EXSC 610: Chapter Essay Questions - Module/Week 4 Assignment
VerifiedAdded on 2022/11/14
|4
|1016
|288
Homework Assignment
AI Summary
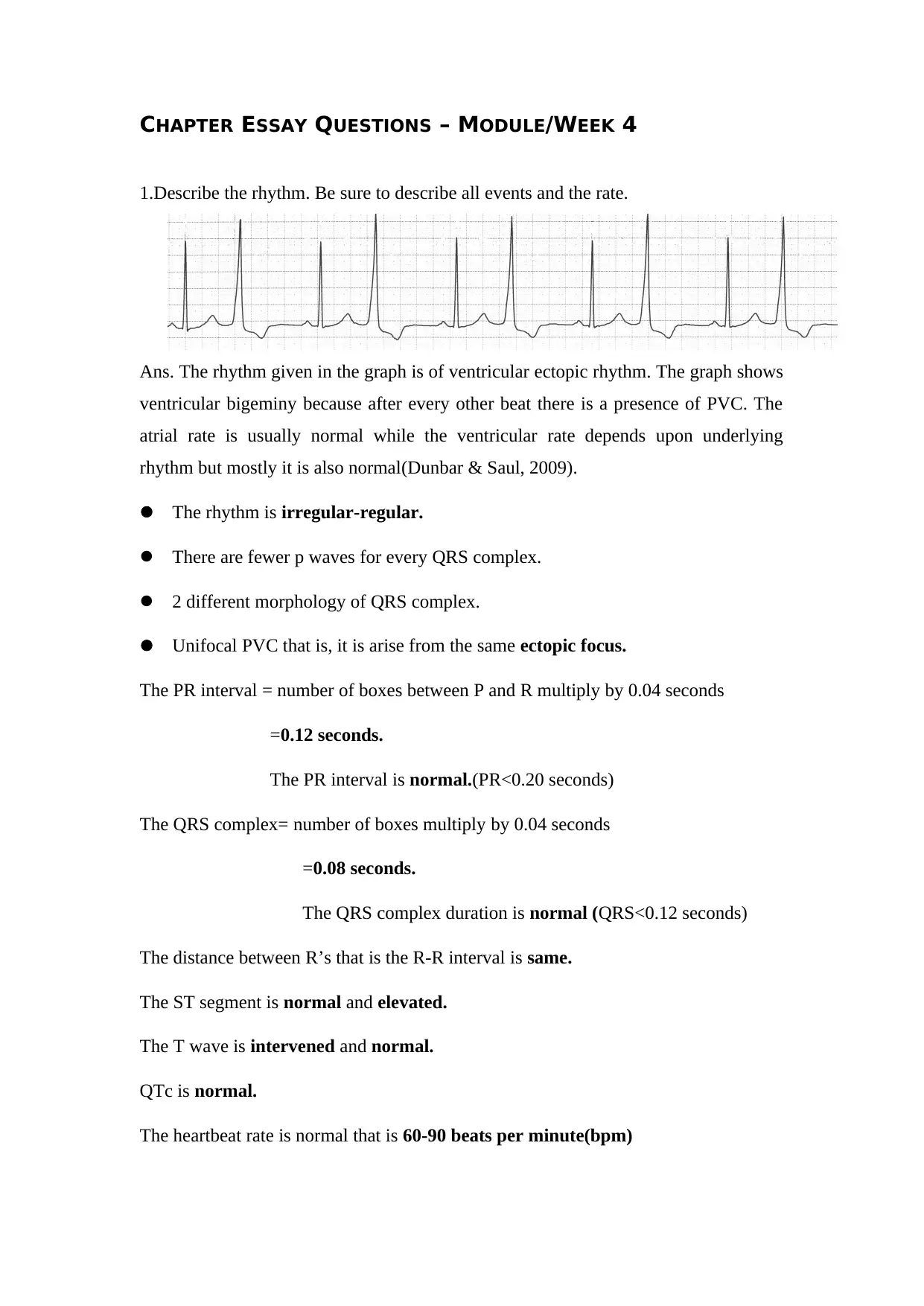
This assignment addresses four essay questions related to ECG interpretation and cardiac rhythms. The first question describes a ventricular ectopic rhythm, detailing the presence of ventricular bigeminy, PVCs, and the characteristics of the ECG graph. The second question explains the causes and variations of PVCs, including single, doublet, triplet, and multiform types. The third question explores the function of electronic pacemakers and their impact on ECG readings, including how they alter QRS complexes and maintain a stable heart rate. The final question defines third-degree atrioventricular block and distinguishes it from atrioventricular dissociation, highlighting the differences in their conditions and ECG presentations. The assignment references the course textbook and additional scholarly sources to support the explanations.
1 out of 4



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.