Comprehensive Analysis of Stroke Epidemiology and Research Principles
VerifiedAdded on 2021/04/17
|13
|3227
|26
Report
AI Summary
This report provides a comprehensive overview of stroke epidemiology in Australia. It begins with an abstract highlighting stroke as a major health concern, particularly among indigenous populations. The report defines stroke, differentiates between ischemic and hemorrhagic types, and presents prevalence data based on ABS surveys. It explores the disproportionate burden of stroke on disadvantaged communities and the associated mortality and healthcare costs. The report delves into the multifactorial nature of stroke causation, identifying both modifiable and non-modifiable risk factors such as hypertension, smoking, and genetic predisposition. It discusses the impact of socioeconomic factors and the need for evidence-based prevention strategies, including national action priorities and population-based health education. The report concludes with a call for improved stroke management and prevention guidelines, highlighting the importance of primary, secondary, and tertiary care interventions. The report also includes a multifactorial model for causation of stroke.

Running head:EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
Epidemiology and Principles of Research
Name of student:
Name of university:
Author note:
Epidemiology and Principles of Research
Name of student:
Name of university:
Author note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
Abstract
Stroke is known to be a major factor for patient mortality and morbidity when speaking on the
global basis. In Australia, the condition has been projected to be a leading contributor to poor
health outcomes of the nation’s population. There exist incontestable inconsistencies in the
distribution of the burden of the disease. The indigenous population has been indicated to suffer
stroke at a much higher rate as compared to their counterpart. Stroke causation is chiefly
multifactorial and different risk factors interact in a complex manner. There is a need of
implementing evidence based strategies for addressing the confounding issues in the near future.
Abstract
Stroke is known to be a major factor for patient mortality and morbidity when speaking on the
global basis. In Australia, the condition has been projected to be a leading contributor to poor
health outcomes of the nation’s population. There exist incontestable inconsistencies in the
distribution of the burden of the disease. The indigenous population has been indicated to suffer
stroke at a much higher rate as compared to their counterpart. Stroke causation is chiefly
multifactorial and different risk factors interact in a complex manner. There is a need of
implementing evidence based strategies for addressing the confounding issues in the near future.
2EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
Stroke acts as a significant contributing factor for the total disease burden on a global
scale and research indicates it to be preceding coronary heart disease as the cause of death.
Further, stroke is a notable reason for disability among individuals. Stroke is defined as the
condition in which cell death in brain is due to poor supply of blood. It is the acute loss of brain
function due to impairment of blood supply. As per the World Health Organization definition for
stroke, it is the "neurological deficit of cerebrovascular cause that persists beyond 24 hours or is
interrupted by death within 24 hours" (1). Medical science classifies stroke into two categories;
hemorrhagic, as a result of bleeding, and ischemic, as a result of the absence of blood flow. Signs
of such a condition include the restriction to feel or move a side of the body, loss of vision to one
side, and difficulties in speaking or understanding. Research indicates that ischemic stroke
constitutes almost 80% of the total stroke cases (2).
In Australia, the prevalence of stroke can be estimated on the basis of self-reported data
collected from the 1998, 2003 and 2009 Surveys of Disability, Ageing and Carers (SDACs)
conducted by the ABS (Australian Bureau of statistics). In the year 2009, approximately 375,759
Australians have had suffered a stroke in their lifetime. Overall, the incidence of stroke was
much higher in males as compared to female (1.9% as compared to 1.3%). 70% of people who
had suffered a stroke had the age and above (3). In Australia, the burden of stroke mostly affects
the disadvantaged populations within the different communities in a disproportionate manner.
Those living in the low socioeconomic group have more chances of suffering from a stroke. The
trend is further magnified in indigenous population (4). As per the reports of AIHW, the overall
stroke incidence is found to be twice among the indigenouspopulation. Disparities in risk factor
prevalence among the two groups contribute to this discreet burden of stroke between the
country’s populations.
Stroke acts as a significant contributing factor for the total disease burden on a global
scale and research indicates it to be preceding coronary heart disease as the cause of death.
Further, stroke is a notable reason for disability among individuals. Stroke is defined as the
condition in which cell death in brain is due to poor supply of blood. It is the acute loss of brain
function due to impairment of blood supply. As per the World Health Organization definition for
stroke, it is the "neurological deficit of cerebrovascular cause that persists beyond 24 hours or is
interrupted by death within 24 hours" (1). Medical science classifies stroke into two categories;
hemorrhagic, as a result of bleeding, and ischemic, as a result of the absence of blood flow. Signs
of such a condition include the restriction to feel or move a side of the body, loss of vision to one
side, and difficulties in speaking or understanding. Research indicates that ischemic stroke
constitutes almost 80% of the total stroke cases (2).
In Australia, the prevalence of stroke can be estimated on the basis of self-reported data
collected from the 1998, 2003 and 2009 Surveys of Disability, Ageing and Carers (SDACs)
conducted by the ABS (Australian Bureau of statistics). In the year 2009, approximately 375,759
Australians have had suffered a stroke in their lifetime. Overall, the incidence of stroke was
much higher in males as compared to female (1.9% as compared to 1.3%). 70% of people who
had suffered a stroke had the age and above (3). In Australia, the burden of stroke mostly affects
the disadvantaged populations within the different communities in a disproportionate manner.
Those living in the low socioeconomic group have more chances of suffering from a stroke. The
trend is further magnified in indigenous population (4). As per the reports of AIHW, the overall
stroke incidence is found to be twice among the indigenouspopulation. Disparities in risk factor
prevalence among the two groups contribute to this discreet burden of stroke between the
country’s populations.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
The burden of stroke mortality is compounding, and the direct impact of stroke on the
central nervous system is the cause of a wide array of disability. Survival from stroke and the
comprehensive rehabilitation process is a major cause off increased cost to the healthcare system.
Stroke was the cause of death for 8300 individuals in Australia in the year 2010 and accounted
for 6% of all deaths in the country (5). Research indicates that death rates due to stroke increase
considerably with age. More females died due to stroke as compared with males. However, age-
specific rates were found to be higher in males than females between the ages of 55 and 84.
Expanded research on this arena indicates that hemorrhagic stroke is more associated with loss of
good health when a comparison is done to ischemic stroke. This can be attributed to the higher
case fatality rate among those with younger age. Raw mortality rate defining stroke burden
emphasizes that the issue can only be controlled with better management strategies addressing
the distinct risk factors.
The healthcare expenditure for strokes in the country is in millions and accounts for
almost 7% of total healthcare expenditure for all cardiovascular diseases. It is to be highlighted
in here that healthcare expenditure is not only a result of expenditure incurred due to a residential
care facility. The cost of healthcare is also related to admission of hospital-admitted patients, out-
of-hospital medical services and pharmaceuticals. Reports of the year 2008–09, the total
estimated expenditure on stroke as indicated by research was found to be more for males as
compared to females (6).
Research highlights that the complications of suffering stroke are multivariate. The
common complications include brain edema, pneumonia, urinary tract infection, seizures,
clinical depression, and deep venous thrombosis. The main aim of management guidelines for
stroke focuses on improvement in quality of life of patients, through primary, secondary and
The burden of stroke mortality is compounding, and the direct impact of stroke on the
central nervous system is the cause of a wide array of disability. Survival from stroke and the
comprehensive rehabilitation process is a major cause off increased cost to the healthcare system.
Stroke was the cause of death for 8300 individuals in Australia in the year 2010 and accounted
for 6% of all deaths in the country (5). Research indicates that death rates due to stroke increase
considerably with age. More females died due to stroke as compared with males. However, age-
specific rates were found to be higher in males than females between the ages of 55 and 84.
Expanded research on this arena indicates that hemorrhagic stroke is more associated with loss of
good health when a comparison is done to ischemic stroke. This can be attributed to the higher
case fatality rate among those with younger age. Raw mortality rate defining stroke burden
emphasizes that the issue can only be controlled with better management strategies addressing
the distinct risk factors.
The healthcare expenditure for strokes in the country is in millions and accounts for
almost 7% of total healthcare expenditure for all cardiovascular diseases. It is to be highlighted
in here that healthcare expenditure is not only a result of expenditure incurred due to a residential
care facility. The cost of healthcare is also related to admission of hospital-admitted patients, out-
of-hospital medical services and pharmaceuticals. Reports of the year 2008–09, the total
estimated expenditure on stroke as indicated by research was found to be more for males as
compared to females (6).
Research highlights that the complications of suffering stroke are multivariate. The
common complications include brain edema, pneumonia, urinary tract infection, seizures,
clinical depression, and deep venous thrombosis. The main aim of management guidelines for
stroke focuses on improvement in quality of life of patients, through primary, secondary and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
tertiary care. Management of stroke patients is complex and needs interventions encompassing
drug therapies, medical supervision and monitoring (7).
The causal factors and the risk factors for stroke are widely noted across the literature.
Causation of stoke has been indicated to be complex, caused due to an imperative association
between risk factors. These factors are both modifiable and non-modifiable across a wide range
of biomedical and behavioural factors. One must note that broader community-based
socioeconomic factors are also involved in this process. The traditionally considered risk factors
include tobacco smoking and hypertension which have been noted as synonymous with
cardiovascular diseases (8). The non-modifiable risk factors include ethnicity, gender age,
inherited disease and weight at birth, while the modifiable risk factors include diabetes mellitus,
hypertension, heart diseases, alcohol abuse, dyslipidemia, obesity, metabolic syndrome,
peripheral artery disease and drug abuse.
A rich pool of studies highlights hypertension to be the most significant contributor to
risk of stroke. The other top risk factors include smoking, obesity, physical activity and diet
which make up near about 80% of the total risk for stroke etiologies across the globe. A small
pool of evidence indicates that hypertension acts as a more prominent risk factor in individuals
for hemorrhagic stroke as compared to ischemic stroke. High blood pressure has been proved to
increase the risk for stroke by four times. Alcohol intake has also been indicated to be more
related to hemorrhagic stroke. There exists strong evidence that genetic basis of certain
individuals acts as a risk factor for stroke. The chances of an individual to suffer a stroke are 2.79
times higher if the person has a parental history of stroke prior to the age of 65 years (9).
tertiary care. Management of stroke patients is complex and needs interventions encompassing
drug therapies, medical supervision and monitoring (7).
The causal factors and the risk factors for stroke are widely noted across the literature.
Causation of stoke has been indicated to be complex, caused due to an imperative association
between risk factors. These factors are both modifiable and non-modifiable across a wide range
of biomedical and behavioural factors. One must note that broader community-based
socioeconomic factors are also involved in this process. The traditionally considered risk factors
include tobacco smoking and hypertension which have been noted as synonymous with
cardiovascular diseases (8). The non-modifiable risk factors include ethnicity, gender age,
inherited disease and weight at birth, while the modifiable risk factors include diabetes mellitus,
hypertension, heart diseases, alcohol abuse, dyslipidemia, obesity, metabolic syndrome,
peripheral artery disease and drug abuse.
A rich pool of studies highlights hypertension to be the most significant contributor to
risk of stroke. The other top risk factors include smoking, obesity, physical activity and diet
which make up near about 80% of the total risk for stroke etiologies across the globe. A small
pool of evidence indicates that hypertension acts as a more prominent risk factor in individuals
for hemorrhagic stroke as compared to ischemic stroke. High blood pressure has been proved to
increase the risk for stroke by four times. Alcohol intake has also been indicated to be more
related to hemorrhagic stroke. There exists strong evidence that genetic basis of certain
individuals acts as a risk factor for stroke. The chances of an individual to suffer a stroke are 2.79
times higher if the person has a parental history of stroke prior to the age of 65 years (9).
5EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
The causal role of certain less well-documented risk factors is also to be discussed in
here. Though further studies are needed to address the fact that role is inconclusive, the factors
are noteworthy. These factors include an increase of the apoB/apoA1 ratio, psychological stress,
sleep-related disorders, poor diet and frequent infection (10). Future characterization of these risk
factors through well-designed clinical research studies would certainly add valuable knowledge.
This would form the base for well-tailored preventive strategies addressing the high prevalence
of stroke.
Model development for stroke causation is to consider the different behavioral risk
factors along with the distinct biomedical risk factors in the context of social and environmental
influences. It is noteworthy that such overarching influences are applicable to diverse
populations of the community (11). Though there are no direct implications in stroke causation,
the distal factors have a notable impact on the prevalence of almost all proximal risk factors. The
findings of research a relevant study indicate deaths due to stroke is more common among those
coming from the lower socioeconomic group. High prevalence of risk factors such as smoking
and hypertension among these individuals are noteworthy. Individuals from this socioeconomic
class are also associated with lower level of education and unemployment. The researchers
contend that the rate of stroke might be underestimated in some epidemiological studies since
distance is a crucial factor for poor hospital attendance in areas that are remote (12).
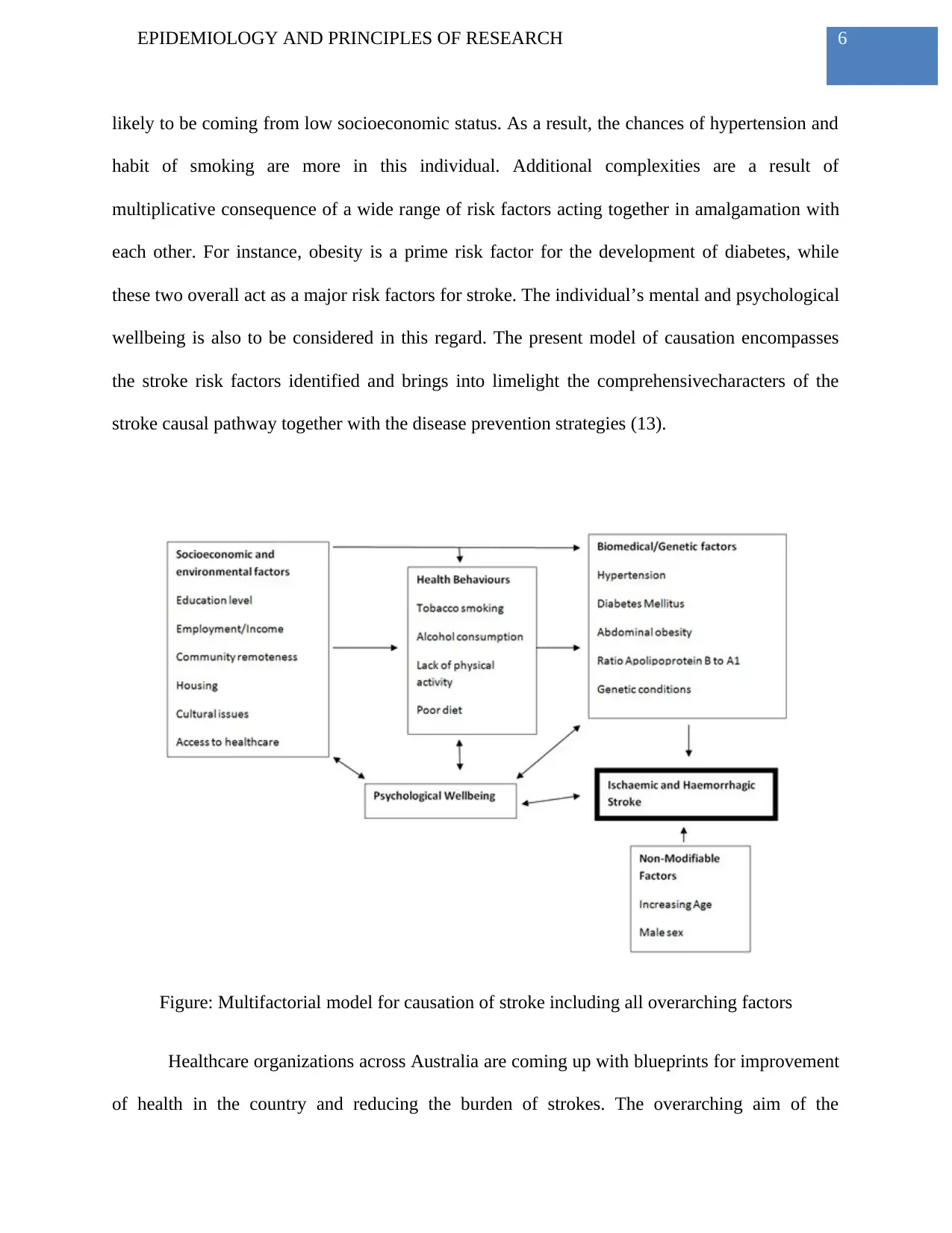
The multifactorial model provided below is a clear representation of a proximal to a
distal causal pathway that highlights schematic associations existing between the diverse factors.
It is found that proximal factors like hypertension and smoking are inextricably associated with
the pathology of stroke. When the perspective is holistic, one can note that the path between
proximal and distal factors is distinct. For instance, an individual having low literacy rate is
The causal role of certain less well-documented risk factors is also to be discussed in
here. Though further studies are needed to address the fact that role is inconclusive, the factors
are noteworthy. These factors include an increase of the apoB/apoA1 ratio, psychological stress,
sleep-related disorders, poor diet and frequent infection (10). Future characterization of these risk
factors through well-designed clinical research studies would certainly add valuable knowledge.
This would form the base for well-tailored preventive strategies addressing the high prevalence
of stroke.
Model development for stroke causation is to consider the different behavioral risk
factors along with the distinct biomedical risk factors in the context of social and environmental
influences. It is noteworthy that such overarching influences are applicable to diverse
populations of the community (11). Though there are no direct implications in stroke causation,
the distal factors have a notable impact on the prevalence of almost all proximal risk factors. The
findings of research a relevant study indicate deaths due to stroke is more common among those
coming from the lower socioeconomic group. High prevalence of risk factors such as smoking
and hypertension among these individuals are noteworthy. Individuals from this socioeconomic
class are also associated with lower level of education and unemployment. The researchers
contend that the rate of stroke might be underestimated in some epidemiological studies since
distance is a crucial factor for poor hospital attendance in areas that are remote (12).
The multifactorial model provided below is a clear representation of a proximal to a
distal causal pathway that highlights schematic associations existing between the diverse factors.
It is found that proximal factors like hypertension and smoking are inextricably associated with
the pathology of stroke. When the perspective is holistic, one can note that the path between
proximal and distal factors is distinct. For instance, an individual having low literacy rate is
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
likely to be coming from low socioeconomic status. As a result, the chances of hypertension and
habit of smoking are more in this individual. Additional complexities are a result of
multiplicative consequence of a wide range of risk factors acting together in amalgamation with
each other. For instance, obesity is a prime risk factor for the development of diabetes, while
these two overall act as a major risk factors for stroke. The individual’s mental and psychological
wellbeing is also to be considered in this regard. The present model of causation encompasses
the stroke risk factors identified and brings into limelight the comprehensivecharacters of the
stroke causal pathway together with the disease prevention strategies (13).
Figure: Multifactorial model for causation of stroke including all overarching factors
Healthcare organizations across Australia are coming up with blueprints for improvement
of health in the country and reducing the burden of strokes. The overarching aim of the
likely to be coming from low socioeconomic status. As a result, the chances of hypertension and
habit of smoking are more in this individual. Additional complexities are a result of
multiplicative consequence of a wide range of risk factors acting together in amalgamation with
each other. For instance, obesity is a prime risk factor for the development of diabetes, while
these two overall act as a major risk factors for stroke. The individual’s mental and psychological
wellbeing is also to be considered in this regard. The present model of causation encompasses
the stroke risk factors identified and brings into limelight the comprehensivecharacters of the
stroke causal pathway together with the disease prevention strategies (13).
Figure: Multifactorial model for causation of stroke including all overarching factors
Healthcare organizations across Australia are coming up with blueprints for improvement
of health in the country and reducing the burden of strokes. The overarching aim of the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
department of health is to bring improvement in the health status of the population and bring it to
the best level. Progressively reducing the inequalities in health outcomes related to stroke would
be the key objective. Improvement in care, primary and secondary, for stroke, across the
continuum of services is to be achieved in the near future by giving equal opportunities to
indigenous population (14).
Preventive strategies for curbing the prevalence of stroke would be effective when
implemented if they target the population who are at higher risk of suffering the condition- the
indigenous population. Approaches to the population, in general, are complementary. The
importance of prevention of hypertension through risk factor prevention strategies would be
amplified due to the concurrent impact on other health conditions. These include the widely
noted influence of tobacco smoking on lung diseases and lack of physical activities on diabetes.
Secondary prevention is required in individuals who suffer from the peripheral arterial disease.
Reduction in smoking habits among the population would also serve as an important preventive
strategy. It is to be mentioned in here that preventive strategies are to be implemented across the
life span of an individual. Evidence from other countries indicates that benefits can be achieved
in the long term when nutritional interventions are implemented (15).
The priorities for national action are to be highlighted at this juncture. The government
is to come forward to support coordinated approaches to tobacco control, physical activity and
nutrition by acting upon present work. The at-risk populations are indigenous Australians,
socioeconomically challenged individuals, older Australians, people with mental health disease,
people living in rural isolation (16). Tools and information are to be developed and disseminated
for supporting general practitioners and consumers to consider the accurate treatment as per the
level of risk of suffering stroke. Population-based strategies would include health education
department of health is to bring improvement in the health status of the population and bring it to
the best level. Progressively reducing the inequalities in health outcomes related to stroke would
be the key objective. Improvement in care, primary and secondary, for stroke, across the
continuum of services is to be achieved in the near future by giving equal opportunities to
indigenous population (14).
Preventive strategies for curbing the prevalence of stroke would be effective when
implemented if they target the population who are at higher risk of suffering the condition- the
indigenous population. Approaches to the population, in general, are complementary. The
importance of prevention of hypertension through risk factor prevention strategies would be
amplified due to the concurrent impact on other health conditions. These include the widely
noted influence of tobacco smoking on lung diseases and lack of physical activities on diabetes.
Secondary prevention is required in individuals who suffer from the peripheral arterial disease.
Reduction in smoking habits among the population would also serve as an important preventive
strategy. It is to be mentioned in here that preventive strategies are to be implemented across the
life span of an individual. Evidence from other countries indicates that benefits can be achieved
in the long term when nutritional interventions are implemented (15).
The priorities for national action are to be highlighted at this juncture. The government
is to come forward to support coordinated approaches to tobacco control, physical activity and
nutrition by acting upon present work. The at-risk populations are indigenous Australians,
socioeconomically challenged individuals, older Australians, people with mental health disease,
people living in rural isolation (16). Tools and information are to be developed and disseminated
for supporting general practitioners and consumers to consider the accurate treatment as per the
level of risk of suffering stroke. Population-based strategies would include health education
8EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
imparted to the population across communities on the risk factors for stroke. Primary care units
have a key role in this regard. Healthcare professionals are to work in collaboration with each
other in the domain of chronic disease management, such as diabetes and mental health
conditions. Further, awareness is to be raised among the healthcare providers and consumers
regarding the necessity of seeking urgent medical treatment when the early signs and symptoms
of stroke are evident. Health workers in remote and rural workers are to be provided with
training and education so that they can handle emergency cases efficiently. On the national level,
there is also a need of revising the guidelines for stroke management and prevention for
incorporating updated developments in the care system for stroke. Increasing the availability of
stoke care unit would also be beneficial (17).
In conclusion, stoke suffered by adults in Australia has become an important health
concern in the country in the recent past. Though research indicates that the risk factors are
almost similar in the country’s indigenous and non-indigenous population, the burden of the
disease is not distributed equally. The issue is more prominent in a community where majority of
the indigenous populations are experiencing worse health, economic and social outcomes as
compared to the non-indigenous counterparts. In addressing the high prevalence rate of stroke
among the population and reducing the burden of the disease, there is a vital need of recognizing
the multifactorial nature of the health condition. Considering the conventional proximal risk
factors would act as a suitable approach for health professionals who are responsible for
delivering primary care across communities. Nevertheless, there exists a large scope for
addressing the distal community-based factors. Socioeconomic, environmental and psychological
factors hold prime importance in this regard. A holistic approach might be beneficial for
addressing the morbidity and mortality related to stroke among adults in Australia. Appropriate
imparted to the population across communities on the risk factors for stroke. Primary care units
have a key role in this regard. Healthcare professionals are to work in collaboration with each
other in the domain of chronic disease management, such as diabetes and mental health
conditions. Further, awareness is to be raised among the healthcare providers and consumers
regarding the necessity of seeking urgent medical treatment when the early signs and symptoms
of stroke are evident. Health workers in remote and rural workers are to be provided with
training and education so that they can handle emergency cases efficiently. On the national level,
there is also a need of revising the guidelines for stroke management and prevention for
incorporating updated developments in the care system for stroke. Increasing the availability of
stoke care unit would also be beneficial (17).
In conclusion, stoke suffered by adults in Australia has become an important health
concern in the country in the recent past. Though research indicates that the risk factors are
almost similar in the country’s indigenous and non-indigenous population, the burden of the
disease is not distributed equally. The issue is more prominent in a community where majority of
the indigenous populations are experiencing worse health, economic and social outcomes as
compared to the non-indigenous counterparts. In addressing the high prevalence rate of stroke
among the population and reducing the burden of the disease, there is a vital need of recognizing
the multifactorial nature of the health condition. Considering the conventional proximal risk
factors would act as a suitable approach for health professionals who are responsible for
delivering primary care across communities. Nevertheless, there exists a large scope for
addressing the distal community-based factors. Socioeconomic, environmental and psychological
factors hold prime importance in this regard. A holistic approach might be beneficial for
addressing the morbidity and mortality related to stroke among adults in Australia. Appropriate
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

9EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
preventive and management strategies are to e implemented at the earliest for stopping the
increasing prevalence of the condition. Collaboration between government and non-government
organizations are pivotal in this regard.
preventive and management strategies are to e implemented at the earliest for stopping the
increasing prevalence of the condition. Collaboration between government and non-government
organizations are pivotal in this regard.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
References
1. Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, Fang
MC, Fisher M, Furie KL, Heck DV, Johnston SC. Guidelines for the prevention of stroke
in patients with stroke and transient ischemic attack: a guideline for healthcare
professionals from the American Heart Association/American Stroke Association. Stroke.
2014 Jan 1:STR-0000000000000024.
2. Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, Deruyter F, Eng JJ,
Fisher B, Harvey RL, Lang CE. Guidelines for adult stroke rehabilitation and recovery: a
guideline for healthcare professionals from the American Heart Association/American
Stroke Association. Stroke. 2016 Jun 1;47(6):e98-169.
3. Aihw.gov.au. 2018 [cited 21 March 2018]. Available from:
https://www.aihw.gov.au/getmedia/3d56c949-68a4-46f3-bc7c-
c40c89904d38/13994.pdf.aspx?inline=true
4. Bray J, Finn J, Cameron P, Smith K, Straney L, Nehme Z, Bladin C. Stroke Public
Awareness Campaign are Associated With Improved Ambulance Use for Stroke and Tia
in Victoria, Australia.
5. Lynch EA, Cadilhac DA, Luker JA, Hillier SL. Current rehabilitation assessment
practices do not identify any unmet rehabilitation needs for patients with stroke in
Australia. International Journal of Stroke. 2015 Sep 1;10:42.
6. Sacks G, Martin J, Veerman L. Australian sugary drinks tax could prevent thousands of
heart attacks and strokes and save 1600 lives. Journal of the Home Economics Institute of
Australia. 2016;23(1):40.
References
1. Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, Fang
MC, Fisher M, Furie KL, Heck DV, Johnston SC. Guidelines for the prevention of stroke
in patients with stroke and transient ischemic attack: a guideline for healthcare
professionals from the American Heart Association/American Stroke Association. Stroke.
2014 Jan 1:STR-0000000000000024.
2. Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, Deruyter F, Eng JJ,
Fisher B, Harvey RL, Lang CE. Guidelines for adult stroke rehabilitation and recovery: a
guideline for healthcare professionals from the American Heart Association/American
Stroke Association. Stroke. 2016 Jun 1;47(6):e98-169.
3. Aihw.gov.au. 2018 [cited 21 March 2018]. Available from:
https://www.aihw.gov.au/getmedia/3d56c949-68a4-46f3-bc7c-
c40c89904d38/13994.pdf.aspx?inline=true
4. Bray J, Finn J, Cameron P, Smith K, Straney L, Nehme Z, Bladin C. Stroke Public
Awareness Campaign are Associated With Improved Ambulance Use for Stroke and Tia
in Victoria, Australia.
5. Lynch EA, Cadilhac DA, Luker JA, Hillier SL. Current rehabilitation assessment
practices do not identify any unmet rehabilitation needs for patients with stroke in
Australia. International Journal of Stroke. 2015 Sep 1;10:42.
6. Sacks G, Martin J, Veerman L. Australian sugary drinks tax could prevent thousands of
heart attacks and strokes and save 1600 lives. Journal of the Home Economics Institute of
Australia. 2016;23(1):40.
11EPIDEMIOLOGY AND PRINCIPLES OF RESEARCH
7. Sajobi TT, Menon BK, Wang M, Lawal O, Shuaib A, Williams D, Poppe AY, Jovin TG,
Casaubon LK, Devlin T, Dowlatshahi D. Early trajectory of stroke severity predicts long-
term functional outcomes in ischemic stroke subjects: results from the ESCAPE Trial
(Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion
With Emphasis on Minimizing CT to Recanalization Times). Stroke. 2017 Jan
1;48(1):105-10.
8. Davis AP, Billings ME, Longstreth Jr WT, Khot SP. AUTHORS RESPOND: Early
diagnosis and treatment of obstructive sleep apnea after stroke: Are we neglecting a
modifiable stroke risk factor?.
9. Brown DL, Conley KM, Sánchez BN, Resnicow K, Cowdery JE, Sais E, Murphy J,
Skolarus LE, Lisabeth LD, Morgenstern LB. A multicomponent behavioral intervention
to reduce stroke risk factor behaviors: the stroke health and risk education cluster-
randomized controlled trial. Stroke. 2015 Oct 1;46(10):2861-7.
10. Lichtman JH, Froelicher ES, Blumenthal JA, Carney RM, Doering LV, Frasure-Smith N,
Freedland KE, Jaffe AS, Leifheit-Limson EC, Sheps DS, Vaccarino V. American Heart
Association Statistics Committee of the Council on Epidemiology and Prevention and the
Council on Cardiovascular and Stroke Nursing. Depression as a risk factor for poor
prognosis among patients with acute coronary syndrome: systematic review and
recommendations: a scientific statement from the American Heart Association.
Circulation. 2014 Mar 25;129(12):1350-69.
11. Towfighi A, Cheng EM, Ayala-Rivera M, McCreath H, Sanossian N, Dutta T, Mehta B,
Bryg R, Rao N, Song S, Razmara A. Randomized controlled trial of a coordinated care
intervention to improve risk factor control after stroke or transient ischemic attack in the
7. Sajobi TT, Menon BK, Wang M, Lawal O, Shuaib A, Williams D, Poppe AY, Jovin TG,
Casaubon LK, Devlin T, Dowlatshahi D. Early trajectory of stroke severity predicts long-
term functional outcomes in ischemic stroke subjects: results from the ESCAPE Trial
(Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion
With Emphasis on Minimizing CT to Recanalization Times). Stroke. 2017 Jan
1;48(1):105-10.
8. Davis AP, Billings ME, Longstreth Jr WT, Khot SP. AUTHORS RESPOND: Early
diagnosis and treatment of obstructive sleep apnea after stroke: Are we neglecting a
modifiable stroke risk factor?.
9. Brown DL, Conley KM, Sánchez BN, Resnicow K, Cowdery JE, Sais E, Murphy J,
Skolarus LE, Lisabeth LD, Morgenstern LB. A multicomponent behavioral intervention
to reduce stroke risk factor behaviors: the stroke health and risk education cluster-
randomized controlled trial. Stroke. 2015 Oct 1;46(10):2861-7.
10. Lichtman JH, Froelicher ES, Blumenthal JA, Carney RM, Doering LV, Frasure-Smith N,
Freedland KE, Jaffe AS, Leifheit-Limson EC, Sheps DS, Vaccarino V. American Heart
Association Statistics Committee of the Council on Epidemiology and Prevention and the
Council on Cardiovascular and Stroke Nursing. Depression as a risk factor for poor
prognosis among patients with acute coronary syndrome: systematic review and
recommendations: a scientific statement from the American Heart Association.
Circulation. 2014 Mar 25;129(12):1350-69.
11. Towfighi A, Cheng EM, Ayala-Rivera M, McCreath H, Sanossian N, Dutta T, Mehta B,
Bryg R, Rao N, Song S, Razmara A. Randomized controlled trial of a coordinated care
intervention to improve risk factor control after stroke or transient ischemic attack in the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.