EXSC 610: Analysis of ECG Waveforms and Heart Rate Methods
VerifiedAdded on 2022/12/14
|8
|1640
|1
Homework Assignment
AI Summary
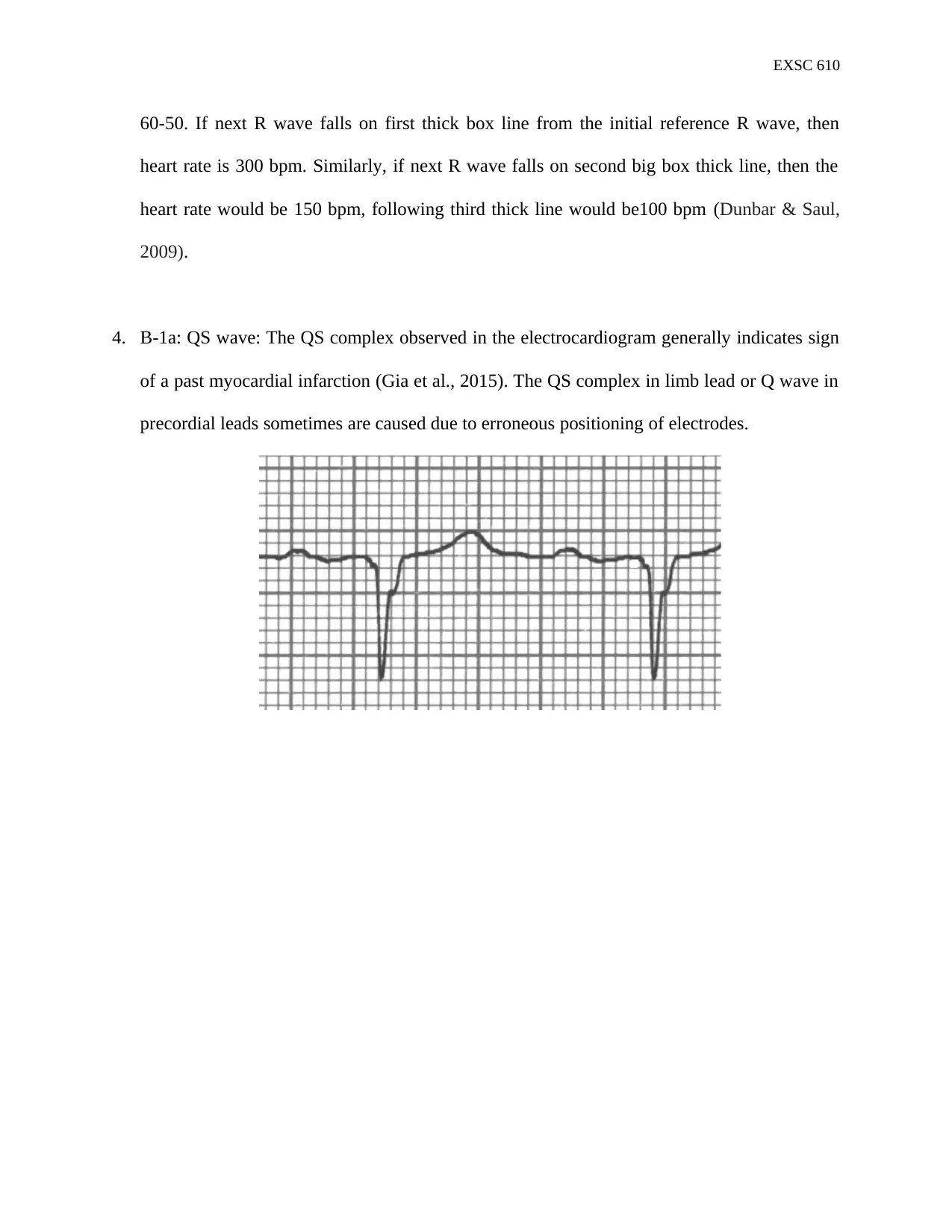
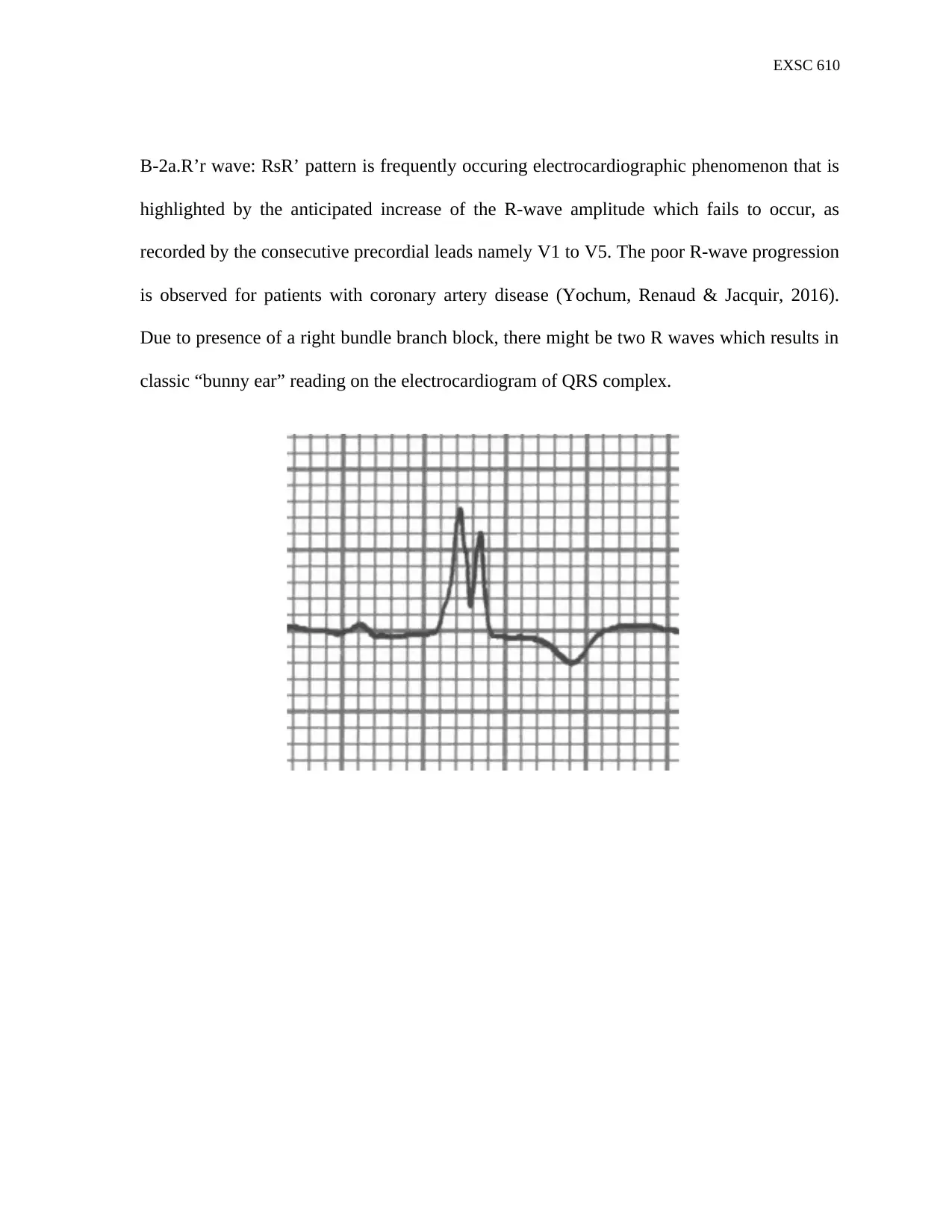
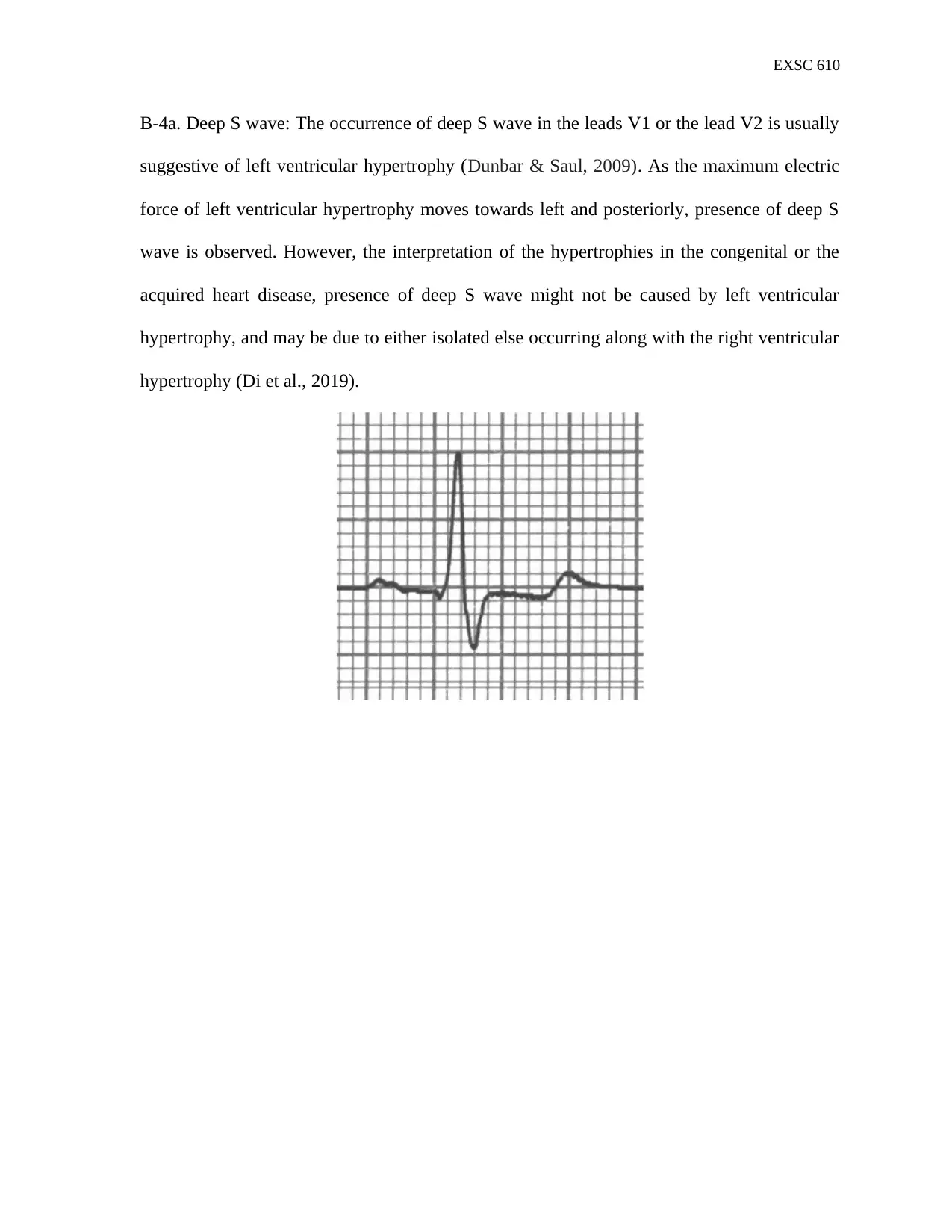
This document provides a comprehensive solution to an EXSC 610 assignment, focusing on the analysis of electrocardiograms (ECGs). The assignment delves into the interpretation of ECG waveforms, specifically the P wave, QRS complex, and T wave, explaining their physiological significance. It also details two methods for calculating heart rate: the 1500 method and the triplets method, providing step-by-step explanations for each. Furthermore, the solution analyzes specific QRS complex morphologies, including QS wave, R'r wave, and deep S wave, linking them to potential clinical implications such as myocardial infarction and ventricular hypertrophy. The document is well-referenced, citing the course textbook and additional scholarly sources to support the interpretations and methods described.
1 out of 8
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.