Western Sydney University: 401168 Evidence Based Health Care Report
VerifiedAdded on 2023/06/07
|18
|5109
|454
Report
AI Summary
This report provides a comprehensive overview of Evidence Based Healthcare (EBP). It begins by defining EBP, emphasizing its meticulous and judicious use of the best available evidence in clinical decision-making, integrating personal clinical expertise with external research and patient values. The report outlines the two fundamental principles of EBP: the reliance on scientific evidence as a component of decision-making, and the existence of hierarchies guiding evidence interpretation. It details the steps involved in EBP, including developing researchable questions, implementing search strategies, critically assessing evidence, integrating sources, and evaluating outcomes. The report also explores the barriers to implementing EBP, such as lack of support, research skills, and communication issues, while also highlighting facilitators like peer support and adequate resources. Furthermore, the report discusses the importance of patient preference in healthcare decision-making, illustrating this with a clinical experience. Finally, the report includes a PICO question analysis and literature search to identify evidence.

Running Head: EVIDENCE BASED HEALTH CARE 1
Evidence Based Health Care
Name of Student
Institutional Affiliation
Evidence Based Health Care
Name of Student
Institutional Affiliation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
EVIDENCE BASED HEALTH CARE 2
Table of Contents
Part A...................................................................................................................................3
Evidence Based Practice......................................................................................................3
The use of research in clinical practice is faced with several barriers (Scurlo
References....................................................................................................................................6
Part B.................................................................................................................................10
Identification of Evidence..............................................................................................10
Clinical Question and Literature Search........................................................................10
PICO Question...........................................................................................................10
PICO Table................................................................................................................10
Conducting Search.....................................................................................................10
Literature Used; Google Scholar...................................................................................10
PICO Components From; Mortality after Distal Femur Fractures in Elderly
Patients. Clinical Orthopaedics and Related Research.........................................................16
References..........................................................................................................................17
Table of Contents
Part A...................................................................................................................................3
Evidence Based Practice......................................................................................................3
The use of research in clinical practice is faced with several barriers (Scurlo
References....................................................................................................................................6
Part B.................................................................................................................................10
Identification of Evidence..............................................................................................10
Clinical Question and Literature Search........................................................................10
PICO Question...........................................................................................................10
PICO Table................................................................................................................10
Conducting Search.....................................................................................................10
Literature Used; Google Scholar...................................................................................10
PICO Components From; Mortality after Distal Femur Fractures in Elderly
Patients. Clinical Orthopaedics and Related Research.........................................................16
References..........................................................................................................................17
EVIDENCE BASED HEALTH CARE 3
Part A
Evidence Based Practice
Evidence based practice (EBP) is a meticulous, unequivocal and shrewd use of the best
present evidence while performing important decision making for a patient (Khammarnia, Haj
Mohammadi, Amani, Rezaeian & Setoodehzadeh, 2015). Personal clinical expertise is
incorporated together with the finest outer medical evidence from methodical research (Budd,
Hough, Wegener & Stiers, 2017; Schaffer, Sandau & Diedrick, 2012). Patient values, personal
preferences, concerns as well as expectations form part of the decision making process when
identifying the best care for a patient (Joseph-Williams, Elwyn & Edwards, 2014). Quality life
and ideal clinical results come as a result of the integration of the above mentioned aspects
(Duke University Medical Center1, 2018).
The specific component, however, that triggers the whole practice of EBP is encounters
of the patient (Duke University Medical Center1, 2018). These patient experiences generate
questions concerning the effects of treatment, efficacy of diagnostic examinations, the prediction
of diseases and the causes of disorders. EBP has its requirements as the clinician’s new skills,
effective and ability to research competently, and even applying official rules in the evaluation of
clinical literature.
EBP follows some clear steps, strategies and processes. This, like all other practices is
bound to challenges that are barriers or challenges to implementing. This study is going to
expound on all these aspects to form a rational discussion.
There are two fundamental principles assumed by EBP. The first one is that scientific evidence
alone cannot inform competent decision making in clinical care (Rice, 2011). This means that
Part A
Evidence Based Practice
Evidence based practice (EBP) is a meticulous, unequivocal and shrewd use of the best
present evidence while performing important decision making for a patient (Khammarnia, Haj
Mohammadi, Amani, Rezaeian & Setoodehzadeh, 2015). Personal clinical expertise is
incorporated together with the finest outer medical evidence from methodical research (Budd,
Hough, Wegener & Stiers, 2017; Schaffer, Sandau & Diedrick, 2012). Patient values, personal
preferences, concerns as well as expectations form part of the decision making process when
identifying the best care for a patient (Joseph-Williams, Elwyn & Edwards, 2014). Quality life
and ideal clinical results come as a result of the integration of the above mentioned aspects
(Duke University Medical Center1, 2018).
The specific component, however, that triggers the whole practice of EBP is encounters
of the patient (Duke University Medical Center1, 2018). These patient experiences generate
questions concerning the effects of treatment, efficacy of diagnostic examinations, the prediction
of diseases and the causes of disorders. EBP has its requirements as the clinician’s new skills,
effective and ability to research competently, and even applying official rules in the evaluation of
clinical literature.
EBP follows some clear steps, strategies and processes. This, like all other practices is
bound to challenges that are barriers or challenges to implementing. This study is going to
expound on all these aspects to form a rational discussion.
There are two fundamental principles assumed by EBP. The first one is that scientific evidence
alone cannot inform competent decision making in clinical care (Rice, 2011). This means that
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
EVIDENCE BASED HEALTH CARE 4
scientific evidence is only a constituent of the decision making practice and cannot take the role
of the other steps. EBP involves integration of the finest scientific evidence together with best
relevant knowledge and judgment, values and principles held by the patient, and the
circumstances of the patient condition as at the time for clinical examination (Murphy,
MacCarthy, McAllister & Gilbert, 2014).
The second major principle of EBP is that there exist hierarchies that direct how
decisions are to be made within each formula of evidence. This means the processes of EBP are
guided by specific rules on how to interpret the evidence available. This principle particularly
addresses EBP as a wholesome process involving decision makers in healthcare settings
collecting and critically evaluating evidence in guiding decisions. This principle is against the
traditional model of decision making whereby healthcare relied on intuition and information
from superiors’ commands (Murphy, et al., 2014).
In order to put the aforementioned principles of evidence based practice a set of skills/
steps has to be followed. These skills are in components such as developing researchable
question, developing and implementing the best search strategy, critically assessing internal and
external evidence, integrating various evidently sources and finally evaluating outcomes
(Murphy, et al., 2014).
The identification of the problem question is enhanced by an accurate assessment and
competent specialized knowledge and practice (Duke University Medical Center2, 2018;
Murphy, et al., 2014). It is advisable to start with the patient because a clinical question starts or
arises from the care of a patient. The assessment here is patient-focused and it involves focusing
on self-motivated and static risk factors. Here the actuarial risks/ needs of a patient are assessed.
scientific evidence is only a constituent of the decision making practice and cannot take the role
of the other steps. EBP involves integration of the finest scientific evidence together with best
relevant knowledge and judgment, values and principles held by the patient, and the
circumstances of the patient condition as at the time for clinical examination (Murphy,
MacCarthy, McAllister & Gilbert, 2014).
The second major principle of EBP is that there exist hierarchies that direct how
decisions are to be made within each formula of evidence. This means the processes of EBP are
guided by specific rules on how to interpret the evidence available. This principle particularly
addresses EBP as a wholesome process involving decision makers in healthcare settings
collecting and critically evaluating evidence in guiding decisions. This principle is against the
traditional model of decision making whereby healthcare relied on intuition and information
from superiors’ commands (Murphy, et al., 2014).
In order to put the aforementioned principles of evidence based practice a set of skills/
steps has to be followed. These skills are in components such as developing researchable
question, developing and implementing the best search strategy, critically assessing internal and
external evidence, integrating various evidently sources and finally evaluating outcomes
(Murphy, et al., 2014).
The identification of the problem question is enhanced by an accurate assessment and
competent specialized knowledge and practice (Duke University Medical Center2, 2018;
Murphy, et al., 2014). It is advisable to start with the patient because a clinical question starts or
arises from the care of a patient. The assessment here is patient-focused and it involves focusing
on self-motivated and static risk factors. Here the actuarial risks/ needs of a patient are assessed.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
EVIDENCE BASED HEALTH CARE 5
This can also be an offender’s assessment. While in most cases, nurses are unaware to be asking
the relevant question, the process is evolving and thus availing more information. Other people
choose to focus on outcome-based questions. Other ways of formulating a focused researchable
question is by looking at the background and treatment recommendations after appraising
evidence, looking at recommended systematic reviews, and comparison of the situation with the
clinical practice guidelines (Budd, et al., 2017; Evans, Yeung, Markoulakis & Guilcher, 2014)
Searching strategies for evidence can be by use of bibliographic databases that have
scientific research literature like PubMed. Systematic reviews and expert opinions are also steps
of EBP that inform searching for evidence. Looking at policies practiced in other jurisdictions is
also important (Murphy, et al., 2014). Personal experiences are also important aspect but not
widely used. However, there are four sources that have been accepted under the principles of
EBP to be taken into account when looking for evidence. They are scientific literature published
in academic journals, organizational data, facts and figures, practitioners’ experience in their
professional nursing and medical careers, and stakeholders’ values and concerns having been
subjects to previous decisions (Murphy, et al., 2014).
There is a need to appraise evidence critically because of different factors. The first on is
that evidence is not always perfect and can lead one astray in many ways. Evidence have been
overstated giving strong claims but only based on a single information source inapplicable in all
situations (Murphy, et al., 2014). Different clinicians use different ways of appraising evidence
to determine its validity in decision making. This can be by examining the credibility of the
source- well-known and trusted journals which are preferred. Credibility is determined by
another factor; how current is the resource? Adequacy of the evidence must also be considered.
All the guidelines to be followed should be examined whether to be following the Medicine’s
This can also be an offender’s assessment. While in most cases, nurses are unaware to be asking
the relevant question, the process is evolving and thus availing more information. Other people
choose to focus on outcome-based questions. Other ways of formulating a focused researchable
question is by looking at the background and treatment recommendations after appraising
evidence, looking at recommended systematic reviews, and comparison of the situation with the
clinical practice guidelines (Budd, et al., 2017; Evans, Yeung, Markoulakis & Guilcher, 2014)
Searching strategies for evidence can be by use of bibliographic databases that have
scientific research literature like PubMed. Systematic reviews and expert opinions are also steps
of EBP that inform searching for evidence. Looking at policies practiced in other jurisdictions is
also important (Murphy, et al., 2014). Personal experiences are also important aspect but not
widely used. However, there are four sources that have been accepted under the principles of
EBP to be taken into account when looking for evidence. They are scientific literature published
in academic journals, organizational data, facts and figures, practitioners’ experience in their
professional nursing and medical careers, and stakeholders’ values and concerns having been
subjects to previous decisions (Murphy, et al., 2014).
There is a need to appraise evidence critically because of different factors. The first on is
that evidence is not always perfect and can lead one astray in many ways. Evidence have been
overstated giving strong claims but only based on a single information source inapplicable in all
situations (Murphy, et al., 2014). Different clinicians use different ways of appraising evidence
to determine its validity in decision making. This can be by examining the credibility of the
source- well-known and trusted journals which are preferred. Credibility is determined by
another factor; how current is the resource? Adequacy of the evidence must also be considered.
All the guidelines to be followed should be examined whether to be following the Medicine’s
EVIDENCE BASED HEALTH CARE 6
trusted guidelines criteria. Other ways are by seeking intervention from other experts in the
institution and following the clinical reasoning cycle. My decision making while appraising
evidence is by following clinical reasoning.
The application of evidence gathered and appraised also follows a clear incorporation
process into practice. The outcomes of the decision are evaluated at this phase. Gathering input
from literature of high quality, opinion from experts, clients and staff. Financial considerations
are important aspects in this step of EBP (Murphy, et al., 2014).
Evaluation of outcomes is an important phase in that it determines areas to be improved
in the future (Murphy, et al., 2014). This majorly by measuring treatment and prevention
outcomes. All these are determined by the satisfaction of the consumer. To avoid a biased
evaluation it is advisable that the evaluation be done early (in advance).
The use of research in clinical practice is faced with several barriers (Scurlock-Evans,
Upton, & Upton, 2014). This is further affected by the organizational setting where the nurses
operate. When nurses don’t get the necessary support in their respective institutions, then an
effective evidence based practice is with challenges. Another aspect is the nurse’s values of
research and skills, the quality of research and the communication and presentation of research
(Shifaza, Evans & Bradley, 2014).
According to Wood, Ohlsen and Ricketts (2017) in mental health clinics, there are certain
barriers to the implementation of collaborative care as per the EBP model. The study highlights
that lack of efficient case managers, soiled working habits, ineffective commissioners and poor
clinical supervision are among the factors that affect the implementation. These factors inhibit a
good coordination between carers. When there is poor communication implementation of change
trusted guidelines criteria. Other ways are by seeking intervention from other experts in the
institution and following the clinical reasoning cycle. My decision making while appraising
evidence is by following clinical reasoning.
The application of evidence gathered and appraised also follows a clear incorporation
process into practice. The outcomes of the decision are evaluated at this phase. Gathering input
from literature of high quality, opinion from experts, clients and staff. Financial considerations
are important aspects in this step of EBP (Murphy, et al., 2014).
Evaluation of outcomes is an important phase in that it determines areas to be improved
in the future (Murphy, et al., 2014). This majorly by measuring treatment and prevention
outcomes. All these are determined by the satisfaction of the consumer. To avoid a biased
evaluation it is advisable that the evaluation be done early (in advance).
The use of research in clinical practice is faced with several barriers (Scurlock-Evans,
Upton, & Upton, 2014). This is further affected by the organizational setting where the nurses
operate. When nurses don’t get the necessary support in their respective institutions, then an
effective evidence based practice is with challenges. Another aspect is the nurse’s values of
research and skills, the quality of research and the communication and presentation of research
(Shifaza, Evans & Bradley, 2014).
According to Wood, Ohlsen and Ricketts (2017) in mental health clinics, there are certain
barriers to the implementation of collaborative care as per the EBP model. The study highlights
that lack of efficient case managers, soiled working habits, ineffective commissioners and poor
clinical supervision are among the factors that affect the implementation. These factors inhibit a
good coordination between carers. When there is poor communication implementation of change
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
EVIDENCE BASED HEALTH CARE 7
becomes a problem (Dang & Dearholt, 2017) .Communication relates to the presentation of
research and that can be either a barrier or a facilitation to literature. When literature is
physically available or published, compiled in one location, statistical analyses being
understandable and the nurse is fully aware of where to find it, the evidence based practice
become a success (Shifaza, et al., 2014). While the aforementioned factors are negative
(barriers), poor EBP results are expected.
This is also supported by another study Bach-Mortensen, Lange & Montgomery (2018)
that lack of support and expertise, and insufficient guidelines on how to perform the care affect
the adaptation of EBPs in clinical fields.
There are also facilitators of the use of research that support an effective interpretation of
the identified literature. They include, peer support by the management, sufficient time to allow
for a review of the literature, the presence of supportive colleagues, availability and adequacy of
the relevant research, reassuring policies, and opportunities for training (Hersen & Sturmey,
2013). These barriers and facilitators can be categorized into, individual factors,
communicational factors, administrative factors and value of research (Shifaza, et al., 2014).
Individual barriers include poor research skills from lack of efficient research methods,
deprived consciousness of research outcomes, poor appraisal skills and even an adverse attitude
towards research (Shifaza, et al., 2014). When a nurse in a mental clinic is not well acquainted
with research skills, she might be unable to apply the best EBP for a patient with other medical
issues apart from mental illness. The beliefs of nurses concerning the significance of research
and self-confidence in the research skills affect EBP decision making. When the nurse has no
confidence in implementing change, the outcomes of her decision are likely to be poor. The same
becomes a problem (Dang & Dearholt, 2017) .Communication relates to the presentation of
research and that can be either a barrier or a facilitation to literature. When literature is
physically available or published, compiled in one location, statistical analyses being
understandable and the nurse is fully aware of where to find it, the evidence based practice
become a success (Shifaza, et al., 2014). While the aforementioned factors are negative
(barriers), poor EBP results are expected.
This is also supported by another study Bach-Mortensen, Lange & Montgomery (2018)
that lack of support and expertise, and insufficient guidelines on how to perform the care affect
the adaptation of EBPs in clinical fields.
There are also facilitators of the use of research that support an effective interpretation of
the identified literature. They include, peer support by the management, sufficient time to allow
for a review of the literature, the presence of supportive colleagues, availability and adequacy of
the relevant research, reassuring policies, and opportunities for training (Hersen & Sturmey,
2013). These barriers and facilitators can be categorized into, individual factors,
communicational factors, administrative factors and value of research (Shifaza, et al., 2014).
Individual barriers include poor research skills from lack of efficient research methods,
deprived consciousness of research outcomes, poor appraisal skills and even an adverse attitude
towards research (Shifaza, et al., 2014). When a nurse in a mental clinic is not well acquainted
with research skills, she might be unable to apply the best EBP for a patient with other medical
issues apart from mental illness. The beliefs of nurses concerning the significance of research
and self-confidence in the research skills affect EBP decision making. When the nurse has no
confidence in implementing change, the outcomes of her decision are likely to be poor. The same
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
EVIDENCE BASED HEALTH CARE 8
case with inability to evaluate quality research from poor research. The opposite of all these
individual barriers is a facilitation to effective EBP.
These are also certain limitations in the institution where EBP is to be performed. The
factors relate to lack of enough time to read, examine, scrutinize, publicize, and implement the
evidence from research (Joseph-Williams, et al., 2014). Others include inadequacy in authority
and facilities to propagate change in the practice setting or support the implementation process
(Duncombe, 2018; Shifaza, et al., 2014).
Patient preference is an analysis of a person who is knowledgeable concerning likelihood
and severity of the consequences and hazards of medical interventions, procedure and results
from aspects of healthcare. Clinical practice guidelines ought to be adopted in a manner that it is
not only the provider’s interests are considered but also the patient’s point of view. Patients have
different characteristics and preferences and therefore the care directed to them should be
flexible to adapt to those preferences in a manner that the patient will take part in the decision
making process. Involvement requires that providers give information to the patient while taking
an action and asking the patient of his or her opinion for the same, how he likes it to be done and
how he generally feels about the EBP paradigm (Budd, et al., 2017).
As much as it is essential to include consumers in the decision making process, some
situations do not necessarily seek patient’s preference. In one of my clinical experiences, a
woman (Veronica) of an advanced age (86 year old) had a fall that broke her left femoral neck,
dislocated uncle and profuse bleeding from bruised knee and shoulder. That was itself an
emergency considering the woman was weak and old and was admitted into the emergency
department unconscious. The decision I made as at that time were not by any way related to the
patient’s preference but I relied on the other aspects of EBP to offer care in collaboration with
case with inability to evaluate quality research from poor research. The opposite of all these
individual barriers is a facilitation to effective EBP.
These are also certain limitations in the institution where EBP is to be performed. The
factors relate to lack of enough time to read, examine, scrutinize, publicize, and implement the
evidence from research (Joseph-Williams, et al., 2014). Others include inadequacy in authority
and facilities to propagate change in the practice setting or support the implementation process
(Duncombe, 2018; Shifaza, et al., 2014).
Patient preference is an analysis of a person who is knowledgeable concerning likelihood
and severity of the consequences and hazards of medical interventions, procedure and results
from aspects of healthcare. Clinical practice guidelines ought to be adopted in a manner that it is
not only the provider’s interests are considered but also the patient’s point of view. Patients have
different characteristics and preferences and therefore the care directed to them should be
flexible to adapt to those preferences in a manner that the patient will take part in the decision
making process. Involvement requires that providers give information to the patient while taking
an action and asking the patient of his or her opinion for the same, how he likes it to be done and
how he generally feels about the EBP paradigm (Budd, et al., 2017).
As much as it is essential to include consumers in the decision making process, some
situations do not necessarily seek patient’s preference. In one of my clinical experiences, a
woman (Veronica) of an advanced age (86 year old) had a fall that broke her left femoral neck,
dislocated uncle and profuse bleeding from bruised knee and shoulder. That was itself an
emergency considering the woman was weak and old and was admitted into the emergency
department unconscious. The decision I made as at that time were not by any way related to the
patient’s preference but I relied on the other aspects of EBP to offer care in collaboration with
EVIDENCE BASED HEALTH CARE 9
my colleagues and deriving the best method to administer care from my superiors and informed
literature search. Veronica’s son who was present just told me to do what is right to help her
mother. His preference was based on what I would choose to do to help the situation.
Some patients are strongly affiliated to their culture, religion, social and spiritual values
(Goldstein & Morrison, 2013). These factors to them are what establish quality of life and
personal beliefs about health. Despite that these factors may be overlooked at some situations, it
is always advisable to put the preferences into considerations as they may determine the
subjectivity of the patient to care given or advised.
my colleagues and deriving the best method to administer care from my superiors and informed
literature search. Veronica’s son who was present just told me to do what is right to help her
mother. His preference was based on what I would choose to do to help the situation.
Some patients are strongly affiliated to their culture, religion, social and spiritual values
(Goldstein & Morrison, 2013). These factors to them are what establish quality of life and
personal beliefs about health. Despite that these factors may be overlooked at some situations, it
is always advisable to put the preferences into considerations as they may determine the
subjectivity of the patient to care given or advised.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
EVIDENCE BASED HEALTH CARE 10
Part B
Identification of Evidence
Clinical Question and Literature Search
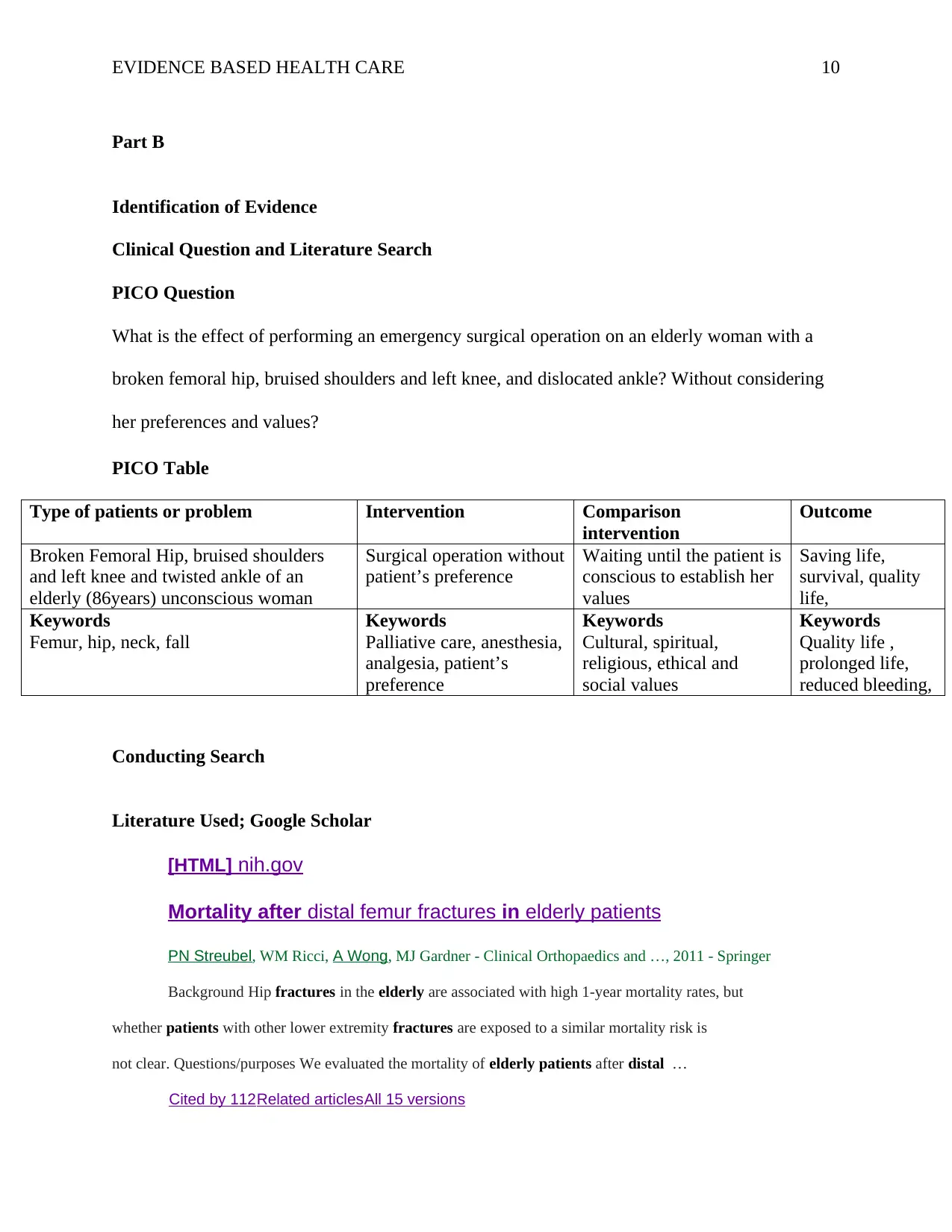
PICO Question
What is the effect of performing an emergency surgical operation on an elderly woman with a
broken femoral hip, bruised shoulders and left knee, and dislocated ankle? Without considering
her preferences and values?
PICO Table
Type of patients or problem Intervention Comparison
intervention
Outcome
Broken Femoral Hip, bruised shoulders
and left knee and twisted ankle of an
elderly (86years) unconscious woman
Surgical operation without
patient’s preference
Waiting until the patient is
conscious to establish her
values
Saving life,
survival, quality
life,
Keywords
Femur, hip, neck, fall
Keywords
Palliative care, anesthesia,
analgesia, patient’s
preference
Keywords
Cultural, spiritual,
religious, ethical and
social values
Keywords
Quality life ,
prolonged life,
reduced bleeding,
Conducting Search
Literature Used; Google Scholar
[HTML] nih.gov
Mortality after distal femur fractures in elderly patients
PN Streubel, WM Ricci, A Wong, MJ Gardner - Clinical Orthopaedics and …, 2011 - Springer
Background Hip fractures in the elderly are associated with high 1-year mortality rates, but
whether patients with other lower extremity fractures are exposed to a similar mortality risk is
not clear. Questions/purposes We evaluated the mortality of elderly patients after distal …
Cited by 112 Related articles All 15 versions
Part B
Identification of Evidence
Clinical Question and Literature Search
PICO Question
What is the effect of performing an emergency surgical operation on an elderly woman with a
broken femoral hip, bruised shoulders and left knee, and dislocated ankle? Without considering
her preferences and values?
PICO Table
Type of patients or problem Intervention Comparison
intervention
Outcome
Broken Femoral Hip, bruised shoulders
and left knee and twisted ankle of an
elderly (86years) unconscious woman
Surgical operation without
patient’s preference
Waiting until the patient is
conscious to establish her
values
Saving life,
survival, quality
life,
Keywords
Femur, hip, neck, fall
Keywords
Palliative care, anesthesia,
analgesia, patient’s
preference
Keywords
Cultural, spiritual,
religious, ethical and
social values
Keywords
Quality life ,
prolonged life,
reduced bleeding,
Conducting Search
Literature Used; Google Scholar
[HTML] nih.gov
Mortality after distal femur fractures in elderly patients
PN Streubel, WM Ricci, A Wong, MJ Gardner - Clinical Orthopaedics and …, 2011 - Springer
Background Hip fractures in the elderly are associated with high 1-year mortality rates, but
whether patients with other lower extremity fractures are exposed to a similar mortality risk is
not clear. Questions/purposes We evaluated the mortality of elderly patients after distal …
Cited by 112 Related articles All 15 versions
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

EVIDENCE BASED HEALTH CARE 11
Distal femur fractures of the elderly—different treatment options in a
biomechanical comparison
D Wähnert, K Hoffmeier, R Fröber, GO Hofmann… - Injury, 2011 - Elsevier
… the four-screw distal locking (SCN) and lowest for two screws distally (T2 … al.Biomechanical
evaluation of the less invasive stabilization system for the internal fixation of distal femur fractures …
Meyer, NA Plaxton, PD Postak, et al.Mechanical comparison of a distal femoral side plate …
Cited by 55Related articles All 8 versions
Risk factors for failure of locked plate fixation of distal femur fractures:
an analysis of 335 cases
WM Ricci, PN Streubel, S Morshed… - … of orthopaedic trauma, 2014 - journals.lww.com
Objectives:Locked plating has become a standard method
to treat supracondylar femur fractures. Emerg.
Cited by 123 Related articles All 7 versions
High complication rate in locking plate fixation of lower
periprosthetic distal femur fractures in patients with total knee arthroplasties
NA Ebraheim, J Liu, SZ Hashmi, KR Sochacki… - The Journal of …, 2012 - Elsevier
… Distal femoral fractures adjacent to a total knee arthroplasty present surgeons with a challenging
situation … procedure, and the challenges faced, the current study found that contralateral reverse
locking plate fixation of a distal periprosthetic femur fracture in patients …
Cited by 46Related articles All 5 versions
… periprosthetic fractures of the knee in the elderly patients: a
comparison of treatment using allograft-implant composites, standard
revision components, distal femoral …
K Saidi, O Ben-Lulu, M Tsuji, O Safir, AE Gross… - The Journal of …, 2014 - Elsevier
Distal femur fractures of the elderly—different treatment options in a
biomechanical comparison
D Wähnert, K Hoffmeier, R Fröber, GO Hofmann… - Injury, 2011 - Elsevier
… the four-screw distal locking (SCN) and lowest for two screws distally (T2 … al.Biomechanical
evaluation of the less invasive stabilization system for the internal fixation of distal femur fractures …
Meyer, NA Plaxton, PD Postak, et al.Mechanical comparison of a distal femoral side plate …
Cited by 55Related articles All 8 versions
Risk factors for failure of locked plate fixation of distal femur fractures:
an analysis of 335 cases
WM Ricci, PN Streubel, S Morshed… - … of orthopaedic trauma, 2014 - journals.lww.com
Objectives:Locked plating has become a standard method
to treat supracondylar femur fractures. Emerg.
Cited by 123 Related articles All 7 versions
High complication rate in locking plate fixation of lower
periprosthetic distal femur fractures in patients with total knee arthroplasties
NA Ebraheim, J Liu, SZ Hashmi, KR Sochacki… - The Journal of …, 2012 - Elsevier
… Distal femoral fractures adjacent to a total knee arthroplasty present surgeons with a challenging
situation … procedure, and the challenges faced, the current study found that contralateral reverse
locking plate fixation of a distal periprosthetic femur fracture in patients …
Cited by 46Related articles All 5 versions
… periprosthetic fractures of the knee in the elderly patients: a
comparison of treatment using allograft-implant composites, standard
revision components, distal femoral …
K Saidi, O Ben-Lulu, M Tsuji, O Safir, AE Gross… - The Journal of …, 2014 - Elsevier
EVIDENCE BASED HEALTH CARE 12
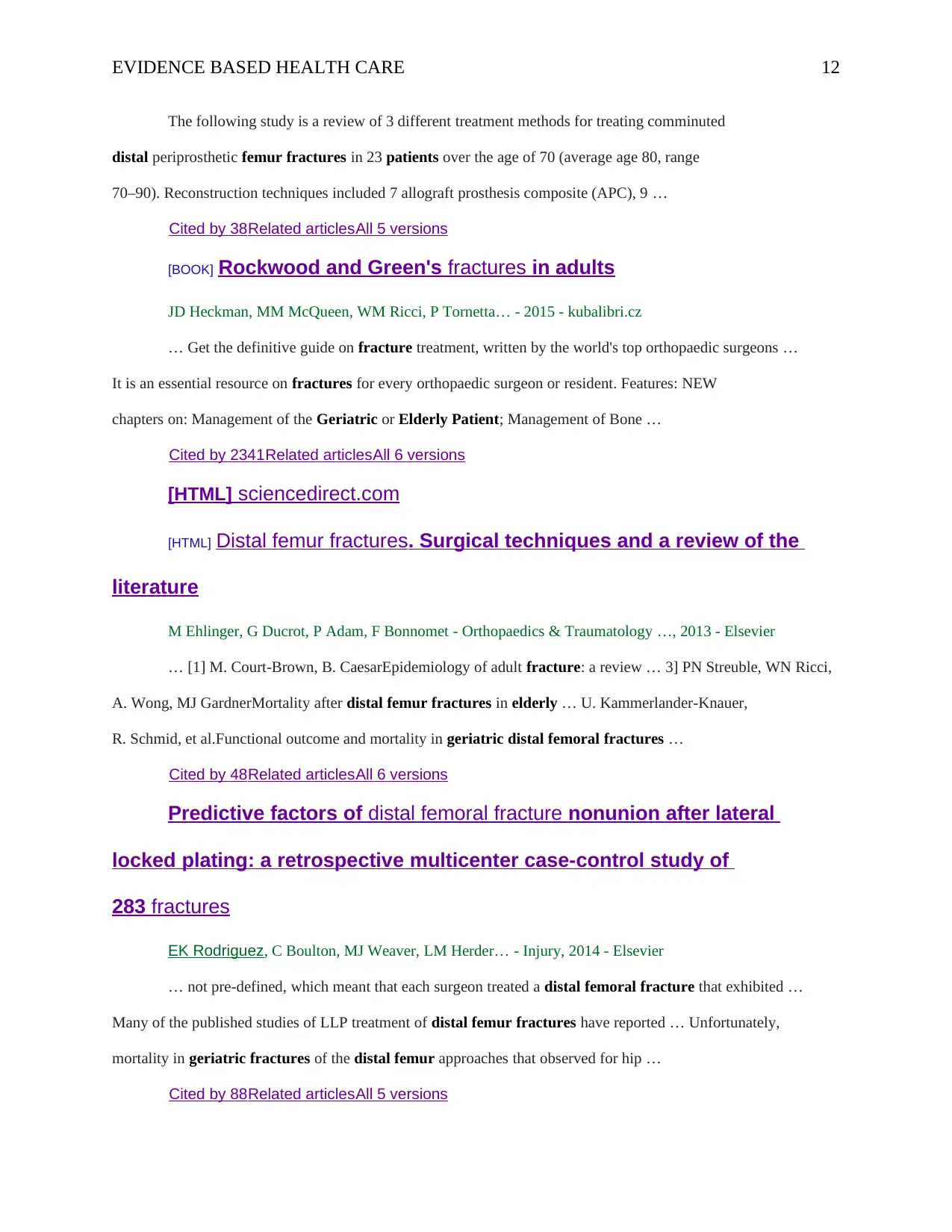
The following study is a review of 3 different treatment methods for treating comminuted
distal periprosthetic femur fractures in 23 patients over the age of 70 (average age 80, range
70–90). Reconstruction techniques included 7 allograft prosthesis composite (APC), 9 …
Cited by 38Related articles All 5 versions
[BOOK] Rockwood and Green's fractures in adults
JD Heckman, MM McQueen, WM Ricci, P Tornetta… - 2015 - kubalibri.cz
… Get the definitive guide on fracture treatment, written by the world's top orthopaedic surgeons …
It is an essential resource on fractures for every orthopaedic surgeon or resident. Features: NEW
chapters on: Management of the Geriatric or Elderly Patient; Management of Bone …
Cited by 2341 Related articlesAll 6 versions
[HTML] sciencedirect.com
[HTML] Distal femur fractures. Surgical techniques and a review of the
literature
M Ehlinger, G Ducrot, P Adam, F Bonnomet - Orthopaedics & Traumatology …, 2013 - Elsevier
… [1] M. Court-Brown, B. CaesarEpidemiology of adult fracture: a review … 3] PN Streuble, WN Ricci,
A. Wong, MJ GardnerMortality after distal femur fractures in elderly … U. Kammerlander-Knauer,
R. Schmid, et al.Functional outcome and mortality in geriatric distal femoral fractures …
Cited by 48Related articles All 6 versions
Predictive factors of distal femoral fracture nonunion after lateral
locked plating: a retrospective multicenter case-control study of
283 fractures
EK Rodriguez, C Boulton, MJ Weaver, LM Herder… - Injury, 2014 - Elsevier
… not pre-defined, which meant that each surgeon treated a distal femoral fracture that exhibited …
Many of the published studies of LLP treatment of distal femur fractures have reported … Unfortunately,
mortality in geriatric fractures of the distal femur approaches that observed for hip …
Cited by 88Related articles All 5 versions
The following study is a review of 3 different treatment methods for treating comminuted
distal periprosthetic femur fractures in 23 patients over the age of 70 (average age 80, range
70–90). Reconstruction techniques included 7 allograft prosthesis composite (APC), 9 …
Cited by 38Related articles All 5 versions
[BOOK] Rockwood and Green's fractures in adults
JD Heckman, MM McQueen, WM Ricci, P Tornetta… - 2015 - kubalibri.cz
… Get the definitive guide on fracture treatment, written by the world's top orthopaedic surgeons …
It is an essential resource on fractures for every orthopaedic surgeon or resident. Features: NEW
chapters on: Management of the Geriatric or Elderly Patient; Management of Bone …
Cited by 2341 Related articlesAll 6 versions
[HTML] sciencedirect.com
[HTML] Distal femur fractures. Surgical techniques and a review of the
literature
M Ehlinger, G Ducrot, P Adam, F Bonnomet - Orthopaedics & Traumatology …, 2013 - Elsevier
… [1] M. Court-Brown, B. CaesarEpidemiology of adult fracture: a review … 3] PN Streuble, WN Ricci,
A. Wong, MJ GardnerMortality after distal femur fractures in elderly … U. Kammerlander-Knauer,
R. Schmid, et al.Functional outcome and mortality in geriatric distal femoral fractures …
Cited by 48Related articles All 6 versions
Predictive factors of distal femoral fracture nonunion after lateral
locked plating: a retrospective multicenter case-control study of
283 fractures
EK Rodriguez, C Boulton, MJ Weaver, LM Herder… - Injury, 2014 - Elsevier
… not pre-defined, which meant that each surgeon treated a distal femoral fracture that exhibited …
Many of the published studies of LLP treatment of distal femur fractures have reported … Unfortunately,
mortality in geriatric fractures of the distal femur approaches that observed for hip …
Cited by 88Related articles All 5 versions
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 18
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.