to lower its goal (Masys,
2015). This affects performance because by lowering the goal, the organization is promoting
low performance that can meet the lowered goals.
Analysis of the current State Value Stream Map of the emergency department based on
System Archetypes
Examining the current system value map of the emergency department provided, it’s
evident that various system archetypes affect the performance in the department. One such
system archetype is the goal drifting archetype. As mentioned above, the goal drifting
archetypes results when the performance of the organization is parallel to the set goals. From
the value stream map given, it can be understood that the main goal of the emergency
department is to provide effective emergency care to the patients at the shortest time possible
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
SYSTEM THINKING 5
because emergencies are delicate situations that require urgent attention. However, the
process of getting emergency care in the department takes too long because of the many
procedures that are involved. For example, every patient is required to undergo six intervals
of waiting periods before being treated by the doctor. Given how delicate emergencies are,
it’s justifiable to say that there are gaps between the actual performances of the department
with its goals. Another system archetype that affects the performance of this ED is limits to
success. From the value stream map provided, it’s evident that various efforts have been put
in place to improve the performance in the emergency department. For example, the
department has made efforts to get the insurance status of each of the patient’s injury. This
will improve performance because some patients cannot cater for their injuries, but since they
have insured those injuries, their treatment cannot proceed. However, these efforts to improve
performance have been met with the constraints of time as a lot of time is taken to check the
patient’s injury insurance status instead of commencing treatment. As a result, the
performance of the department has been slowed down by the efforts that were meant to
improve performance.
Another system archetype that is affecting the performance of the department based
on the value stream map provided is shifting the burden. From the value stream map
provided, it’s evident that the main problem of this department is long patient turnaround
time. However, Instead of the department focusing to find the root cause of the problem and
addressing it, the department introduced two positions which are the attending nurse and the
attending physician to attend to patients directly on behalf of the doctor. This might have
helped shortly, however, since the root cause of the problem was not identified and addressed
properly, the turnaround time of patients in the department was still long. Also, fixes that fail
archetypes exist in this department based on the value stream map provided. The fixes that
fail as described above happen when the solution meant to address the problem produces
because emergencies are delicate situations that require urgent attention. However, the
process of getting emergency care in the department takes too long because of the many
procedures that are involved. For example, every patient is required to undergo six intervals
of waiting periods before being treated by the doctor. Given how delicate emergencies are,
it’s justifiable to say that there are gaps between the actual performances of the department
with its goals. Another system archetype that affects the performance of this ED is limits to
success. From the value stream map provided, it’s evident that various efforts have been put
in place to improve the performance in the emergency department. For example, the
department has made efforts to get the insurance status of each of the patient’s injury. This
will improve performance because some patients cannot cater for their injuries, but since they
have insured those injuries, their treatment cannot proceed. However, these efforts to improve
performance have been met with the constraints of time as a lot of time is taken to check the
patient’s injury insurance status instead of commencing treatment. As a result, the
performance of the department has been slowed down by the efforts that were meant to
improve performance.
Another system archetype that is affecting the performance of the department based
on the value stream map provided is shifting the burden. From the value stream map
provided, it’s evident that the main problem of this department is long patient turnaround
time. However, Instead of the department focusing to find the root cause of the problem and
addressing it, the department introduced two positions which are the attending nurse and the
attending physician to attend to patients directly on behalf of the doctor. This might have
helped shortly, however, since the root cause of the problem was not identified and addressed
properly, the turnaround time of patients in the department was still long. Also, fixes that fail
archetypes exist in this department based on the value stream map provided. The fixes that
fail as described above happen when the solution meant to address the problem produces
SYSTEM THINKING 6
unintended consequences. From the value map provided, it’s evident that the section that
required the injury status of every patient to be checked before a patient proceeds to the
registration section was introduced to fix the problem of delayed treatment. This is so
because some patients cannot afford the cost of their treatment, but if such patients have
insured their injuries, they can be treated. However, the time taken to confirm the status of
the injury further added to the waiting time which contributes to the long turnaround of the
patients. This means that instead of solving the problem, the fixes introduced further
worsened the problem.
Recommended new State Value Stream Map with desired reduction in
Patient turnaround time
unintended consequences. From the value map provided, it’s evident that the section that
required the injury status of every patient to be checked before a patient proceeds to the
registration section was introduced to fix the problem of delayed treatment. This is so
because some patients cannot afford the cost of their treatment, but if such patients have
insured their injuries, they can be treated. However, the time taken to confirm the status of
the injury further added to the waiting time which contributes to the long turnaround of the
patients. This means that instead of solving the problem, the fixes introduced further
worsened the problem.
Recommended new State Value Stream Map with desired reduction in
Patient turnaround time
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
SYSTEM THINKING 7
Patient
Enter enters triage nurse section who sorts patients
based on the ESI levels
ESI-1 patient
Most severe injuries
ESI-2 patient
Severe injurie
ESI-3 patient
Require several tests
ESI-5 patien
Require no te
ESI-4 patient
Require one test
Intermediate care unit
Has less severe injuries
Elderly patient Young patient
Critical care unit
Has severe injuries that require
urgent action
Alterna care unit
Has minor injuries
MD assessment
Diagnostic testing
is done by a technician
Follow up treatment Patient leaves the ED Patient is discharge
from ED
Is
Diagnostic
test
required?
Yes
No
Patient
Enter enters triage nurse section who sorts patients
based on the ESI levels
ESI-1 patient
Most severe injuries
ESI-2 patient
Severe injurie
ESI-3 patient
Require several tests
ESI-5 patien
Require no te
ESI-4 patient
Require one test
Intermediate care unit
Has less severe injuries
Elderly patient Young patient
Critical care unit
Has severe injuries that require
urgent action
Alterna care unit
Has minor injuries
MD assessment
Diagnostic testing
is done by a technician
Follow up treatment Patient leaves the ED Patient is discharge
from ED
Is
Diagnostic
test
required?
Yes
No
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
SYSTEM THINKING 8
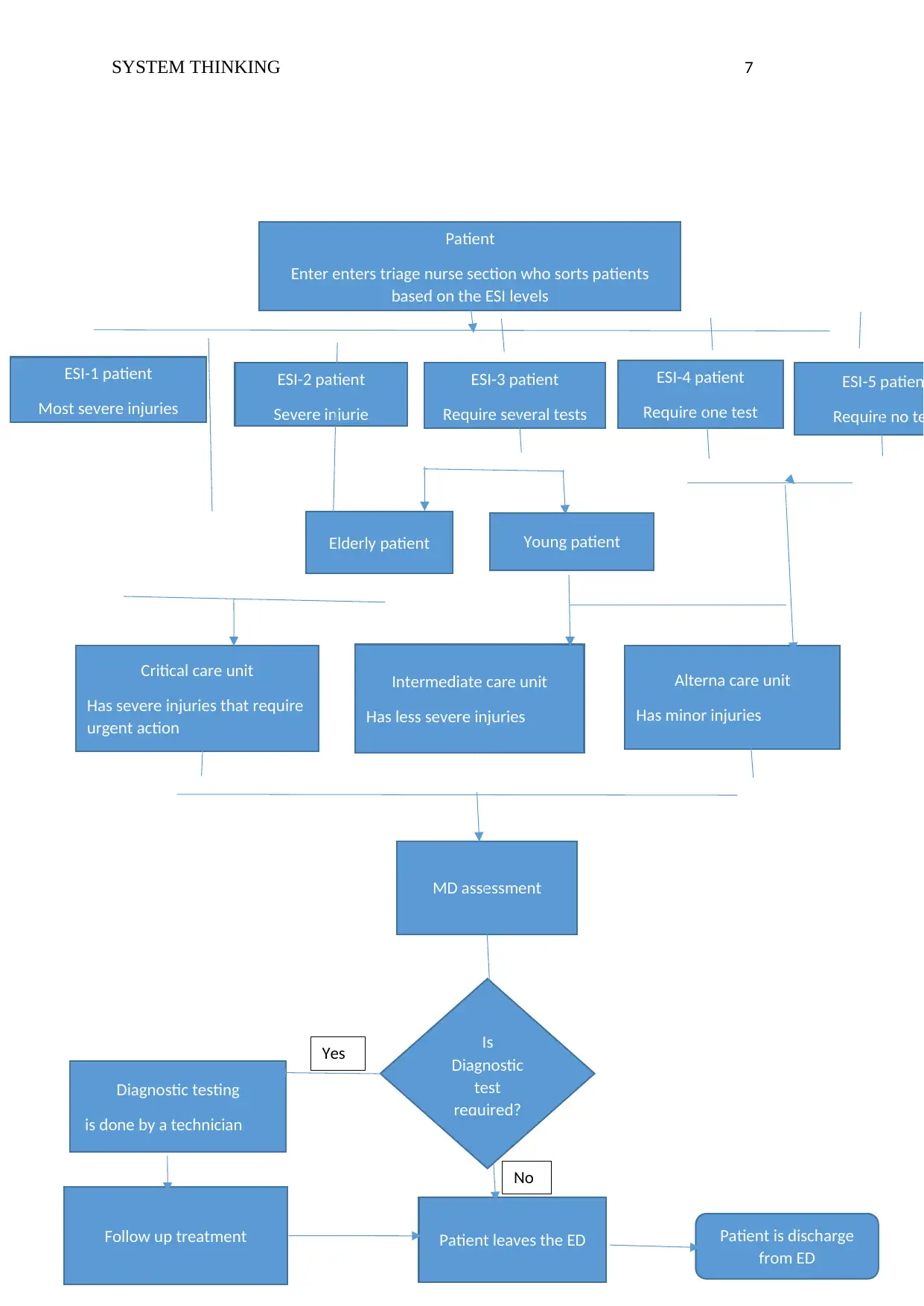
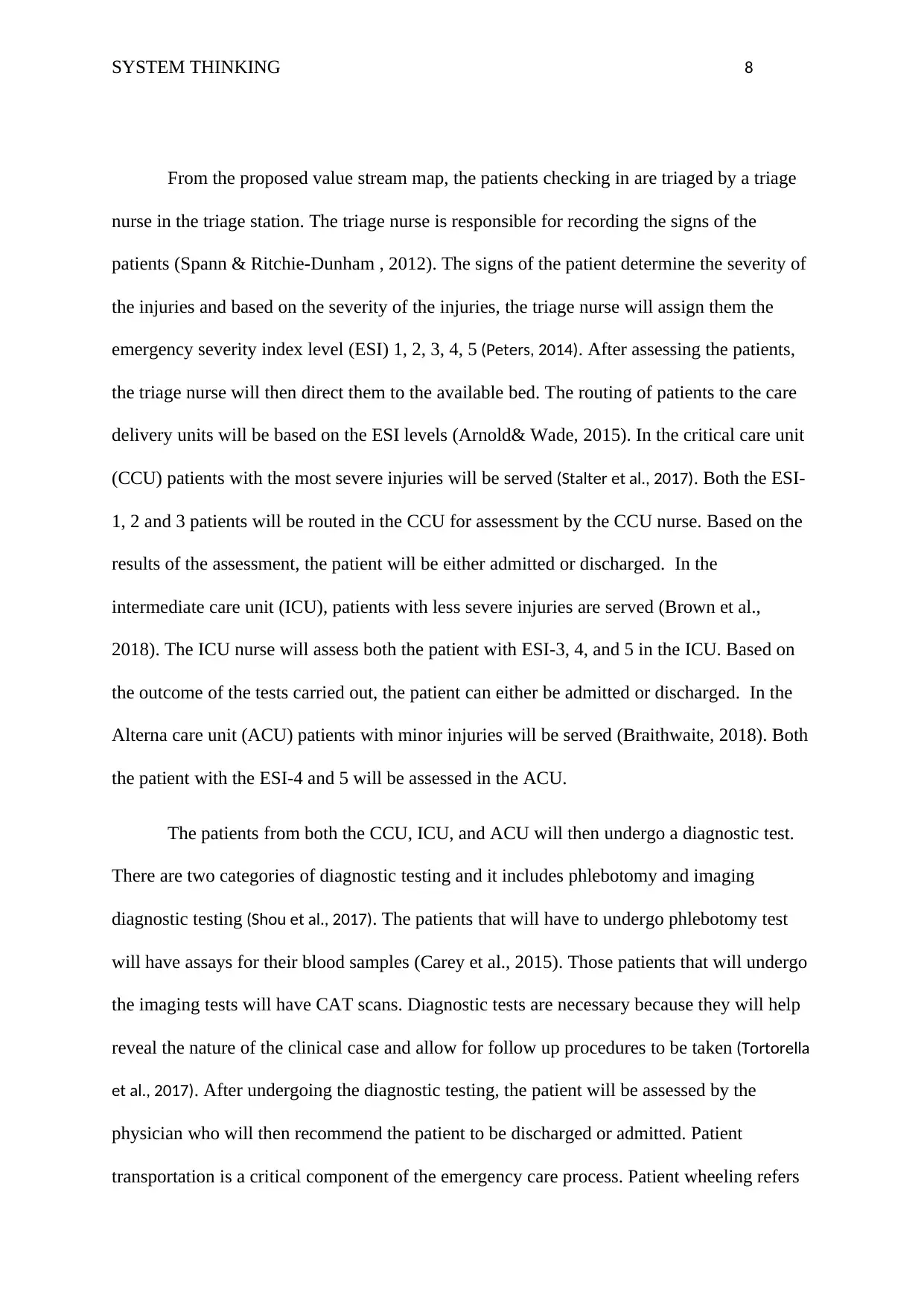
From the proposed value stream map, the patients checking in are triaged by a triage
nurse in the triage station. The triage nurse is responsible for recording the signs of the
patients (Spann & Ritchie-Dunham , 2012). The signs of the patient determine the severity of
the injuries and based on the severity of the injuries, the triage nurse will assign them the
emergency severity index level (ESI) 1, 2, 3, 4, 5 (Peters, 2014). After assessing the patients,
the triage nurse will then direct them to the available bed. The routing of patients to the care
delivery units will be based on the ESI levels (Arnold& Wade, 2015). In the critical care unit
(CCU) patients with the most severe injuries will be served (Stalter et al., 2017). Both the ESI-
1, 2 and 3 patients will be routed in the CCU for assessment by the CCU nurse. Based on the
results of the assessment, the patient will be either admitted or discharged. In the
intermediate care unit (ICU), patients with less severe injuries are served (Brown et al.,
2018). The ICU nurse will assess both the patient with ESI-3, 4, and 5 in the ICU. Based on
the outcome of the tests carried out, the patient can either be admitted or discharged. In the
Alterna care unit (ACU) patients with minor injuries will be served (Braithwaite, 2018). Both
the patient with the ESI-4 and 5 will be assessed in the ACU.
The patients from both the CCU, ICU, and ACU will then undergo a diagnostic test.
There are two categories of diagnostic testing and it includes phlebotomy and imaging
diagnostic testing (Shou et al., 2017). The patients that will have to undergo phlebotomy test
will have assays for their blood samples (Carey et al., 2015). Those patients that will undergo
the imaging tests will have CAT scans. Diagnostic tests are necessary because they will help
reveal the nature of the clinical case and allow for follow up procedures to be taken (Tortorella
et al., 2017). After undergoing the diagnostic testing, the patient will be assessed by the
physician who will then recommend the patient to be discharged or admitted. Patient
transportation is a critical component of the emergency care process. Patient wheeling refers
From the proposed value stream map, the patients checking in are triaged by a triage
nurse in the triage station. The triage nurse is responsible for recording the signs of the
patients (Spann & Ritchie-Dunham , 2012). The signs of the patient determine the severity of
the injuries and based on the severity of the injuries, the triage nurse will assign them the
emergency severity index level (ESI) 1, 2, 3, 4, 5 (Peters, 2014). After assessing the patients,
the triage nurse will then direct them to the available bed. The routing of patients to the care
delivery units will be based on the ESI levels (Arnold& Wade, 2015). In the critical care unit
(CCU) patients with the most severe injuries will be served (Stalter et al., 2017). Both the ESI-
1, 2 and 3 patients will be routed in the CCU for assessment by the CCU nurse. Based on the
results of the assessment, the patient will be either admitted or discharged. In the
intermediate care unit (ICU), patients with less severe injuries are served (Brown et al.,
2018). The ICU nurse will assess both the patient with ESI-3, 4, and 5 in the ICU. Based on
the outcome of the tests carried out, the patient can either be admitted or discharged. In the
Alterna care unit (ACU) patients with minor injuries will be served (Braithwaite, 2018). Both
the patient with the ESI-4 and 5 will be assessed in the ACU.
The patients from both the CCU, ICU, and ACU will then undergo a diagnostic test.
There are two categories of diagnostic testing and it includes phlebotomy and imaging
diagnostic testing (Shou et al., 2017). The patients that will have to undergo phlebotomy test
will have assays for their blood samples (Carey et al., 2015). Those patients that will undergo
the imaging tests will have CAT scans. Diagnostic tests are necessary because they will help
reveal the nature of the clinical case and allow for follow up procedures to be taken (Tortorella
et al., 2017). After undergoing the diagnostic testing, the patient will be assessed by the
physician who will then recommend the patient to be discharged or admitted. Patient
transportation is a critical component of the emergency care process. Patient wheeling refers
SYSTEM THINKING 9
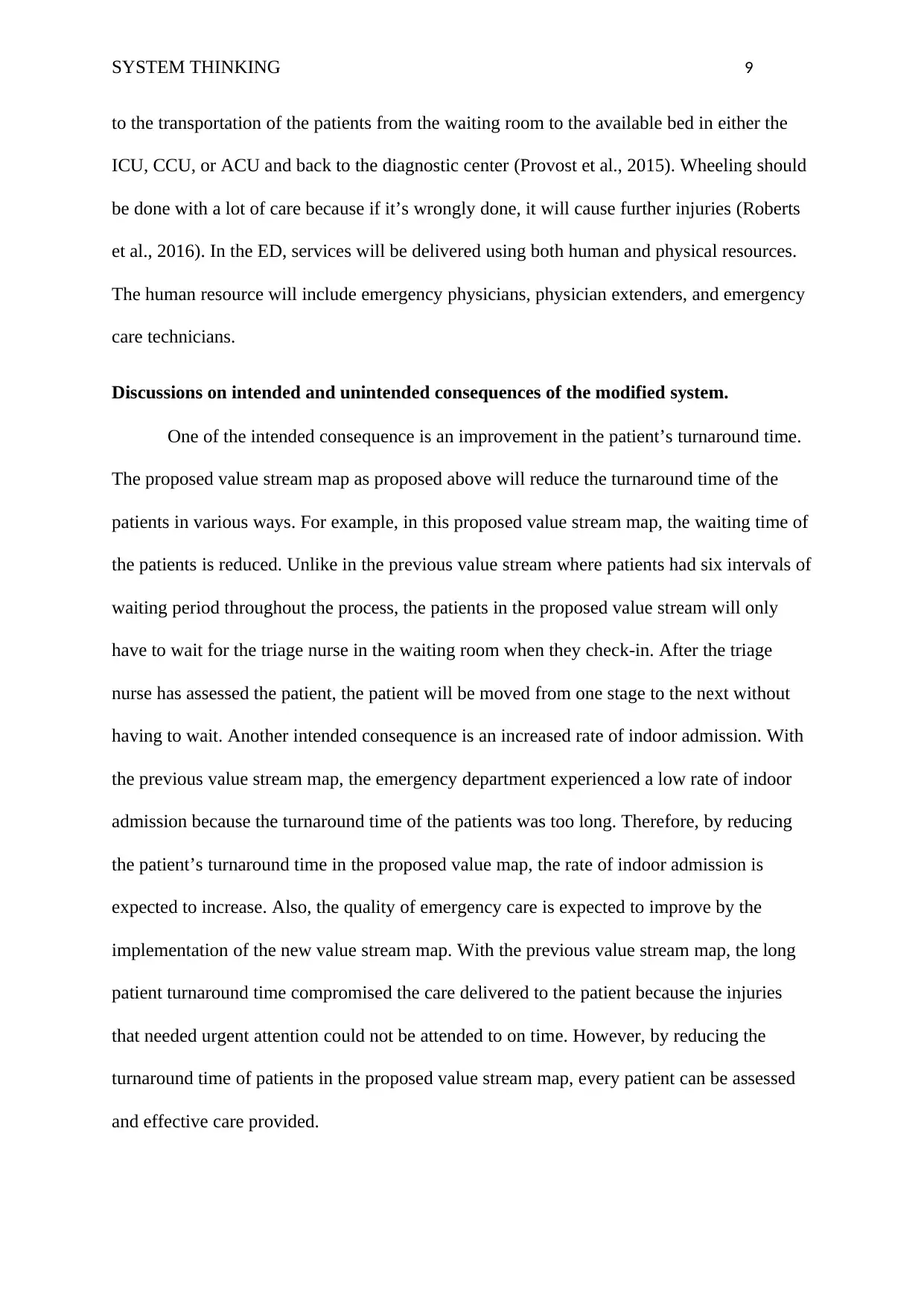
to the transportation of the patients from the waiting room to the available bed in either the
ICU, CCU, or ACU and back to the diagnostic center (Provost et al., 2015). Wheeling should
be done with a lot of care because if it’s wrongly done, it will cause further injuries (Roberts
et al., 2016). In the ED, services will be delivered using both human and physical resources.
The human resource will include emergency physicians, physician extenders, and emergency
care technicians.
Discussions on intended and unintended consequences of the modified system.
One of the intended consequence is an improvement in the patient’s turnaround time.
The proposed value stream map as proposed above will reduce the turnaround time of the
patients in various ways. For example, in this proposed value stream map, the waiting time of
the patients is reduced. Unlike in the previous value stream where patients had six intervals of
waiting period throughout the process, the patients in the proposed value stream will only
have to wait for the triage nurse in the waiting room when they check-in. After the triage
nurse has assessed the patient, the patient will be moved from one stage to the next without
having to wait. Another intended consequence is an increased rate of indoor admission. With
the previous value stream map, the emergency department experienced a low rate of indoor
admission because the turnaround time of the patients was too long. Therefore, by reducing
the patient’s turnaround time in the proposed value map, the rate of indoor admission is
expected to increase. Also, the quality of emergency care is expected to improve by the
implementation of the new value stream map. With the previous value stream map, the long
patient turnaround time compromised the care delivered to the patient because the injuries
that needed urgent attention could not be attended to on time. However, by reducing the
turnaround time of patients in the proposed value stream map, every patient can be assessed
and effective care provided.
to the transportation of the patients from the waiting room to the available bed in either the
ICU, CCU, or ACU and back to the diagnostic center (Provost et al., 2015). Wheeling should
be done with a lot of care because if it’s wrongly done, it will cause further injuries (Roberts
et al., 2016). In the ED, services will be delivered using both human and physical resources.
The human resource will include emergency physicians, physician extenders, and emergency
care technicians.
Discussions on intended and unintended consequences of the modified system.
One of the intended consequence is an improvement in the patient’s turnaround time.
The proposed value stream map as proposed above will reduce the turnaround time of the
patients in various ways. For example, in this proposed value stream map, the waiting time of
the patients is reduced. Unlike in the previous value stream where patients had six intervals of
waiting period throughout the process, the patients in the proposed value stream will only
have to wait for the triage nurse in the waiting room when they check-in. After the triage
nurse has assessed the patient, the patient will be moved from one stage to the next without
having to wait. Another intended consequence is an increased rate of indoor admission. With
the previous value stream map, the emergency department experienced a low rate of indoor
admission because the turnaround time of the patients was too long. Therefore, by reducing
the patient’s turnaround time in the proposed value map, the rate of indoor admission is
expected to increase. Also, the quality of emergency care is expected to improve by the
implementation of the new value stream map. With the previous value stream map, the long
patient turnaround time compromised the care delivered to the patient because the injuries
that needed urgent attention could not be attended to on time. However, by reducing the
turnaround time of patients in the proposed value stream map, every patient can be assessed
and effective care provided.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
SYSTEM THINKING 10
The main unintended consequence of this proposed system is for it to result in long
waits among the patients in the ED. The reason for developing this new value stream map
was to help reduce the turnaround time of the patient in the emergency department.
Therefore, it’s not expected that instead of reducing the turnaround time, the new value
stream map will make it even longer.
Conclusion
This report seeks to identify those archetypes that affect the performance in the
emergency department of a public hospital and closely examine them. This is done by first,
covering the complexities that exist in the management of the emergency depart operations.
Based on the patients’ feedback, there is a need for waiting time in the emergency department
to be improved. For the waiting time to be improved, the functioning of the whole department
needs to be examined in relation to system archetypes. This is so because various types of
system archetypes can affect the performance in an organization. Based on the value stream
provided, the system archetypes that affect the performance of the emergency department
include the goal drifting archetype, limits to success, limits to success, and fixes that fail. The
proposed value stream map will reduce the patient’s turnaround time by eliminating waiting
time as much as possible through the smooth flow of information throughout the department.
Recommendations
This paper recommends that emergency care should be provided to patients with
emergencies only. All patients presented or presenting themselves in the ED should be
assessed by the triage nurse to determine their level of injuries and ascertain whether they
require emergency care. Patients found not eligible for emergency care should be turned
away. This is important because it will help reduce congestion which contributes to long
waits that affect performance in the ED. Also, this paper recommends that the qualified
The main unintended consequence of this proposed system is for it to result in long
waits among the patients in the ED. The reason for developing this new value stream map
was to help reduce the turnaround time of the patient in the emergency department.
Therefore, it’s not expected that instead of reducing the turnaround time, the new value
stream map will make it even longer.
Conclusion
This report seeks to identify those archetypes that affect the performance in the
emergency department of a public hospital and closely examine them. This is done by first,
covering the complexities that exist in the management of the emergency depart operations.
Based on the patients’ feedback, there is a need for waiting time in the emergency department
to be improved. For the waiting time to be improved, the functioning of the whole department
needs to be examined in relation to system archetypes. This is so because various types of
system archetypes can affect the performance in an organization. Based on the value stream
provided, the system archetypes that affect the performance of the emergency department
include the goal drifting archetype, limits to success, limits to success, and fixes that fail. The
proposed value stream map will reduce the patient’s turnaround time by eliminating waiting
time as much as possible through the smooth flow of information throughout the department.
Recommendations
This paper recommends that emergency care should be provided to patients with
emergencies only. All patients presented or presenting themselves in the ED should be
assessed by the triage nurse to determine their level of injuries and ascertain whether they
require emergency care. Patients found not eligible for emergency care should be turned
away. This is important because it will help reduce congestion which contributes to long
waits that affect performance in the ED. Also, this paper recommends that the qualified
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
SYSTEM THINKING 11
physicians, the nurses and other personnel that work in the emergency department must
always be available throughout the day and night. This is so because the emergencies happen
unexpectedly. This means that emergency providers should be available to handle the
emergency whenever it arises.
physicians, the nurses and other personnel that work in the emergency department must
always be available throughout the day and night. This is so because the emergencies happen
unexpectedly. This means that emergency providers should be available to handle the
emergency whenever it arises.
SYSTEM THINKING 12
Reference
Arnold, R. D., & Wade, J. P. (2015). A definition of systems thinking: A systems
approach. Procedia Computer Science, 44, 669-678.
Behl, D. V., & Ferreira, S. (2014). Systems thinking: An analysis of key factors and
relationships. Procedia Computer Science, 36, 104-109.
Bal, A., Ceylan, C., & Taçoğlu, C. (2017). Using value stream mapping and discrete event
simulation to improve efficiency of emergency departments. International Journal of
Healthcare Management, 10(3), 196-206.
Brown, G., Reeders, D., Cogle, A., Madden, A., Kim, J., & O'Donnell, D. (2018). A systems
thinking approach to understanding and demonstrating the role of peer-led programs
and leadership in the response to HIV and hepatitis C: findings from the W3
project. Frontiers in public health, 6.
Braithwaite, J. (2018). Changing how we think about healthcare improvement. bmj, 361,
k2014.
Carey, G., Malbon, E., Carey, N., Joyce, A., Crammond, B., & Carey, A. (2015). Systems
science and systems thinking for public health: a systematic review of the field. BMJ
open, 5(12), e009002.
Doğan, N. Ö., & Unutulmaz, O. (2016). Lean production in healthcare: a simulation-based
value stream mapping in the physical therapy and rehabilitation department of a
public hospital. Total Quality Management & Business Excellence, 27(1-2), 64-80.
Reference
Arnold, R. D., & Wade, J. P. (2015). A definition of systems thinking: A systems
approach. Procedia Computer Science, 44, 669-678.
Behl, D. V., & Ferreira, S. (2014). Systems thinking: An analysis of key factors and
relationships. Procedia Computer Science, 36, 104-109.
Bal, A., Ceylan, C., & Taçoğlu, C. (2017). Using value stream mapping and discrete event
simulation to improve efficiency of emergency departments. International Journal of
Healthcare Management, 10(3), 196-206.
Brown, G., Reeders, D., Cogle, A., Madden, A., Kim, J., & O'Donnell, D. (2018). A systems
thinking approach to understanding and demonstrating the role of peer-led programs
and leadership in the response to HIV and hepatitis C: findings from the W3
project. Frontiers in public health, 6.
Braithwaite, J. (2018). Changing how we think about healthcare improvement. bmj, 361,
k2014.
Carey, G., Malbon, E., Carey, N., Joyce, A., Crammond, B., & Carey, A. (2015). Systems
science and systems thinking for public health: a systematic review of the field. BMJ
open, 5(12), e009002.
Doğan, N. Ö., & Unutulmaz, O. (2016). Lean production in healthcare: a simulation-based
value stream mapping in the physical therapy and rehabilitation department of a
public hospital. Total Quality Management & Business Excellence, 27(1-2), 64-80.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.