Epidemiology Assignment: Comparing Death Rates, Risk Factors, and HPV
VerifiedAdded on 2021/05/31
|10
|2001
|67
Homework Assignment
AI Summary
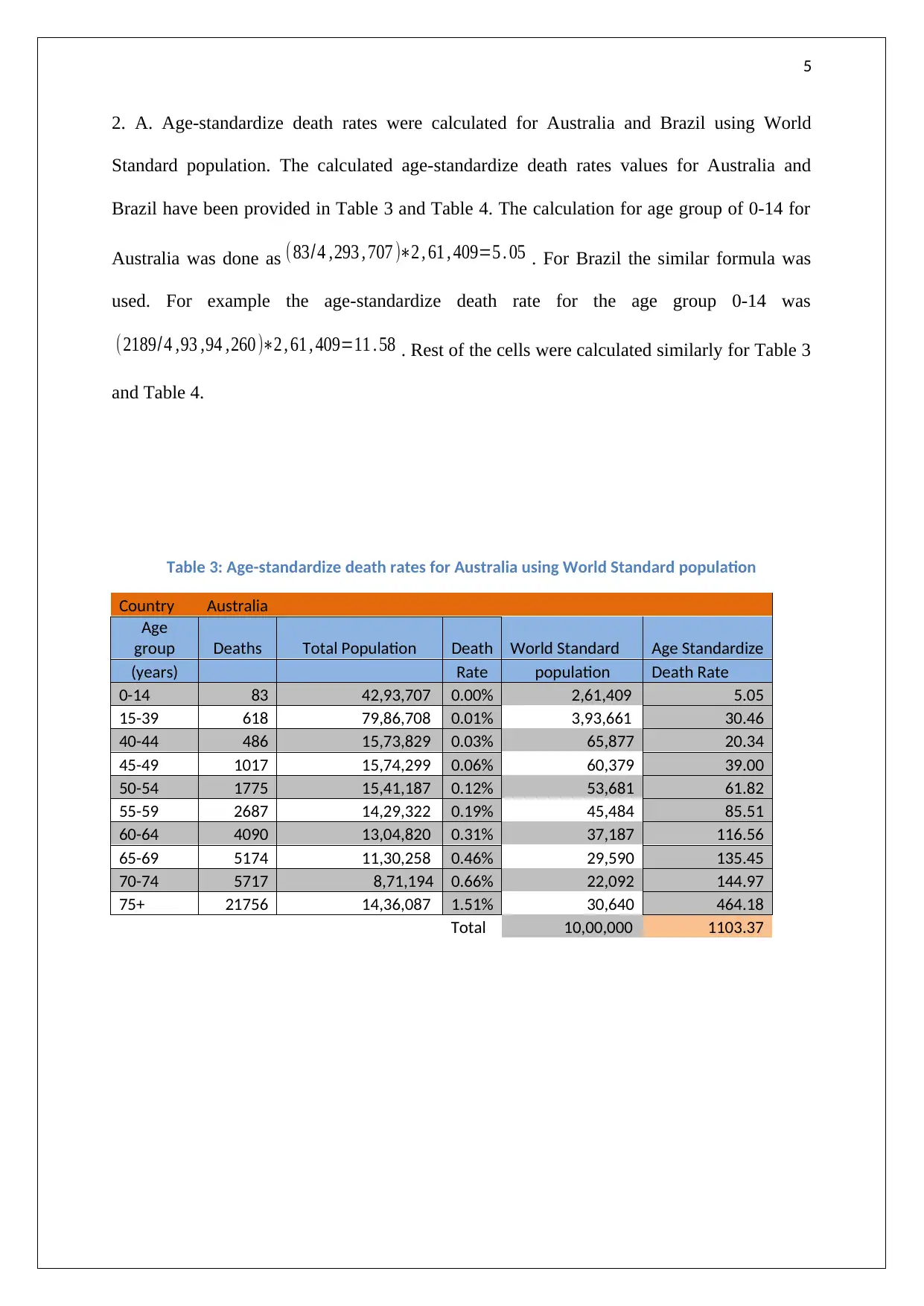
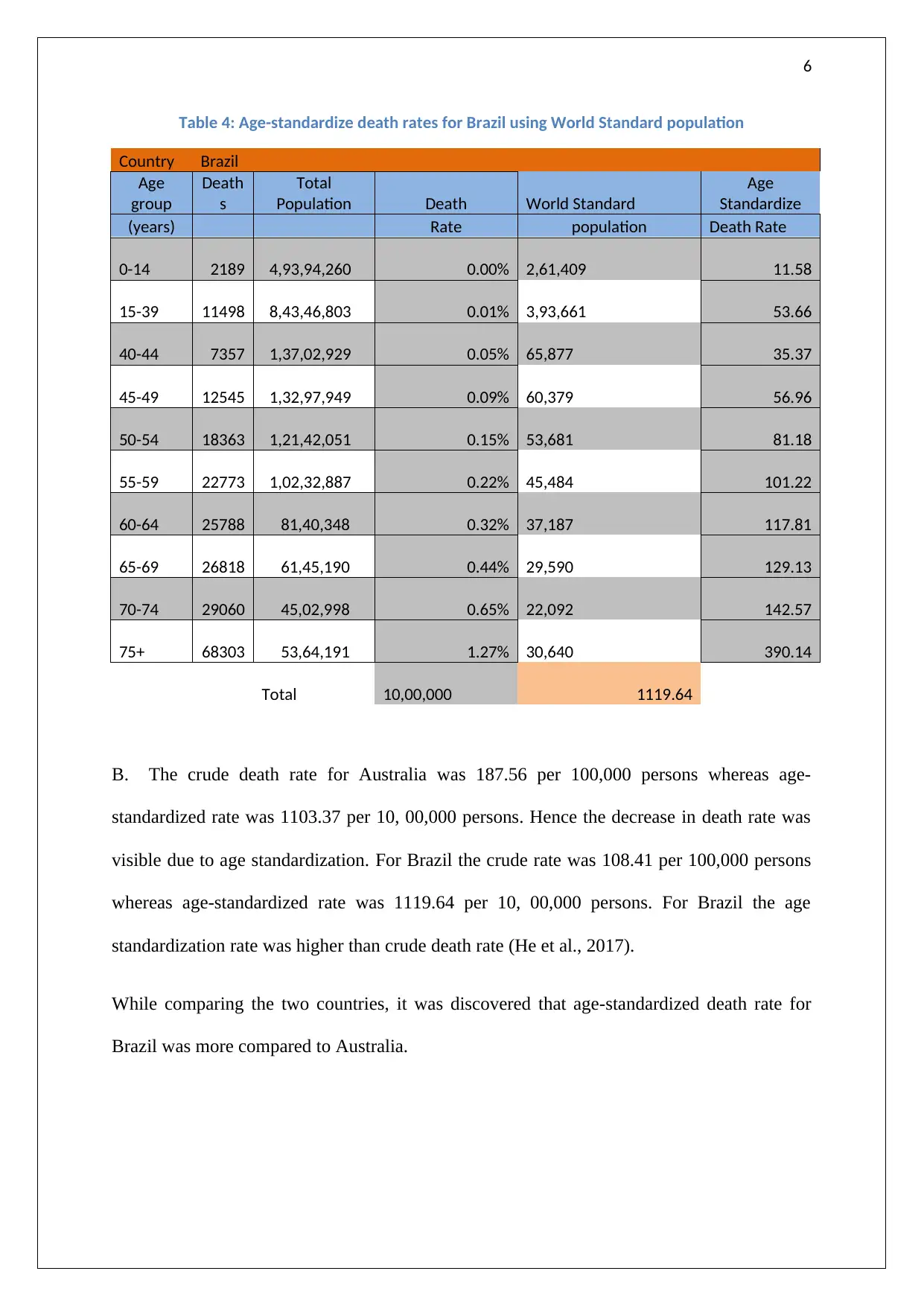
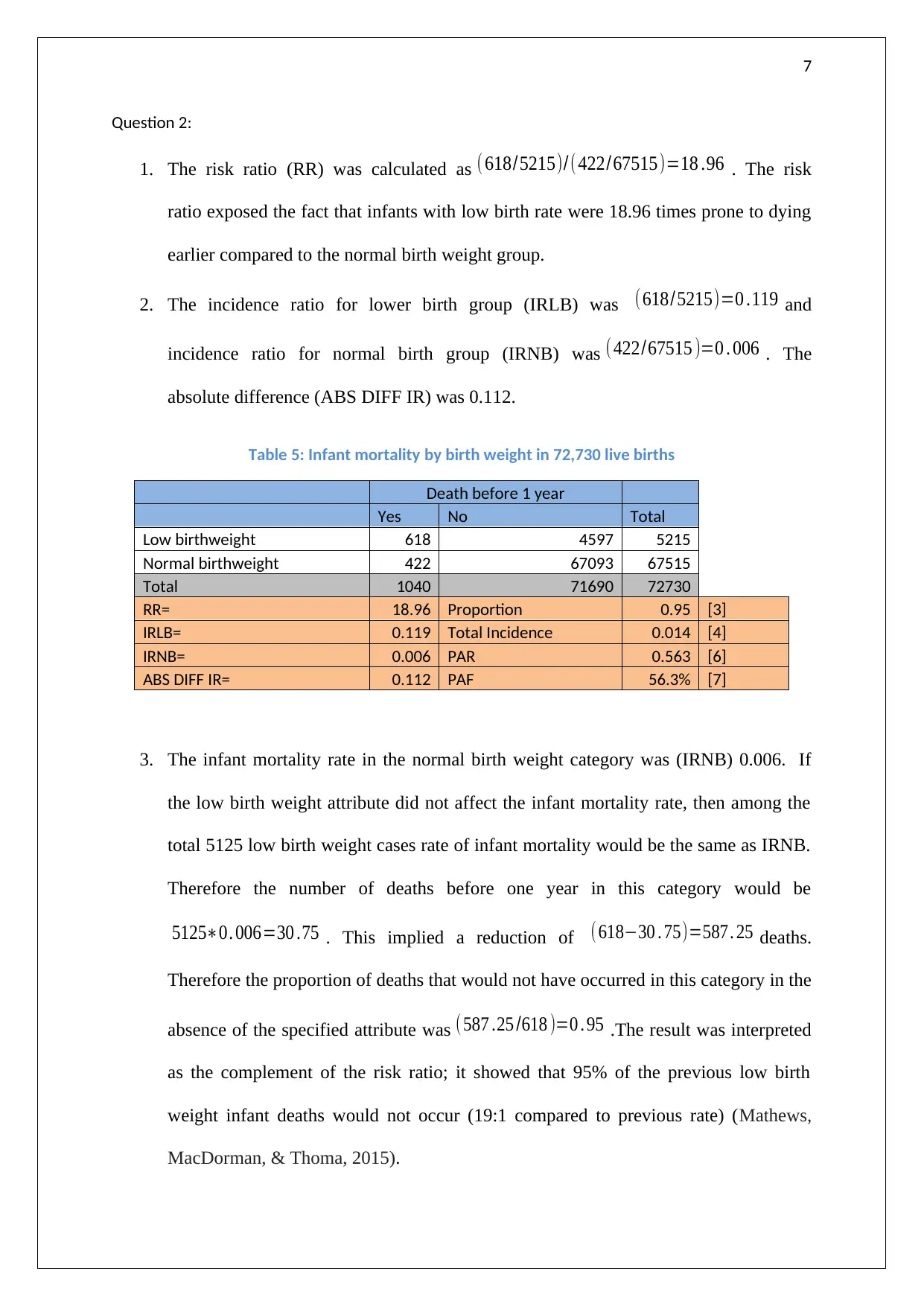
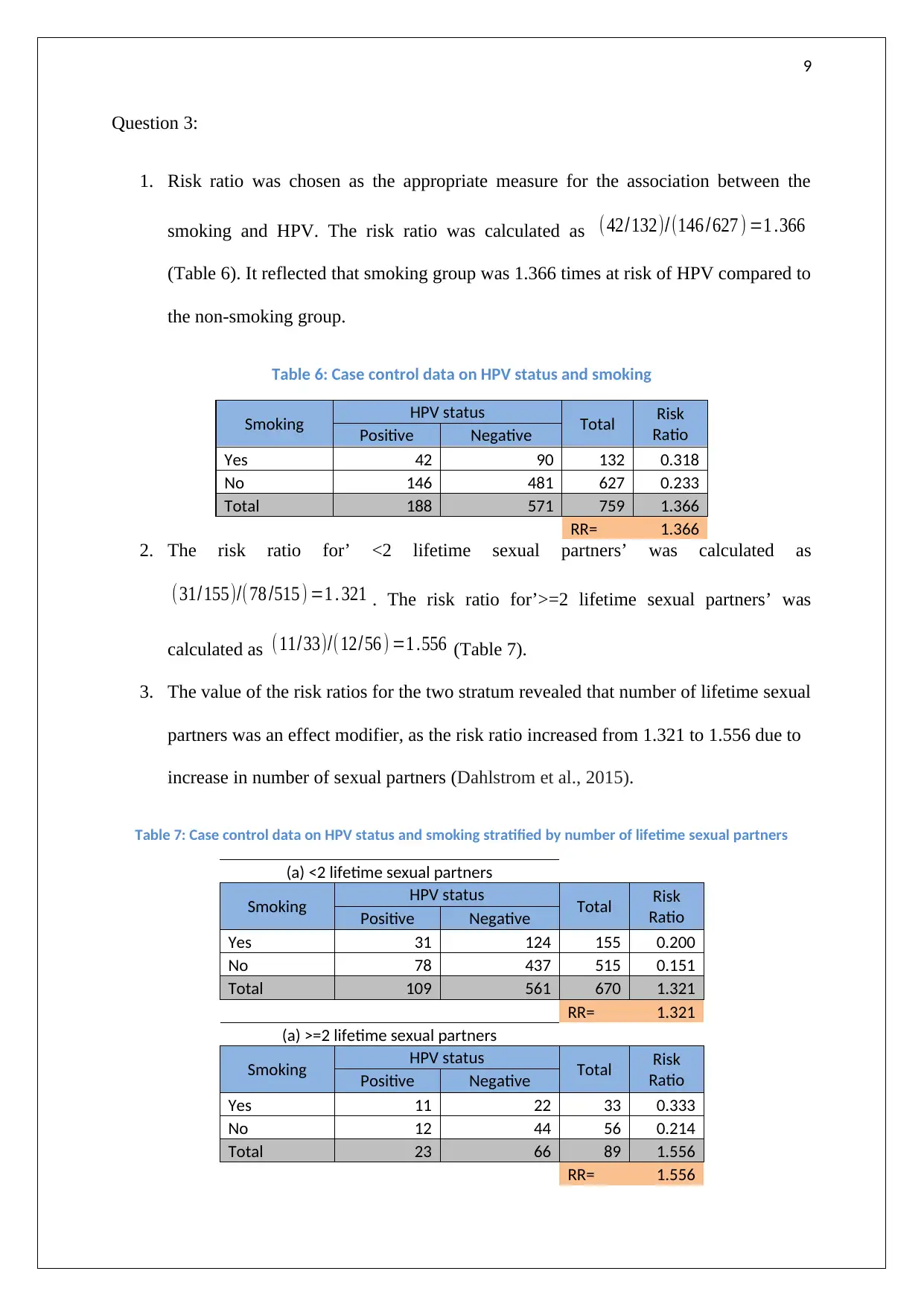
This epidemiology assignment analyzes cancer and infant mortality data, exploring various statistical measures and risk factors. The assignment begins by comparing crude and age-specific cancer death rates between Australia and Brazil, highlighting the exponential increase in death rates with age and the differences observed in specific age groups. It then delves into age-standardized death rates, demonstrating how this method adjusts for population age differences. The assignment also examines infant mortality, calculating risk ratios related to low birth weight and assessing the impact of this factor on infant mortality rates. Finally, it investigates the association between smoking and HPV, calculating risk ratios and exploring the effect of lifetime sexual partners as a potential modifier. The analysis includes the use of tables, graphs, and statistical calculations to support the findings.
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.