Certificate III Fitness - Assessment 3.2: Client Appraisal & Screening
VerifiedAdded on 2022/10/17
|24
|6720
|5
Practical Assignment
AI Summary
This assignment focuses on client screening and fitness assessment, a core component of the Certificate III in Fitness. Students are tasked with conducting a 60-minute health screening and fitness assessment for a chosen client from provided case studies. The assessment requires the use of the Fitness Australia Pre-exercise Screening tool, including explaining the purpose, discussing outcomes, and completing Stages 1 and 2. Students must also conduct and record goal setting, health appraisals (resting heart rate, blood pressure, BMI, W:H ratio, girths, skinfolds, BIA), and fitness appraisals (aerobic submax or step test, sit & reach, maximal push-up test, plank test, and curl-ups test). The assignment emphasizes obtaining consent, using effective communication, and explaining the rationale behind each test. The assessment evaluates the student's ability to apply theoretical knowledge to a practical scenario, demonstrating their understanding of client assessment protocols and procedures.
1 | Document 355 - Assessment 3.2 - Client Screening &
Assessment v3
Assessment 3.2
Client Screening & Assessment
Assessment 3.2 Instructions and Required Resources
Before you begin CLICK HERE to watch aninstructional video on how to successfully complete this
assessment. This video will outline the skills and resources you require to receive an excellent grade.
Prior to completing this assessment, we recommend you watch the following online lecture presentatio
relevant to this assessment:
Lecture Presentation 3.1 - The Components of a Health Screening
Lecture Presentation 3.2 - Delivering a First Class Health Screening
Lecture Presentation 3.3 - Health Assessments
Lecture Presentation 3.4 - Physical Fitness Assessments
Lecture Presentation 3.5 - Understanding the Referral Process
Prior to completing this assessment, we recommend you read the following chapter from the Certificat
Fitness Course Manual
Chapter 3 - Client Screening & Assessment
Student Name
Assessor Name
Qualification SIS30315 - Certificate III in Fitness
Delivery Method Online Face to Face
Assessment Type Case Study Role Play
Units of Competency
SISFFIT001 Provide health screening and fitness orientation
SISFFIT006 Conduct fitness appraisals
Please complete the following:
Declaration: I have read, understand and agree to the assessment tasks and criteria outline
document and agree to complete this assessment in accordance with Australian Fitness Acade
assessment policy. I declare that all evidence submitted for this assessment is the product of
work and every attempt has been made to accurately reference all sources to prevent plagiar
STUDENT SIGNATURE: Date:
Assessment v3
Assessment 3.2
Client Screening & Assessment
Assessment 3.2 Instructions and Required Resources
Before you begin CLICK HERE to watch aninstructional video on how to successfully complete this
assessment. This video will outline the skills and resources you require to receive an excellent grade.
Prior to completing this assessment, we recommend you watch the following online lecture presentatio
relevant to this assessment:
Lecture Presentation 3.1 - The Components of a Health Screening
Lecture Presentation 3.2 - Delivering a First Class Health Screening
Lecture Presentation 3.3 - Health Assessments
Lecture Presentation 3.4 - Physical Fitness Assessments
Lecture Presentation 3.5 - Understanding the Referral Process
Prior to completing this assessment, we recommend you read the following chapter from the Certificat
Fitness Course Manual
Chapter 3 - Client Screening & Assessment
Student Name
Assessor Name
Qualification SIS30315 - Certificate III in Fitness
Delivery Method Online Face to Face
Assessment Type Case Study Role Play
Units of Competency
SISFFIT001 Provide health screening and fitness orientation
SISFFIT006 Conduct fitness appraisals
Please complete the following:
Declaration: I have read, understand and agree to the assessment tasks and criteria outline
document and agree to complete this assessment in accordance with Australian Fitness Acade
assessment policy. I declare that all evidence submitted for this assessment is the product of
work and every attempt has been made to accurately reference all sources to prevent plagiar
STUDENT SIGNATURE: Date:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

AUSTRALIAN FITNESS ACADEMY © | 2
Student Assessment Tasks
This assessment is to be completed after reviewing resources from Topic 3 – Client Screening
Assessment
Students are required to address ALL questions in this assessment task.
To complete the assessment:
• Download the document ‘Assessment 3.2 – Case Studies - Initial Appraisal’.
• Give the case studies to a friend, family member or classmate and have them select one of t
clients from the case study options.
• Have your friend, family member or classmate play the role of the chosen client and conduct
60-minute health screening and fitness assessment for them.
• Your friend, family member or classmate will be required to respond to your questions using
information provided in the chosen case study.
Task A:
When conducting the health and fitness consultation for your client:
1. Using the editable Fitness Australia Pre-exercise Screening tool on the next page, conduct a
pre-exercise health screening for your client (based on the case study provided):
When completing the pre-exercise screening be sure to:
a. Explain the purpose of pre-exercise health screening questionnaire to the client
b. Discuss the outcomes of the pre-exercise screening questionnaire with the client
c. Complete Stages 1 and 2 of the form
Assessor Use Only
Satisfactory Resubmit
ASSESSMENT TIP
Before you complete the Fitness Australia Pre-exercise Screening Tool
each of the following resources which will assist you in completing the
screening document:
• Adult Pre-Exercise Screening Tool - User Guide
• Instructional Video - How to complete the Fitness Australia Pre-Exerc
Screening Tool
Student Assessment Tasks
This assessment is to be completed after reviewing resources from Topic 3 – Client Screening
Assessment
Students are required to address ALL questions in this assessment task.
To complete the assessment:
• Download the document ‘Assessment 3.2 – Case Studies - Initial Appraisal’.
• Give the case studies to a friend, family member or classmate and have them select one of t
clients from the case study options.
• Have your friend, family member or classmate play the role of the chosen client and conduct
60-minute health screening and fitness assessment for them.
• Your friend, family member or classmate will be required to respond to your questions using
information provided in the chosen case study.
Task A:
When conducting the health and fitness consultation for your client:
1. Using the editable Fitness Australia Pre-exercise Screening tool on the next page, conduct a
pre-exercise health screening for your client (based on the case study provided):
When completing the pre-exercise screening be sure to:
a. Explain the purpose of pre-exercise health screening questionnaire to the client
b. Discuss the outcomes of the pre-exercise screening questionnaire with the client
c. Complete Stages 1 and 2 of the form
Assessor Use Only
Satisfactory Resubmit
ASSESSMENT TIP
Before you complete the Fitness Australia Pre-exercise Screening Tool
each of the following resources which will assist you in completing the
screening document:
• Adult Pre-Exercise Screening Tool - User Guide
• Instructional Video - How to complete the Fitness Australia Pre-Exerc
Screening Tool
Page 3
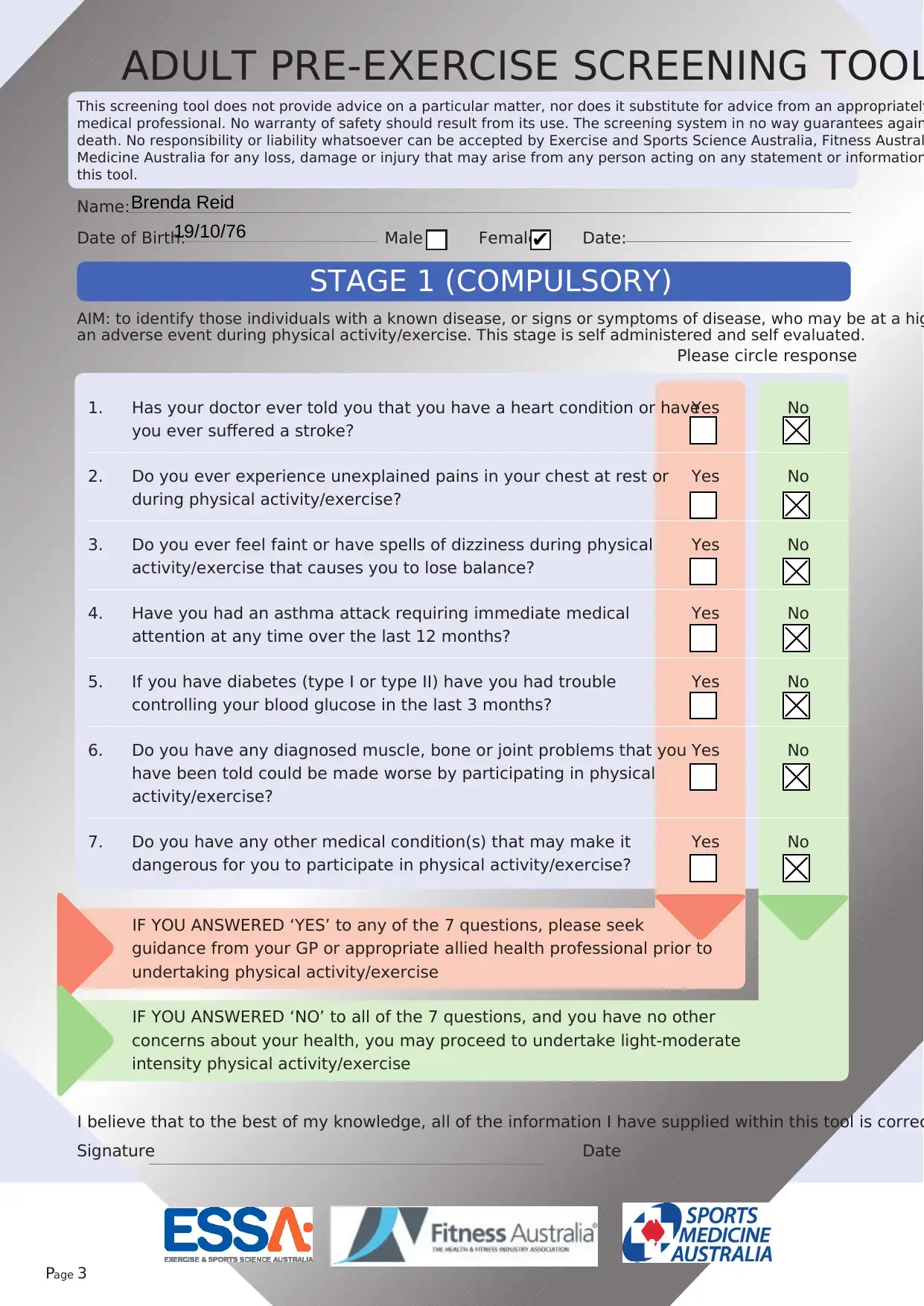
ADULT PRE-EXERCISE SCREENING TOOL
STAGE 1 (COMPULSORY)
AIM: to identify those individuals with a known disease, or signs or symptoms of disease, who may be at a hig
an adverse event during physical activity/exercise. This stage is self administered and self evaluated.
1. Has your doctor ever told you that you have a heart condition or have
you ever suffered a stroke?
Yes No
2. Do you ever experience unexplained pains in your chest at rest or
during physical activity/exercise?
Yes No
3. Do you ever feel faint or have spells of dizziness during physical
activity/exercise that causes you to lose balance?
Yes No
4. Have you had an asthma attack requiring immediate medical
attention at any time over the last 12 months?
Yes No
5. If you have diabetes (type I or type II) have you had trouble
controlling your blood glucose in the last 3 months?
Yes No
6. Do you have any diagnosed muscle, bone or joint problems that you
have been told could be made worse by participating in physical
activity/exercise?
Yes No
7. Do you have any other medical condition(s) that may make it
dangerous for you to participate in physical activity/exercise?
Yes No
IF YOU ANSWERED ‘YES’ to any of the 7 questions, please seek
guidance from your GP or appropriate allied health professional prior to
undertaking physical activity/exercise
IF YOU ANSWERED ‘NO’ to all of the 7 questions, and you have no other
concerns about your health, you may proceed to undertake light-moderate
intensity physical activity/exercise
Name:
Date of Birth: Male Female Date:
Please circle response
This screening tool does not provide advice on a particular matter, nor does it substitute for advice from an appropriately
medical professional. No warranty of safety should result from its use. The screening system in no way guarantees again
death. No responsibility or liability whatsoever can be accepted by Exercise and Sports Science Australia, Fitness Austral
Medicine Australia for any loss, damage or injury that may arise from any person acting on any statement or information
this tool.
I believe that to the best of my knowledge, all of the information I have supplied within this tool is correc
Signature Date
Brenda Reid
19/10/76 ✔
ADULT PRE-EXERCISE SCREENING TOOL
STAGE 1 (COMPULSORY)
AIM: to identify those individuals with a known disease, or signs or symptoms of disease, who may be at a hig
an adverse event during physical activity/exercise. This stage is self administered and self evaluated.
1. Has your doctor ever told you that you have a heart condition or have
you ever suffered a stroke?
Yes No
2. Do you ever experience unexplained pains in your chest at rest or
during physical activity/exercise?
Yes No
3. Do you ever feel faint or have spells of dizziness during physical
activity/exercise that causes you to lose balance?
Yes No
4. Have you had an asthma attack requiring immediate medical
attention at any time over the last 12 months?
Yes No
5. If you have diabetes (type I or type II) have you had trouble
controlling your blood glucose in the last 3 months?
Yes No
6. Do you have any diagnosed muscle, bone or joint problems that you
have been told could be made worse by participating in physical
activity/exercise?
Yes No
7. Do you have any other medical condition(s) that may make it
dangerous for you to participate in physical activity/exercise?
Yes No
IF YOU ANSWERED ‘YES’ to any of the 7 questions, please seek
guidance from your GP or appropriate allied health professional prior to
undertaking physical activity/exercise
IF YOU ANSWERED ‘NO’ to all of the 7 questions, and you have no other
concerns about your health, you may proceed to undertake light-moderate
intensity physical activity/exercise
Name:
Date of Birth: Male Female Date:
Please circle response
This screening tool does not provide advice on a particular matter, nor does it substitute for advice from an appropriately
medical professional. No warranty of safety should result from its use. The screening system in no way guarantees again
death. No responsibility or liability whatsoever can be accepted by Exercise and Sports Science Australia, Fitness Austral
Medicine Australia for any loss, damage or injury that may arise from any person acting on any statement or information
this tool.
I believe that to the best of my knowledge, all of the information I have supplied within this tool is correc
Signature Date
Brenda Reid
19/10/76 ✔
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

EXERCISE INTENSITY GUIDELINES
< 40%
HRmax
≥ 90%
HRmax
Very hard
RPE# ≥ 7
• An intensity that
generally cannot be
sustained for longer
than about
10 minutes
HIGH
70 to <90%
HRmax
Hard
RPE# 5-6
• An aerobicactivity in
which a conversation
generally cannot
be maintained
uninterrupted
• An intensity that m
last up to about 30
minutes
VIGOROUS
55 to <70%
HRmax
Moderate to
somewhat hard
RPE# 3-4
• An aerobicactivity
that is able to be
conducted whilst
maintaining a
conversation
uninterrupted
• An intensity that m
last between 30 and
60 minutes
MODERATE
40 to <55%
HRmax
Very light to light
RPE# 1-2
• An aerobicactivity
that does not cause a
noticeable change in
breathing rate
• An intensity that ca
be sustained for at
least 60 minutes
LIGHT
SEDENTARY Very, very light
RPE# < 1
• Activities that usually
involve sitting or
lying and that have
little additional
movement and a low
energy requirement
INTENSITY
CATEGORY
HEART RATE
MEASURES
PERCEIVED EXERTION
MEASURES
DESCRIPTIVE
MEASURES
# = Borg’s Rating of Perceived Exertion (RPE) scale, category scale 0-10
Page 4
< 40%
HRmax
≥ 90%
HRmax
Very hard
RPE# ≥ 7
• An intensity that
generally cannot be
sustained for longer
than about
10 minutes
HIGH
70 to <90%
HRmax
Hard
RPE# 5-6
• An aerobicactivity in
which a conversation
generally cannot
be maintained
uninterrupted
• An intensity that m
last up to about 30
minutes
VIGOROUS
55 to <70%
HRmax
Moderate to
somewhat hard
RPE# 3-4
• An aerobicactivity
that is able to be
conducted whilst
maintaining a
conversation
uninterrupted
• An intensity that m
last between 30 and
60 minutes
MODERATE
40 to <55%
HRmax
Very light to light
RPE# 1-2
• An aerobicactivity
that does not cause a
noticeable change in
breathing rate
• An intensity that ca
be sustained for at
least 60 minutes
LIGHT
SEDENTARY Very, very light
RPE# < 1
• Activities that usually
involve sitting or
lying and that have
little additional
movement and a low
energy requirement
INTENSITY
CATEGORY
HEART RATE
MEASURES
PERCEIVED EXERTION
MEASURES
DESCRIPTIVE
MEASURES
# = Borg’s Rating of Perceived Exertion (RPE) scale, category scale 0-10
Page 4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
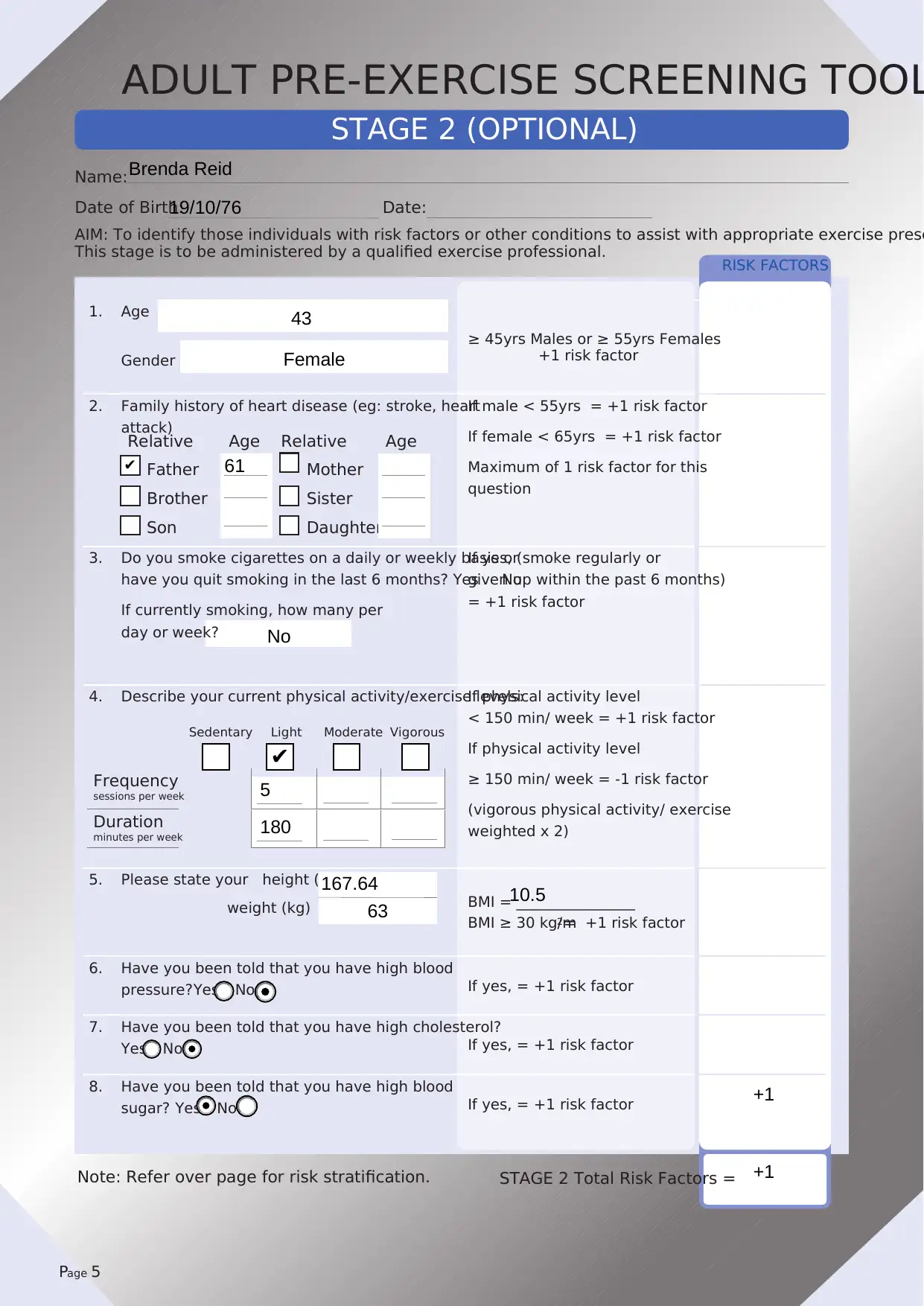
RISK FACTORS
Relative Age Relative Age
Father Mother
Brother Sister
Son Daughter
1. Age
Gender
≥ 45yrs Males or ≥ 55yrs Females
+1 risk factor
2. Family history of heart disease (eg: stroke, heart
attack)
If male < 55yrs = +1 risk factor
If female < 65yrs = +1 risk factor
Maximum of 1 risk factor for this
question
3. Do you smoke cigarettes on a daily or weekly basis or
have you quit smoking in the last 6 months? Yes No
If currently smoking, how many per
day or week?
If yes, (smoke regularly or
given up within the past 6 months)
= +1 risk factor
4. Describe your current physical activity/exercise levels:If physical activity level
< 150 min/ week = +1 risk factor
If physical activity level
≥ 150 min/ week = -1 risk factor
(vigorous physical activity/ exercise
weighted x 2)
5. Please state your height (cm)
weight (kg) BMI = ________________
BMI ≥ 30 kg/m2 = +1 risk factor
6. Have you been told that you have high blood
pressure? Yes No If yes, = +1 risk factor
7. Have you been told that you have high cholesterol?
Yes No If yes, = +1 risk factor
8. Have you been told that you have high blood
sugar? Yes No If yes, = +1 risk factor
STAGE 2 (OPTIONAL)
AIM: To identify those individuals with risk factors or other conditions to assist with appropriate exercise presc
This stage is to be administered by a qualified exercise professional.
STAGE 2 Total Risk Factors =
Name:
Date of Birth: Date:
Page 5
Note: Refer over page for risk stratification.
Sedentary Light Moderate Vigorous
Frequency
sessions per week
Duration
minutes per week
ADULT PRE-EXERCISE SCREENING TOOL
Brenda Reid
19/10/76
43
Female
✔ 61
No
✔
5
180
167.64 10.5
63
+1
+1
Relative Age Relative Age
Father Mother
Brother Sister
Son Daughter
1. Age
Gender
≥ 45yrs Males or ≥ 55yrs Females
+1 risk factor
2. Family history of heart disease (eg: stroke, heart
attack)
If male < 55yrs = +1 risk factor
If female < 65yrs = +1 risk factor
Maximum of 1 risk factor for this
question
3. Do you smoke cigarettes on a daily or weekly basis or
have you quit smoking in the last 6 months? Yes No
If currently smoking, how many per
day or week?
If yes, (smoke regularly or
given up within the past 6 months)
= +1 risk factor
4. Describe your current physical activity/exercise levels:If physical activity level
< 150 min/ week = +1 risk factor
If physical activity level
≥ 150 min/ week = -1 risk factor
(vigorous physical activity/ exercise
weighted x 2)
5. Please state your height (cm)
weight (kg) BMI = ________________
BMI ≥ 30 kg/m2 = +1 risk factor
6. Have you been told that you have high blood
pressure? Yes No If yes, = +1 risk factor
7. Have you been told that you have high cholesterol?
Yes No If yes, = +1 risk factor
8. Have you been told that you have high blood
sugar? Yes No If yes, = +1 risk factor
STAGE 2 (OPTIONAL)
AIM: To identify those individuals with risk factors or other conditions to assist with appropriate exercise presc
This stage is to be administered by a qualified exercise professional.
STAGE 2 Total Risk Factors =
Name:
Date of Birth: Date:
Page 5
Note: Refer over page for risk stratification.
Sedentary Light Moderate Vigorous
Frequency
sessions per week
Duration
minutes per week
ADULT PRE-EXERCISE SCREENING TOOL
Brenda Reid
19/10/76
43
Female
✔ 61
No
✔
5
180
167.64 10.5
63
+1
+1
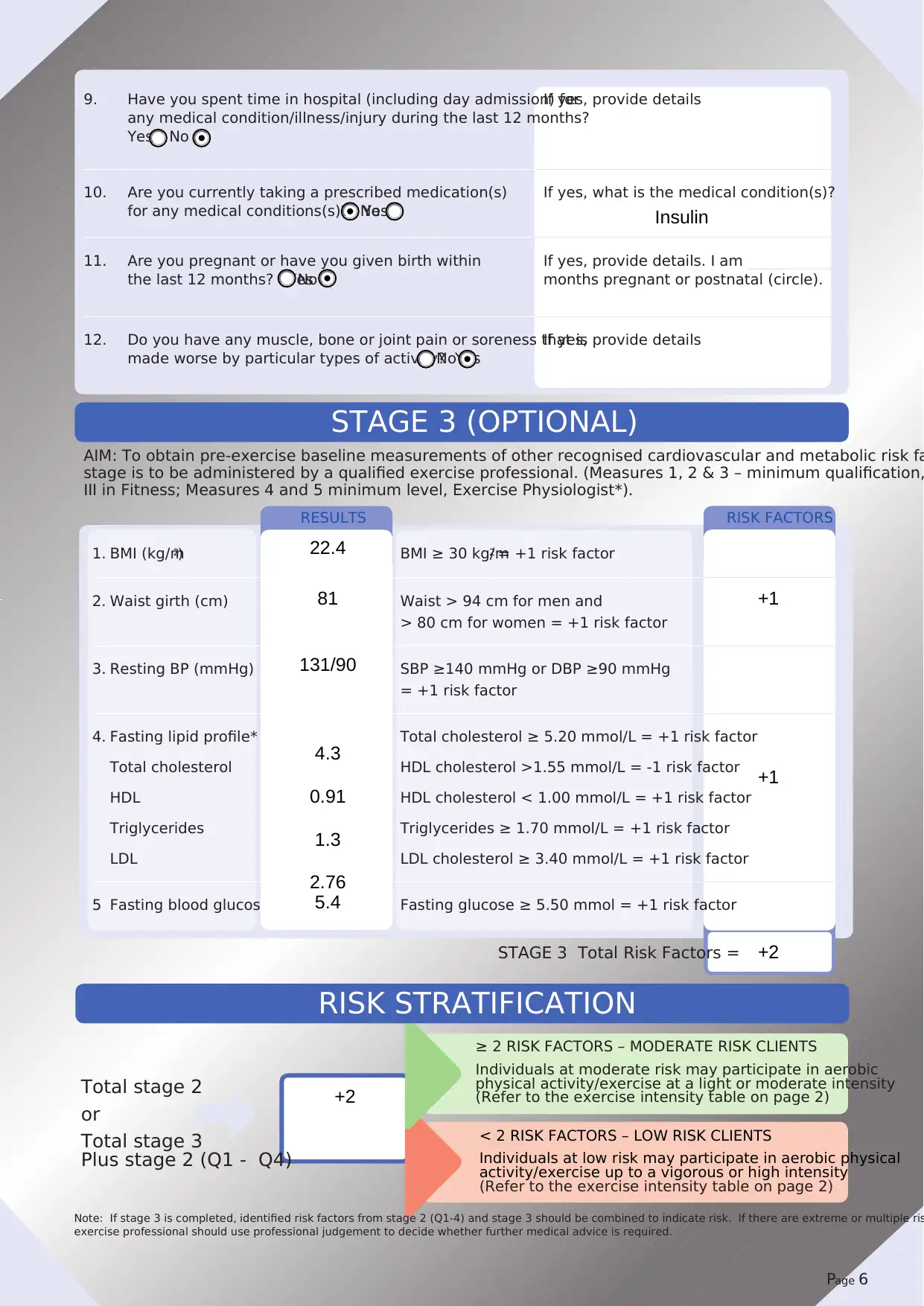
1. BMI (kg/m2) BMI ≥ 30 kg/m2 = +1 risk factor
2. Waist girth (cm) Waist > 94 cm for men and
> 80 cm for women = +1 risk factor
3. Resting BP (mmHg) SBP ≥140 mmHg or DBP ≥90 mmHg
= +1 risk factor
4. Fasting lipid profile*
Total cholesterol
HDL
Triglycerides
LDL
Total cholesterol ≥ 5.20 mmol/L = +1 risk factor
HDL cholesterol >1.55 mmol/L = -1 risk factor
HDL cholesterol < 1.00 mmol/L = +1 risk factor
Triglycerides ≥ 1.70 mmol/L = +1 risk factor
LDL cholesterol ≥ 3.40 mmol/L = +1 risk factor
5 Fasting blood glucose* Fasting glucose ≥ 5.50 mmol = +1 risk factor
RESULTS
STAGE 3 Total Risk Factors =
RISK STRATIFICATION
STAGE 3 (OPTIONAL)
AIM: To obtain pre-exercise baseline measurements of other recognised cardiovascular and metabolic risk fa
stage is to be administered by a qualified exercise professional. (Measures 1, 2 & 3 – minimum qualification,
III in Fitness; Measures 4 and 5 minimum level, Exercise Physiologist*).
RISK FACTORS
Total stage 2
or
Total stage 3
Plus stage 2 (Q1 - Q4)
Note: If stage 3 is completed, identified risk factors from stage 2 (Q1-4) and stage 3 should be combined to indicate risk. If there are extreme or multiple ris
exercise professional should use professional judgement to decide whether further medical advice is required.
≥ 2 RISK FACTORS – MODERATE RISK CLIENTS
Individuals at moderate risk may participate in aerobic
physical activity/exercise at a light or moderate intensity
(Refer to the exercise intensity table on page 2)
< 2 RISK FACTORS – LOW RISK CLIENTS
Individuals at low risk may participate in aerobic physical
activity/exercise up to a vigorous or high intensity
(Refer to the exercise intensity table on page 2)
9. Have you spent time in hospital (including day admission) for
any medical condition/illness/injury during the last 12 months?
Yes No
If yes, provide details
10. Are you currently taking a prescribed medication(s)
for any medical conditions(s)? YesNo
If yes, what is the medical condition(s)?
11. Are you pregnant or have you given birth within
the last 12 months? YesNo
If yes, provide details. I am _____________
months pregnant or postnatal (circle).
12. Do you have any muscle, bone or joint pain or soreness that is
made worse by particular types of activity? YesNo
If yes, provide details
Page 6
Insulin
22.4
81 +1
131/90
4.3
0.91
1.3
2.76
+1
5.4
+2
+2
2. Waist girth (cm) Waist > 94 cm for men and
> 80 cm for women = +1 risk factor
3. Resting BP (mmHg) SBP ≥140 mmHg or DBP ≥90 mmHg
= +1 risk factor
4. Fasting lipid profile*
Total cholesterol
HDL
Triglycerides
LDL
Total cholesterol ≥ 5.20 mmol/L = +1 risk factor
HDL cholesterol >1.55 mmol/L = -1 risk factor
HDL cholesterol < 1.00 mmol/L = +1 risk factor
Triglycerides ≥ 1.70 mmol/L = +1 risk factor
LDL cholesterol ≥ 3.40 mmol/L = +1 risk factor
5 Fasting blood glucose* Fasting glucose ≥ 5.50 mmol = +1 risk factor
RESULTS
STAGE 3 Total Risk Factors =
RISK STRATIFICATION
STAGE 3 (OPTIONAL)
AIM: To obtain pre-exercise baseline measurements of other recognised cardiovascular and metabolic risk fa
stage is to be administered by a qualified exercise professional. (Measures 1, 2 & 3 – minimum qualification,
III in Fitness; Measures 4 and 5 minimum level, Exercise Physiologist*).
RISK FACTORS
Total stage 2
or
Total stage 3
Plus stage 2 (Q1 - Q4)
Note: If stage 3 is completed, identified risk factors from stage 2 (Q1-4) and stage 3 should be combined to indicate risk. If there are extreme or multiple ris
exercise professional should use professional judgement to decide whether further medical advice is required.
≥ 2 RISK FACTORS – MODERATE RISK CLIENTS
Individuals at moderate risk may participate in aerobic
physical activity/exercise at a light or moderate intensity
(Refer to the exercise intensity table on page 2)
< 2 RISK FACTORS – LOW RISK CLIENTS
Individuals at low risk may participate in aerobic physical
activity/exercise up to a vigorous or high intensity
(Refer to the exercise intensity table on page 2)
9. Have you spent time in hospital (including day admission) for
any medical condition/illness/injury during the last 12 months?
Yes No
If yes, provide details
10. Are you currently taking a prescribed medication(s)
for any medical conditions(s)? YesNo
If yes, what is the medical condition(s)?
11. Are you pregnant or have you given birth within
the last 12 months? YesNo
If yes, provide details. I am _____________
months pregnant or postnatal (circle).
12. Do you have any muscle, bone or joint pain or soreness that is
made worse by particular types of activity? YesNo
If yes, provide details
Page 6
Insulin
22.4
81 +1
131/90
4.3
0.91
1.3
2.76
+1
5.4
+2
+2
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

7 | Assessment 3.2 - Client Screening & Assessment
2. Use the template documents on the following pages to conduct and record all of the followin
the client:
a. Goal Setting, including:
• Client expectations
• Exercise/activity preferences
• Current and past physical activity participation
b. Health Appraisals, including:
• Resting Heart Rate
• Blood Pressure
• BMI
• W:H Ratio
• Girths
• Skinfolds (if available)
• BIA Body Composition Analysis (if available)
c. Fitness Appraisals, including:
• Aerobic Submax or Step Test
• Sit & Reach
• Maximal Push Up Test
• Plank Test
• Curl Ups Test
Assessor Use Only
Satisfactory Resubmit
ASSESSMENT TIP
Before you complete the client health and fitness assessment click on
following videos for tips on how to conduct each of the health and fitne
appraisals:
• Health and Fitness Consultation
• Blood Pressure
• Girth Measurements
• Resting Heart Rate
• Skinfolds
• Sit and Reach Test
2. Use the template documents on the following pages to conduct and record all of the followin
the client:
a. Goal Setting, including:
• Client expectations
• Exercise/activity preferences
• Current and past physical activity participation
b. Health Appraisals, including:
• Resting Heart Rate
• Blood Pressure
• BMI
• W:H Ratio
• Girths
• Skinfolds (if available)
• BIA Body Composition Analysis (if available)
c. Fitness Appraisals, including:
• Aerobic Submax or Step Test
• Sit & Reach
• Maximal Push Up Test
• Plank Test
• Curl Ups Test
Assessor Use Only
Satisfactory Resubmit
ASSESSMENT TIP
Before you complete the client health and fitness assessment click on
following videos for tips on how to conduct each of the health and fitne
appraisals:
• Health and Fitness Consultation
• Blood Pressure
• Girth Measurements
• Resting Heart Rate
• Skinfolds
• Sit and Reach Test
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
AUSTRALIAN FITNESS ACADEMY © | 8
3. When conducting the appraisal, ensure you:
a. Obtain consent
b. Use open and closed questioning to obtain information in a polite and friendly manner
c. Communicate the name of the test to the client
d. Explain to the client why you are conducting the test in relation to their goals
e. Explain to the client the process/procedure involved in the test
f. State and discuss the meaning of the test results for the client
g. Communicate appropriately for the client and develop rapport
h. Monitor the client for signs and symptoms of intolerance and discontinue fitness assessme
required
ASSESSMENT TIP
If you would like a chance to practice the health consultation prior to c
this assessment, you can download all of the relevant documents by cl
the resources below:
• Adult pre-exercise screening tool
• Medical questionnaire - PARQ form
• Anthropometry measurements recording form
• Physical fitness assessment recording template
3. When conducting the appraisal, ensure you:
a. Obtain consent
b. Use open and closed questioning to obtain information in a polite and friendly manner
c. Communicate the name of the test to the client
d. Explain to the client why you are conducting the test in relation to their goals
e. Explain to the client the process/procedure involved in the test
f. State and discuss the meaning of the test results for the client
g. Communicate appropriately for the client and develop rapport
h. Monitor the client for signs and symptoms of intolerance and discontinue fitness assessme
required
ASSESSMENT TIP
If you would like a chance to practice the health consultation prior to c
this assessment, you can download all of the relevant documents by cl
the resources below:
• Adult pre-exercise screening tool
• Medical questionnaire - PARQ form
• Anthropometry measurements recording form
• Physical fitness assessment recording template
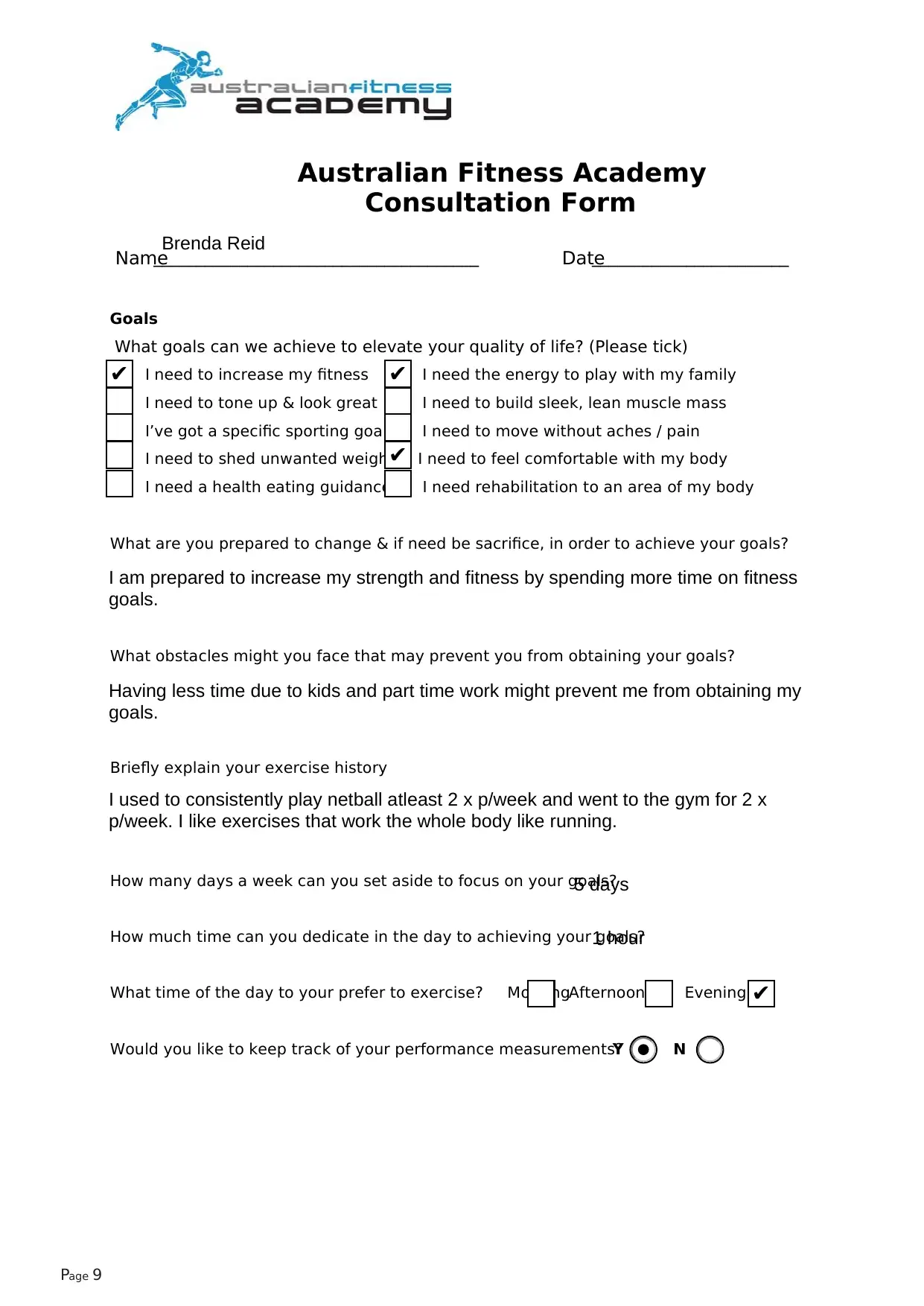
Australian Fitness Academy
Consultation Form
Name______________________________________ Date_______________________
Goals
What goals can we achieve to elevate your quality of life? (Please tick)
I need to increase my fitness I need the energy to play with my family
I need to tone up & look great I need to build sleek, lean muscle mass
I’ve got a specific sporting goal I need to move without aches / pain
I need to shed unwanted weight I need to feel comfortable with my body
I need a health eating guidance I need rehabilitation to an area of my body
What are you prepared to change & if need be sacrifice, in order to achieve your goals?
What obstacles might you face that may prevent you from obtaining your goals?
Briefly explain your exercise history
How many days a week can you set aside to focus on your goals?
How much time can you dedicate in the day to achieving your goals?
What time of the day to your prefer to exercise? MorningAfternoon Evening
Would you like to keep track of your performance measurements?Y N
Page 9
Brenda Reid
✔ ✔
✔
I am prepared to increase my strength and fitness by spending more time on fitness
goals.
Having less time due to kids and part time work might prevent me from obtaining my
goals.
I used to consistently play netball atleast 2 x p/week and went to the gym for 2 x
p/week. I like exercises that work the whole body like running.
5 days
1 hour
✔
Consultation Form
Name______________________________________ Date_______________________
Goals
What goals can we achieve to elevate your quality of life? (Please tick)
I need to increase my fitness I need the energy to play with my family
I need to tone up & look great I need to build sleek, lean muscle mass
I’ve got a specific sporting goal I need to move without aches / pain
I need to shed unwanted weight I need to feel comfortable with my body
I need a health eating guidance I need rehabilitation to an area of my body
What are you prepared to change & if need be sacrifice, in order to achieve your goals?
What obstacles might you face that may prevent you from obtaining your goals?
Briefly explain your exercise history
How many days a week can you set aside to focus on your goals?
How much time can you dedicate in the day to achieving your goals?
What time of the day to your prefer to exercise? MorningAfternoon Evening
Would you like to keep track of your performance measurements?Y N
Page 9
Brenda Reid
✔ ✔
✔
I am prepared to increase my strength and fitness by spending more time on fitness
goals.
Having less time due to kids and part time work might prevent me from obtaining my
goals.
I used to consistently play netball atleast 2 x p/week and went to the gym for 2 x
p/week. I like exercises that work the whole body like running.
5 days
1 hour
✔
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
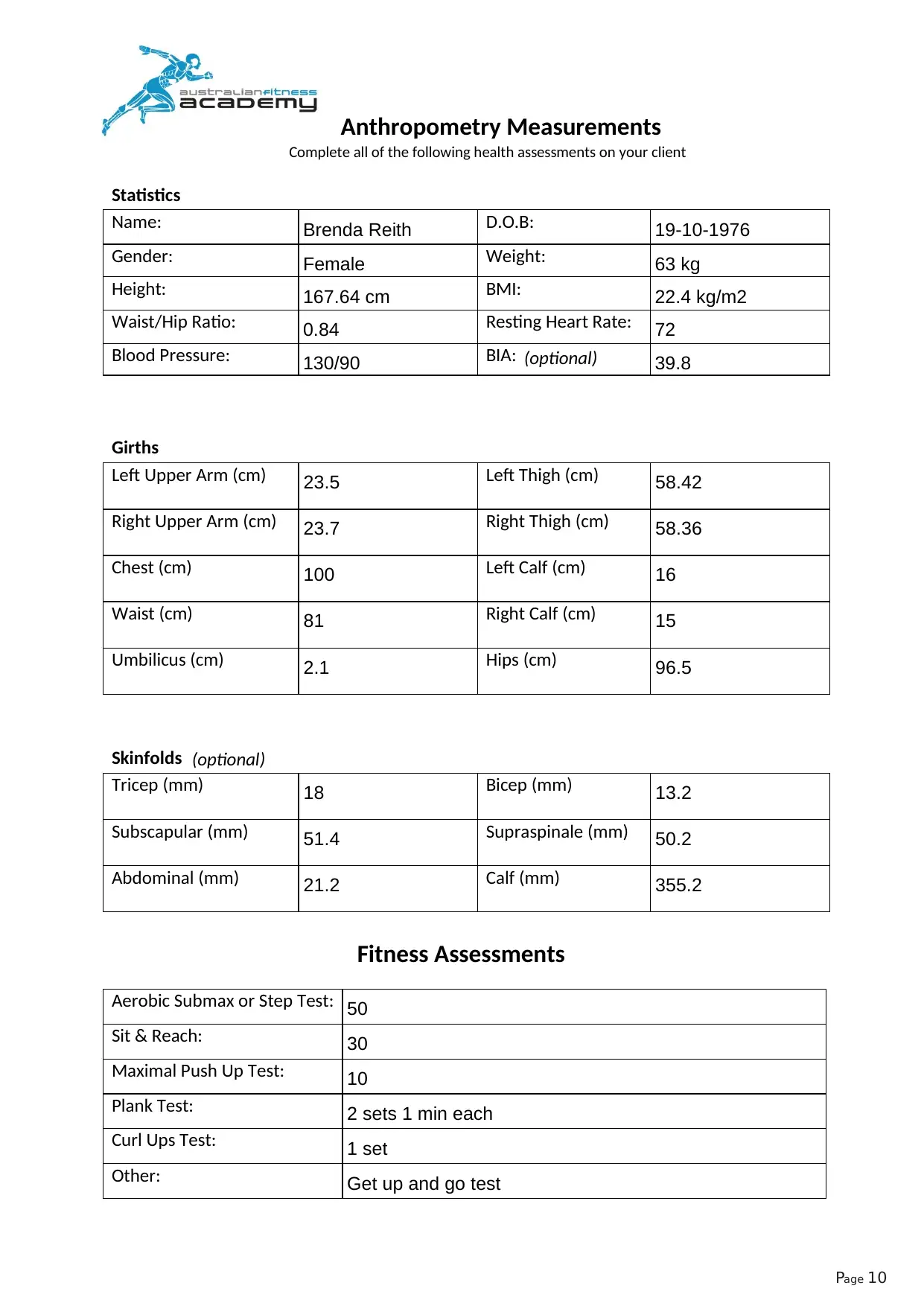
Anthropometry Measurements
Statistics
Name: D.O.B:
Gender: Weight:
Height: BMI:
Waist/Hip Ratio: Resting Heart Rate:
Blood Pressure: BIA:
Girths
Left Upper Arm (cm) Left Thigh (cm)
Right Upper Arm (cm) Right Thigh (cm)
Chest (cm) Left Calf (cm)
Waist (cm) Right Calf (cm)
Umbilicus (cm) Hips (cm)
Skinfolds
Tricep (mm) Bicep (mm)
Subscapular (mm) Supraspinale (mm)
Abdominal (mm) Calf (mm)
Fitness Assessments
Aerobic Submax or Step Test:
Sit & Reach:
Maximal Push Up Test:
Plank Test:
Curl Ups Test:
Other:
Page 10
Complete all of the following health assessments on your client
(optional)
(optional)
Brenda Reith 19-10-1976
Female 63 kg
167.64 cm 22.4 kg/m2
0.84 72
130/90 39.8
23.5 58.42
23.7 58.36
100 16
81 15
2.1 96.5
18 13.2
51.4 50.2
21.2 355.2
50
30
10
2 sets 1 min each
1 set
Get up and go test
Statistics
Name: D.O.B:
Gender: Weight:
Height: BMI:
Waist/Hip Ratio: Resting Heart Rate:
Blood Pressure: BIA:
Girths
Left Upper Arm (cm) Left Thigh (cm)
Right Upper Arm (cm) Right Thigh (cm)
Chest (cm) Left Calf (cm)
Waist (cm) Right Calf (cm)
Umbilicus (cm) Hips (cm)
Skinfolds
Tricep (mm) Bicep (mm)
Subscapular (mm) Supraspinale (mm)
Abdominal (mm) Calf (mm)
Fitness Assessments
Aerobic Submax or Step Test:
Sit & Reach:
Maximal Push Up Test:
Plank Test:
Curl Ups Test:
Other:
Page 10
Complete all of the following health assessments on your client
(optional)
(optional)
Brenda Reith 19-10-1976
Female 63 kg
167.64 cm 22.4 kg/m2
0.84 72
130/90 39.8
23.5 58.42
23.7 58.36
100 16
81 15
2.1 96.5
18 13.2
51.4 50.2
21.2 355.2
50
30
10
2 sets 1 min each
1 set
Get up and go test
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11 | Assessment 3.2 - Client Screening & Assessment
Briefly outline how you communicated each of the following during your health consultation:
a. Obtain consent
b. Use open and closed questioning to obtain information in a polite and friendly manner
c. Communicate the name of the test to the client
d. Explain to the client why you are conducting the test in relation to their goals
e. Explain to the client the process/procedure involved in the test
f. State and discuss the meaning of the test results for the client
g. Communicate appropriately for the client and develop rapport
h. Monitor the client for signs and symptoms of intolerance and discontinue fitness assessme
required
Assessor Use Only
Satisfactory Resubmit
For the purpose of health and fitness assessment i would like to take your consent first on an
individual level so that you can provide your informed as well as written consent for the
assessment in the written consent form.
The idea behind the health consultation is through some open and closed ended questions such
as:
1. Could you tell me more about your problem?
2. Tell me the history of your problem?
3. When did it start?
4. How did it come on?
5. As you have mentioned earlier about the problem, could you please tell me more?
Closed questions:
1. “What do you already know about your illness?”
2.“What is your understanding of the illness?”
3.“How much information would you like to receive at this
time?”
4.“Do you prefer to receive the information in stages or all
at once?”
5. What are your health goals?
6. How far you can go to achieve them?
7. How much time you will be able to spend to achieve your goals?
The test is about the health screening and fitness assessment and it will help to achieve a
particular goal.
The tests such as anthropometry measurement, etc will be carried out to rely on body
measurements to evaluate a patient's overall health such as body mass index, or BMI, is a
measurement of a person's weight-to-height ratio, statistics, girths, skin-folds, etc.
Body measurements are always taken on the right side of the body. However,
some measurements may be taken on the left side of the body because of casts,
amputation or other reasons.
1. Waist Circumference: Measure the circumference of the waist right above the
iliac crest. Ask participant to stand and conduct the measure only
over undergarments if the participant will permit this.
2. Hip- Measure the hip at the ½ way point between the iliac crest and the greater trocanter.
Remove stockings etc. to avoid inaccurate measure. Ask participant to stand and conduct the
measurement procedure.
3. Height- Measure is done standing up against a wall surface and
with a special device.
4. Weight- Measure is done standing on weight scale without
pressure support
5. Get up and Go test- Place mark at the end of the 10 feet distance. Place chair in a flat and
safe surface. Explain to participant to not push up from the chair
from rising and to cross arms in from of chest for
balance when rising from chair. Prepare timer for 30 seconds
These measures provide valuable information because persons with certain values may be at
increased risk for cardiovascular disease, arthritis, adult onset diabetes and limitations in
ambulation that may lead to falls and possible bone fractures. The anthropometric data obtained
in this study will provide valuable and essential information needed to better understand the
functional health status.
Precision and accuracy are the goals for the measurement process. Accuracy in both
observation and recording of measurement is essential. When an error is noted the procedure
must be repeated.
If during the measurement the respondent becomes unsteady, weak or indicates that they must
discontinue the procedure, stop immediately and assist the individual to a chair or to
obtain their balance. After a period of rest you may ask them if they wish to proceed. If
they indicate they will continue proceed with caution. If they do not wish to continue
then discontinue the process and record in the anthropometric log.
Briefly outline how you communicated each of the following during your health consultation:
a. Obtain consent
b. Use open and closed questioning to obtain information in a polite and friendly manner
c. Communicate the name of the test to the client
d. Explain to the client why you are conducting the test in relation to their goals
e. Explain to the client the process/procedure involved in the test
f. State and discuss the meaning of the test results for the client
g. Communicate appropriately for the client and develop rapport
h. Monitor the client for signs and symptoms of intolerance and discontinue fitness assessme
required
Assessor Use Only
Satisfactory Resubmit
For the purpose of health and fitness assessment i would like to take your consent first on an
individual level so that you can provide your informed as well as written consent for the
assessment in the written consent form.
The idea behind the health consultation is through some open and closed ended questions such
as:
1. Could you tell me more about your problem?
2. Tell me the history of your problem?
3. When did it start?
4. How did it come on?
5. As you have mentioned earlier about the problem, could you please tell me more?
Closed questions:
1. “What do you already know about your illness?”
2.“What is your understanding of the illness?”
3.“How much information would you like to receive at this
time?”
4.“Do you prefer to receive the information in stages or all
at once?”
5. What are your health goals?
6. How far you can go to achieve them?
7. How much time you will be able to spend to achieve your goals?
The test is about the health screening and fitness assessment and it will help to achieve a
particular goal.
The tests such as anthropometry measurement, etc will be carried out to rely on body
measurements to evaluate a patient's overall health such as body mass index, or BMI, is a
measurement of a person's weight-to-height ratio, statistics, girths, skin-folds, etc.
Body measurements are always taken on the right side of the body. However,
some measurements may be taken on the left side of the body because of casts,
amputation or other reasons.
1. Waist Circumference: Measure the circumference of the waist right above the
iliac crest. Ask participant to stand and conduct the measure only
over undergarments if the participant will permit this.
2. Hip- Measure the hip at the ½ way point between the iliac crest and the greater trocanter.
Remove stockings etc. to avoid inaccurate measure. Ask participant to stand and conduct the
measurement procedure.
3. Height- Measure is done standing up against a wall surface and
with a special device.
4. Weight- Measure is done standing on weight scale without
pressure support
5. Get up and Go test- Place mark at the end of the 10 feet distance. Place chair in a flat and
safe surface. Explain to participant to not push up from the chair
from rising and to cross arms in from of chest for
balance when rising from chair. Prepare timer for 30 seconds
These measures provide valuable information because persons with certain values may be at
increased risk for cardiovascular disease, arthritis, adult onset diabetes and limitations in
ambulation that may lead to falls and possible bone fractures. The anthropometric data obtained
in this study will provide valuable and essential information needed to better understand the
functional health status.
Precision and accuracy are the goals for the measurement process. Accuracy in both
observation and recording of measurement is essential. When an error is noted the procedure
must be repeated.
If during the measurement the respondent becomes unsteady, weak or indicates that they must
discontinue the procedure, stop immediately and assist the individual to a chair or to
obtain their balance. After a period of rest you may ask them if they wish to proceed. If
they indicate they will continue proceed with caution. If they do not wish to continue
then discontinue the process and record in the anthropometric log.
AUSTRALIAN FITNESS ACADEMY © | 12
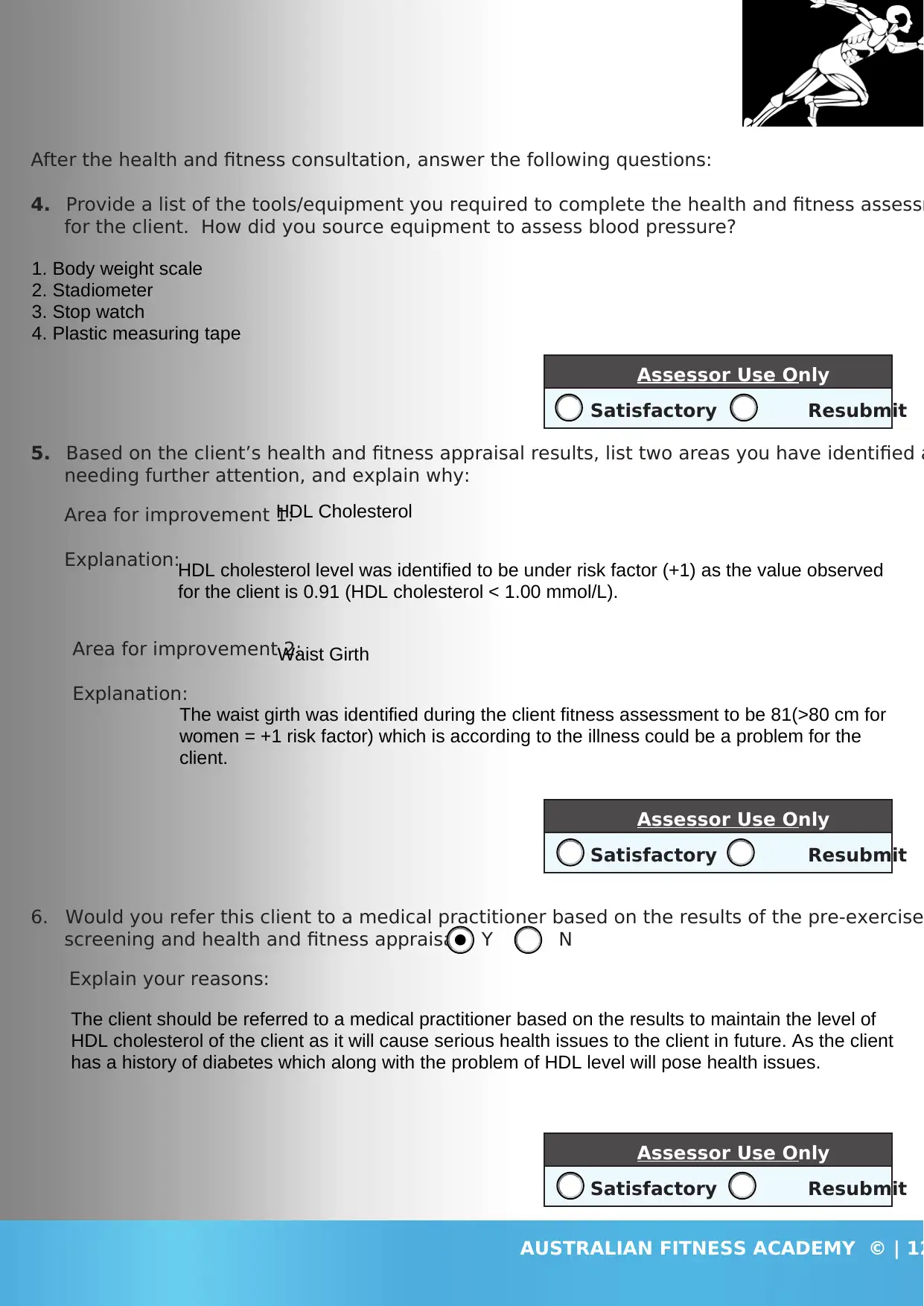
After the health and fitness consultation, answer the following questions:
4. Provide a list of the tools/equipment you required to complete the health and fitness assessm
for the client. How did you source equipment to assess blood pressure?
5. Based on the client’s health and fitness appraisal results, list two areas you have identified a
needing further attention, and explain why:
Area for improvement 1:
Explanation:
Area for improvement 2:
Explanation:
6. Would you refer this client to a medical practitioner based on the results of the pre-exercise
screening and health and fitness appraisal? Y / N
Explain your reasons:
Assessor Use Only
Satisfactory Resubmit
Assessor Use Only
Satisfactory Resubmit
Assessor Use Only
Satisfactory Resubmit
1. Body weight scale
2. Stadiometer
3. Stop watch
4. Plastic measuring tape
HDL Cholesterol
HDL cholesterol level was identified to be under risk factor (+1) as the value observed
for the client is 0.91 (HDL cholesterol < 1.00 mmol/L).
Waist Girth
The waist girth was identified during the client fitness assessment to be 81(>80 cm for
women = +1 risk factor) which is according to the illness could be a problem for the
client.
The client should be referred to a medical practitioner based on the results to maintain the level of
HDL cholesterol of the client as it will cause serious health issues to the client in future. As the client
has a history of diabetes which along with the problem of HDL level will pose health issues.
After the health and fitness consultation, answer the following questions:
4. Provide a list of the tools/equipment you required to complete the health and fitness assessm
for the client. How did you source equipment to assess blood pressure?
5. Based on the client’s health and fitness appraisal results, list two areas you have identified a
needing further attention, and explain why:
Area for improvement 1:
Explanation:
Area for improvement 2:
Explanation:
6. Would you refer this client to a medical practitioner based on the results of the pre-exercise
screening and health and fitness appraisal? Y / N
Explain your reasons:
Assessor Use Only
Satisfactory Resubmit
Assessor Use Only
Satisfactory Resubmit
Assessor Use Only
Satisfactory Resubmit
1. Body weight scale
2. Stadiometer
3. Stop watch
4. Plastic measuring tape
HDL Cholesterol
HDL cholesterol level was identified to be under risk factor (+1) as the value observed
for the client is 0.91 (HDL cholesterol < 1.00 mmol/L).
Waist Girth
The waist girth was identified during the client fitness assessment to be 81(>80 cm for
women = +1 risk factor) which is according to the illness could be a problem for the
client.
The client should be referred to a medical practitioner based on the results to maintain the level of
HDL cholesterol of the client as it will cause serious health issues to the client in future. As the client
has a history of diabetes which along with the problem of HDL level will pose health issues.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 24
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.