UWS Epidemiology (401076) Assignment 2: CHD Study Analysis, 2018
VerifiedAdded on 2023/06/04
|7
|2224
|135
Homework Assignment
AI Summary
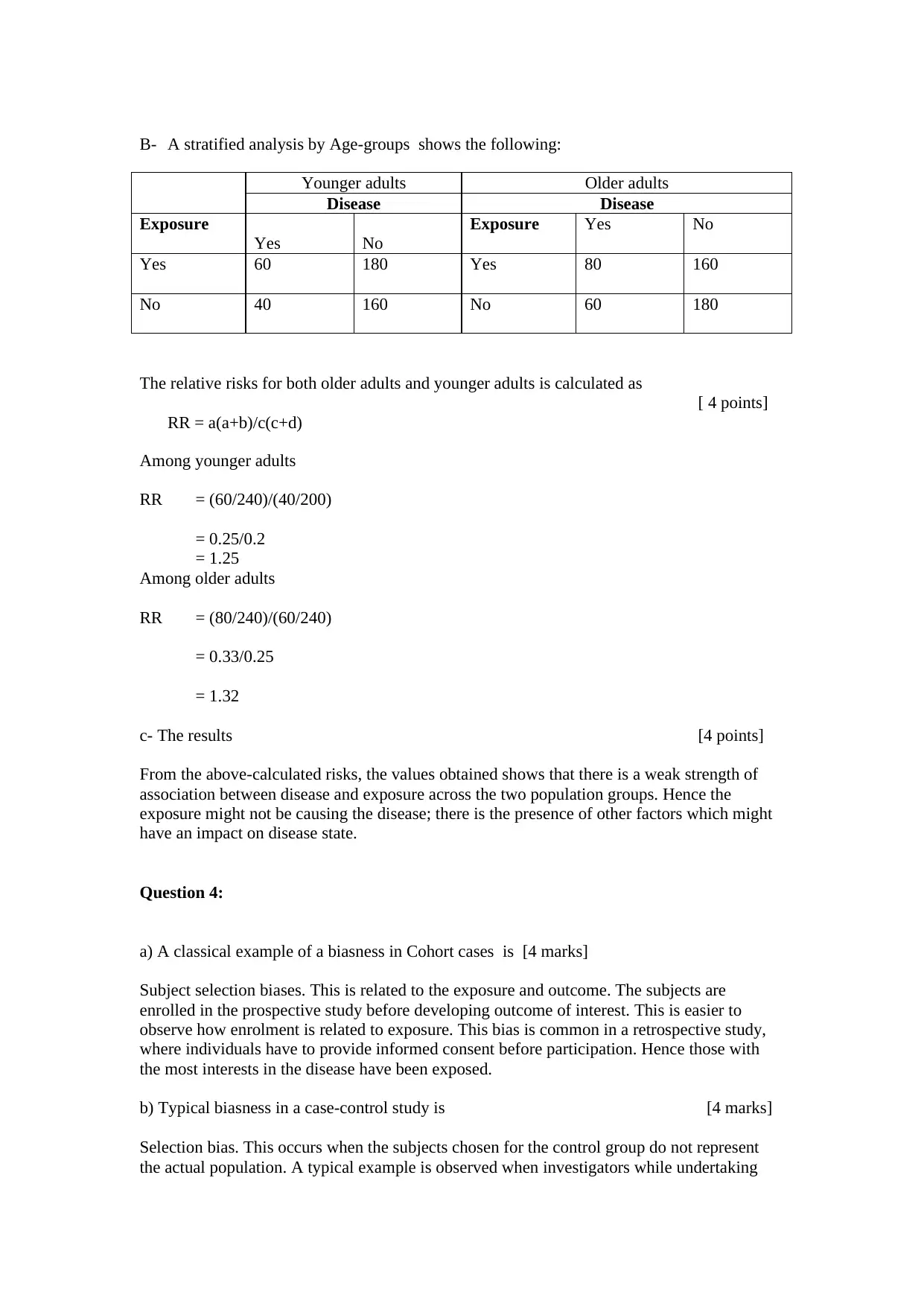
This assignment provides a comprehensive analysis of epidemiological studies related to coronary heart disease (CHD). It begins by examining a cohort study on the long-term effects of physical activity on CHD incidence, addressing aspects such as study design, data sources, and the impact of confounders like hyperlipidemia, hypertension, and diabetes. The assignment further delves into a case-control study investigating the effect of dietary fat intake on melanoma, calculating relative risks and attributable risks to assess the association between low-fat diets and skin cancer. Additionally, it explores the concept of bias in cohort and case-control studies and discusses methods for addressing confounding factors. The analysis covers key epidemiological concepts such as risk ratios, rate ratios, and the interpretation of statistical results, providing a detailed understanding of the factors influencing CHD and melanoma risks. Desklib offers a wealth of similar solved assignments and past papers to aid students in their studies.

1 out of 7
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.