Research Methods in Health: A Literature Review on Indian EMS System
VerifiedAdded on 2023/06/05
|31
|5318
|78
Literature Review
AI Summary
This literature review examines the state of Emergency Medical Services (EMS) in India, highlighting the increasing mortality and morbidity rates due to injuries and non-communicable diseases. It emphasizes the need for urgent improvements in emergency services to prevent unnecessary deaths and disabilities. The review explores the fragmented and uncoordinated nature of EMS in India, citing issues such as lack of standardization, absence of regulation, and varying quality of services. It discusses the role of public, private, and non-profit sectors in providing pre-hospital services, including the challenges of awareness and access to emergency numbers. The review also addresses the government's initiatives in reinforcing emergency referral services and the implementation of public-private partnerships. It highlights the barriers to efficient EMS, including cultural differences, poor infrastructure, and communication issues. Furthermore, the review suggests potential solutions such as strengthening existing networks, standardizing procedures, and establishing a centralized medical emergency authority. The literature also explores the need for increased funding, better integration and coordination among existing services, and the importance of public and private partnerships. The document concludes by emphasizing the need for further research to enhance the understanding of EMS in India and its connection to various factors.

1
NAME OF THE STUDENT-SHARU JACOB
STUDENT ID-n10031561
SUBJECT NAME-RESEARCH METHODS IN HEALTH
NAME OF THE STUDENT-SHARU JACOB
STUDENT ID-n10031561
SUBJECT NAME-RESEARCH METHODS IN HEALTH
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
Literature Review
Several studies suggested that mortality and morbidity rate is increasing due to injuries and non-
communicable disease in low and middle income countries including India which suggests that
emergency services needs to be improved urgently to prevent needless death and disability
(Hirshon, et al., 2013) (Kotagal, et al., 2014). Rajdou, Mahajan and Balinga further supported
this notion by stating that the trauma structure in India still needs massive improvements. They
also presented the data that seriously injured people in India have six times more chances to
expire as compared to other nations with improved and efficient trauma structure. These
countries offer early referral to absolute care leads to better outcome and reduction in poor
outcomes (Radjou, Mahajan, & Baliga, 2013). On overlooking, the specific flaws in the EMS of
India, two of the studies conducted by Garg and Subhan; Jain called the emergency medical
services in India as fragmented (Subhan & Jain, 2010) (Garg, 2012). Further another study
conducted by Sriram et. al. called the EMS in India as fragmented, uncoordinated, and of poor
quality. In Sriram et.al, study, it was concluded that the stakeholders informed about an absence
of regulation and standardization of EMS facilities at the national and regional level in the given
hospital. They observed that most of the organizations independently planned and executed their
EMT training programs as per their requirements without any accreditation from a national
institution or authority. Further, the trainees were also not needed to get a certification from
external institutions (Sriram, Gururaj, Razzak, Naseer, & Hyder, 2016). Another study outlined
that the pre-hospital services in India are provided by several providers from public, for-profit
and non-profit sectors, with are varying from extremely basic patient transport to highly
specialized, mobile coronary care units. The study also found out that majority of the people
Literature Review
Several studies suggested that mortality and morbidity rate is increasing due to injuries and non-
communicable disease in low and middle income countries including India which suggests that
emergency services needs to be improved urgently to prevent needless death and disability
(Hirshon, et al., 2013) (Kotagal, et al., 2014). Rajdou, Mahajan and Balinga further supported
this notion by stating that the trauma structure in India still needs massive improvements. They
also presented the data that seriously injured people in India have six times more chances to
expire as compared to other nations with improved and efficient trauma structure. These
countries offer early referral to absolute care leads to better outcome and reduction in poor
outcomes (Radjou, Mahajan, & Baliga, 2013). On overlooking, the specific flaws in the EMS of
India, two of the studies conducted by Garg and Subhan; Jain called the emergency medical
services in India as fragmented (Subhan & Jain, 2010) (Garg, 2012). Further another study
conducted by Sriram et. al. called the EMS in India as fragmented, uncoordinated, and of poor
quality. In Sriram et.al, study, it was concluded that the stakeholders informed about an absence
of regulation and standardization of EMS facilities at the national and regional level in the given
hospital. They observed that most of the organizations independently planned and executed their
EMT training programs as per their requirements without any accreditation from a national
institution or authority. Further, the trainees were also not needed to get a certification from
external institutions (Sriram, Gururaj, Razzak, Naseer, & Hyder, 2016). Another study outlined
that the pre-hospital services in India are provided by several providers from public, for-profit
and non-profit sectors, with are varying from extremely basic patient transport to highly
specialized, mobile coronary care units. The study also found out that majority of the people
3
have no awareness of the number to call in case of an emergency such as Dial 108/102/1298
Ambulances, Centralized Accident and Trauma Service (CATS), private ambulance models are
available with a wide range of dispatch and transport facilities. (Sharma & Brandler, 2014).
Another significant aspect of emergency medical service is the emergency referral services.
Government of India has taken initiative to reinforce emergency referral services to enhance the
reach for facility-based intrapartum service delivery. Government has designed and planned
several models for executing the service based on the health infrastructure and several other
aspects of different states (Shankar Prinja, et al., 2014). ERS, which is implemented in all the
states, is publicly financed however, the mechanism of delivery differs. For example, in states of
Jharkhand, Gujarat, Madhya Pradesh and Haryana, delivery of ERS is publicly managed while in
states like Bihar, Kerala, Rajasthan and Punjab ERS provision is based on public-private
partnership (PPP) mode with public funding and private delivery (Sundararaman, Chakraborty,
Nair, Mokashi, & Ved, 2012). However, another study contradicts the findings and identifies the
ERS of India as poor. The study found that often the emergency patients are referred government
hospitals which leads to wasting of the crucial time which could save patient’s life or improve
health outcomes. Further, for the government hospitals, the study reported that there are no well-
defined distinction of roles and responsibilities in emergency department (Garg, 2012).
In public as well as private sector, a failure of integration and standardization with regards to
human resources and regulation within leadership and governance is observed. Due to lack of
standardization, the organizations were free to set their own objectives which resulted in diverse
range of strategies and approaches. It further led to the conclusion that the EMS scenario in India
persists to be fragmented, with least control over the quantity or quality of services. As there is a
lack of sufficient governing systems at the national or sub-national levels, the duty for
have no awareness of the number to call in case of an emergency such as Dial 108/102/1298
Ambulances, Centralized Accident and Trauma Service (CATS), private ambulance models are
available with a wide range of dispatch and transport facilities. (Sharma & Brandler, 2014).
Another significant aspect of emergency medical service is the emergency referral services.
Government of India has taken initiative to reinforce emergency referral services to enhance the
reach for facility-based intrapartum service delivery. Government has designed and planned
several models for executing the service based on the health infrastructure and several other
aspects of different states (Shankar Prinja, et al., 2014). ERS, which is implemented in all the
states, is publicly financed however, the mechanism of delivery differs. For example, in states of
Jharkhand, Gujarat, Madhya Pradesh and Haryana, delivery of ERS is publicly managed while in
states like Bihar, Kerala, Rajasthan and Punjab ERS provision is based on public-private
partnership (PPP) mode with public funding and private delivery (Sundararaman, Chakraborty,
Nair, Mokashi, & Ved, 2012). However, another study contradicts the findings and identifies the
ERS of India as poor. The study found that often the emergency patients are referred government
hospitals which leads to wasting of the crucial time which could save patient’s life or improve
health outcomes. Further, for the government hospitals, the study reported that there are no well-
defined distinction of roles and responsibilities in emergency department (Garg, 2012).
In public as well as private sector, a failure of integration and standardization with regards to
human resources and regulation within leadership and governance is observed. Due to lack of
standardization, the organizations were free to set their own objectives which resulted in diverse
range of strategies and approaches. It further led to the conclusion that the EMS scenario in India
persists to be fragmented, with least control over the quantity or quality of services. As there is a
lack of sufficient governing systems at the national or sub-national levels, the duty for
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
emergency care systems is dispersed across a range of public and private actors, without a
compulsory force linking these factors and eventually directing the system. Public sector support
for services seems to be central to the long-term financial sustainability of EMS organizations.
However, the laws and public policy regarding EMS is either lacking or poorly imposed in India.
In addition, for improvement in the current EMS scenario in India, more regular and increased
funding will be required. Further, there is need for integration and coordination among existing
services, and better organization and leadership. It can be achieved by making EMS
administration and leadership a more desired career choice. (Nielsen, et al., 2012).
It is essential that the guidelines by the Supreme Court of India must be compulsorily presented
publicly at emergency in order to remind doctors of their responsibilities and rights and the
patients could get the required care easily. When they fails to provide the needed fund and
assistance then it must come in the notice of people by auditing through authorized audit
companies.
Another study identified the barriers to implementing efficient EMS which were classified into
six divisions and those were culture differences, poor infrastructure, inefficient communication
resulting in ill-coordination, lack of transport, equipment and human resource (Kironji, et al.,
2018). Another study supported the argument by revealing that seriously injured patients miss
useful prehospital time in the emergency as there is lack of guidance about destination and inter
facility transfer, absence of efficient transportation, and no concept of initial trauma care
(Radjou, Mahajan, & Baliga, 2013). The extension of EMS especially in rural areas or under
reach areas can be done by making use of the already present systems of first responders which
are mostly the commercial drivers and lay persons. Initiatives can be taken to improve their
efficiency by providing them more comprehensive first aid training, and better including their
emergency care systems is dispersed across a range of public and private actors, without a
compulsory force linking these factors and eventually directing the system. Public sector support
for services seems to be central to the long-term financial sustainability of EMS organizations.
However, the laws and public policy regarding EMS is either lacking or poorly imposed in India.
In addition, for improvement in the current EMS scenario in India, more regular and increased
funding will be required. Further, there is need for integration and coordination among existing
services, and better organization and leadership. It can be achieved by making EMS
administration and leadership a more desired career choice. (Nielsen, et al., 2012).
It is essential that the guidelines by the Supreme Court of India must be compulsorily presented
publicly at emergency in order to remind doctors of their responsibilities and rights and the
patients could get the required care easily. When they fails to provide the needed fund and
assistance then it must come in the notice of people by auditing through authorized audit
companies.
Another study identified the barriers to implementing efficient EMS which were classified into
six divisions and those were culture differences, poor infrastructure, inefficient communication
resulting in ill-coordination, lack of transport, equipment and human resource (Kironji, et al.,
2018). Another study supported the argument by revealing that seriously injured patients miss
useful prehospital time in the emergency as there is lack of guidance about destination and inter
facility transfer, absence of efficient transportation, and no concept of initial trauma care
(Radjou, Mahajan, & Baliga, 2013). The extension of EMS especially in rural areas or under
reach areas can be done by making use of the already present systems of first responders which
are mostly the commercial drivers and lay persons. Initiatives can be taken to improve their
efficiency by providing them more comprehensive first aid training, and better including their
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
endeavors within formal EMS, are necessary. Another study also supports this idea that
strengthening the existing network of unofficial sources of drivers and police and with training,
funding fast transport with taxes on roads and vehicle fuels and standardizing the private
ambulance providers. It could be more cost-effective in a society in which assisting and helping
others is not just wanted, but is essential for general financial survival (Roy, et al., 2010).
The Government of Delhi in an attempt to address the issue of uncoordinated EMS set up the
Centralized Accidents and Trauma Services (CATS) in the early 1990s. CATS were
subsequently set up across the whole country. However, it fail to provide any reasonable gains
and failed in spite of having a toll free number -102 which is the emergency telephone number
for ambulance in several parts of India. But, there are different emergency numbers in different
states and Union Territories. Therefore, there is a critical requirement of a centralized Medical
Emergency authority that will be responsible for providing guidelines for introducing emergency
services with a single telephone number throughout the country. The centralized body can serve
several essential purpose such as planning protocols, granting technical support, training,
capacity creation, and certification of emergency services. Several studies have identified the
need of standardization of procedures, guidelines, and personal competencies along with creation
of law in parliament to offer legal safeguard for the workers in emergency services. For example,
Government of Gujarat state took the initiative by introducing the Gujarat Emergency Medical
Services Authority. It is a required measure in the correct direction. Gujarat was the first state to
truly pass emergency services regulation in India. Although in Gujarat, a statewide system of
emergency care by integrating government, non-government organizations (NGOs), and other
private firms, has been established (Subhan & Jain, 2010). In India if different working bodies
such as Securities and Exchange Board of India, Telecom Regulatory Authority of India, and
endeavors within formal EMS, are necessary. Another study also supports this idea that
strengthening the existing network of unofficial sources of drivers and police and with training,
funding fast transport with taxes on roads and vehicle fuels and standardizing the private
ambulance providers. It could be more cost-effective in a society in which assisting and helping
others is not just wanted, but is essential for general financial survival (Roy, et al., 2010).
The Government of Delhi in an attempt to address the issue of uncoordinated EMS set up the
Centralized Accidents and Trauma Services (CATS) in the early 1990s. CATS were
subsequently set up across the whole country. However, it fail to provide any reasonable gains
and failed in spite of having a toll free number -102 which is the emergency telephone number
for ambulance in several parts of India. But, there are different emergency numbers in different
states and Union Territories. Therefore, there is a critical requirement of a centralized Medical
Emergency authority that will be responsible for providing guidelines for introducing emergency
services with a single telephone number throughout the country. The centralized body can serve
several essential purpose such as planning protocols, granting technical support, training,
capacity creation, and certification of emergency services. Several studies have identified the
need of standardization of procedures, guidelines, and personal competencies along with creation
of law in parliament to offer legal safeguard for the workers in emergency services. For example,
Government of Gujarat state took the initiative by introducing the Gujarat Emergency Medical
Services Authority. It is a required measure in the correct direction. Gujarat was the first state to
truly pass emergency services regulation in India. Although in Gujarat, a statewide system of
emergency care by integrating government, non-government organizations (NGOs), and other
private firms, has been established (Subhan & Jain, 2010). In India if different working bodies
such as Securities and Exchange Board of India, Telecom Regulatory Authority of India, and
6
Insurance Regulatory and Development Authority to standardize share market, telecom, and
insurance services, respectively, then establishing a governing authority for standardizing the
health services, especially the emergencies, can also be taken seriously.
One study suggested that public and private partnerships can be significant in executing a
structured prehospital care system in India which can be a justifiable solution for improving
EMS (Sharma & Brandler, 2014). Another study revealed that Public-Private Partnership mode
can be an option to move forward to improve the quality and expand the reach of EMS in India
(Gupta & Basu, 2014). But the organizers of private firms have showed apprehension that if the
collaboration with the government will achieve the desired goal of expanding the scope of EMS
throughout India at a reasonable price. One of the case study revealed that the hospitals adheres
to the regulated model across the states and union territories where they have contractual
arrangements. Procedures for fleet handling, information systems and training, and placement
were efficiently organized at the organizational stage. The public-private partnership seems poor
in direction. This study supports the implementation of Public-Private Partnership mode.
However another study also raised a debatable issue that whether the state-funded EMS scheme
will be sufficiently strong a poorly resourced facility in which public hospitals are ill-funded
(Gupta & Basu, 2014). Further, one of the studies concluded that due to lack of an EMS system
currently, the prehospital care is the responsibility of the citizen which he/she fulfills by using
societal associations. It is essential to stop this system and move this responsibility to the state.
The arguable point is whether the state-funded EMS system will be strong enough in a setting,
which is poor in resources where public hospitals are ill-funded. (Roy, et al., 2010). Even though
trauma is a commonly recognized public health issue, its primary prevention has lingered in the
field of town organizers and railroad constructers and developers. A combined research on
Insurance Regulatory and Development Authority to standardize share market, telecom, and
insurance services, respectively, then establishing a governing authority for standardizing the
health services, especially the emergencies, can also be taken seriously.
One study suggested that public and private partnerships can be significant in executing a
structured prehospital care system in India which can be a justifiable solution for improving
EMS (Sharma & Brandler, 2014). Another study revealed that Public-Private Partnership mode
can be an option to move forward to improve the quality and expand the reach of EMS in India
(Gupta & Basu, 2014). But the organizers of private firms have showed apprehension that if the
collaboration with the government will achieve the desired goal of expanding the scope of EMS
throughout India at a reasonable price. One of the case study revealed that the hospitals adheres
to the regulated model across the states and union territories where they have contractual
arrangements. Procedures for fleet handling, information systems and training, and placement
were efficiently organized at the organizational stage. The public-private partnership seems poor
in direction. This study supports the implementation of Public-Private Partnership mode.
However another study also raised a debatable issue that whether the state-funded EMS scheme
will be sufficiently strong a poorly resourced facility in which public hospitals are ill-funded
(Gupta & Basu, 2014). Further, one of the studies concluded that due to lack of an EMS system
currently, the prehospital care is the responsibility of the citizen which he/she fulfills by using
societal associations. It is essential to stop this system and move this responsibility to the state.
The arguable point is whether the state-funded EMS system will be strong enough in a setting,
which is poor in resources where public hospitals are ill-funded. (Roy, et al., 2010). Even though
trauma is a commonly recognized public health issue, its primary prevention has lingered in the
field of town organizers and railroad constructers and developers. A combined research on
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
primary prevention of road traffic accidents, domestic injuries, industrial trauma and civil mass
fatality has not been conducted in India to this point. Therefore, further research is needed in
future to understand the different aspects of EMS in India and their connections with each other
as it will enhance the overall understanding of the functioning and governance of EMS
organizations.
REFERENCES
1. Garg, R. H. (2012). Who killed Rambhor?: The state of emergency medical services in
India. J Emerg Trauma Shock, 5(1), 49–54.
2. Gupta, R., & Basu, S. (2014). Ziqitza Healthcare Limited: Challenge of Scaling up
Emergency Medical Services (EMS) in India using Public-Private Partnership (PPP)
Mode. Asian Journal of Management Cases, 11(1), 5-21.
3. Hirshon, Risko, Calvello, Stewart, Ramirez, Narayan, . . . O'Neill. (2013). Acute Care
Research Collaborative at the University of Maryland Global Health I. Health systems
and services: the role of acute care, 91, 386–388.
4. Kironji, A. G., Anest, T., Wallis, L., Razzak, J., Jenson, A., Hansoti, B., . . . Ramirez, S.
S. (2018). Identifying barriers for out of hospital emergency care in low and low-middle
income countries: a systematic review. BMC Health Serv Res, 18.
5. Kotagal, Agarwal-Harding, Mock, Quansah, Arreola-Risa, & Meara. (2014). Health and
economic benefits of improved injury prevention and trauma care worldwide. PloS one,
9.
6. Nielsen, Mock, Joshipura, Rubiano, Zakariah, & Rivara. (2012). Assessment of the status
of prehospital care in 13 low- and middle-income countries. Prehospital emergency care :
official journal of the National Association of EMS Physicians and the National
Association of State EMS Directors, 16, 381–389.
7. Radjou, A. N., Mahajan, P., & Baliga, D. K. (2013). Where do I go? A trauma victim's
plea in an informal trauma system. J Emerg Trauma Shock, 6(3), 164-170.
primary prevention of road traffic accidents, domestic injuries, industrial trauma and civil mass
fatality has not been conducted in India to this point. Therefore, further research is needed in
future to understand the different aspects of EMS in India and their connections with each other
as it will enhance the overall understanding of the functioning and governance of EMS
organizations.
REFERENCES
1. Garg, R. H. (2012). Who killed Rambhor?: The state of emergency medical services in
India. J Emerg Trauma Shock, 5(1), 49–54.
2. Gupta, R., & Basu, S. (2014). Ziqitza Healthcare Limited: Challenge of Scaling up
Emergency Medical Services (EMS) in India using Public-Private Partnership (PPP)
Mode. Asian Journal of Management Cases, 11(1), 5-21.
3. Hirshon, Risko, Calvello, Stewart, Ramirez, Narayan, . . . O'Neill. (2013). Acute Care
Research Collaborative at the University of Maryland Global Health I. Health systems
and services: the role of acute care, 91, 386–388.
4. Kironji, A. G., Anest, T., Wallis, L., Razzak, J., Jenson, A., Hansoti, B., . . . Ramirez, S.
S. (2018). Identifying barriers for out of hospital emergency care in low and low-middle
income countries: a systematic review. BMC Health Serv Res, 18.
5. Kotagal, Agarwal-Harding, Mock, Quansah, Arreola-Risa, & Meara. (2014). Health and
economic benefits of improved injury prevention and trauma care worldwide. PloS one,
9.
6. Nielsen, Mock, Joshipura, Rubiano, Zakariah, & Rivara. (2012). Assessment of the status
of prehospital care in 13 low- and middle-income countries. Prehospital emergency care :
official journal of the National Association of EMS Physicians and the National
Association of State EMS Directors, 16, 381–389.
7. Radjou, A. N., Mahajan, P., & Baliga, D. K. (2013). Where do I go? A trauma victim's
plea in an informal trauma system. J Emerg Trauma Shock, 6(3), 164-170.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
8. Roy, Murlidhar, Chowdhury, Patil, Supe, Vaishnav, & Vatkar. (2010). Where there are
no emergency medical services-prehospital care for the injured in Mumbai, India.
Prehosp Disaster Med, 25(2), 145-51.
9. Shankar Prinja, 1. ,., Mokashi, T., Aggarwal, A. K., Kaur, M., Reddy, K. R., & Kumar,
R. (2014). Evaluation ofPublicly Financed and Privately Delivered Model of Emergency
Referral Services for Maternal and Child Health Care in India. PLoS One, 9(10).
10. Sharma, & Brandler. (2014). Emergency Medical Services in India: The Present and
Future. Prehospital and disaster medicine, 1-4.
11. Sriram, Gururaj, Razzak, Naseer, & Hyder. (2016). Comparative analysis of three pre-
hospital emergency medical services organizations in India and Pakistan. Public Health,
169–175.
12. Subhan, & Jain. (2010). Emergency care in India: The building blocks. Int J Emerg Med,
3, 2017-11.
13. Sundararaman, Chakraborty, Nair, Mokashi, & Ved. (2012). Publicly Financed
Emergency Response and Patient Transport Systems Under NRHM. New Delhi: National
Health Systems Resource Centre.
APPENDICES
PART 1-KEY WORDS AND SEARCH TERMS
1. Governance- 12396 articles were identified. 7903 met the inclusion criteria. None of
them were found relevant to the topic.
2. Governance and emergency medical services- 210 articles were identified. 152 met the
inclusion criteria. 3 were found relevant to the topic.
3. Emergency medical services- 134450 articles were identified. 53281met the inclusion
criteria. 2 of them were relevant.
4. Emergency medical services and India- 917 articles were identified. 551 met the
inclusion criteria. 4 were found relevant
8. Roy, Murlidhar, Chowdhury, Patil, Supe, Vaishnav, & Vatkar. (2010). Where there are
no emergency medical services-prehospital care for the injured in Mumbai, India.
Prehosp Disaster Med, 25(2), 145-51.
9. Shankar Prinja, 1. ,., Mokashi, T., Aggarwal, A. K., Kaur, M., Reddy, K. R., & Kumar,
R. (2014). Evaluation ofPublicly Financed and Privately Delivered Model of Emergency
Referral Services for Maternal and Child Health Care in India. PLoS One, 9(10).
10. Sharma, & Brandler. (2014). Emergency Medical Services in India: The Present and
Future. Prehospital and disaster medicine, 1-4.
11. Sriram, Gururaj, Razzak, Naseer, & Hyder. (2016). Comparative analysis of three pre-
hospital emergency medical services organizations in India and Pakistan. Public Health,
169–175.
12. Subhan, & Jain. (2010). Emergency care in India: The building blocks. Int J Emerg Med,
3, 2017-11.
13. Sundararaman, Chakraborty, Nair, Mokashi, & Ved. (2012). Publicly Financed
Emergency Response and Patient Transport Systems Under NRHM. New Delhi: National
Health Systems Resource Centre.
APPENDICES
PART 1-KEY WORDS AND SEARCH TERMS
1. Governance- 12396 articles were identified. 7903 met the inclusion criteria. None of
them were found relevant to the topic.
2. Governance and emergency medical services- 210 articles were identified. 152 met the
inclusion criteria. 3 were found relevant to the topic.
3. Emergency medical services- 134450 articles were identified. 53281met the inclusion
criteria. 2 of them were relevant.
4. Emergency medical services and India- 917 articles were identified. 551 met the
inclusion criteria. 4 were found relevant
9
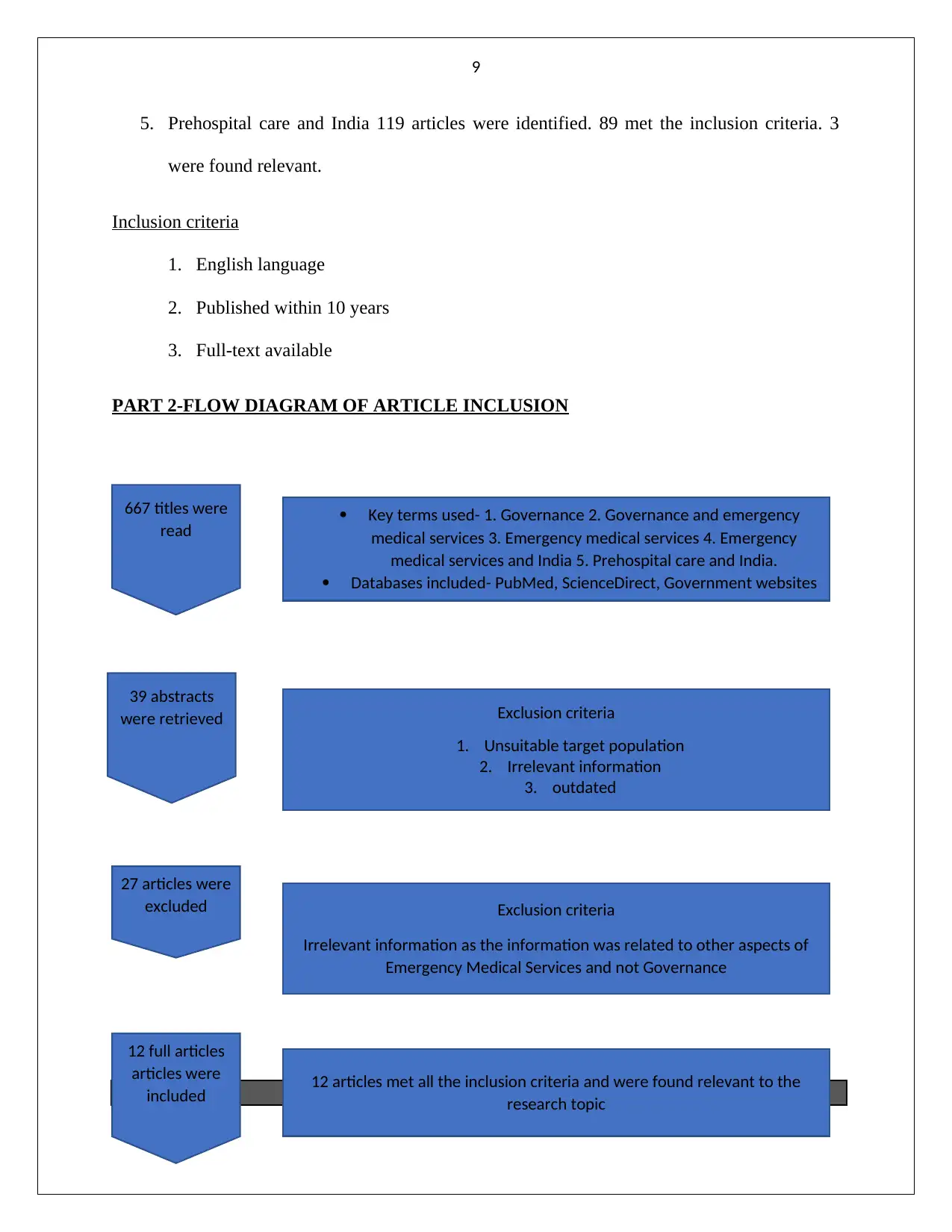
5. Prehospital care and India 119 articles were identified. 89 met the inclusion criteria. 3
were found relevant.
Inclusion criteria
1. English language
2. Published within 10 years
3. Full-text available
PART 2-FLOW DIAGRAM OF ARTICLE INCLUSION
School of Public Health and cial Work
12 full articles
articles were
included
667 titles were
read
39 abstracts
were retrieved
27 articles were
excluded
Key terms used- 1. Governance 2. Governance and emergency
medical services 3. Emergency medical services 4. Emergency
medical services and India 5. Prehospital care and India.
Databases included- PubMed, ScienceDirect, Government websites
Exclusion criteria
1. Unsuitable target population
2. Irrelevant information
3. outdated
Exclusion criteria
Irrelevant information as the information was related to other aspects of
Emergency Medical Services and not Governance
12 articles met all the inclusion criteria and were found relevant to the
research topic
5. Prehospital care and India 119 articles were identified. 89 met the inclusion criteria. 3
were found relevant.
Inclusion criteria
1. English language
2. Published within 10 years
3. Full-text available
PART 2-FLOW DIAGRAM OF ARTICLE INCLUSION
School of Public Health and cial Work
12 full articles
articles were
included
667 titles were
read
39 abstracts
were retrieved
27 articles were
excluded
Key terms used- 1. Governance 2. Governance and emergency
medical services 3. Emergency medical services 4. Emergency
medical services and India 5. Prehospital care and India.
Databases included- PubMed, ScienceDirect, Government websites
Exclusion criteria
1. Unsuitable target population
2. Irrelevant information
3. outdated
Exclusion criteria
Irrelevant information as the information was related to other aspects of
Emergency Medical Services and not Governance
12 articles met all the inclusion criteria and were found relevant to the
research topic
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
Queensland University of Technology
HLN707 Research Methods in Health
Assessment Item 1, Part A.
Expression of Intent.
Student name: SHARU JACOB
Student number: n10031561
What course (code) and major are you enrolled in? PU84(Master of health
management)
Depending on your course and major, this unit will serve different purposes. For some
students, it is an elective unit and there is no requirement to undertake the research.
Are you taking this as an elective? yes no
For other students, HLN707 will help you develop a research proposal and undertake
either a research project or research thesis.
Which one are you intending to complete?
HLN703 (24cp project) HLN700 or HLN750 (48cp thesis)
Internship (PU84 only)
If this is you, are you taking HLN707 the semester before you do your project or thesis?
yes Semester enrolled:__________ no
Queensland University of Technology
HLN707 Research Methods in Health
Assessment Item 1, Part A.
Expression of Intent.
Student name: SHARU JACOB
Student number: n10031561
What course (code) and major are you enrolled in? PU84(Master of health
management)
Depending on your course and major, this unit will serve different purposes. For some
students, it is an elective unit and there is no requirement to undertake the research.
Are you taking this as an elective? yes no
For other students, HLN707 will help you develop a research proposal and undertake
either a research project or research thesis.
Which one are you intending to complete?
HLN703 (24cp project) HLN700 or HLN750 (48cp thesis)
Internship (PU84 only)
If this is you, are you taking HLN707 the semester before you do your project or thesis?
yes Semester enrolled:__________ no
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
If No please explain why? ______________________________________
You may be able to explore an idea of your own, or there are a number of
potential research projects available on Blackboard.
If you are interested in one of these projects, in the first instance, you must discuss this
with Kaeleen or Erika.
Which type of research are you considering at this stage? Please circle or highlight
Literature review: scoping review systematic (narrative) review
systematic review (meta-ethnography)
Methodology: qualitative mixed methods quantitative
Secondary data analysis using: qualitative or quantitative data
Tentative research question:
GOVERNANCE OF EMERGENCY MEDICAL SERVICES IN INDIA, A SCOPING
REVIEW
Background: (What is the context to your research proposal?).
The mortality rate in emergency medical services and prehospital care is high in spite of
several initiatives taken by the Government. Due to the poor condition of the emergency
services, the health outcome for the patient drops down. Medical Emergency has not been
defined by the Indian Judicial system and it is still largely left to the discretion of medical
professionals to define it. At present, the peripheral level health centers, i.e., S/C, PHC, and
CHC, are nothing more than the referring centers. Doctors also show unwillingness to
attend to emergency cases as they deem it medico legal cases. EMS in India has been
identified as unfragmented and coordinated therefore, it is essential to understand the
If No please explain why? ______________________________________
You may be able to explore an idea of your own, or there are a number of
potential research projects available on Blackboard.
If you are interested in one of these projects, in the first instance, you must discuss this
with Kaeleen or Erika.
Which type of research are you considering at this stage? Please circle or highlight
Literature review: scoping review systematic (narrative) review
systematic review (meta-ethnography)
Methodology: qualitative mixed methods quantitative
Secondary data analysis using: qualitative or quantitative data
Tentative research question:
GOVERNANCE OF EMERGENCY MEDICAL SERVICES IN INDIA, A SCOPING
REVIEW
Background: (What is the context to your research proposal?).
The mortality rate in emergency medical services and prehospital care is high in spite of
several initiatives taken by the Government. Due to the poor condition of the emergency
services, the health outcome for the patient drops down. Medical Emergency has not been
defined by the Indian Judicial system and it is still largely left to the discretion of medical
professionals to define it. At present, the peripheral level health centers, i.e., S/C, PHC, and
CHC, are nothing more than the referring centers. Doctors also show unwillingness to
attend to emergency cases as they deem it medico legal cases. EMS in India has been
identified as unfragmented and coordinated therefore, it is essential to understand the
12
governance of these services in order to hold the system accountable and look for
improvement.
Broadly, what is research topic or area? (up to 5 keywords)
1. Governance
2. Governance and emergency medical services
3. Emergency medical services
4. Emergency medical services and India
5. Prehospital care and India.
Now, describe your research topic in a little more detail.
The research topic will identify the challenges faced in the emergency medical services in
India. It will also identify the reasons for these challenges especially in terms of structures,
processes and systems involved in EMS. Further, the research will provide the
recommendations to improve the governance of EMS in India so that mortality rate can be
lowered and health outcomes for patient can be improved.
What is the aim (1) of your proposal?
To understand the structures and processes involved in Emergency medical services in
India and look for scope in improvement of EMS in India
What are objectives (3) of your proposal?
1. To identify the current status of emergency medical services in India
2. To understand the structures and processes involved in Emergency medical services
in India
governance of these services in order to hold the system accountable and look for
improvement.
Broadly, what is research topic or area? (up to 5 keywords)
1. Governance
2. Governance and emergency medical services
3. Emergency medical services
4. Emergency medical services and India
5. Prehospital care and India.
Now, describe your research topic in a little more detail.
The research topic will identify the challenges faced in the emergency medical services in
India. It will also identify the reasons for these challenges especially in terms of structures,
processes and systems involved in EMS. Further, the research will provide the
recommendations to improve the governance of EMS in India so that mortality rate can be
lowered and health outcomes for patient can be improved.
What is the aim (1) of your proposal?
To understand the structures and processes involved in Emergency medical services in
India and look for scope in improvement of EMS in India
What are objectives (3) of your proposal?
1. To identify the current status of emergency medical services in India
2. To understand the structures and processes involved in Emergency medical services
in India
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 31
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.